
A Narrative Review on Multi-Domain Instrumental Approaches to Evaluate Neuromotor Function in Rehabilitation
 , , ,
, , ,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Methods: Rationale and Research Questions
3. Results
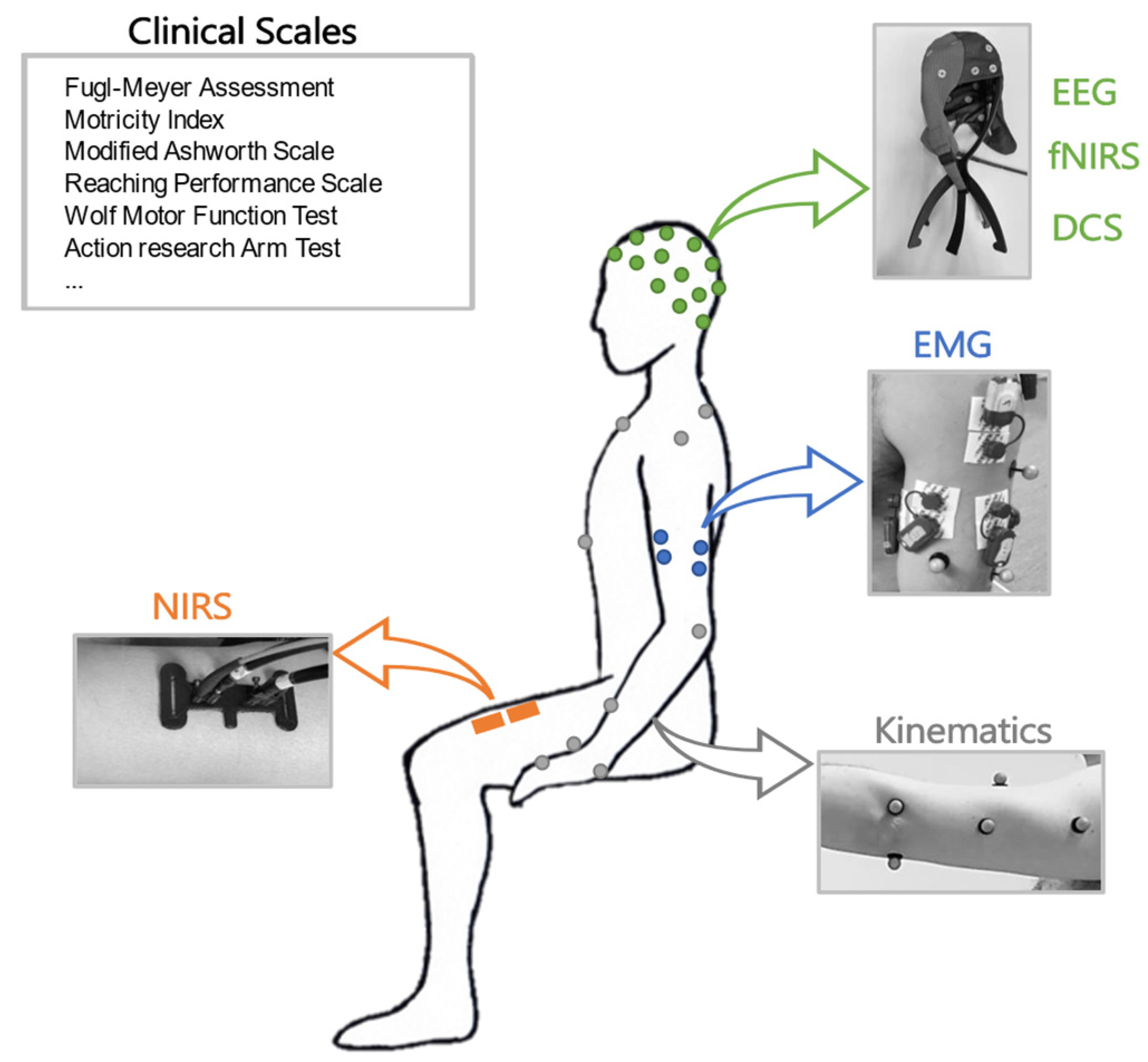
3.1. Summary of the Main Domains of Assessment and Main Achievements
3.1.1. Clinical Scales
3.1.2. Kinematics
3.1.3. EMG
Applications of EMG in Rehabilitation
3.1.4. EEG
Applications of EEG in Rehabilitation
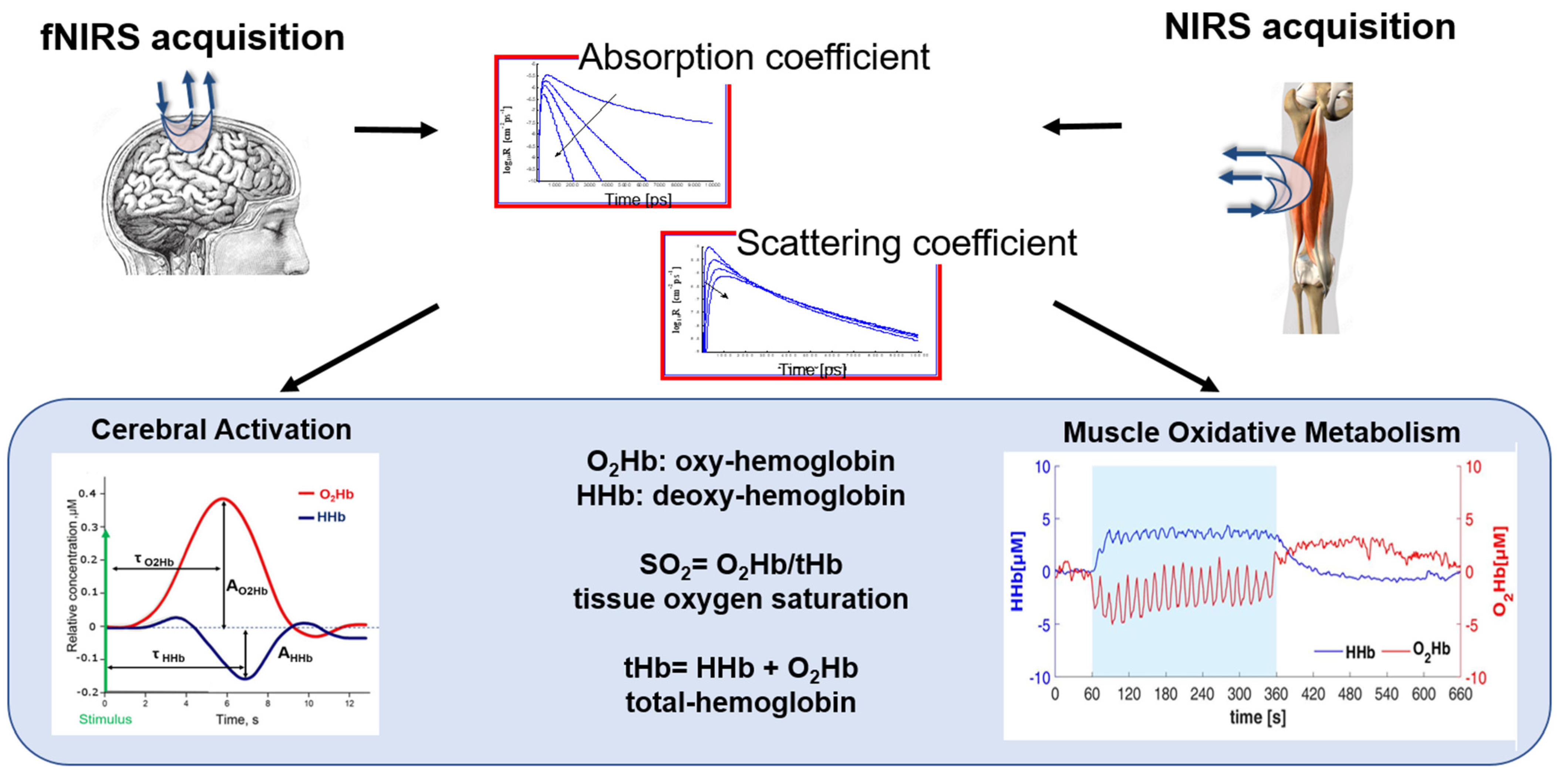
3.1.5. NIRS
Applications of NIRS in Rehabilitation (Brain)
Applications of NIRS in Rehabilitation (Skeletal Muscle)
3.2. Summary and Achievements of the Main Multi-Domain Instrumental Approaches
3.2.1. EEG + EMG
3.2.2. Kinematics + EMG
3.2.3. Kinematics + EEG
3.2.4. NIRS + EMG
3.2.5. fNIRS + EEG
3.2.6. fNIRS and NIRS + DCS
3.2.7. NIRS + Others
4. Discussion
4.1. Advantages of Multi-Domain Approaches
4.2. Disadvantages of Multi-Domain Approaches
4.3. Approaches to the Analysis of Multiple Domains in Clinical Practice
4.4. Clinical Adoption of Multi-Domain Approach: Future Perspective and Barriers
4.5. Future Research and Practice
- (i)
- Adopt standardized methods and criteria for selecting, combining, and analyzing multi-domain data to ensure the validity, reliability, and comparability of results across studies and settings [168]. To achieve this, it is necessary to match the study design with clinical needs in terms of setup complexity and time for preparation [163], and to define guidelines of good practice for all the combinations of assessments;
- (ii)
- Validate multi-domain approaches against gold-standard measures and clinical outcomes to establish their accuracy, sensitivity, and specificity for different patient populations and conditions;
- (iii)
- Integrate multi-domain approaches into clinical practice and research by developing user-friendly interfaces, protocols, and guidelines that facilitate their application and interpretation by clinicians and researchers. The comfort and psychological state of the patient has to be preserved, since the use of many sensors may interfere with the execution of tasks; thus, the sensors should be made less invasive. To foster the use of multi-domain approaches, instrumental measures and clinical observation must be linked so that clinicians may be more encouraged to apply multi-domain approaches and employ such techniques for evaluations and clinical decision-making. Clinicians or other professional figures have to be instructed on the use of the instrumentation and trained to interpret the results [167];
- (iv)
- Explore novel multi-domain combinations and methods that can capture more aspects of motor function and recovery, such as neural plasticity, muscle metabolism, or cognitive–motor interactions.
4.6. Messages Learnt
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Santisteban, L.; Térémetz, M.; Bleton, J.P.; Baron, J.C.; Maier, M.A.; Lindberg, P.G. Upper limb outcome measures used in stroke rehabilitation studies: A systematic literature review. PLoS ONE 2016, 11, e0154792. [Google Scholar] [CrossRef]
- Skorvanek, M.; Goldman, J.G.; Jahanshahi, M.; Marras, C.; Rektorova, I.; Schmand, B.; van Duijn, E.; Goetz, C.G.; Weintraub, D.; Stebbins, G.T.; et al. Global scales for cognitive screening in Parkinson’s disease: Critique and recommendations. Mov. Disord. 2018, 33, 208–218. [Google Scholar] [CrossRef]
- MacEira-Elvira, P.; Popa, T.; Schmid, A.C.; Hummel, F.C. Wearable technology in stroke rehabilitation: Towards improved diagnosis and treatment of upper-limb motor impairment. J. Neuroeng. Rehabil. 2019, 16, 142. [Google Scholar] [CrossRef]
- Lambercy, O.; Maggioni, S.; Lünenburger, L.; Gassert, R.; Bolliger, M. Robotic and wearable sensor technologies for measurements/clinical assessments. In Neurorehabilitation Technology, 2nd ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 183–207. ISBN 9783319286037. [Google Scholar]
- Fleury, L.; Koch, P.J.; Wessel, M.J.; Bonvin, C.; San Millan, D.; Constantin, C.; Vuadens, P.; Adolphsen, J.; Cadic Melchior, A.; Brügger, J.; et al. Toward individualized medicine in stroke-The TiMeS project: Protocol of longitudinal, multi-modal, multi-domain study in stroke. Front. Neurol. 2022, 13, 939640. [Google Scholar] [CrossRef]
- Levin, M.F.; Hiengkaew, V.; Nilanont, Y.; Cheung, D.; Dai, D.; Shaw, J.; Bayley, M.; Saposnik, G. Relationship between Clinical Measures of Upper Limb Movement Quality and Activity Poststroke. Neurorehabil. Neural Repair 2019, 33, 432–441. [Google Scholar] [CrossRef]
- Gao, Z.; Pang, Z.; Chen, Y.; Lei, G.; Zhu, S.; Li, G.; Shen, Y.; Xu, W. Restoring After Central Nervous System Injuries: Neural Mechanisms and Translational Applications of Motor Recovery. Neurosci. Bull. 2022, 38, 1569–1587. [Google Scholar] [CrossRef] [PubMed]
- Alt Murphy, M.; Resteghini, C.; Feys, P.; Lamers, I. An overview of systematic reviews on upper extremity outcome measures after stroke. BMC Neurol. 2015, 15, 29. [Google Scholar] [CrossRef] [Green Version]
- Velstra, I.M.; Ballert, C.S.; Cieza, A. A systematic literature review of outcome measures for upper extremity function using the international classification of functioning, disability, and health as reference. PM R 2011, 3, 846–860. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, A.A.; Seelen, H.A.; Willmann, R.D.; Kingma, H. Technology-assisted training of arm-hand skills in stroke: Concepts on reacquisition of motor control and therapist guidelines for rehabilitation technology design. J. Neuroeng. Rehabil. 2009, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemmens, R.J.M.; Timmermans, A.A.A.; Janssen-Potten, Y.J.M.; Smeets, R.J.E.M.; Seelen, H.A.M. Valid and reliable instruments for arm-hand assessment at ICF activity level in persons with hemiplegia: A systematic review. BMC Neurol. 2012, 12, 21. [Google Scholar] [CrossRef] [Green Version]
- Lang, C.E.; Bland, M.D.; Bailey, R.R.; Schaefer, S.Y.; Birkenmeier, R.L. Assessment of upper extremity impairment, function, and activity after stroke: Foundations for clinical decision making. J. Hand Ther. 2013, 26, 104–115. [Google Scholar] [CrossRef] [Green Version]
- Fugl Meyer, A.R.; Jaasko, L.; Leyman, I. The post stroke hemiplegic patient. I. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef]
- Wolf, S.L.; Lecraw, D.E.; Barton, L.A.; Jann, B.B. Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head-injured patients. Exp. Neurol. 1989, 104, 125–132. [Google Scholar] [CrossRef]
- Demers, M.; Levin, M.F. Do Activity Level Outcome Measures Commonly Used in Neurological Practice Assess Upper-Limb Movement Quality? Neurorehabil. Neural Repair 2017, 31, 623–637. [Google Scholar] [CrossRef] [Green Version]
- Gasperini, G.; Rota, M.; Guanziroli, E.; Bissolotti, L.; Balestrieri, F.; Chisari, C.; Currà, A.; Del Felice, A.; Farina, N.; Manganotti, P.; et al. Development and Rasch Validation of an Observational Assessment Tool of Upper Limb Functional Impairment in Stroke Survivors: Functional Assessment Test for Upper Limb. Arch. Phys. Med. Rehabil. 2022, 104, 597–604. [Google Scholar] [CrossRef]
- Kwakkel, G.; Lannin, N.A.; Borschmann, K.; English, C.; Ali, M.; Churilov, L.; Saposnik, G.; Winstein, C.; van Wegen, E.E.H.; Wolf, S.L.; et al. Standardized measurement of sensorimotor recovery in stroke trials: Consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2017, 12, 451–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veerbeek, J.M.; Kwakkel, G.; Van Wegen, E.E.H.; Ket, J.C.F.; Heymans, M.W. Early prediction of outcome of activities of daily living after stroke: A systematic review. Stroke 2011, 42, 1482–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alt Murphy, M.; Al-Shallawi, A.; Sunnerhagen, K.S.; Pandyan, A. Early prediction of upper limb functioning after stroke using clinical bedside assessments: A prospective longitudinal study. Sci. Rep. 2022, 12, 22053. [Google Scholar] [CrossRef] [PubMed]
- De Los Reyes-Guzmán, A.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Mazzoleni, S.; Do Tran, V.; Dario, P.; Posteraro, F. Wrist Robot-Assisted Rehabilitation Treatment in Subacute and Chronic Stroke Patients: From Distal-to-Proximal Motor Recovery. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1889–1896. [Google Scholar] [CrossRef]
- Van Dokkum, L.; Hauret, I.; Mottet, D.; Froger, J.; Métrot, J.; Laffont, I. The contribution of kinematics in the assessment of upper limb motor recovery early after stroke. Neurorehabil. Neural Repair 2014, 28, 4–12. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Burdet, E. A robust and sensitive metric for quantifying movement smoothness. IEEE Trans. Biomed. Eng. 2012, 59, 2126–2136. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.E.; Wagner, J.M.; Bastian, A.J.; Hu, Q.; Edwards, D.F.; Sahrmann, S.A.; Dromerick, A.W. Deficits in grasp versus reach during acute hemiparesis. Exp. Brain Res. 2005, 166, 126–136. [Google Scholar] [CrossRef]
- Hussain, N.; Alt Murphy, M.; Lundgren-Nilsson, Å.; Sunnerhagen, K.S. Relationship between self-reported and objectively measured manual ability varies during the first year post-stroke. Sci. Rep. 2020, 10, 5093. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, B.; Fasoli, S.; Krebs, H.I.; Hughes, R.; Volpe, B.; Frontera, W.R.; Stein, J.; Hogan, N. Movement smoothness changes during stroke recovery. J. Neurosci. 2002, 22, 8297–8304. [Google Scholar] [CrossRef] [PubMed]
- Palermo, E.; Hayes, D.R.; Russo, E.F.; Calabrò, R.S.; Pacilli, A.; Filoni, S. Translational effects of robot-mediated therapy in subacute stroke patients: An experimental evaluation of upper limb motor recovery. PeerJ 2018, 2018, e5544. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. Neuroeng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Maura, R.M.; Rueda Parra, S.; Stevens, R.E.; Weeks, D.L.; Wolbrecht, E.T.; Perry, J.C. Literature review of stroke assessment for upper-extremity physical function via EEG, EMG, kinematic, and kinetic measurements and their reliability. J. Neuroeng. Rehabil. 2023, 20, 21. [Google Scholar] [CrossRef]
- Drost, G.; Stegeman, D.F.; van Engelen, B.G.M.; Zwarts, M.J. Clinical applications of high-density surface EMG: A systematic review. J. Electromyogr. Kinesiol. 2006, 16, 586–602. [Google Scholar] [CrossRef]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG: An update. J. Appl. Physiol. 2014, 117, 1215–1230. [Google Scholar] [CrossRef] [Green Version]
- Thornton, R.C.; Michell, A.W. Techniques and applications of EMG: Measuring motor units from structure to function. J. Neurol. 2012, 259, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Bonato, P.; Catani, F.; D’Alessio, T.; Knaflitz, M.; Marcacci, M.; Simoncini, L. Myoelectric activation pattern during gait in total knee replacement: Relationship with kinematics, kinetics, and clinical outcome. IEEE Trans. Rehabil. Eng. 1999, 7, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Cheung, V.C.K.; D’Avella, A.; Bizzi, E. Adjustments of motor pattern for load compensation via modulated activations of muscle synergies during natural behaviors. J. Neurophysiol. 2009, 101, 1235–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bizzi, E.; Cheung, V.C.K.; D’Avella, A.; Saltiel, P.; Tresch, M. Combining modules for movement. Brain Res. Rev. 2008, 57, 125–133. [Google Scholar] [CrossRef] [Green Version]
- D’Avella, A.; Bizzi, E. Shared and specific muscle synergies in natural motor behaviors. Proc. Natl. Acad. Sci. USA 2005, 102, 3076–3081. [Google Scholar] [CrossRef] [PubMed]
- Cifrek, M.; Medved, V.; Tonković, S.; Ostojić, S. Surface EMG based muscle fatigue evaluation in biomechanics. Clin. Biomech. 2009, 24, 327–340. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Y.; Ma, A.; Ma, G.; Ye, Y.; Li, R.; Lu, T. A Comparative Study of EMG Indices in Muscle Fatigue Evaluation Based on Grey Relational Analysis during All-Out Cycling Exercise. Biomed Res. Int. 2018, 2018, 9341215. [Google Scholar] [CrossRef] [Green Version]
- Al-Mulla, M.R.; Sepulveda, F.; Colley, M. A review of non-invasive techniques to detect and predict localised muscle fatigue. Sensors 2011, 11, 3545–3594. [Google Scholar] [CrossRef] [Green Version]
- Farina, D.; Merletti, R.; Enoka, R.M. The extraction of neural strategies from the surface EMG. J. Appl. Physiol. 2004, 96, 1486–1495. [Google Scholar] [CrossRef] [Green Version]
- Stegeman, D.F.; Blok, J.H.; Hermens, H.J.; Roeleveld, K. Surface EMG models: Properties and applications. J. Electromyogr. Kinesiol. 2000, 10, 313–326. [Google Scholar] [CrossRef]
- Chowdhury, R.H.; Reaz, M.B.I.; Bin Mohd Ali, M.A.; Bakar, A.A.A.; Chellappan, K.; Chang, T.G. Surface electromyography signal processing and classification techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef] [Green Version]
- Campanini, I.; Disselhorst-Klug, C.; Rymer, W.Z.; Merletti, R. Surface EMG in Clinical Assessment and Neurorehabilitation: Barriers Limiting Its Use. Front. Neurol. 2020, 11, 934. [Google Scholar] [CrossRef]
- Patten, C.; Lexell, J.; Brown, H.E. Weakness and strength training in persons with poststroke hemiplegia: Rationale, method, and efficacy. J. Rehabil. Res. Dev. 2004, 41, 293–312. [Google Scholar] [CrossRef]
- MG, B.; DJ, C.; SA, K. Evaluation of abnormal synergy patterns poststroke: Relationship of the Fugl-Meyer Assessment to hemiparetic locomotion. Neurorehabil. Neural Repair 2010, 24, 328–337. [Google Scholar] [CrossRef]
- Cheung, V.C.K.; Turolla, A.; Agostini, M.; Silvoni, S.; Bennis, C.; Kasi, P.; Paganoni, S.; Bonato, P.; Bizzi, E. Muscle synergy patterns as physiological markers of motor cortical damage. Proc. Natl. Acad. Sci. USA 2012, 109, 14652–14656. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, K.; Hayashi, Y. An EMG-based control for an upper-limb power-assist exoskeleton robot. IEEE Trans. Syst. Man, Cybern. Part B Cybern. 2012, 42, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Scheme, E.; Englehart, K. Electromyogram pattern recognition for control of powered upper-limb prostheses: State of the art and challenges for clinical use. J. Rehabil. Res. Dev. 2011, 48, 643–660. [Google Scholar] [CrossRef]
- McDonald, A.C.; Mulla, D.M.; Keir, P.J. Using EMG Amplitude and Frequency to Calculate a Multimuscle Fatigue Score and Evaluate Global Shoulder Fatigue. Hum. Factors 2019, 61, 526–536. [Google Scholar] [CrossRef]
- Scano, A.; Re, R.; Tomba, A.; Amata, O.; Pirovano, I.; Brambilla, C.; Contini, D.; Spinelli, L.; Amendola, C.; Caserta, A.V.; et al. Non-Surgical Lower-Limb Rehabilitation Enhances Quadriceps Strength in Inpatients with Hip Fracture : A Study on Force Capacity and Fatigue. Appl. Sci. 2023, 13, 6855. [Google Scholar] [CrossRef]
- Nunez, P.L.; Srinivasan, R. Electric Fields of the Brain: The neurophysics of EEG; Oxford University Press: Oxford, UK, 2009; ISBN 9780199865673. [Google Scholar]
- Teplan, M. Fundamentals of EEG measurement. Meas. Sci. Rev. 2002, 2, 1–11. [Google Scholar]
- Seeber, M.; Cantonas, L.M.; Hoevels, M.; Sesia, T.; Visser-Vandewalle, V.; Michel, C.M. Subcortical electrophysiological activity is detectable with high-density EEG source imaging. Nat. Commun. 2019, 10, 753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friston, K.J. Functional and Effective Connectivity: A Review. Brain Connect. 2011, 1, 13–36. [Google Scholar] [CrossRef]
- Pereda, E.; Quiroga, R.Q.; Bhattacharya, J. Nonlinear multivariate analysis of neurophysiological signals. Prog. Neurobiol. 2005, 77, 1–37. [Google Scholar] [CrossRef] [Green Version]
- Blinowska, K.J. Review of the methods of determination of directed connectivity from multichannel data. Med. Biol. Eng. Comput. 2011, 49, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Stinear, C.M. Prediction of motor recovery after stroke: Advances in biomarkers. Lancet. Neurol. 2017, 16, 826–836. [Google Scholar] [CrossRef]
- Finnigan, S.P.; Walsh, M.; Rose, S.E.; Chalk, J.B. Quantitative EEG indices of sub-acute ischaemic stroke correlate with clinical outcomes. Clin. Neurophysiol. 2007, 118, 2525–2532. [Google Scholar] [CrossRef]
- Trujillo, P.; Mastropietro, A.; Scano, A.; Chiavenna, A.; Mrakic-Sposta, S.; Caimmi, M.; Molteni, F.; Rizzo, G. Quantitative EEG for predicting upper limb motor recovery in chronic stroke robot-Assisted rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 27, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Meng, L.; Pang, J.; Zhu, X.; Ming, D. Characterization of EEG Data Revealing Relationships with Cognitive and Motor Symptoms in Parkinson’s Disease: A Systematic Review. Front. Aging Neurosci. 2020, 12, 373. [Google Scholar] [CrossRef]
- Reid, L.B.; Rose, S.E.; Boyd, R.N. Rehabilitation and neuroplasticity in children with unilateral cerebral palsy. Nat. Rev. Neurol. 2015, 11, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Piazza, C.; Pirovano, I.; Mastropietro, A.; Genova, C.; Gagliardi, C.; Turconi, A.C.; Malerba, G.; Panzeri, D.; Maghini, C.; Reni, G.; et al. Development and preliminary testing of a system for the multimodal analysis of gait training in a virtual reality environment. Electronics 2021, 10, 2838. [Google Scholar] [CrossRef]
- Simis, M.; Doruk Camsari, D.; Imamura, M.; Filippo, T.R.M.; Rubio De Souza, D.; Battistella, L.R.; Fregni, F. Electroencephalography as a Biomarker for Functional Recovery in Spinal Cord Injury Patients. Front. Hum. Neurosci. 2021, 15, 179. [Google Scholar] [CrossRef]
- De Vico Fallani, F.; Sinatra, R.; Astolfi, L.; Mattia, D.; Cincotti, F.; Latora, V.; Salinari, S.; Marciani, M.G.; Colosimo, A.; Babiloni, F. Community structure of cortical networks in spinal cord injured patients. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS’08—“Personalized Healthcare through Technology”, Vancouver, Canada, 20–25 August 2008; Volume 2008, pp. 3995–3998. [Google Scholar]
- Irimia, A.; Van Horn, J.D. Functional neuroimaging of traumatic brain injury: Advances and clinical utility. Neuropsychiatr. Dis. Treat. 2015, 11, 2355–2365. [Google Scholar] [CrossRef] [Green Version]
- Bistriceanu, C.E.; Danciu, F.A.; Cuciureanu, D.I. Cortical connectivity in stroke using signals from resting-state EEG: A review of current literature. Acta Neurol. Belg. 2022, 123, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Hordacre, B.; Goldsworthy, M.R.; Welsby, E.; Graetz, L.; Ballinger, S.; Hillier, S. Resting State Functional Connectivity Is Associated with Motor Pathway Integrity and Upper-Limb Behavior in Chronic Stroke. Neurorehabil. Neural Repair 2020, 34, 547–557. [Google Scholar] [CrossRef]
- De Vico Fallani, F.; Clausi, S.; Leggio, M.; Chavez, M.; Valencia, M.; Maglione, A.G.; Babiloni, F.; Cincotti, F.; Mattia, D.; Molinari, M. Interhemispheric Connectivity Characterizes Cortical Reorganization in Motor-Related Networks After Cerebellar Lesions. Cerebellum 2017, 16, 358–375. [Google Scholar] [CrossRef]
- Hoshino, T.; Oguchi, K.; Inoue, K.; Hoshino, A.; Hoshiyama, M. Relationship between lower limb function and functional connectivity assessed by EEG among motor-related areas after stroke. Top. Stroke Rehabil. 2021, 28, 614–623. [Google Scholar] [CrossRef] [PubMed]
- De Vico Fallani, F.; Astolfi, L.; Cincotti, F.; Mattia, D.; La Rocca, D.; Maksuti, E.; Salinari, S.; Babiloni, F.; Vegso, B.; Kozmann, G.; et al. Evaluation of the brain network organization from EEG signals: A preliminary evidence in stroke patient. Anat. Rec. 2009, 292, 2023–2031. [Google Scholar] [CrossRef]
- Wang, X.; Wong, W.W.; Sun, R.; Chu, W.C.W.; Tong, K.Y. Differentiated effects of robot hand training with and without neural guidance on neuroplasticity patterns in chronic stroke. Front. Neurol. 2018, 9, 810. [Google Scholar] [CrossRef] [Green Version]
- Samogin, J.; Marino, M.; Porcaro, C.; Wenderoth, N.; Dupont, P.; Swinnen, S.P.; Mantini, D. Frequency-dependent functional connectivity in resting state networks. Hum. Brain Mapp. 2020, 41, 5187–5198. [Google Scholar] [CrossRef] [PubMed]
- Romeo, Z.; Mantini, D.; Durgoni, E.; Passarini, L.; Meneghello, F.; Zorzi, M. Electrophysiological signatures of resting state networks predict cognitive deficits in stroke. Cortex 2021, 138, 59–71. [Google Scholar] [CrossRef]
- Caliandro, P.; Vecchio, F.; Miraglia, F.; Reale, G.; Della Marca, G.; La Torre, G.; Lacidogna, G.; Iacovelli, C.; Padua, L.; Bramanti, P.; et al. Small-World Characteristics of Cortical Connectivity Changes in Acute Stroke. Neurorehabil. Neural Repair 2017, 31, 81–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vecchio, F.; Caliandro, P.; Reale, G.; Miraglia, F.; Piludu, F.; Masi, G.; Iacovelli, C.; Simbolotti, C.; Padua, L.; Leone, E.; et al. Acute cerebellar stroke and middle cerebral artery stroke exert distinctive modifications on functional cortical connectivity: A comparative study via EEG graph theory. Clin. Neurophysiol. 2019, 130, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Tomino, C.; Miraglia, F.; Iodice, F.; Erra, C.; Di Iorio, R.; Judica, E.; Alù, F.; Fini, M.; Rossini, P.M. Cortical connectivity from EEG data in acute stroke: A study via graph theory as a potential biomarker for functional recovery. Int. J. Psychophysiol. 2019, 146, 133–138. [Google Scholar] [CrossRef]
- Nicolo, P.; Magnin, C.; Pedrazzini, E.; Plomp, G.; Mottaz, A.; Schnider, A.; Guggisberg, A.G. Comparison of Neuroplastic Responses to Cathodal Transcranial Direct Current Stimulation and Continuous Theta Burst Stimulation in Subacute Stroke. Arch. Phys. Med. Rehabil. 2018, 99, 862–872.e1. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Formaggio, E.; Bosco, A.; Guanziroli, E.; Piccione, F.; Masiero, S.; Del Felice, A. Brain Connectivity Modulation after Exoskeleton-Assisted Gait in Chronic Hemiplegic Stroke Survivors: A Pilot Study. Am. J. Phys. Med. Rehabil. 2020, 99, 694–700. [Google Scholar] [CrossRef]
- Maggio, M.G.; Naro, A.; Manuli, A.; Maresca, G.; Balletta, T.; Latella, D.; De Luca, R.; Calabrò, R.S. Effects of Robotic Neurorehabilitation on Body Representation in Individuals with Stroke: A Preliminary Study Focusing on an EEG-Based Approach. Brain Topogr. 2021, 34, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Pichiorri, F.; Petti, M.; Caschera, S.; Astolfi, L.; Cincotti, F.; Mattia, D. An EEG index of sensorimotor interhemispheric coupling after unilateral stroke: Clinical and neurophysiological study. Eur. J. Neurosci. 2018, 47, 158–163. [Google Scholar] [CrossRef]
- Fanciullacci, C.; Panarese, A.; Spina, V.; Lassi, M.; Mazzoni, A.; Artoni, F.; Micera, S.; Chisari, C. Connectivity Measures Differentiate Cortical and Subcortical Sub-Acute Ischemic Stroke Patients. Front. Hum. Neurosci. 2021, 15, 368. [Google Scholar] [CrossRef]
- Park, C.H.; Chang, W.H.; Ohn, S.H.; Kim, S.T.; Bang, O.Y.; Pascual-Leone, A.; Kim, Y.H. Longitudinal changes of resting-state functional connectivity during motor recovery after stroke. Stroke 2011, 42, 1357–1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirovano, I.; Mastropietro, A.; Antonacci, Y.; Barà, C.; Guanziroli, E.; Molteni, F.; Faes, L.; Rizzo, G. Resting State EEG Directed Functional Connectivity Unveils Changes in Motor Network Organization in Subacute Stroke Patients After Rehabilitation. Front. Physiol. 2022, 13, 591. [Google Scholar] [CrossRef]
- Wu, J.; Quinlan, E.B.; Dodakian, L.; McKenzie, A.; Kathuria, N.; Zhou, R.J.; Augsburger, R.; See, J.; Le, V.H.; Srinivasan, R.; et al. Connectivity measures are robust biomarkers of cortical function and plasticity after stroke. Brain 2015, 138, 2359–2369. [Google Scholar] [CrossRef] [Green Version]
- Philips, G.R.; Daly, J.J.; Príncipe, J.C. Topographical measures of functional connectivity as biomarkers for post-stroke motor recovery. J. Neuroeng. Rehabil. 2017, 14, 67. [Google Scholar] [CrossRef]
- Asadi, B.; Cuenca-Zaldivar, J.N.; Nakhostin Ansari, N.; Ibáñez, J.; Herrero, P.; Calvo, S. Brain Analysis with a Complex Network Approach in Stroke Patients Based on Electroencephalography: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 666. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, V.; Ferrari, M. A Mini-Review on Functional Near-Infrared Spectroscopy (fNIRS): Where Do We Stand, and Where Should We Go? Photonics 2019, 6, 87. [Google Scholar] [CrossRef] [Green Version]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016, 21, 091313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85 Pt 1, 6–27. [Google Scholar] [CrossRef]
- Torricelli, A.; Contini, D.; Pifferi, A.; Caffini, M.; Re, R.; Zucchelli, L.; Spinelli, L. Time domain functional NIRS imaging for human brain mapping. Neuroimage 2014, 85 Pt 1, 28–50. [Google Scholar] [CrossRef] [Green Version]
- Durduran, T.; Yodh, A.G. Diffuse correlation spectroscopy for non-invasive, micro-vascular cerebral blood flow measurement. Neuroimage 2014, 85, 51. [Google Scholar] [CrossRef] [Green Version]
- Giacalone, G.; Zanoletti, M.; Re, R.; Germinario, B.; Contini, D.; Spinelli, L.; Torricelli, A.; Roveri, L. Time-domain near-infrared spectroscopy in acute ischemic stroke patients. Neurophotonics 2019, 6, 1. [Google Scholar] [CrossRef]
- Roldán, M.; Kyriacou, P.A. Near-infrared spectroscopy (NIRS) in traumatic brain injury (TBI). Sensors 2021, 21, 1586. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, K.; Currim, F.; Lindberg, C.M.; Razjouyan, J.; Gilligan, B.; Lee, H.; Canada, K.J.; Goebel, N.; Mehl, M.R.; Lunden, M.M.; et al. Discovery of associative patterns between workplace sound level and physiological wellbeing using wearable devices and empirical Bayes modeling. npj Digit. Med. 2023, 6, 5. [Google Scholar] [CrossRef]
- Thewissen, L.; Caicedo, A.; Lemmers, P.; Van Bel, F.V.; Van Huffel, S.V.; Naulaers, G. Measuring near-infrared spectroscopy derived cerebral autoregulation in neonates: From research tool toward bedside multimodal monitoring. Front. Pediatr. 2018, 6, 117. [Google Scholar] [CrossRef] [PubMed]
- Mihara, M.; Miyai, I. Review of functional near-infrared spectroscopy in neurorehabilitation. Neurophotonics 2016, 3, 031414. [Google Scholar] [CrossRef]
- Lin, J.H.; Maikala, R.V.; McGorry, R.; Brunette, C. NIRS application in evaluating threaded-fastener driving assembly tasks. Int. J. Ind. Ergon. 2010, 40, 146–152. [Google Scholar] [CrossRef]
- Bonnal, J.; Monnet, F.; Le, B.T.; Pila, O.; Grosmaire, A.G.; Ozsancak, C.; Duret, C.; Auzou, P. Relation between Cortical Activation and Effort during Robot-Mediated Walking in Healthy People: A Functional Near-Infrared Spectroscopy Neuroimaging Study (fNIRS). Sensors 2022, 22, 5542. [Google Scholar] [CrossRef]
- Lacerenza, M.; Spinelli, L.; Buttafava, M.; Dalla Mora, A.; Zappa, F.; Pifferi, A.; Tosi, A.; Cozzi, B.; Torricelli, A.; Contini, D. Monitoring the motor cortex hemodynamic response function in freely moving walking subjects: A time-domain fNIRS pilot study. Neurophotonics 2021, 8, 015006. [Google Scholar] [CrossRef]
- Xie, F.; Huang, S.; Miao, T.; He, S.; Lin, Z.; Xie, L. Development of a Wireless Multichannel Near-Infrared Spectroscopy Sensor System for Monitoring Muscle Activity. IEEE Sens. J. 2022, 22, 22714–22724. [Google Scholar] [CrossRef]
- Scholkmann, F.; Tachtsidis, I.; Wolf, M.; Wolf, U. Systemic physiology augmented functional near-infrared spectroscopy: A powerful approach to study the embodied human brain. Neurophotonics 2022, 9, 030801. [Google Scholar] [CrossRef]
- Barstow, T.J. Understanding near infrared spectroscopy and its application to skeletal muscle research. J. Appl. Physiol. 2019, 126, 1360–1376. [Google Scholar] [CrossRef]
- Tuesta, M.; Yáñez-Sepúlveda, R.; Verdugo-Marchese, H.; Mateluna, C.; Alvear-Ordenes, I. Near-Infrared Spectroscopy Used to Assess Physiological Muscle Adaptations in Exercise Clinical Trials: A Systematic Review. Biology 2022, 11, 1073. [Google Scholar] [CrossRef]
- Adami, A.; Rossiter, H.B. Principles, insights, and potential pitfalls of the noninvasive determination of muscle oxidative capacity by near-infrared spectroscopy. J. Appl. Physiol. 2018, 124, 245–248. [Google Scholar] [CrossRef] [Green Version]
- Wȩgrzynowska-Teodorczyk, K.; Siennicka, A.; Josiak, K.; Zymliński, R.; Kasztura, M.; Banasiak, W.; Ponikowski, P.; Woźniewski, M. Evaluation of Skeletal Muscle Function and Effects of Early Rehabilitation during Acute Heart Failure: Rationale and Study Design. Biomed Res. Int. 2018, 2018, 6982897. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, F.; Lamberti, N.; Ficarra, V.; Tsolaki, E.; Straudi, S.; Zamboni, P.; Basaglia, N.; Gasbarro, V. Biomarkers of muscle metabolism in peripheral artery disease: A dynamic NIRS-assisted study to detect adaptations following revascularization and exercise training. Diagnostics 2020, 10, 312. [Google Scholar] [CrossRef]
- Soares, R.N.; Murias, J.M.; Saccone, F.; Puga, L.; Moreno, G.; Resnik, M.; De Roia, G.F. Effects of a rehabilitation program on microvascular function of CHD patients assessed by near-infrared spectroscopy. Physiol. Rep. 2019, 7, e14145. [Google Scholar] [CrossRef] [Green Version]
- Ferrante, J.M.; Piasecki, A.K.; Ohman-Strickland, P.A.; Crabtree, B.F. Family physicians’ practices and attitudes regarding care of extremely obese patients. Obesity 2009, 17, 1710–1716. [Google Scholar] [CrossRef]
- Brambilla, C.; Pirovano, I.; Mira, R.M.; Rizzo, G.; Scano, A.; Mastropietro, A. Combined use of emg and eeg techniques for neuromotor assessment in rehabilitative applications: A systematic review. Sensors 2021, 21, 7014. [Google Scholar] [CrossRef]
- Liu, J.; Sheng, Y.; Liu, H. Corticomuscular coherence and its applications: A review. Front. Hum. Neurosci. 2019, 13, 100. [Google Scholar] [CrossRef] [Green Version]
- von Carlowitz-Ghori, K.; Bayraktaroglu, Z.; Hohlefeld, F.U.; Losch, F.; Curio, G.; Nikulin, V.V. Corticomuscular coherence in acute and chronic stroke. Clin. Neurophysiol. 2014, 125, 1182–1191. [Google Scholar] [CrossRef]
- Pan, L.L.H.; Yang, W.W.; Kao, C.L.; Tsai, M.W.; Wei, S.H.; Fregni, F.; Chen, V.C.F.; Chou, L.W. Effects of 8-week sensory electrical stimulation combined with motor training on EEG-EMG coherence and motor function in individuals with stroke. Sci. Rep. 2018, 8, 9217. [Google Scholar] [CrossRef] [Green Version]
- Calabrò, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Simori, G.; Banica, A.; Brusturean, E.; Burz, A.; Craciunas, R.; Ulinici, I.; et al. The impact of robotic rehabilitation on the motor system in neurological diseases. A multimodal neurophysiological approach. Int. J. Environ. Res. Public Health 2020, 17, 6557. [Google Scholar] [CrossRef]
- Kim, B.; Kim, L.; Kim, Y.H.; Yoo, S.K. Cross-association analysis of EEG and EMG signals according to movement intention state. Cogn. Syst. Res. 2017, 44, 1–9. [Google Scholar] [CrossRef]
- Bao, S.C.; Wong, W.W.; Leung, T.W.H.; Tong, K.Y. Cortico-Muscular Coherence Modulated by High-Definition Transcranial Direct Current Stimulation in People with Chronic Stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 304–313. [Google Scholar] [CrossRef]
- Yang, H.; Wan, J.; Jin, Y.; Yu, X.; Fang, Y. EEG- and EMG-Driven Poststroke Rehabilitation: A Review. IEEE Sens. J. 2022, 22, 23649–23660. [Google Scholar] [CrossRef]
- D’Addio, G.; Cesarelli, M.; Romano, M.; Faiella, G.; Lullo, F.; Pappone, N. Kinematic and EMG patterns evaluation of upper arm reaching movements. In Proceedings of the IEEE RAS and EMBS International Conference on Biomedical Robotics and Biomechatronics, Rome, Italy, 24–27 June 2012; pp. 1383–1387. [Google Scholar]
- Kim, J.; Kim, H.; Kim, J. Quantitative assessment test for upper-limb motor function by using EMG and kinematic analysis in the practice of occupational therapy. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Jeju, Republic of Korea, 11–15 July 2017; Volume 2017, pp. 1158–1161. [Google Scholar]
- De Marchis, C.; Patané, F.; Petrarca, M.; Carniel, S.; Schmid, M.; Conforto, S.; Castelli, E.; Cappa, P.; D’Alessio, T. EMG and kinematics assessment of postural responses during balance perturbation on a 3D robotic platform: Preliminary results in children with hemiplegia. In XIII Mediterranean Conference on Medical and Biological Engineering and Computing; IFMBE Proceedings Series; Springer: Seville, Spain, 2014; Volume 41, pp. 69–72. [Google Scholar]
- Zhang, X.; Tang, X.; Zhu, X.; Gao, X.; Chen, X.; Chen, X. A regression-based framework for quantitative assessment of muscle spasticity using combined emg and inertial data from wearable sensors. Front. Neurosci. 2019, 13, 398. [Google Scholar] [CrossRef] [Green Version]
- Campanini, I.; Cosma, M.; Manca, M.; Merlo, A. Added Value of Dynamic EMG in the Assessment of the Equinus and the Equinovarus Foot Deviation in Stroke Patients and Barriers Limiting Its Usage. Front. Neurol. 2020, 11, 583399. [Google Scholar] [CrossRef]
- Scano, A.; Mira, R.M.; D’Avella, A. Mixed matrix factorization: A novel algorithm for the extraction of kinematic-muscular synergies. J. Neurophysiol. 2022, 127, 529–547. [Google Scholar] [CrossRef]
- Mazzoleni, S.; Coscia, M.; Rossi, G.; Aliboni, S.; Posteraro, F.; Carrozza, M.C. Effects of an upper limb robot-mediated therapy on paretic upper limb in chronic hemiparetic subjects: A biomechanical and EEG-based approach for functional assessment. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, ICORR 2009, Kyoto, Japan, 23–26 June 2009; pp. 92–97. [Google Scholar]
- Comani, S.; Schinaia, L.; Tamburro, G.; Velluto, L.; Sorbi, S.; Conforto, S.; Guarnieri, B. Assessing neuro-motor recovery in a stroke survivor with high-resolution EEG, robotics and Virtual Reality. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Milan, Italy, 25–29 August 2015; Volume 2015, pp. 3925–3928. [Google Scholar]
- Molteni, E.; Preatoni, E.; Cimolin, V.; Bianchi, A.M.; Galli, M.; Rodano, R. A methodological study for the multifactorial assessment of Motor Adaptation: Integration of kinematic and neural factors. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC’10, Buenos Aires, Argentina, 31 August–4 September 2010; Volume 2010, pp. 4910–4913. [Google Scholar]
- Caimmi, M.; Visani, E.; Digiacomo, F.; Scano, A.; Chiavenna, A.; Gramigna, C.; Molinari Tosatti, L.; Franceschetti, S.; Molteni, F.; Panzica, F. Predicting Functional Recovery in Chronic Stroke Rehabilitation Using Event-Related Desynchronization-Synchronization during Robot-Assisted Movement. Biomed Res. Int. 2016, 2016, 7051340. [Google Scholar] [CrossRef]
- Belfatto, A.; Scano, A.; Chiavenna, A.; Mastropietro, A.; Mrakic-Sposta, S.; Pittaccio, S.; Tosatti, L.M.; Molteni, F.; Rizzo, G. A multiparameter approach to evaluate post-stroke patients: An application on robotic rehabilitation. Appl. Sci. 2018, 8, 2248. [Google Scholar] [CrossRef] [Green Version]
- Pierella, C.; Pirondini, E.; Kinany, N.; Coscia, M.; Giang, C.; Miehlbradt, J.; Magnin, C.; Nicolo, P.; Dalise, S.; Sgherri, G.; et al. A multimodal approach to capture post-stroke temporal dynamics of recovery. J. Neural Eng. 2020, 17, 045002. [Google Scholar] [CrossRef]
- Scano, A.; Zanoletti, M.; Pirovano, I.; Spinelli, L.; Contini, D.; Torricelli, A.; Re, R. NIRS-EMG for clinical applications: A systematic review. Appl. Sci. 2019, 9, 2952. [Google Scholar] [CrossRef] [Green Version]
- Taelman, J.; Vanderhaegen, J.; Robijns, M.; Naulaers, G.; Spaepen, A.; Huffel, S. Van Estimation of Muscle Fatigue Using Surface Electromyography and Near-Infrared Spectroscopy. Adv. Exp. Med. Biol. 2011, 701, 353–359. [Google Scholar] [CrossRef]
- Scano, A.; Pirovano, I.; Manunza, M.E.; Spinelli, L.; Contini, D.; Torricelli, A.; Re, R. Sustained fatigue assessment during isometric exercises with time-domain near infrared spectroscopy and surface electromyography signals. Biomed. Opt. Express 2020, 11, 7357. [Google Scholar] [CrossRef]
- Re, R.; Scano, A.; Pirovano, I.; Manunza, M.E.; Spinelli, L.; Contini, D.; Torricelli, A. Assessment of muscular sustained fatigue: A TD-NIRS and sEMG study. In Proceedings of the Optics InfoBase Conference Papers; Optica Publishing Group: Munich, Germany, 2021; p. ETu4A.6. [Google Scholar]
- Kankaanpää, M.; Colier, W.N.; Taimela, S.; Anders, C.; Airaksinen, O.; Kokko-Aro, S.M.; Hänninen, O. Back extensor muscle oxygenation and fatigability in healthy subjects and low back pain patients during dynamic back extension exertion. Pathophysiology 2005, 12, 267–273. [Google Scholar] [CrossRef]
- Søgaard, K.; Blangsted, A.K.; Nielsen, P.K.; Hansen, L.; Andersen, L.L.; Vedsted, P.; Sjøgaard, G. Changed activation, oxygenation, and pain response of chronically painful muscles to repetitive work after training interventions: A randomized controlled trial. Eur. J. Appl. Physiol. 2012, 112, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jigjid, E.; Kawashima, N.; Ogata, H.; Nakazawa, K.; Akai, M.; Eto, F.; Haga, N. Effects of passive leg movement on the oxygenation level of lower limb muscle in chronic stroke patients. Neurorehabil. Neural Repair 2008, 22, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, N.; Nakazawa, K.; Akai, M. Muscle oxygenation of the paralyzed lower limb in spinal cord-injured persons. Med. Sci. Sports Exerc. 2005, 37, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.; Keyser, R.E.; Chin, L.M.K.; Bulea, T.C.; Wutzke, C.J.; Guccione, A.A. EMG median frequency shifts without change in muscle oxygenation following novel locomotor training in individuals with incomplete spinal cord injury. Disabil. Rehabil. 2022, 44, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Chiarelli, A.M.; Zappasodi, F.; Di Pompeo, F.; Merla, A. Simultaneous functional near-infrared spectroscopy and electroencephalography for monitoring of human brain activity and oxygenation: A review. Neurophotonics 2017, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Mora, D.A.; Almeida, Y.; Vieira, C.; Badia, S.B.I. A study on EEG power and connectivity in a virtual reality bimanual rehabilitation training system. In Proceedings of the Conference Proceedings—IEEE International Conference on Systems, Man and Cybernetics; Institute of Electrical and Electronics Engineers Inc.: Bari, Italy, 2019; Volume 2019-October, pp. 2818–2822. [Google Scholar]
- Li, J.; Thakor, N.; Bezerianos, A. Brain Functional Connectivity in Unconstrained Walking with and without an Exoskeleton. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 730–739. [Google Scholar] [CrossRef]
- Abtahi, M.; Bahram Borgheai, S.; Jafari, R.; Constant, N.; Diouf, R.; Shahriari, Y.; Mankodiya, K. Merging fNIRS-EEG Brain Monitoring and Body Motion Capture to Distinguish Parkinsons Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1246–1253. [Google Scholar] [CrossRef]
- Dutta, A.; Jacob, A.; Chowdhury, S.R.; Das, A.; Nitsche, M.A. EEG-NIRS Based Assessment of Neurovascular Coupling During Anodal Transcranial Direct Current Stimulation—A Stroke Case Series. J. Med. Syst. 2015, 39, 36. [Google Scholar] [CrossRef]
- Jindal, U.; Sood, M.; Dutta, A.; Chowdhury, S.R. Development of point of care testing device for neurovascular coupling from simultaneous recording of EEG and NIRS during anodal transcranial direct current stimulation. IEEE J. Transl. Eng. Health Med. 2015, 3, 2389230. [Google Scholar] [CrossRef] [PubMed]
- Othman, M.H.; Bhattacharya, M.; Møller, K.; Kjeldsen, S.; Grand, J.; Kjaergaard, J.; Dutta, A.; Kondziella, D. Resting-State NIRS–EEG in Unresponsive Patients with Acute Brain Injury: A Proof-of-Concept Study. Neurocrit. Care 2021, 34, 31–44. [Google Scholar] [CrossRef]
- Berger, A.; Horst, F.; Müller, S.; Steinberg, F.; Doppelmayr, M. Current state and future prospects of EEG and fNIRS in robot-assisted gait rehabilitation: A brief review. Front. Hum. Neurosci. 2019, 13, 172. [Google Scholar] [CrossRef]
- Wang, Z.; Cao, C.; Chen, L.; Gu, B.; Liu, S.; Xu, M.; He, F.; Ming, D. Multimodal Neural Response and Effect Assessment During a BCI-Based Neurofeedback Training After Stroke. Front. Neurosci. 2022, 16, 859. [Google Scholar] [CrossRef]
- Durduran, T.; Zhou, C.; Buckley, E.M.; Kim, M.N.; Yu, G.; Choe, R.; Gaynor, J.W.; Spray, T.L.; Durning, S.M.; Mason, S.E.; et al. Optical measurement of cerebral hemodynamics and oxygen metabolism in neonates with congenital heart defects. J. Biomed. Opt. 2010, 15, 037004. [Google Scholar] [CrossRef] [Green Version]
- Rajaram, A.; Yip, L.C.M.; Milej, D.; Suwalski, M.; Kewin, M.; Lo, M.; Carson, J.J.L.; Han, V.; Bhattacharya, S.; Diop, M.; et al. Perfusion and metabolic neuromonitoring during ventricular taps in infants with post-hemorrhagic ventricular dilatation. Brain Sci. 2020, 10, 452. [Google Scholar] [CrossRef] [PubMed]
- De Carli, A.; Andresen, B.; Giovannella, M.; Durduran, T.; Contini, D.; Spinelli, L.; Weigel, U.M.; Passera, S.; Pesenti, N.; Mosca, F.; et al. Cerebral oxygenation and blood flow in term infants during postnatal transition: BabyLux project. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F648–F653. [Google Scholar] [CrossRef]
- Guoqiang Yu, K.G. Diffuse Correlation Spectroscopy (DCS) for Assessment of Tissue Blood Flow in Skeletal Muscle: Recent Progress. Anat. Physiol. 2013, 3, 1000128. [Google Scholar] [CrossRef]
- Zanoletti, M.; Amendola, C.; Buttafava, M.; Carteano, T.; Contini, D.; Cortese, L.; Demarteau, L.; Frabasile, L.; Sagarzazu, E.G.; Guadagno, C.N.; et al. VASCOVID: Hybrid diffuse optical platform combined with a pulse-oximeter and an automatized inflatable tourniquet for the assessment of metabolism and endothelial health in the intensive care. In Proceedings of the Optics InfoBase Conference Papers; Optica Publishing Group: Fort Lauderdale, FL, USA, 2022; p. OS4D.2. [Google Scholar]
- Baker, W.B.; Li, Z.; Schenkel, S.S.; Chandra, M.; Busch, D.R.; Englund, E.K.; Schmitz, K.H.; Yodh, A.G.; Floyd, T.F.; Mohler, E.R. Effects of exercise training on calf muscle oxygen extraction and blood flow in patients with peripheral artery disease. J. Appl. Physiol. 2017, 123, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, V.; Farzam, P.; Anderson, P.; Farzam, P.Y.; Wiese, D.; Carp, S.A.; Ferrari, M.; Franceschini, M.A. Diffuse correlation spectroscopy and frequency-domain near-infrared spectroscopy for measuring microvascular blood flow in dynamically exercising human muscles. J. Appl. Physiol. 2019, 127, 1328–1337. [Google Scholar] [CrossRef]
- Watanabe, T.; Murase, N.; Kime, R.; Kurosawa, Y.; Fuse, S.; Hamaoka, T. Effects of Exercise Training on Cardiac and Skeletal Muscle Functions in Patients with Chronic Heart Failure. Adv. Exp. Med. Biol. 2021, 1269, 101–105. [Google Scholar]
- Whyte, E.; Thomas, S.; Marzolini, S. Muscle Oxygenation of the Paretic and Nonparetic Legs During and After Arterial Occlusion in Chronic Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106265. [Google Scholar] [CrossRef] [PubMed]
- Buma, F.E.; van Kordelaar, J.; Raemaekers, M.; van Wegen, E.E.H.; Ramsey, N.F.; Kwakkel, G. Brain activation is related to smoothness of upper limb movements after stroke. Exp. Brain Res. 2016, 234, 2077–2089. [Google Scholar] [CrossRef]
- Gracies, J.M.; Pradines, M.; Ghédira, M.; Loche, C.M.; Mardale, V.; Hennegrave, C.; Gault-Colas, C.; Audureau, E.; Hutin, E.; Baude, M.; et al. Guided Self-rehabilitation Contract vs conventional therapy in chronic stroke-induced hemiparesis: NEURORESTORE, a multicenter randomized controlled trial. BMC Neurol. 2019, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Zollo, L.; Rossini, L.; Bravi, M.; Magrone, G.; Sterzi, S.; Guglielmelli, E. Quantitative evaluation of upper-limb motor control in robot-aided rehabilitation. Med. Biol. Eng. Comput. 2011, 49, 1131–1144. [Google Scholar] [CrossRef]
- Do Tran, V.; Dario, P.; Mazzoleni, S. Kinematic measures for upper limb robot-assisted therapy following stroke and correlations with clinical outcome measures: A review. Med. Eng. Phys. 2018, 53, 13–31. [Google Scholar] [CrossRef]
- Lang, C.E.; Barth, J.; Holleran, C.L.; Konrad, J.D.; Bland, M.D. Implementation of wearable sensing technology for movement: Pushing forward into the routine physical rehabilitation care field. Sensors 2020, 20, 5744. [Google Scholar] [CrossRef]
- Feldner, H.A.; Howell, D.; Kelly, V.E.; McCoy, S.W.; Steele, K.M. “Look, Your Muscles Are Firing!”: A Qualitative Study of Clinician Perspectives on the Use of Surface Electromyography in Neurorehabilitation. Arch. Phys. Med. Rehabil. 2019, 100, 663–675. [Google Scholar] [CrossRef]
- De Luca, C.J.; Donald Gilmore, L.; Kuznetsov, M.; Roy, S.H. Filtering the surface EMG signal: Movement artifact and baseline noise contamination. J. Biomech. 2010, 43, 1573–1579. [Google Scholar] [CrossRef]
- Manca, A.; Cereatti, A.; Bar-On, L.; Botter, A.; Della Croce, U.; Knaflitz, M.; Maffiuletti, N.A.; Mazzoli, D.; Merlo, A.; Roatta, S.; et al. A Survey on the Use and Barriers of Surface Electromyography in Neurorehabilitation. Front. Neurol. 2020, 11, 1137. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Temporiti, F.; Gatti, R.; Gupta, S.; Sandrini, G.; Serrao, M. Translation of surface electromyography to clinical and motor rehabilitation applications: The need for new clinical figures. Transl. Neurosci. 2023, 14, 20220279. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic review on kinematic assessments of upper limb movements after stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef]
- Wagner, A.K. TBI translational rehabilitation research in the 21st Century: Exploring a Rehabilomics research model. Eur. J. Phys. Rehabil. Med. 2010, 46, 549–555. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Needs and Open Points | Lessons Learnt and Solutions |
|---|---|
| Need for multi-domain assessments and approaches | The use of many different sensors allows us to characterize pathologies with a multifactorial approach, improving clinical standards |
| Provide homogeneous guidelines for data analysis | Adopt standardized methods and criteria for selecting, combining, and analyzing multi-domain data to ensure the validity, reliability, and comparability of results across studies and settings |
| Validate multi-domain approaches | Validate multi-domain approaches against gold-standard measures and clinical outcomes to establish their accuracy, sensitivity, and specificity for different patient populations and conditions |
| Some approaches do not show coherent outcomes |
|
| Preliminary recommendation for clinical practice | Explore novel multi-domain combinations and methods that can capture more aspects of motor function and recovery |
| Adopt multi-domain approaches as a clinical standard | Integrate multi-domain approaches into clinical practice and research by developing user-friendly interfaces, protocols, and guidelines that facilitate their application and interpretation by clinicians and researchers |
| Guarantee tolerable treatments and protocols to patients | Reduce the encumbrance and increase the transparency of multisensory approaches to improve patients’ tolerability |
| Conform multi-domain approaches to clinical time requirements | Reduce research protocols to their essence to be compliant to clinical timings |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scano, A.; Guanziroli, E.; Brambilla, C.; Amendola, C.; Pirovano, I.; Gasperini, G.; Molteni, F.; Spinelli, L.; Molinari Tosatti, L.; Rizzo, G.; et al. A Narrative Review on Multi-Domain Instrumental Approaches to Evaluate Neuromotor Function in Rehabilitation. Healthcare 2023, 11, 2282. https://doi.org/10.3390/healthcare11162282
Scano A, Guanziroli E, Brambilla C, Amendola C, Pirovano I, Gasperini G, Molteni F, Spinelli L, Molinari Tosatti L, Rizzo G, et al. A Narrative Review on Multi-Domain Instrumental Approaches to Evaluate Neuromotor Function in Rehabilitation. Healthcare. 2023; 11(16):2282. https://doi.org/10.3390/healthcare11162282
Chicago/Turabian StyleScano, Alessandro, Eleonora Guanziroli, Cristina Brambilla, Caterina Amendola, Ileana Pirovano, Giulio Gasperini, Franco Molteni, Lorenzo Spinelli, Lorenzo Molinari Tosatti, Giovanna Rizzo, and et al. 2023. "A Narrative Review on Multi-Domain Instrumental Approaches to Evaluate Neuromotor Function in Rehabilitation" Healthcare 11, no. 16: 2282. https://doi.org/10.3390/healthcare11162282