

Can Vitamin D Levels Alter the Effectiveness of Short-Term Facelift Interventions?

Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical and Paraclinical Investigation
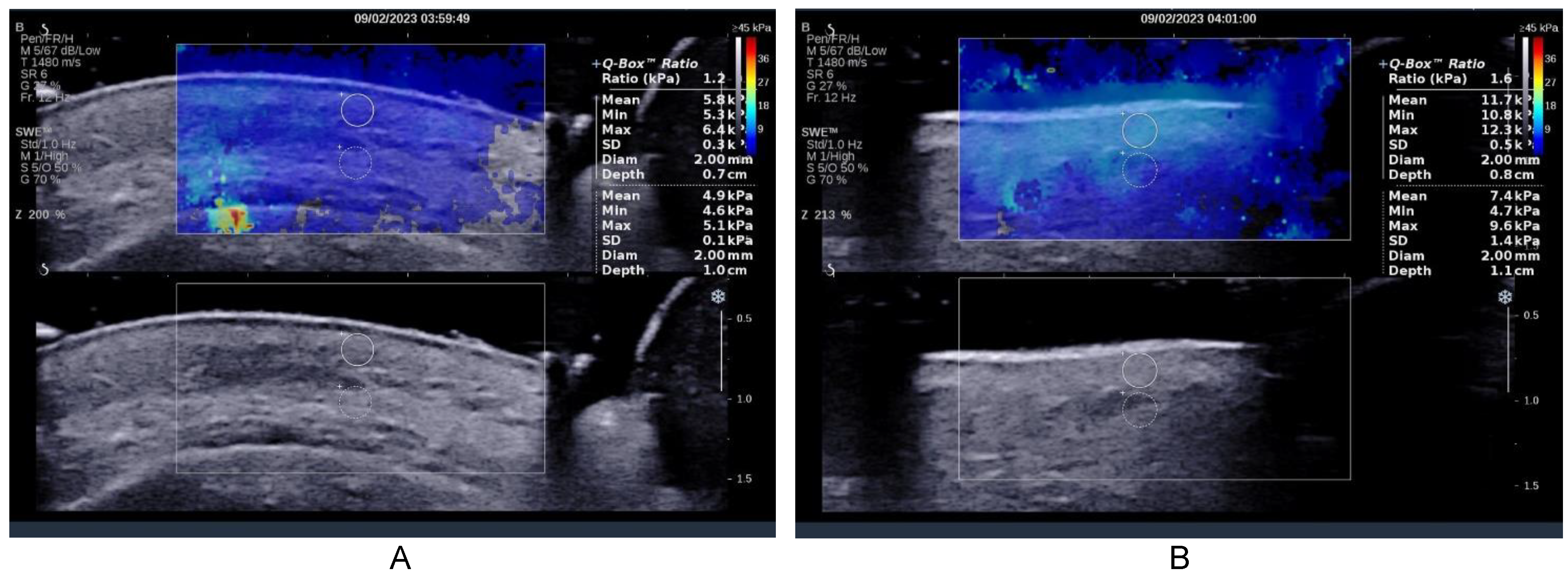
2.2. Ultrasound Examination
2.3. The Rapid Vitamin D Test
- -
- Insufficient ≤ 10 µg/mL.
- -
- Enough 30 µg/mL.
- -
- Optimal 100 µg/mL.
- -
- >100 µg/mL.
2.4. Statistical Analysis
3. Results
3.1. Demographic Description

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Groups | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| NC | C | NC + C | |||||||
| n | % | n | % | n | % | n | % | ||
| Gender | Men | 27 | 17.3 | 6 | 3.8 | 0 | 0.0 | 33 | 21.15 |
| Women | 66 | 42.3 | 43 | 27.6 | 14 | 9.0 | 123 | 78.85 | |
| Environment of provenance | Urban | 80 | 51.3 | 45 | 28.8 | 14 | 9.0 | 139 | 89.10 |
| Rural | 13 | 8.3 | 4 | 2.6 | 0 | 0.0 | 17 | 10.90 | |
| Education | Secondary education | 41 | 26.3 | 6 | 3.8 | 0 | 0.0 | 47 | 30.12 |
| High education | 52 | 33.3 | 43 | 27.6 | 14 | 9.0 | 109 | 69.88 | |
| Age | 45.76 ± 8.09 | 60.71 ± 8.41 | 66.50 ± 5.79 | 50.92 ± 10.60 | |||||
| Total | 156 | ||||||||
3.2. Facelifting
3.3. Minim-Invasive Facelifting with PLA-CL Suspension Wires for Medical Purposes
3.4. Combined Lifting
3.5. Risk Factors
3.6. Vitamin D3
3.7. Correlations
4. Discussion
4.1. Clarification of the Nature and the History of Concerns Related to the Occurrence of Facial Ptosis
4.2. Patient Motivation for Requesting the Procedure
- When did the prospective patient start thinking about surgery to alter their appearance? Was there a particular triggering event? Are there specific influences that may influence their outcome expectations in unrealistic ways?
- Has the prospective patient done anything else to improve their appearance? These questions should elicit information about any unusual or maladaptive behaviors that exist in relation to their physical appearance [51] to be documented examples of individuals with BDD attempting to modify their appearance on their own.
- Why is the prospective patient interested in surgery at this time? What factors led the patient to request a consultation at this time? Is it in response to a significant life event (e.g., divorce) or a series of events? If so, the clinician can explore the feasibility of the proposed surgical intervention in response. Is the future patient’s motivation for surgery a result of intrinsic or extrinsic factors?
4.3. Understanding of the Procedure by the Future Patient
4.4. Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Franco, A.C.; Aveleira, C.; Cavadas, C. Skin senescence: Mechanisms and impact on whole-body aging. Trends. Mol. Med. 2022, 28, 97–109. [Google Scholar] [CrossRef]
- Tit, D.M.; Bungau, S.; Iovan, C.; Nistor Cseppento, D.C.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the hormone replacement therapy and of soy isoflavones on bone resorption in postmenopause. J. Clin. Med. 2018, 7, 297. [Google Scholar] [CrossRef] [PubMed]
- Ţiţ, D.M.; Pallag, A.; Iovan, C.; Furău, G.; Furău, C.; Bungău, S. Somatic-vegetative Symptoms Evolution in Postmenopausal Women Treated with Phytoestrogens and Hormone Replacement Therapy. Iran. J. Public Health 2017, 46, 1528–1534. [Google Scholar] [PubMed]
- Iblher, N.; Stark, G.-B.; Penna, V. The aging perioral region—Do we really know what is happening. J. Nutr. Health Aging 2012, 16, 581–585. [Google Scholar] [CrossRef] [PubMed]
- del Toro, E.; Aldrich, J. Extended SMAS Facelift. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Manturova, N.E.; Stupin, V.A.; Smirnova, G.O.; Silina, E.V. Influence of pharmacological preconditioning on the results of lifting operations efficiency. Heliyon 2018, 4, e00758. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.; Massi, M.N.; Anwar, A.I.; Djawad, K.; Wahab, S. The Use of Autologous Serum in Dermatology. Skinmed 2022, 20, 97–104. [Google Scholar]
- Moore, A.C.M.; Kachare, S.D.; Barber, D.A.; Barrow, L.; O’Daniel, T.G. Total Intravenous Anesthesia With Dexmedetomidine for Hemodynamic Stability and Enhanced Recovery in Facial Aesthetic Surgery. Aesthet Surg. J. 2022, 42, Np602–Np610. [Google Scholar] [CrossRef]
- Khunger, N. Complications in Cosmetic Surgery: A Time to Reflect and Review and not Sweep Them Under the Carpet. J. Cutan Aesthet Surg. 2015, 8, 189–190. [Google Scholar] [CrossRef]
- Couto, R.A.; Charafeddine, A.H.; Zins, J.E. Facelift in patients with massive weight loss. Clin. Plast. Surg. 2019, 46, 559–571. [Google Scholar] [CrossRef]
- Zins, J.E.; Fardo, D. The “anterior-only” approach to neck rejuvenation: An alternative to face lift surgery. Plast. Reconstr. Surg. 2005, 115, 1761–1768. [Google Scholar] [CrossRef]
- Zins, J.E.; Morrison, C.M. Aesthetic surgery of the aging face and neck. Plast. Reconstr. Surg. 2009, 29, 449–463. [Google Scholar]
- Grover, R.; Jones, B.M.; Waterhouse, N. The prevention of haematoma following rhytidectomy: A review of 1078 consecutive facelifts. Br. J. Plast. Surg. 2001, 54, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Mast, B.A. Plastic Surgery: A Practical Guide to Operative Care; Georg Thieme Verlag: Stuttgart, Germany, 2021. [Google Scholar]
- Wynn, T.A. Common and unique mechanisms regulate fibrosis in various fibroproliferative diseases. J. Clin. Investig. 2007, 117, 524–529. [Google Scholar] [CrossRef]
- Iredale, J.P. Models of liver fibrosis: Exploring the dynamic nature of inflammation and repair in a solid organ. J. Clin. Investig. 2007, 117, 539–548. [Google Scholar] [CrossRef]
- Feldman, D.; Pike, J.W.; Adams, J.S. Vitamin D: Two-Volume Set; Academic Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Artaza, J.N.; Norris, K.C. Vitamin D reduces the expression of collagen and key profibrotic factors by inducing an antifibrotic phenotype in mesenchymal multipotent cells. J. Endocrinol. 2009, 200, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Mentella, M.C.; Scaldaferri, F.; Pizzoferrato, M.; Gasbarrini, A.; Miggiano, G.A.D. The Association of Disease Activity, BMI and Phase Angle with Vitamin D Deficiency in Patients with IBD. Nutrients 2019, 11, 2583. [Google Scholar] [CrossRef] [PubMed]
- PĂdureanu, R.; Albu, C.V.; PĂdureanu, V.; BugĂ, A.M. Oxidative Stress and Vitamin D as Predictors in Multiple Sclerosis. Curr. Health Sci. J. 2020, 46, 371–378. [Google Scholar] [CrossRef]
- Żmijewski, M.A. Nongenomic Activities of Vitamin D. Nutrients 2022, 14, 5104. [Google Scholar] [CrossRef]
- Vestita, M.; Tedeschi, P.; Bonamonte, D. Anatomy and Physiology of the Skin. Textb. Plast. Reconstr. Surg. Basic Princ. New Perspect. 2022, 3, 203–213. [Google Scholar]
- Ge, Y.; Luo, J.; Li, D.; Li, C.; Huang, J.; Yu, H.; Lin, X.; Li, Y.; Man, M.; Zhang, J.; et al. Deficiency of vitamin D receptor in keratinocytes augments dermal fibrosis and inflammation in a mouse model of HOCl-induced scleroderma. Biochem. Biophys. Res. Commun. 2022, 591, 1–6. [Google Scholar] [CrossRef]
- Amrein, K.; Oudemans-van Straaten, H.M.; Berger, M.M. Vitamin therapy in critically ill patients: Focus on thiamine, vitamin C, and vitamin D. Intensive Care Med. 2018, 44, 1940–1944. [Google Scholar] [CrossRef]
- Javed, F.; Malmstrom, H.; Kellesarian, S.V.; Al-Kheraif, A.A.; Vohra, F.; Romanos, G.E. Efficacy of vitamin D3 supplementation on osseointegration of implants. Implant. Dent. 2016, 25, 281–287. [Google Scholar] [CrossRef]
- Chen, L.; Wilson, R.; Bennett, E.; Zosky, G.R. Identification of vitamin D sensitive pathways during lung development. Respir. Res. 2016, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Anagnos, D.; Trivedi, M.K.; Branton, A.; Trivedi, D.; Nayak, G.; Mondal, S.C.; Jana, S. Influence of biofield treated vitamin D3 on proliferation, differentiation, and maturation of bone-related parameters in MG-63 cell-line. Int. J. Biomed. Eng. Clin. Sci. 2018, 1, 6–14. [Google Scholar] [CrossRef]
- Ding, J.; Kwan, P.; Ma, Z.; Iwashina, T.; Wang, J.; Shankowsky, H.A.; Tredget, E.E. Synergistic effect of vitamin D and low concentration of transforming growth factor beta 1, a potential role in dermal wound healing. Burns 2016, 42, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Shany, S.; Sigal-Batikoff, I.; Lamprecht, S. Vitamin D and myofibroblasts in fibrosis and cancer: At cross-purposes with TGF-β/SMAD signaling. Anticancer Res. 2016, 36, 6225–6234. [Google Scholar] [CrossRef]
- Bass, J.J.; Nakhuda, A.; Deane, C.S.; Brook, M.S.; Wilkinson, D.J.; Phillips, B.E.; Philp, A.; Tarum, J.; Kadi, F.; Andersen, D. Overexpression of the vitamin D receptor (VDR) induces skeletal muscle hypertrophy. Mol. Metab. 2020, 42, 101059. [Google Scholar] [CrossRef]
- Kjellström, T. Effects on bone, on vitamin D, and calcium metabolism. In Cadmium and Health: A Toxicological and Epidemiological Appraisal; CRC Press: Boca Raton, FL, USA, 2019; pp. 111–158. [Google Scholar]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. Vitamin D for skeletal and non-skeletal health: What we should know. J. Clin. Orthop. Trauma 2019, 10, 1082–1093. [Google Scholar] [CrossRef]
- Garfinkel, R.J.; Dilisio, M.F.; Agrawal, D.K. Vitamin D and its effects on articular cartilage and osteoarthritis. Orthop. J. Sport. Med. 2017, 5, 2325967117711376. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Yu, H.-T.; Kao, J.-P.; Yang, C.-C.; Chiang, S.-S.; Mishchuk, D.O.; Mau, J.-L.; Slupsky, C.M. Consumption of vitamin D2 enhanced mushrooms is associated with improved bone health. J. Nutr. Biochem. 2015, 26, 696–703. [Google Scholar] [CrossRef]
- Bocheva, G.; Slominski, R.M.; Slominski, A.T. The Impact of Vitamin D on Skin Aging. Int. J. Mol. Sci. 2021, 22, 9097. [Google Scholar] [CrossRef] [PubMed]
- Brown Lobbins, M.L.; Slominski, A.T.; Hasty, K.A.; Zhang, S.; Miller, D.D.; Li, W.; Kim, T.-K.; Janjetovic, Z.; Tuckey, R.C.; Scott, I.-S.O.; et al. Modulation by 17,20S(OH)2pD of Fibrosis-Related Mediators in Dermal Fibroblast Lines from Healthy Donors and from Patients with Systemic Sclerosis. Int. J. Mol. Sci. 2022, 23, 367. [Google Scholar] [CrossRef]
- Nejat, S.; Montazeri, A.; Holakouie Naieni, K.; Mohammad, K.; Majdzadeh, S. The World Health Organization quality of Life (WHOQOL-BREF) questionnaire: Translation and validation study of the Iranian version. J. Sch. Public Health Inst. Public Health Res. 2006, 4, 1–12. [Google Scholar]
- Mohammad Zadeh, A.; Najafi, M. Validating of the Big Five Inventory (BFI-10): A very brief measure of the five factor personality model. Educ. Meas. 2010, 1, 117–130. [Google Scholar]
- Sarwer, D.B.; Spitzer, J.C. Body image dysmorphic disorder in persons who undergo aesthetic medical treatments. Aesthetic Surg. J. 2012, 32, 999–1009. [Google Scholar] [CrossRef]
- Althubaiti, G.A. The Hybrid Facelift. Plast Reconstr. Surg. Glob. Open 2022, 10, e4503. [Google Scholar] [CrossRef]
- Cè, M.; D’Amico, N.C.; Danesini, G.M.; Foschini, C.; Oliva, G.; Martinenghi, C.; Cellina, M. Ultrasound Elastography: Basic Principles and Examples of Clinical Applications with Artificial Intelligence—A Review. BioMedInformatics 2023, 3, 17–43. [Google Scholar] [CrossRef]
- Ozturk, A.; Grajo, J.R.; Dhyani, M.; Anthony, B.W.; Samir, A.E. Principles of ultrasound elastography. Abdom Radiol 2018, 43, 773–785. [Google Scholar] [CrossRef]
- Sigrist, R.M.; Liau, J.; El Kaffas, A.; Chammas, M.C.; Willmann, J.K. Ultrasound elastography: Review of techniques and clinical applications. Theranostics 2017, 7, 1303. [Google Scholar] [CrossRef]
- Chung, K. Grabb and Smith’s Plastic Surgery; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2019. [Google Scholar]
- Edgerton, M.T.; Langman, M.W.; Pruzinsky, T. Plastic surgery and psychotherapy in the treatment of 100 psychologically disturbed patients. Plast. Reconstr. Surg. 1991, 88, 594–608. [Google Scholar] [CrossRef]
- Sarwer, D.B. Body image, cosmetic surgery, and minimally invasive treatments. Body Image 2019, 31, 302–308. [Google Scholar] [CrossRef]
- Das, S.S.; Bharadwaj, P.; Bilal, M.; Barani, M.; Rahdar, A.; Taboada, P.; Bungau, S.; Kyzas, G.Z. Stimuli-responsive polymeric nanocarriers for drug delivery, imaging, and theragnosis. Polymers 2020, 12, 1397. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, M.; Endres, L.; Pasca, B.; Tit, D.M.; Uivarosan, D.; Copolovici, D.M.; Aleya, L.; Bungau, S. Study on the Stability and Compatibility of the Cosmetic Products with Lavandula angustifolia Oil Kept in PPH Polypropylene Homopolymer Plastic Containers. Mater. Plast. 2019, 56, 133. [Google Scholar] [CrossRef]
- Bungau, S.; Vesa, C.M.; Abid, A.; Behl, T.; Tit, D.M.; Purza, A.L.; Pasca, B.; Todan, L.M.; Endres, L. Withaferin A—A promising phytochemical compound with multiple results in dermatological diseases. Molecules 2021, 26, 2407. [Google Scholar] [CrossRef] [PubMed]
- Behl, T.; Sharma, A.; Sharma, L.; Sehgal, A.; Zengin, G.; Brata, R.; Fratila, O.; Bungau, S. Exploring the Multifaceted Therapeutic Potential of Withaferin A and Its Derivatives. Biomedicines 2020, 8, 571. [Google Scholar] [CrossRef]
- Veale, D.; De Haro, L.; Lambrou, C. Cosmetic rhinoplasty in body dysmorphic disorder. Br. J. Plast. Surg. 2003, 56, 546–551. [Google Scholar] [CrossRef]
- Goodman, G.D.; Kaufman, J.; Day, D.; Weiss, R.; Kawata, A.K.; Garcia, J.K.; Santangelo, S.; Gallagher, C.J. Impact of Smoking and Alcohol Use on Facial Aging in Women: Results of a Large Multinational, Multiracial, Cross-sectional Survey. J. Clin. Aesthet. Derm. 2019, 12, 28–39. [Google Scholar]
- Li, S.; Cho, E.; Drucker, A.M.; Qureshi, A.A.; Li, W.-Q. Alcohol intake and risk of rosacea in US women. J. Am. Acad. Dermatol. 2017, 76, 1061–1067.e1062. [Google Scholar] [CrossRef]
- Addolorato, G.; Capristo, E.; Marini, M.; Santini, P.; Scognamiglio, U.; Attilia, M.; Messineo, D.; Sasso, G.; Gasbarrini, G.; Ceccanti, M. Body composition changes induced by chronic ethanol abuse: Evaluation by dual energy X-ray absorptiometry. Am. J. Gastroenterol. 2000, 95, 2323–2327. [Google Scholar] [CrossRef]
- Kaya, K.S.; Cakmak, O. Facelift Techniques: An Overview. Facial. Plast. Surg. 2022, 38, 540–545. [Google Scholar] [CrossRef]
- Guyuron, B.; Seyed Forootan, N.S.; Katira, K. The Super-High SMAS Facelift Technique with Tailor Tack Plication. Aesthetic Plast. Surg. 2018, 42, 1531–1539. [Google Scholar] [CrossRef] [PubMed]
- Rat, L.A.; Moldovan, A.F.; Trifan, D.F.; Matiș, L.; Murvai, G.F.; Maris, L.; Ghitea, T.C.; Maghiar, M.A. Can the Correlation of Periodontopathies with Gastrointestinal Diseases Be Used as Indicators in Severe Colorectal Diseases? Biomedicines 2023, 11, 402. [Google Scholar] [CrossRef]
- Nistor-Cseppento, C.D.; Moga, T.D.; Bungau, A.F.; Tit, D.M.; Negrut, N.; Pasca, B.; Bochis, C.F.; Ghitea, T.C.; Jurcau, A.; Purza, A.L.; et al. The Contribution of Diet Therapy and Probiotics in the Treatment of Sarcopenia Induced by Prolonged Immobilization Caused by the COVID-19 Pandemic. Nutrients 2022, 14, 4701. [Google Scholar] [CrossRef] [PubMed]
- Stoita, M.; Abid, A.; VESA, C.; Aron, R.A.C.; Ghitea, T.C.; Angelescu, G.; Popa, A. Epidemiology and Pathophysiological Mechanisms involved in Alteration of Glomerular Function in Diabetic Patients. Arch. Balk. Med. Union 2021, 56, 1. [Google Scholar] [CrossRef]
- Murdaca, G.; Tonacci, A.; Negrini, S.; Greco, M.; Borro, M.; Puppo, F.; Gangemi, S. Emerging role of vitamin D in autoimmune diseases: An update on evidence and therapeutic implications. Autoimmun. Rev. 2019, 18, 102350. [Google Scholar] [CrossRef]
- Li, S.; Niu, G.; Wu, Y.; Du, G.; Huang, C.; Yin, X.; Liu, Z.; Song, C.; Leng, H. Vitamin D prevents articular cartilage erosion by regulating collagen II turnover through TGF-β1 in ovariectomized rats. Osteoarthr. Cartil. 2016, 24, 345–353. [Google Scholar] [CrossRef]
- Rai, V.; Dietz, N.E.; Dilisio, M.F.; Radwan, M.M.; Agrawal, D.K. Vitamin D attenuates inflammation, fatty infiltration, and cartilage loss in the knee of hyperlipidemic microswine. Arthritis Res. Ther. 2016, 18, 203. [Google Scholar] [CrossRef]
- McKnight, G.; Shah, J.; Hargest, R. Physiology of the skin. Surgery 2022, 40, 8–12. [Google Scholar] [CrossRef]
- Philips, N.; Portillo-Esnaola, M.; Samuel, P.; Gallego-Rentero, M.; Keller, T.; Franco, J. Anti-aging and anti-carcinogenic effects of 1α, 25-dihyroxyvitamin D 3 on skin. Plast. Aesthetic Res. 2022, 9, 4. [Google Scholar] [CrossRef]












| Parameters | Upper | Middle | Lower | |
|---|---|---|---|---|
| Before | ||||
| Right | Derm | 7.2 ± 0.6 | 7.0 ± 0.4 | 8.8 ± 1.1 |
| TCS | 9.9 ± 0.8 | 13.8 ± 3.5 | 8.4 ± 0.8 | |
| Left | Derm | 5.5 ± 0.4 | 6.7 ± 0.8 | 9.5 ± 0.5 |
| TCS | 7.1 ± 0.2 | 6.5 ± 0.8 | 11.0 ± 1.3 | |
| After | ||||
| Right | Derm | 7.1 ± 0.5 | 6.9 ± 0.7 | 8.1 ± 1.4 |
| TCS | 8.9 ± 0.6 | 10.1 ± 2.5 | 8.7 ± 0.6 | |
| Left | Derm | 5.7 ± 0.4 | 6.0 ± 0.6 | 7.1 ± 0.8 |
| TCS | 7.0 ± 0.3 | 6.9 ± 0.5 | 8.5 ± 1.1 | |
| Before | ||||
|---|---|---|---|---|
| Parameters | Upper | Middle | Lower | |
| Right | Derm | 5.5 ± 0.7 | 7.3 ± 1.2 | 5.6 ± 0.7 |
| TCS | 6.5 ± 0.4 | 8.7 ± 1.1 | 7.1 ± 0.5 | |
| Left | Derm | 6.1 ± 0.4 | 7.5 ± 0.8 | 4.1 ± 1.0 |
| TCS | 4.9 ± 1.1 | 7.8 ± 1.2 | 6.2 ± 0.6 | |
| After | ||||
| Right | Derm | 7.7 ± 1.0 | 4.4 ± 0.4 | 5.5 ± 0.6 |
| TCS | 9.5 ± 0.6 | 7.8 ± 1.1 | 9.5 ± 0.5 | |
| Left | Derm | 6.0 ± 1.0 | 6.3 ± 0.9 | 3.9 ± 1.0 |
| TCS | 8.9 ± 0.7 | 7.2 ± 0.7 | 6.7 ± 0.7 | |
| Parameters | Groups | ||||||
|---|---|---|---|---|---|---|---|
| NC | C | NC + C | |||||
| n | % | n | % | n | % | ||
| Hypertension | No | 68 | 43.6 | 33 | 21.2 | 8 | 5.1 |
| Yes | 25 | 16.0 | 16 | 10.3 | 6 | 3.8 | |
| Alcohol consumption | No | 77 | 49.4 | 30 | 19.2 | 8 | 5.1 |
| Yes | 16 | 10.3 | 19 | 12.2 | 6 | 3.8 | |
| Smoking | No | 89 | 57.1 | 38 | 24.4 | 12 | 7.7 |
| Yes | 4 | 2.6 | 11 | 7.1 | 2 | 1.3 | |
| Diabetes melitus | No | 81 | 51.9 | 43 | 27.6 | 11 | 7.1 |
| Yes | 12 | 7.7 | 6 | 3.8 | 3 | 1.9 | |
| Vitamin D | Groups | ||||||
|---|---|---|---|---|---|---|---|
| NC | C | NC + C | |||||
| n | % | n | % | n | % | ||
| Initial | Insufficient < 10 µg/mL | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sufficient 30 µg/mL | 17 | 18.3 | 0 | 0.0 | 14 | 100.0 | |
| Optim 100 µg/mL | 76 | 81.7 | 49 | 100 | 0 | 0.0 | |
| Exces > 100 µg/mL | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Final | Insufficient < 10 µg/mL | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Sufficient 30 µg/mL | 15 | 16.1 | 7 | 14.3 | 12 | 85.7 | |
| Optim 100 µg/mL | 78 | 83.9 | 42 | 85.7 | 2 | 14.3 | |
| Exces > 100 µg/mL | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trifan, D.F.; Tirla, A.G.; Moldovan, A.F.; Moș, C.; Bodog, F.; Maghiar, T.T.; Manole, F.; Ghitea, T.C. Can Vitamin D Levels Alter the Effectiveness of Short-Term Facelift Interventions? Healthcare 2023, 11, 1490. https://doi.org/10.3390/healthcare11101490
Trifan DF, Tirla AG, Moldovan AF, Moș C, Bodog F, Maghiar TT, Manole F, Ghitea TC. Can Vitamin D Levels Alter the Effectiveness of Short-Term Facelift Interventions? Healthcare. 2023; 11(10):1490. https://doi.org/10.3390/healthcare11101490
Chicago/Turabian StyleTrifan, Daniela Florina, Adrian Gheorghe Tirla, Andrada Florina Moldovan, Calin Moș, Florian Bodog, Teodor Traian Maghiar, Felicia Manole, and Timea Claudia Ghitea. 2023. "Can Vitamin D Levels Alter the Effectiveness of Short-Term Facelift Interventions?" Healthcare 11, no. 10: 1490. https://doi.org/10.3390/healthcare11101490