
Effectiveness of the Boston Brace in the Treatment of Paediatric Scoliosis: A Longitudinal Study from 2010–2020 in a National Spinal Centre
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
3.1. Patients with IS
3.1.1. Patients with IS at the End of Bracing/No Need for Scoliosis Surgery (98 Patients; 85 AIS, 9 JIS, 4 IIS)
3.1.2. Patients with IS at the End of Bracing Who Underwent Scoliosis Surgery (84 Patients; 48 AIS, 36 JIS)
3.2. Patients with Non-IS
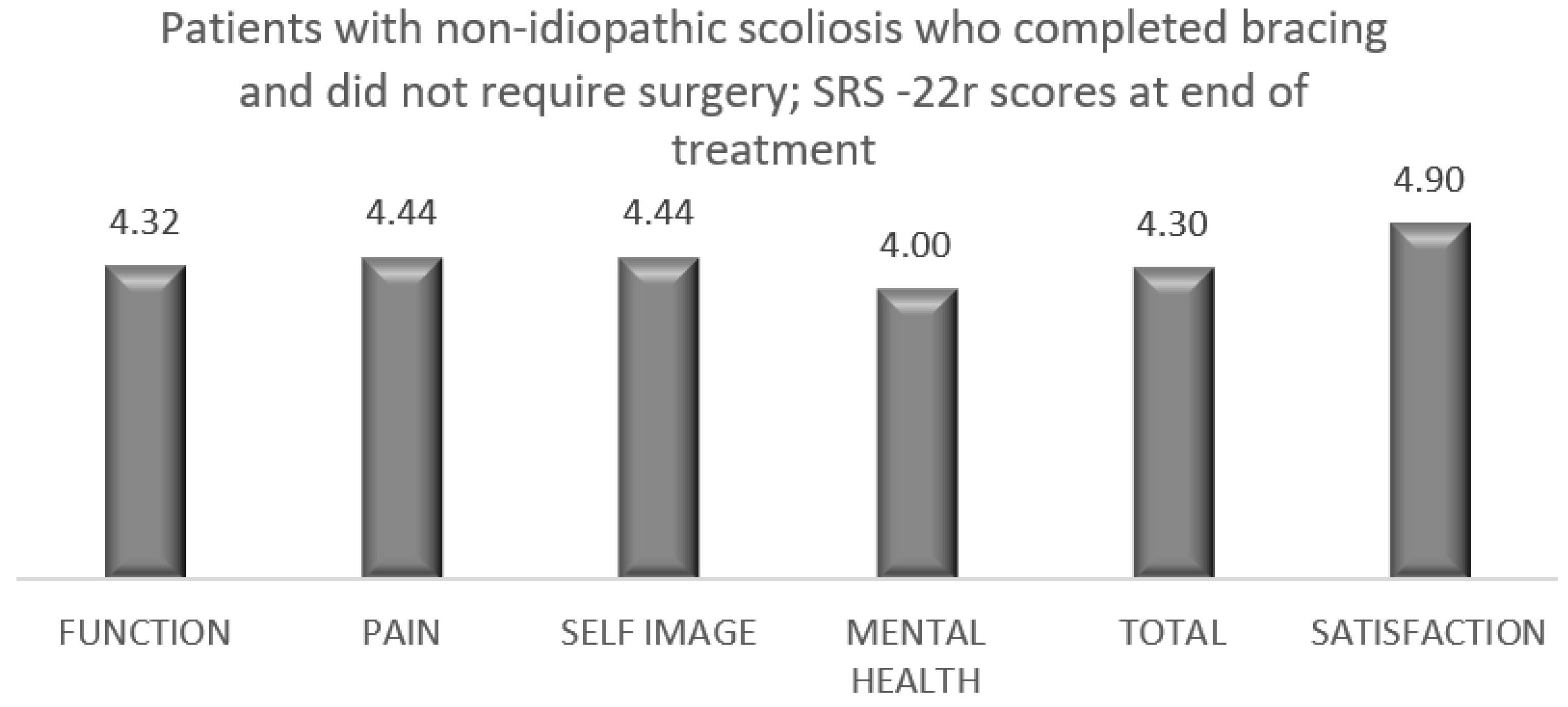
3.2.1. Patients with Non-IS at the End of Bracing/No Need for Scoliosis Surgery (20 Patients; 5 with Congenital Scoliosis, 5 with NM Scoliosis, 6 with Syndromic Scoliosis, 4 with Secondary Scoliosis)
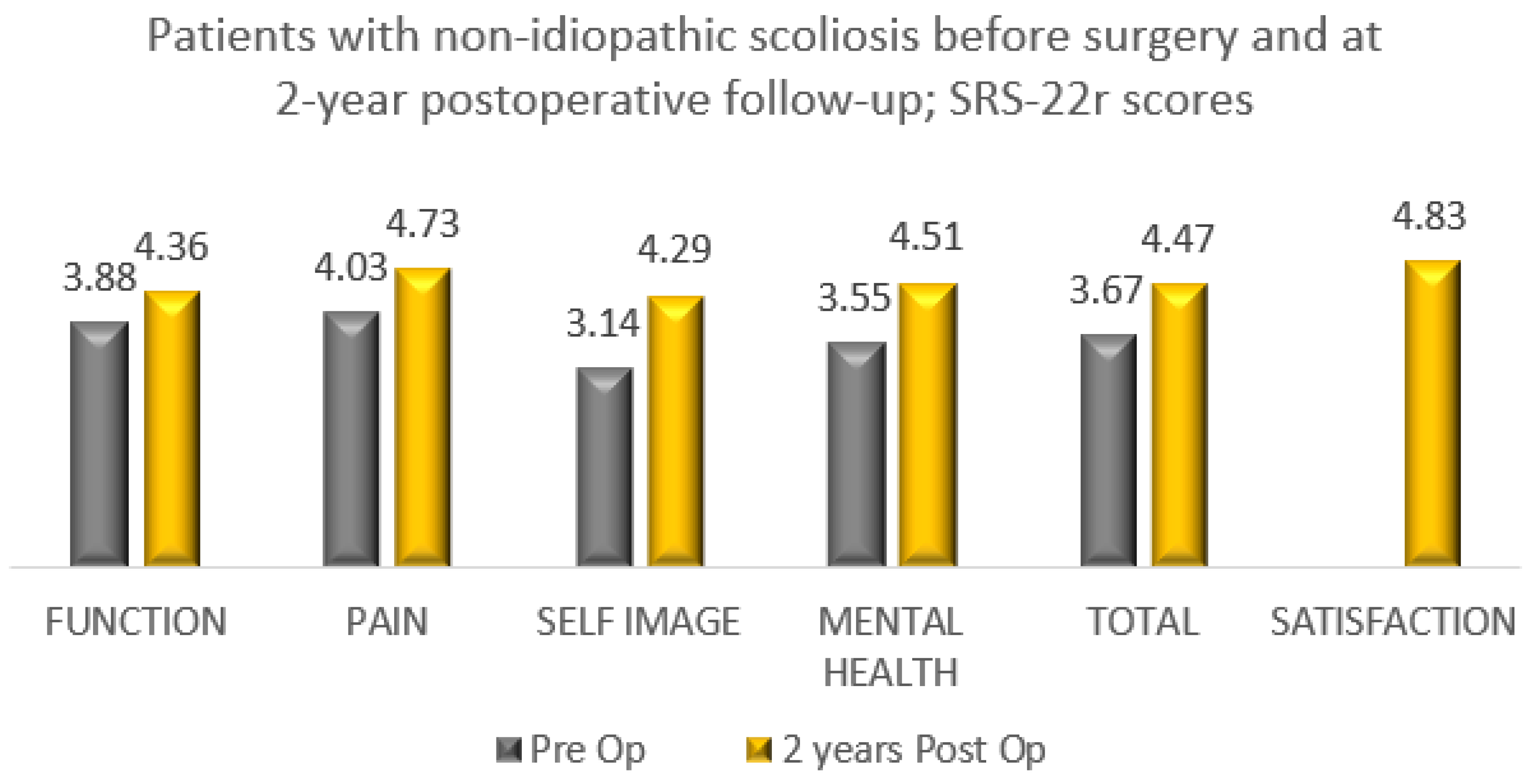
3.2.2. Patients with Non-IS at the End of Bracing Who Underwent Scoliosis Surgery (47 Patients; 9 with Congenital Scoliosis, 3 with NM Scoliosis, 21 with Syndromic Scoliosis, 14 with Secondary Scoliosis)
3.3. Multivariate Logistic Regression Analysis
3.4. Patient Reported Outcomes (End of Bracing and after Scoliosis Surgery)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sud, A.; Tsirikos, A. Current concepts and controversies on adolescent idiopathic scoliosis: Part I. Indian J. Orthop. 2013, 47, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Nachemson, A.L.; Lonstein, J.E.; Weinstein, S.L. Report of the SRS Prevalence and Natural History Committee 1982. In Proceedings of the Scoliosis Research Society 17th Annual Meeting, Denver, CO, USA, 22–25 September 1982; pp. 22–25. [Google Scholar]
- Weinstein, S.L.; Ponseti, I.V. Curve progression in idiopathic scoliosis. J. Bone Joint Surg. Am. 1983, 65, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Tambe, A.D.; Panikkar, S.J.; Millner, P.A.; Tsirikos, A.I. Current concepts in the surgical management of adolescent idiopathic scoliosis. Bone Jt. J. 2018, 100B, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Spratt, K.F.; Peterson, K.K.; Spoonamore, M.J.; Ponseti, I.V. Health and function of patients with untreated idiopathic scoliosis: A 50-year natural history study. JAMA 2003, 289, 559–5567. [Google Scholar] [CrossRef] [PubMed]
- Risser, J.C. The iliac apophysis: An invaluable sign in the management of scoliosis. Clin. Orthop. Relat. Res. 1958, 11, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of bracing in adolescents with idiopathic scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Loughenbury, P.R.; Tsirikos, A.I. Current concepts in the treatment of neuromuscular scoliosis: Clinical assessment, treatment options, and surgical outcomes. Bone J. Open. 2022, 3, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Hedequist, D.; Emans, J. Congenital scoliosis. A review and update. J. Pediatr. Orthop. 2007, 27, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Tsirikos, A.I.; Augustithis, G.A.; McKean, G.; Karampalis, C. Cyanotic congenital cardiac disease and scoliosis: Preoperative assessment, surgical treatment and outcomes. Med. Princ. Pract. 2020, 29, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Feng, Z.; Wu, Z.; Qiu, Y.; Zhu, Z.; Xu, L. Brace treatment can serve as a time-buying tactic for patients with congenital scoliosis. J. Orthop. Surg. Res. 2019, 14, 194. [Google Scholar] [CrossRef] [PubMed]
- Sponseller, P.D. Results of brace treatment of scoliosis in Marfan syndrome. Spine 2000, 25, 2350–2354. [Google Scholar] [CrossRef] [PubMed]
- Canavese, F.; Dimeglio, A. Normal and abnormal spine and thoracic cage development. World J. Orthop. 2013, 4, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.; Khoury, J.; Kishan, S.; Browne, R.; Mooney, J.; Arnold, K.D.; McConnell, S.J.; Bauman, J.A.; Finegold, D. Predicting scoliosis progression from skeletal maturity: A simplified classification during adolescence. J. Bone Jt. Surg. Am. 2008, 90, 540–553. [Google Scholar] [CrossRef]
- Schiller, J.R.; Thakur, N.A.; Eberson, C.P. Brace management in adolescent idiopathic scoliosis. Clin. Orthop. Relat. Res. 2010, 468, 670–678. [Google Scholar] [CrossRef]
- Costa, L.; Schlosser, T.P.C.; Jimale, H.; Homans, J.F.; Kruyt, M.C.; Castelein, R.M. The effectiveness of different concepts of bracing in adolescent idiopathic scoliosis (AIS): A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 2145. [Google Scholar] [CrossRef]
- Richards, B.S.; Bernstein, R.M.; D’Amato, C.R.; Thompson, G.H. Standardisation of criteria for adolescent idiopathic scoliosis brace studies. Spine 2005, 30, 2068–2075. [Google Scholar] [CrossRef] [PubMed]
- Lonstein, J.E.; Winter, R.B. The Milwaukee brace for the treatment of adolescent idiopathic scoliosis. A review of one thousand and twenty patients. J. Bone Jt. Surg. 1994, 76, 1207–1221. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, S.S.; Nelson, I.W.; Ho, E.K.; Hsu, L.C.; Leong, J.C. New prognostic factors to predict the final outcome of brace treatment in adoelescent idiopathic scoliosis. Spine 1995, 20, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Ovadia, D.; Eylon, S.; Mashiah, A.; Wientroub, S.; Lebel, E.D. Factors associated with the success of the Rigo System Cheneau brace in treating mild to moderate adolescent idiopathic scoliosis. J. Child. Orthop. 2012, 6, 327–331. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | Neuromuscular (10 Patients) | Syndromic (24 Patients) | Secondary (19 Patients) |
|---|---|---|---|
| Hemiplegic cerebral palsy | 5 | - | - |
| Charcot–Marie–Tooth disease | 3 | - | - |
| Congenital hypotonia | 2 | - | - |
| Scoliosis with Chiari I malformation and syringomyelia | - | - | 7 |
| Scoliosis with syringomyelia | - | - | 5 |
| Scoliosis with congenital cardiac disease | - | - | 5 |
| Scoliosis with intraspinal tumour | - | - | 2 |
| Chromosome abnormality | - | 10 | - |
| Marfan syndrome | - | 4 | - |
| Neurofibromatosis type-1 | - | 2 | - |
| Pierre Robin syndrome | - | 2 | - |
| Prader–Willi syndrome | - | 2 | - |
| Ehlers–Danlos syndrome | - | 1 | - |
| Hurler syndrome | - | 1 | - |
| Cleidocranial dysostosis | - | 1 | - |
| Carey–Fineman–Ziter syndrome | - | 1 | - |
| Data | AIS (85 Patients) | JIS (9 Patients) | IIS (4 Patients) |
|---|---|---|---|
| Type of scoliosis | TH: 10; TH and L: 41; double TH: 4; TL/L: 21 | TH: 2; TH and L: 6; double TH: 1 | TH: 1; TL/L:3 |
| TH scoliosis pre-brace | 28° (range: 16–43°) | 32° (range: 13–56°) | 56° |
| TH scoliosis in 1st brace | 19° (range: 0–38°) | 16° (range: 0–24°) | 24° |
| TH scoliosis at last follow-up | 26° (range: 0–42°) | 20° (range: 0–40°) | 17° |
| Mean TH scoliosis improvement | 7° | 5° | 41° |
| TL/L scoliosis pre-brace | 28° (range: 13–44°) | 21° (range: 20–35°) | 43° (range: 36–50°) |
| TL/L scoliosis in 1st brace | 17° (range: 0–34°) | 11° (range: 0–22°) | 26° (range: 19–36°) |
| TL/L scoliosis at last follow-up | 21° (range: 0–40°) | 16° (range: 0–20°) | 2° (range: 0–5°) |
| Mean TL/L scoliosis improvement | 7° | 5° | 41° |
| Triradiate cartilage | Open: 28 Closed: 48 | Open: 9 | Open: 4 |
| Risser grade (start of bracing) | 0.4 (range: 0–2) | 0 | 0 |
| Risser grade (end of bracing) | 4.8 (range: 0–5) | 4.7 (range: 3–5) | 0 (range: 0–1) |
| Age (start of bracing); years | 12.9 (range: 10.1–15.9) | 7.2 (range: 3.3–10) | 2.3 (range: 1.9–2.4) |
| Age (end of bracing); years | 16.1 (range: 12.8–18.4) | 15.5 (range: 13.6–18.1) | 8.8 (range: 6.4–12.2) |
| Years in brace treatment | 3.2 (range: 0.5–9.1) | 8.4 (range: 4.1–14.4) | 6.4 (range: 3.8–9.6) |
| Follow-up (after bracing); years | 2.2 (range: 2–2.5) | 2.1 (range: 2–2.3) | 2 (range: 2–2.1) |
| Data | AIS (48 Patients) | JIS (36 Patients) |
|---|---|---|
| Type of scoliosis | TH: 9; TH and L: 31; double TH: 3; TL/L: 5 | TH: 10; TH and L: 21; double TH: 4 |
| TH scoliosis pre-brace | 35.4° (range: 15–64°) | 41° (range: 22–70°) |
| TH scoliosis in 1st brace | 27.7° (range: 8–51°) | 27.7° (range: 10–70°) |
| TH scoliosis at end of bracing | 48.9° (range: 17–84°) | 59.8° (range: 11–97°) |
| TH scoliosis preoperatively | 50.4° (range: 17–84°) | 64.3° (range: 46–97°) |
| TH scoliosis at last follow-up | 18.1° (range: 4–41°) | 24.9° (range: 4–50°) |
| Mean TH scoliosis improvement | 17.3° | 16° |
| TL/L scoliosis pre-brace | 32.4° (range: 18–51°) | 33.6° (range: 17–54°) |
| TL/L scoliosis in 1st brace | 24.4° (range: 14–51°) | 24.4° (range: 9–46°) |
| TL/L scoliosis at end of bracing | 45.1° (range: 22–66°) | 47.8° (range: 12–69°) |
| TL/L scoliosis preoperatively | 48.8° (range: 28–66°) | 54.4° (range: 31–69°) |
| TL/L scoliosis at last follow-up | 17.6° (range: 2–45°) | 19.1° (range: 4–29°) |
| Mean TL/L scoliosis improvement | 14.8° | 14° |
| Triradiate cartilage | Open: 32 Closed: 16 | Open: 36 |
| Risser grade (start of bracing) | 0.1 (range: 0–2) | 0 |
| Risser grade (end of bracing) | 4 (range: 4–5) | 3.5 (range: 0–5) |
| Age (start of bracing); years | 12.5 (range: 10.2–15.8) | 7.8 (range: 3.1–10) |
| Age (end of bracing); years | 14.6 (range: 11.2–17.7) | 12.5 (range: 9.8–16.8) |
| Age at scoliosis surgery; years | 14.9 (range: 11.6–18.4) | 12.8 (range: 10.2–16.8) |
| Years in brace treatment | 2.4 (range: 0.6–5.1) | 5 (range: 1.6–9.4) |
| Follow-up (post-surgery); years | 2.8 (range: 2–3.5) | 3.5 (range: 2.6–4.8) |
| Data | AIS without Surgery (71 Patients) | AIS with Surgery (26 Patients) |
|---|---|---|
| Type of scoliosis | TH: 9; TH and L: 37; double TH: 4; TL/L: 21 | TH: 3; TH and L: 15; double TH: 3; TL/L:5 |
| TH scoliosis pre-brace | 26.3° (range: 16–40°) | 29.1° (range: 15–39°) |
| TH scoliosis in 1st brace | 18.2° (range: 0–38°) | 22.8° (range: 8–36°) |
| TH scoliosis at end of bracing | 25.4° (range: 0–45°) | 44° (range: 17–65°) |
| TH scoliosis preoperatively | - | 47° (range: 17–65°) |
| TH scoliosis at last follow-up | - | 18.4° (range: 4–38°) |
| Mean TH scoliosis improvement | 0.9° | 10.7° |
| TL/L scoliosis pre-brace | 25.1° (range: 13–40°) | 30.8° (range:18–40°) |
| TL/L scoliosis in 1st brace | 16.3° (range: 0–34°) | 22.8° (range: 14–32°) |
| TL/L scoliosis at end of bracing | 21° (range: 0–38°) | 40° (range: 22–66°) |
| TL/L scoliosis preoperatively | - | 44.3° (range: 28–66°) |
| TL/L scoliosis at last follow-up | - | 17.2° (range: 2–45°) |
| Mean TL/L scoliosis improvement | 4.1° | 13.6° |
| Triradiate cartilage | Open: 27 Closed: 44 | Open: 15 Closed: 11 |
| Risser grade (start of bracing) | 0.4 (range: 0–2) | 0.19 (range: 0–2) |
| Risser grade (end of bracing) | 4.7 (range: 4–5) | 4.2 (range: 1–5) |
| Age (start of bracing); years | 12.9 (range: 9.9–15.9) | 12.6 (range: 10.3–15.8) |
| Age (end of bracing); years | 16 (range: 14.8–18.4) | 15 (range:11.9–17.6) |
| Age at scoliosis surgery; years | - | 15.4 (range: 12.6–17.8) |
| Years in brace treatment | 3.2 (range: 0.5–9.1) | 2.1 (range: 0.2–4.2) |
| Follow-up (after bracing); years | 4 (range: 0.9–8.7) | - |
| Follow-up (post-surgery); years | - | 5 (range: 1.8–8.9) |
| Data | Congenital Scoliosis (9 Patients) | NM Scoliosis (3 Patients) | Syndromic Scoliosis (21 Patients) | Secondary Scoliosis (14 Patients) |
|---|---|---|---|---|
| Type of scoliosis | TH: 2; TH and L: 7 | TH and L: 2; TL/L: 1 | TH: 8; TH and L: 9; double TH: 1; TL/L: 3 | TH: 6; TH and L: 7; TL/L: 1 |
| TH scoliosis pre-brace | 40.4° (range: 25–59°) | 32° (range: 27–37°) | 35.8° (range: 20–65°) | 47.2° (range: 21–78°) |
| TH scoliosis in 1st brace | 32.3° (range: 15–46°) | 26.5° (range: 24–29°) | 28.2° (range: 15–54°) | 33.9° (range: 14–51°) |
| TH scoliosis at end of bracing | 50.1° (range: 10–72°) | 53° (range: 46–60°) | 72° (range: 43–98°) | 74° (range: 34–117°) |
| TH scoliosis preoperatively | 56.1° (range: 10–72°) | 56° (range: 52–60°) | 76.5° (range: 50–98°) | 74° (range: 34–117°) |
| TH scoliosis at last follow-up | 32.6° (range: 11–43°) | 29.5° (range: 28–31°) | 31.8° (range: 17–45°) | 31.7° (range: 17–63°) |
| Mean TH scoliosis improvement | 7.8° | 2.5° | 4° | 15.5° |
| TL/L scoliosis pre-brace | 32.1° (range: 22–48°) | 35.5° (range: 31–40°) | 33.5° (range: 14–58°) | 41.8° (range: 24–51°) |
| TL/L scoliosis in 1st brace | 24.2° (range: 16–33°) | 21° (range: 17–23°) | 20.8° (range: 10–35°) | 25.5° (range: 18–35°) |
| TL/L scoliosis at end of bracing | 45.5° (range: 13–85°) | 57.8° (range: 36–67°) | 57.7° (range: 39–81°) | 38.4° (range: 27–70°) |
| TL/L scoliosis preoperatively | 48.3° (range: 13–85°) | 60.3° (range: 46–67°) | 60° (range: 43–81°) | 48.4° (range: 38–70°) |
| TL/L scoliosis at last follow-up | 22.7° (range: 8–50°) | 26.3° (range: 18–32°) | 22.9° (range: 8–30°) | 17.5° (range: 12–31°) |
| Mean TL/L scoliosis improvement | 9.4° | 9.2° | 10.6° | 24.3° |
| Triradiate cartilage | Open: 9 | Open: 3 | Open: 21 | Open: 13; Closed: 1 |
| Risser grade (start of bracing) | 0.5 (range: 0–1) | 0 | 0 | 0 |
| Risser grade (end of bracing) | 4.5 (range: 4–5) | 4.5 (range: 4–5) | 2.3 (range: 0–5) | 3.6 (range: 0–5) |
| Age (start of bracing); years | 5.3 (range: 1.6–11.7) | 7.2 (range: 6.2–8) | 6.8 (range: 2.2–14.2) | 8.8 (range: 1.7–3.6) |
| Age (end of bracing); years | 12.9 (range: 10.2–15.8) | 13.7 (range: 12.7–15.1) | 12.4 (range: 9.6–16.7) | 12.6 (range: 9.9–15.9) |
| Age at scoliosis surgery; years | 13.3 (range: 10.6–16.1) | 13.9 (range: 12.7–15.6) | 12.7 (range: 10.4–16.7) | 12.6 (range: 10.3–5.9) |
| Years in brace treatment | 5.2 (range: 2.1–8.8) | 6.7 (range: 5.3–7.7) | 5.8 (range: 2.4–11.8) | 4 (range: 1.2–7.3) |
| Follow-up (post-surgery); years | 4.5 (2.5–5) | 4.5 (2–4.8) | 4.1 (2.4–4.5) | 4.2 (2.6–5) |
| Characteristics | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Scoliosis angle | 1.684 | 1.153–2.657 | 0.03 * |
| Triradiate cartilage | 1.719 | 1.165–3.475 | 0.02 * |
| Risser grade | 1.518 | 0.872–2.914 | 0.04 * |
| Menarche | 1.894 | 1.243–3.576 | 0.03 * |
| Idiopathic diagnosis | 3.982 | 2.771–4.956 | 0.008 * |
| AIS | 2.365 | 1.917–3.867 | 0.01 * |
| Mean Score | Range | Yes | No | |
|---|---|---|---|---|
| - | 109 | 0 | |
| 9 | 100 | ||
| 4.8 | 3–5 | - | - |
| 4.9 | 3–5 | - | - |
| 4.9 | 4–5 | - | - |
| 4.8 | 3–5 | - | - |
| 4.6 | 3–5 | - | - |
| 3.1 | 0–5 | - | - |
| 2.0 | 0–5 | - | - |
| 4.6 | 1–5 | - | - |
| 4.5 | 3–5 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsirikos, A.I.; Adam, R.; Sutters, K.; Fernandes, M.; García-Martínez, S. Effectiveness of the Boston Brace in the Treatment of Paediatric Scoliosis: A Longitudinal Study from 2010–2020 in a National Spinal Centre. Healthcare 2023, 11, 1491. https://doi.org/10.3390/healthcare11101491
Tsirikos AI, Adam R, Sutters K, Fernandes M, García-Martínez S. Effectiveness of the Boston Brace in the Treatment of Paediatric Scoliosis: A Longitudinal Study from 2010–2020 in a National Spinal Centre. Healthcare. 2023; 11(10):1491. https://doi.org/10.3390/healthcare11101491
Chicago/Turabian StyleTsirikos, Athanasios I., Rachel Adam, Kirsty Sutters, Maureen Fernandes, and Silvia García-Martínez. 2023. "Effectiveness of the Boston Brace in the Treatment of Paediatric Scoliosis: A Longitudinal Study from 2010–2020 in a National Spinal Centre" Healthcare 11, no. 10: 1491. https://doi.org/10.3390/healthcare11101491