
Artificial Intelligence Models in Health Information Exchange: A Systematic Review of Clinical Implications
 , ,
, ,
Abstract
:1. Introduction
1.1. Background
1.2. Problem Statement and Research Questions
- What are the implementations of AI models in the HIE?
- What is the effectiveness of different AI models in improving clinical outcomes based on HIE data?
- What are the barriers to the implementation of AI in HIE?
- What limitations have been identified in current studies, and what potential future research directions are suggested?
1.3. Objectives
2. Methods
2.1. Search Strategy
| Research Units | Keywords/Terms |
| Health Information Systems/Standards | “Health Information Exchange”, “Health Level Seven”, “HL7”, “HIE”, “FHIR”, “HIO”, “Fast Healthcare Interoperability Resource” |
| Artificial Intelligence & Data Analytics Methods | “Machine Learning”, “Natural Language Processing”, “Artificial Intelligence”, “Logistic Models” |
2.2. Data Sources and Databases Searched
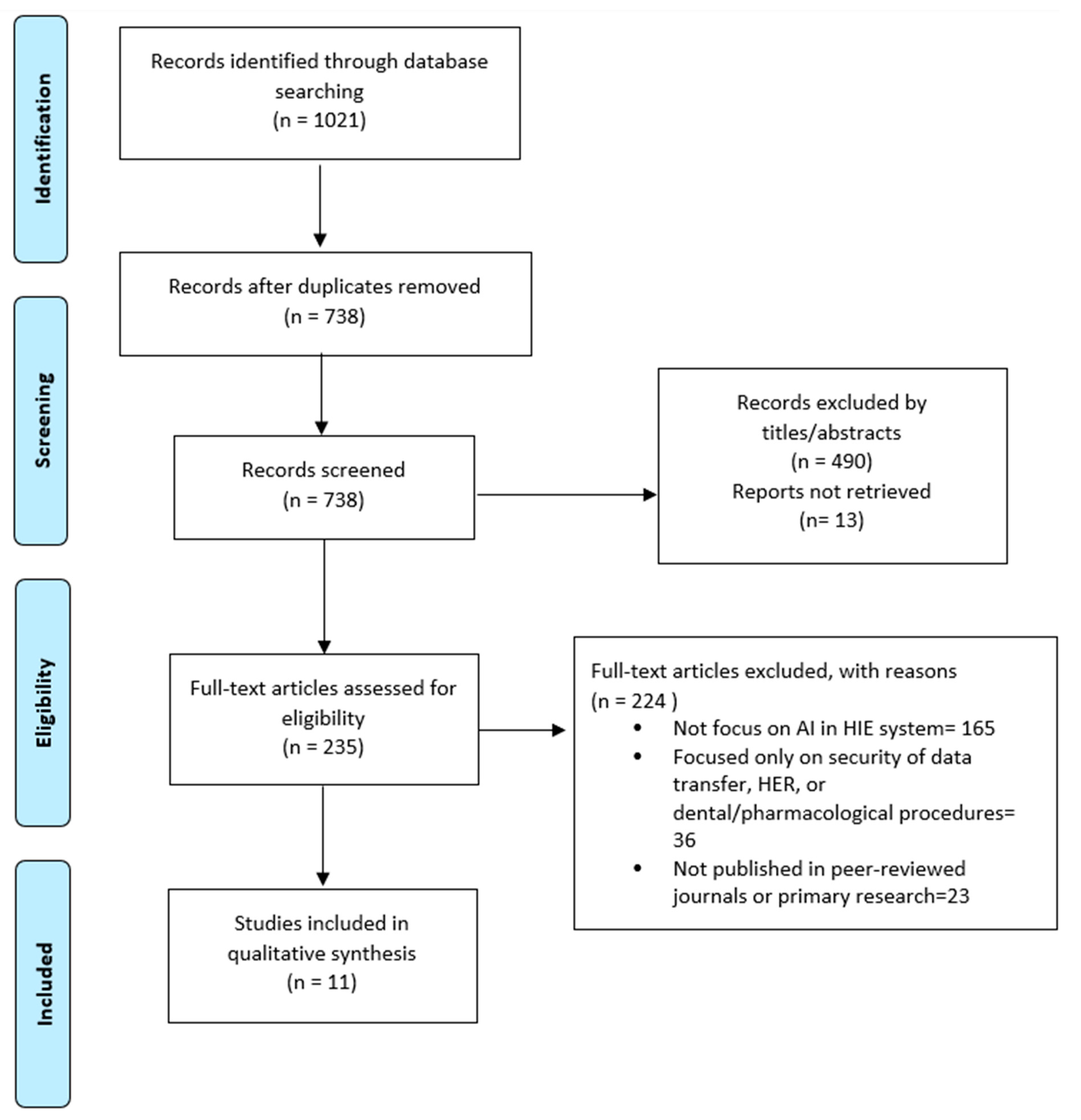
2.3. Study Eligibility and Selection Process
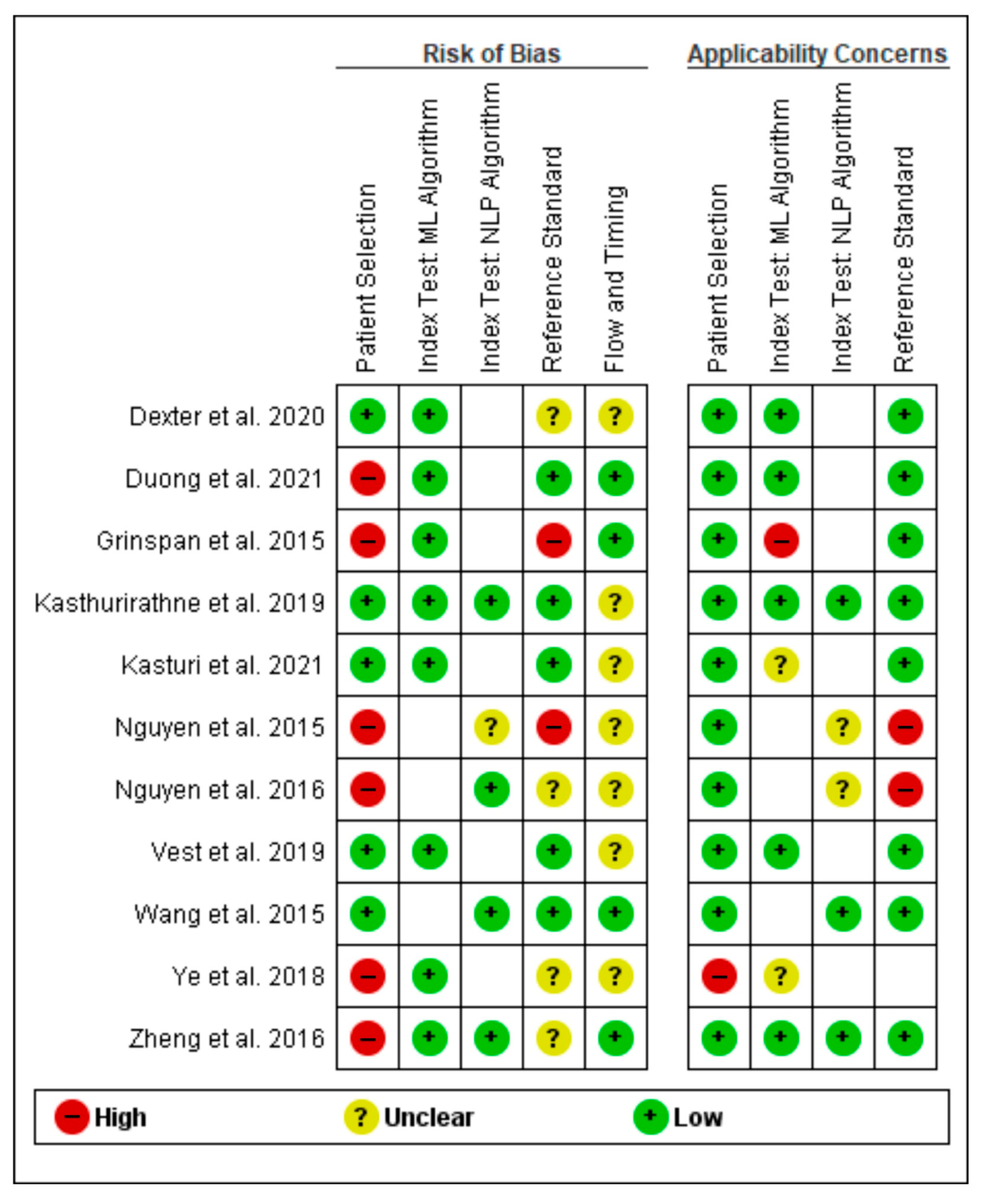
2.4. Data Quality and Risk of Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Included Studies
3.1.1. Number of Included Studies
3.1.2. Type of Studies
3.1.3. Parameters Obtained
3.2. Types of HIE Standard, FHIR Medical Coding Systems, and Application Programming Interface (API)
3.3. Types of AI Models, Applicability, and Validation
3.4. Models Metric Scores
4. Discussion
4.1. Implications and Key Findings
4.1.1. Health Information Exchange, Fast Healthcare Interoperability Resources, and Application Programming Interface
4.1.2. FHIR Medical Coding System
4.1.3. AI Models in Healthcare Data Exchange
4.2. Strengths and Limitations of the Review
4.3. Future Directions and Recommendations
- Future research should utilize diverse data sources (e.g., imaging records and lab findings) and explore alternative machine-learning methods to improve the model’s ability to identify a broader range of disorders.
- Include diverse patient populations and real-world settings to assess technical design effectiveness and conduct longer-term risk evaluations.
- To ensure inclusivity, future research should implement strict population confounding controls, critically analyze effects across models, and prioritize addressing healthcare disparities, with a focus on underserved areas and age-related concerns.
- To optimize model accuracy and predictive value, studies should account for intervention effects, balance sensitivity with positive predictive value, and try to integrate all pertinent predictive markers to enrich model contributions.
- Further exploration of the ethical, legal, and societal implications of AI in HIE data can enhance our understanding of the significant challenges and issues in healthcare AI.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suraj, V.; Del Vecchio Fitz, C.; Kleiman, L.B.; Bhavnani, S.K.; Jani, C.; Shah, S.; McKay, R.R.; Warner, J.; Alterovitz, G. SMART COVID Navigator, a Clinical Decision Support Tool for COVID-19 Treatment: Design and Development Study. J. Med. Internet Res. 2022, 24, e29279. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, M.; Celi, L.A.; Stone, D.J. State of the art review: The data revolution in critical care. Crit. Care 2015, 19, 118. [Google Scholar] [CrossRef] [PubMed]
- Pysmennyi, I. Integrated medical data management systems review. Visnyk Universytetu Ukr. 2019, 23, 166–177. [Google Scholar] [CrossRef]
- Wilkerson, M.L.; Henricks, W.H.; Castellani, W.J.; Whitsitt, M.S.; Sinard, J.H. Management of laboratory data and information exchange in the electronic health record. Arch. Pathol. Lab. Med. 2015, 139, 319–327. [Google Scholar] [CrossRef]
- Yılmaz, Ö.; Erdur, R.C.; Türksever, M. SAMS–a systems architecture for developing intelligent health information systems. J. Med. Syst. 2013, 37, 9989. [Google Scholar] [CrossRef]
- Lapointe, L.; Mignerat, M.; Vedel, I. The IT productivity paradox in health: A stakeholder’s perspective. Int. J. Med. Inform. 2011, 80, 102–115. [Google Scholar] [CrossRef]
- Horth, R.Z.; Wagstaff, S.; Jeppson, T.; Patel, V.; McClellan, J.; Bissonette, N.; Friedrichs, M.; Dunn, A.C. Use of electronic health records from a statewide health information exchange to support public health surveillance of diabetes and hypertension. BMC Public Health 2019, 19, 1106. [Google Scholar] [CrossRef]
- World Health Organization. Global Diffusion of eHealth: Making Universal Health Coverage Achievable: Report of the Third Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Geraci, A. IEEE Standard Computer Dictionary: Compilation of IEEE Standard Computer Glossaries; IEEE Press: Piscataway, NJ, USA, 1991. [Google Scholar]
- Shapiro, J.S.; Mostashari, F.; Hripcsak, G.; Soulakis, N.; Kuperman, G. Using health information exchange to improve public health. Am. J. Public Health 2011, 101, 616–623. [Google Scholar] [CrossRef]
- Birkhead, G.S. Successes and Continued Challenges of Electronic Health Records for Chronic Disease Surveillance; American Public Health Association: Washington, DC, USA, 2017; Volume 107, pp. 1365–1367. [Google Scholar]
- Garg, N.; Kuperman, G.; Onyile, A.; Lowry, T.; Genes, N.; DiMaggio, C.; Richardson, L.; Husk, G.; Shapiro, J.S. Validating Health Information Exchange (HIE) Data For Quality Measurement Across Four Hospitals. AMIA Annu. Symp. Proc. 2014, 2014, 573–579. [Google Scholar]
- Engel, N.; Wang, H.; Jiang, X.; Lau, C.Y.; Patterson, J.; Acharya, N.; Beaton, M.; Sulieman, L.; Pavinkurve, N.; Natarajan, K. EHR Data Quality Assessment Tools and Issue Reporting Workflows for the ‘All of Us’ Research Program Clinical Data Research Network. AMIA Annu. Symp. Proc. 2022, 2022, 186–195. [Google Scholar]
- Pitoglou, S.; Filntisi, A.; Anastasiou, A.; Matsopoulos, G.K.; Koutsouris, D. Measuring the impact of anonymization on real-world consolidated health datasets engineered for secondary research use: Experiments in the context of MODELHealth project. Front. Digit. Health 2022, 4, 841853. [Google Scholar] [CrossRef] [PubMed]
- Eapen, B.R.; Sartipi, K.; Archer, N. Serverless on FHIR: Deploying machine learning models for healthcare on the cloud. arXiv 2020, arXiv:2006.04748. [Google Scholar]
- Eapen, B.R.; Archer, N.; Sartipi, K.; Yuan, Y. Drishti: A sense-plan-act extension to open mHealth framework using FHIR. In Proceedings of the 2019 IEEE/ACM 1st International Workshop on Software Engineering for Healthcare (SEH), Montreal, QC, Canada, 27 May 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 49–52. [Google Scholar]
- Ayaz, M.; Pasha, M.F.; Alahmadi, T.J.; Abdullah, N.N.B.; Alkahtani, H.K. Transforming Healthcare Analytics with FHIR: A Framework for Standardizing and Analyzing Clinical Data. Healthcare 2023, 11, 1729. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Holweg, F.; Achenbach, S.; Deppenwiese, N.; Gaede, L.; Prokosch, H.U. Towards a FHIR-Based Data Model for Coronary Angiography Observations. Stud. Health Technol. Inf. 2022, 292, 96–99. [Google Scholar] [CrossRef]
- Wegner, P.; Jose, G.M.; Lage-Rupprecht, V.; Golriz Khatami, S.; Zhang, B.; Springstubbe, S.; Jacobs, M.; Linden, T.; Ku, C.; Schultz, B.; et al. Common data model for COVID-19 datasets. Bioinformatics 2022, 38, 5466–5468. [Google Scholar] [CrossRef]
- Areia, M.; Mori, Y.; Correale, L.; Repici, A.; Bretthauer, M.; Sharma, P.; Taveira, F.; Spadaccini, M.; Antonelli, G.; Ebigbo, A.; et al. Cost-effectiveness of artificial intelligence for screening colonoscopy: A modelling study. Lancet. Digit. Health 2022, 4, e436–e444. [Google Scholar] [CrossRef]
- Huang, B.; Huang, H.; Zhang, S.; Zhang, D.; Shi, Q.; Liu, J.; Guo, J. Artificial intelligence in pancreatic cancer. Theranostics 2022, 12, 6931–6954. [Google Scholar] [CrossRef]
- Pei, Q.; Luo, Y.; Chen, Y.; Li, J.; Xie, D.; Ye, T. Artificial intelligence in clinical applications for lung cancer: Diagnosis, treatment and prognosis. Clin. Chem. Lab. Med. 2022, 60, 1974–1983. [Google Scholar] [CrossRef]
- Oemig, F.; Blobel, B. Natural language processing supporting interoperability in healthcare. In Text Mining: From Ontology Learning to Automated Text Processing Applications; Springer: Berlin/Heidelberg, Germany, 2014; pp. 137–156. [Google Scholar]
- Ohno-Machado, L. Realizing the full potential of electronic health records: The role of natural language processing. J. Am. Med. Inform. Assoc. 2011, 18, 539. [Google Scholar] [CrossRef]
- Siddique, S.; Chow, J.C. Machine learning in healthcare communication. Encyclopedia 2021, 1, 220–239. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Grinspan, Z.M.; Shapiro, J.S.; Abramson, E.L.; Hooker, G.; Kaushal, R.; Kern, L.M. Predicting frequent ED use by people with epilepsy with health information exchange data. Neurology 2015, 85, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Luo, J.; Hao, S.; Xu, H.; Shin, A.Y.; Jin, B.; Liu, R.; Deng, X.; Wang, L.; Zheng, L.; et al. NLP based congestive heart failure case finding: A prospective analysis on statewide electronic medical records. Int. J. Med. Inform. 2015, 84, 1039–1047. [Google Scholar] [CrossRef]
- Nguyen, A.N.; Moore, J.; O’Dwyer, J.; Philpot, S. Assessing the Utility of Automatic Cancer Registry Notifications Data Extraction from Free-Text Pathology Reports. AMIA Annu. Symp. Proc. AMIA Symp. 2015, 2015, 953–962. [Google Scholar]
- Nguyen, A.N.; Moore, J.; O’Dwyer, J.; Philpot, S. Automated Cancer Registry Notifications: Validation of a Medical Text Analytics System for Identifying Patients with Cancer from a State-Wide Pathology Repository. AMIA Annu. Symp Proc. 2016, 2016, 964–973. [Google Scholar]
- Zheng, L.; Wang, Y.; Hao, S.Y.; Shin, A.Y.; Jin, B.; Ngo, A.D.; Jackson-Browne, M.S.; Feller, D.J.; Fu, T.Y.; Zhang, K.; et al. Web-based Real-Time Case Finding for the Population Health Management of Patients With Diabetes Mellitus: A Prospective Validation of the Natural Language Processing-Based Algorithm with Statewide Electronic Medical Records. Jmir. Med. Inform. 2016, 4, 38–50. [Google Scholar] [CrossRef]
- Chengyin, Y.; Tianyun, F.; Shiying, H.; Yan, Z.; Wang, O.; Bo, J.; Minjie, X.; Modi, L.; Xin, Z.; Qian, W.; et al. Prediction of Incident Hypertension Within the Next Year: Prospective Study Using Statewide Electronic Health Records and Machine Learning. J. Med. Internet Res. 2018, 20, 22. [Google Scholar] [CrossRef]
- Vest, J.R.; Ben-Assuli, O. Prediction of emergency department revisits using area-level social determinants of health measures and health information exchange information. Int. J. Med. Inform. 2019, 129, 205–210. [Google Scholar] [CrossRef]
- Kasthurirathne, S.N.; Biondich, P.G.; Grannis, S.J.; Purkayastha, S.; Vest, J.R.; Jones, J.F. Identification of patients in need of advanced care for depression using data extracted from a statewide health information exchange: A machine learning approach. J. Med. Internet Res. 2019, 21, e13809. [Google Scholar] [CrossRef] [PubMed]
- Dexter, G.P.; Grannis, S.J.; Dixon, B.E.; Kasthurirathne, S.N. Generalization of machine learning approaches to identify notifiable conditions from a statewide health information exchange. AMIA Summits Transl. Sci. Proc. 2020, 2020, 152. [Google Scholar] [PubMed]
- Duong, S.Q.; Zheng, L.; Xia, M.J.; Jin, B.; Liu, M.D.; Li, Z.; Hao, S.Y.; Alfreds, S.T.; Sylvester, K.G.; Widen, E.; et al. Identification of patients at risk of new onset heart failure: Utilizing a large statewide health information exchange to train and validate a risk prediction model. PLoS ONE 2021, 16, e0260885. [Google Scholar] [CrossRef] [PubMed]
- Kasturi, S.N.; Park, J.; Wild, D.; Khan, B.; Haggstrom, D.A.; Grannis, S. Predicting COVID-19-related health care resource utilization across a statewide patient population: Model development study. J. Med. Internet Res. 2021, 23, e31337. [Google Scholar] [CrossRef]
- Zong, N.; Ngo, V.; Stone, D.J.; Wen, A.; Zhao, Y.; Yu, Y.; Liu, S.; Huang, M.; Wang, C.; Jiang, G. Leveraging genetic reports and electronic health records for the prediction of primary cancers: Algorithm development and validation study. JMIR Med. Inform. 2021, 9, e23586. [Google Scholar] [CrossRef]
- Tseng, T.W.; Su, C.F.; Lai, F. Fast Healthcare Interoperability Resources for Inpatient Deterioration Detection with Time-Series Vital Signs: Design and Implementation Study. JMIR Med. Inform. 2022, 10, e42429. [Google Scholar] [CrossRef]
- Amrollahi, F.; Shashikumar, S.P.; Kathiravelu, P.; Sharma, A.; Nemati, S. AIDEx—An Open-source Platform for Real-Time Forecasting Sepsis and A Case Study on Taking ML Algorithms to Production. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 5610–5614. [Google Scholar] [CrossRef]
- Henry, J.R.; Lynch, D.; Mals, J.; Shashikumar, S.P.; Holder, A.; Sharma, A.; Nemati, S. A FHIR-enabled streaming sepsis prediction system for ICUs. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: Piscataway, NJ, USA; pp. 4093–4096. [Google Scholar]
- Stern, E.; Micoulaud Franchi, J.A.; Dumas, G.; Moreira, J.; Mouchabac, S.; Maruani, J.; Philip, P.; Lejoyeux, M.; Geoffroy, P.A. How Can Digital Mental Health Enhance Psychiatry? Neuroscientist 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Shah, N.; Costello, K.; Mehta, A.; Kumar, D. Applications of Digital Health Technologies in Knee Osteoarthritis: Narrative Review. JMIR Rehabil. Assist. Technol. 2022, 9, e33489. [Google Scholar] [CrossRef]
- Sharma, S.; Mohanty, V.; Balappanavar, A.Y.; Chahar, P.; Rijhwani, K. Role of Digital Media in Promoting Oral Health: A Systematic Review. Cureus 2022, 14, e28893. [Google Scholar] [CrossRef]
- Lareyre, F.; Chaptoukaev, H.; Kiang, S.C.; Chaudhuri, A.; Behrendt, C.A.; Zuluaga, M.A.; Raffort, J. Telemedicine and Digital Health Applications in Vascular Surgery. J. Clin. Med. 2022, 11, 6047. [Google Scholar] [CrossRef] [PubMed]
- Nusir, M.; Rekik, M. Systematic review of co-design in digital health for COVID-19 research. Univers Access Inf. Soc. 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Janett, R.S.; Yeracaris, P.P. Electronic Medical Records in the American Health System: Challenges and lessons learned. Cien. Saude Colet. 2020, 25, 1293–1304. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.C.; Pollak, J.P.; Mandl, K.D. The Patient Role in a Federal National-Scale Health Information Exchange. J. Med. Internet Res. 2022, 24, e41750. [Google Scholar] [CrossRef]
- Lee, J.; Choi, J.Y. Improved efficiency of coding systems with health information technology. Sci. Rep. 2021, 11, 10294. [Google Scholar] [CrossRef]
- Harrison, J.E.; Weber, S.; Jakob, R.; Chute, C.G. ICD-11: An international classification of diseases for the twenty-first century. BMC Med. Inf. Decis. Mak. 2021, 21, 206. [Google Scholar] [CrossRef]
- Lin, H.L.; Cheng, S.M.; Hsu, D.F.; Huang, C.C.; Wu, D.C. Information System Implementation Optimizes Medical Coding. Stud. Health Technol. Inf. 2019, 264, 1706–1707. [Google Scholar] [CrossRef]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A standards-based, interoperable apps platform for electronic health records. J. Am. Med. Inform. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef]
- Vorisek, C.N.; Lehne, M.; Klopfenstein, S.A.I.; Mayer, P.J.; Bartschke, A.; Haese, T.; Thun, S. Fast Healthcare Interoperability Resources (FHIR) for Interoperability in Health Research: Systematic Review. JMIR Med. Inf. 2022, 10, e35724. [Google Scholar] [CrossRef]
- Pfaff, E.R.; Champion, J.; Bradford, R.L.; Clark, M.; Xu, H.; Fecho, K.; Krishnamurthy, A.; Cox, S.; Chute, C.G.; Overby Taylor, C.; et al. Fast Healthcare Interoperability Resources (FHIR) as a Meta Model to Integrate Common Data Models: Development of a Tool and Quantitative Validation Study. JMIR Med. Inf. 2019, 7, e15199. [Google Scholar] [CrossRef]
- Hylock, R.H.; Zeng, X. A Blockchain Framework for Patient-Centered Health Records and Exchange (HealthChain): Evaluation and Proof-of-Concept Study. J. Med. Internet Res. 2019, 21, e13592. [Google Scholar] [CrossRef] [PubMed]
- Bender, D.; Sartipi, K. HL7 FHIR: An Agile and RESTful approach to healthcare information exchange. In Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; IEEE: Piscataway, NJ, USA. [Google Scholar]
- Haase, K. Java Message Service API Tutorial; Sun Microsystems, Inc.: Santa Clara, CA, USA, 2002. [Google Scholar]
- World Health Organization. International Classification of Diseases (ICD). Available online: https://www.who.int/standards/classifications/classification-of-diseases (accessed on 20 March 2023).
- Juarez, J.M.; Riestra, T.; Campos, M.; Morales, A.; Palma, J.; Marin, R. Medical knowledge management for specific hospital departments. Expert Syst. Appl. 2009, 36, 12214–12224. [Google Scholar] [CrossRef]
- SNOMED CT. Systematized Nomenclature of Medicine Clinical Terms. Available online: https://www.snomed.org/ (accessed on 20 March 2023).
- Kasparick, M.; Andersen, B.; Franke, S.; Rockstroh, M.; Golatowski, F.; Timmermann, D.; Ingenerf, J.; Neumuth, T. Enabling artificial intelligence in high acuity medical environments. Minim. Invasive Ther. Allied Technol. 2019, 28, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Robb, L. Potential for Machine Learning in Burn Care. J. Burn. Care Res. 2022, 43, 632–639. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J.J.; Young, A.; Johnson, M.J.; Beattie, R.M. Using machine learning to impact on long-term clinical care: Principles, challenges, and practicalities. Pediatr. Res. 2023, 93, 324–333. [Google Scholar] [CrossRef]
- Feretzakis, G.; Karlis, G.; Loupelis, E.; Kalles, D.; Chatzikyriakou, R.; Trakas, N.; Karakou, E.; Sakagianni, A.; Tzelves, L.; Petropoulou, S.; et al. Using Machine Learning Techniques to Predict Hospital Admission at the Emergency Department. J. Crit. Care Med. (Targu Mures) 2022, 8, 107–116. [Google Scholar] [CrossRef]
- Chang, J.; Liu, Y.; Saey, S.A.; Chang, K.C.; Shrader, H.R.; Steckly, K.L.; Rajput, M.; Sonka, M.; Chan, C.H.F. Machine-learning based investigation of prognostic indicators for oncological outcome of pancreatic ductal adenocarcinoma. Front. Oncol. 2022, 12, 895515. [Google Scholar] [CrossRef]
- Miller, D.D.; Brown, E.W. Artificial Intelligence in Medical Practice: The Question to the Answer? Am. J. Med. 2018, 131, 129–133. [Google Scholar] [CrossRef]
- Beam, A.L.; Kohane, I.S. Translating Artificial Intelligence Into Clinical Care. JAMA 2016, 316, 2368–2369. [Google Scholar] [CrossRef]
- Tuegel, E.J.; Ingraffea, A.R.; Eason, T.G.; Spottswood, S.M. Reengineering Aircraft Structural Life Prediction Using a Digital Twin. Int. J. Aerosp. Eng. 2011, 2011, 154798. [Google Scholar] [CrossRef]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, G.; Koppius, O.R. Predictive analytics in information systems research. MIS Q. 2011, 35, 553–572. [Google Scholar] [CrossRef]
- Göbel, K.; Niessen, C.; Seufert, S.; Schmid, U. Explanatory machine learning for justified trust in human-AI collaboration: Experiments on file deletion recommendations. Front. Artif. Intell. 2022, 5, 919534. [Google Scholar] [CrossRef] [PubMed]
- Sievering, A.W.; Wohlmuth, P.; Geßler, N.; Gunawardene, M.A.; Herrlinger, K.; Bein, B.; Arnold, D.; Bergmann, M.; Nowak, L.; Gloeckner, C.; et al. Comparison of machine learning methods with logistic regression analysis in creating predictive models for risk of critical in-hospital events in COVID-19 patients on hospital admission. BMC Med. Inf. Decis. Mak. 2022, 22, 309. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Lin, H.; Yang, X.; Gong, J.; An, K.; Zheng, Z.; Hou, J. An In-Hospital Mortality Risk Model for Elderly Patients Undergoing Cardiac Valvular Surgery Based on LASSO-Logistic Regression and Machine Learning. J. Cardiovasc. Dev. Dis. 2023, 10, 87. [Google Scholar] [CrossRef] [PubMed]
- Aoki, S. BioRender. Available online: https://www.biorender.com (accessed on 5 April 2023).
- Pethani, F.; Dunn, A.G. Natural language processing for clinical notes in dentistry: A systematic review. J. Biomed. Inf. 2023, 138, 104282. [Google Scholar] [CrossRef]
- Clapp, M.A.; Kim, E.; James, K.E.; Perlis, R.H.; Kaimal, A.J.; McCoy, T.H., Jr. Natural language processing of admission notes to predict severe maternal morbidity during the delivery encounter. Am. J. Obs. Gynecol. 2022, 227, 511.e1–511.e18. [Google Scholar] [CrossRef]
- Abu-El-Rub, N.; Urbain, J.; Kowalski, G.; Osinski, K.; Spaniol, R.; Liu, M.; Taylor, B.; Waitman, L.R. Natural Language Processing for Enterprise-scale De-identification of Protected Health Information in Clinical Notes. AMIA Annu. Symp. Proc. 2022, 2022, 92–101. [Google Scholar]
- Rahman, M.; Nowakowski, S.; Agrawal, R.; Naik, A.; Sharafkhaneh, A.; Razjouyan, J. Validation of a Natural Language Processing Algorithm for the Extraction of the Sleep Parameters from the Polysomnography Reports. Healthcare 2022, 10, 1837. [Google Scholar] [CrossRef]
- Kimia, A.A.; Savova, G.; Landschaft, A.; Harper, M.B. An Introduction to Natural Language Processing: How You Can Get More From Those Electronic Notes You Are Generating. Pediatr. Emerg. Care 2015, 31, 536–541. [Google Scholar] [CrossRef]
- Liaw, W.; Kakadiaris, I. Artificial intelligence and family medicine: Better together. Fam. Med. 2020, 52, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Statsenko, Y.; Al Zahmi, F.; Habuza, T.; Almansoori, T.M.; Smetanina, D.; Simiyu, G.L.; Neidl-Van Gorkom, K.; Ljubisavljevic, M.; Awawdeh, R.; Elshekhali, H.; et al. Impact of Age and Sex on COVID-19 Severity Assessed From Radiologic and Clinical Findings. Front. Cell Infect. Microbiol. 2021, 11, 777070. [Google Scholar] [CrossRef] [PubMed]
- Bhanot, K.; Qi, M.; Erickson, J.S.; Guyon, I.; Bennett, K.P. The Problem of Fairness in Synthetic Healthcare Data. Entropy 2021, 23, 1165. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Study Design | Subjects | Outcome | HIE Network | FHIR Coding System | AI Model/Algorithms | Level of Implementation | Validation Method | Metric Score |
|---|---|---|---|---|---|---|---|---|---|
| Grinspan et al., 2015 [29] | Retrospective Cohort | 8041 Patients | Epilepsy | NYCLIX, Manhattan, US | ICD-9 | ML: LR, Lasso elastic LR, DT, RF, AdaBoost, CART, SVM | Prediction | Holdout | AUC: 78–88% Sensitivity: 12–30% PPV: 60–81% Calibration: 5–15% |
| Wang et al., 2015 [30] | Cohort | 18,295 Patients | CHF | HealthInfoNet, Maine, US | ICD-9-CM SNOMED CT | NLP: RF | Data Extraction Case Finding | Prospective Cohort Manual Review Mann–Whitney Test Cross-Validation | RC: Sensitivity: 69%, Specificity: 98.80%, PPV: 92%, NPV: 94.10%, F1: 78.90% PC: Sensitivity: 64%, Specificity: 98.80%, PPV: 91.40%, NPV: 93.20%, F1: 75.30% |
| Nguyen et al., 2015 [31] | Development and Evaluation | 500 Pathology Reports (201 notifiable cancer) | Notifiable Cancer | QCCAT, Queensland, Australia | SNOMED CT ICD-O | NLP: Medtex | Data Extraction | Manual Review | Recall: 78% Precision: 83% F-measure: 80% |
| Nguyen et al., 2016 [32] | Retrospective Observational | 45.3 M Pathology Reports (119,581 histology and cytology) | Notifiable Cancer | QCCAT, Queensland, Australia | SNOMED CT | NLP: Medtex | Data Extraction | Manual Review | Sensitivity: 96.50% Specificity: 96.50% PPV: 83.70% F1: 89.60% |
| Zheng et al., 2016 [33] | Cohort | 1.12 M patients (retrospective) 935,891 patients (prospective) | DM | HealthInfoNet, Maine, US | ICD-9-CM SNOMED CT | ML: RF NLP: DT | Data Extraction Case Finding | Manual Review Prospective Cohort | RC: Sensitivity 62%, Specificity 99.40%, PPV 95.40%, NPV 92.90% PC: Sensitivity 68%, Specificity 98.50%, PPV 90.10%, NPV 93.90% |
| Ye et al., 2018 [34] | Cohort | 823,627 Patients (retrospective) 680,810 Patients (prospective) | HTN | HealthInfoNet, Maine, US | ICD-9-CM ICD-10-CM | ML: XGBoost | Prediction | Prospective Cohort | RC: AUC 91.70% PC: AUC 87% |
| Vest et al., 2019 [35] | Retrospective Observational | 279,611 Patients | ED Visits | INPC, Indiana, US | N/A | ML: DT | Prediction | Holdout Cross-Validation | Travel SDOH: AUC 61% EHR with current visit data: AUC 69.60% EHR with Prior visit data: AUC of 70.70% HIE data: AUC of 71.30% All data: AUC 73.20% |
| Kasthurirathne et al., 2019 [36] | Retrospective Cohort | 84,317 Patients | Depression Advanced Care | INPC, Indiana, US | ICD-9 ICD-10 | ML: RF NLP | Data Extraction Prediction | Holdout | High-risk patients AUC: 86.31–94.43% Overall patient AUC: 78.87% Sensitivity: 68.79–83.91% Specificity:76.03–92.18% |
| Dexter et al., 2020 [37] | Retrospective Observational | 1.7 M Laboratory Reports | Syphilis Salmonella Histoplasmosis | INPC, Indiana, US | LOINC | ML: RF | Data Extraction Prediction | Holdout Laboratory-Level Holdout | Syphilis: AUC: 99.22%, Recall: 91%, Precision: 89%, F1: 90% Salmonella: AUC: 99.91%, Recall: 95%, Precision: 97%, F1: 96% Histoplasmosis: AUC: 99.18%, Recall: 96%, Precision: 88%, F1: 92% |
| Duong et al., 2021 [38] | Cohort | 497,470 Patients (retrospective) 521,347 Patients (prospective) | HF | HealthInfoNet, Maine, US | ICD9 ICD-10-CM | ML: XGBoost | Prediction | Prospective Cohort Cross-Validation | AUC: 82.40% (81.80–83%) Sensitivity: 29.20% Specificity: 97.10% PPV 10% NPV 99.20% |
| Kasturi et al., 2021 [39] | Retrospective Cohort | 96,026 Patients | Health Care Resource Utilization (COVID-19) | CoRDaCo, INPC, Indiana, US | N/A | ML: XGBoost | Prediction | Holdout | 1 Week: AUC: 88.74%, Sensitivity: 52.50%, Specificity: 95.78% 6 Weeks: AUC: 86.21%, Sensitivity: 52.57%, Specificity: 94.26% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borna, S.; Maniaci, M.J.; Haider, C.R.; Maita, K.C.; Torres-Guzman, R.A.; Avila, F.R.; Lunde, J.J.; Coffey, J.D.; Demaerschalk, B.M.; Forte, A.J. Artificial Intelligence Models in Health Information Exchange: A Systematic Review of Clinical Implications. Healthcare 2023, 11, 2584. https://doi.org/10.3390/healthcare11182584
Borna S, Maniaci MJ, Haider CR, Maita KC, Torres-Guzman RA, Avila FR, Lunde JJ, Coffey JD, Demaerschalk BM, Forte AJ. Artificial Intelligence Models in Health Information Exchange: A Systematic Review of Clinical Implications. Healthcare. 2023; 11(18):2584. https://doi.org/10.3390/healthcare11182584
Chicago/Turabian StyleBorna, Sahar, Michael J. Maniaci, Clifton R. Haider, Karla C. Maita, Ricardo A. Torres-Guzman, Francisco R. Avila, Julianne J. Lunde, Jordan D. Coffey, Bart M. Demaerschalk, and Antonio J. Forte. 2023. "Artificial Intelligence Models in Health Information Exchange: A Systematic Review of Clinical Implications" Healthcare 11, no. 18: 2584. https://doi.org/10.3390/healthcare11182584