
The Voice of Patients Really Matters: Using Patient-Reported Outcomes and Experiences Measures to Assess Effectiveness of Home-Based Integrated Care—A Scoping Review of Practice

Abstract
:1. Introduction
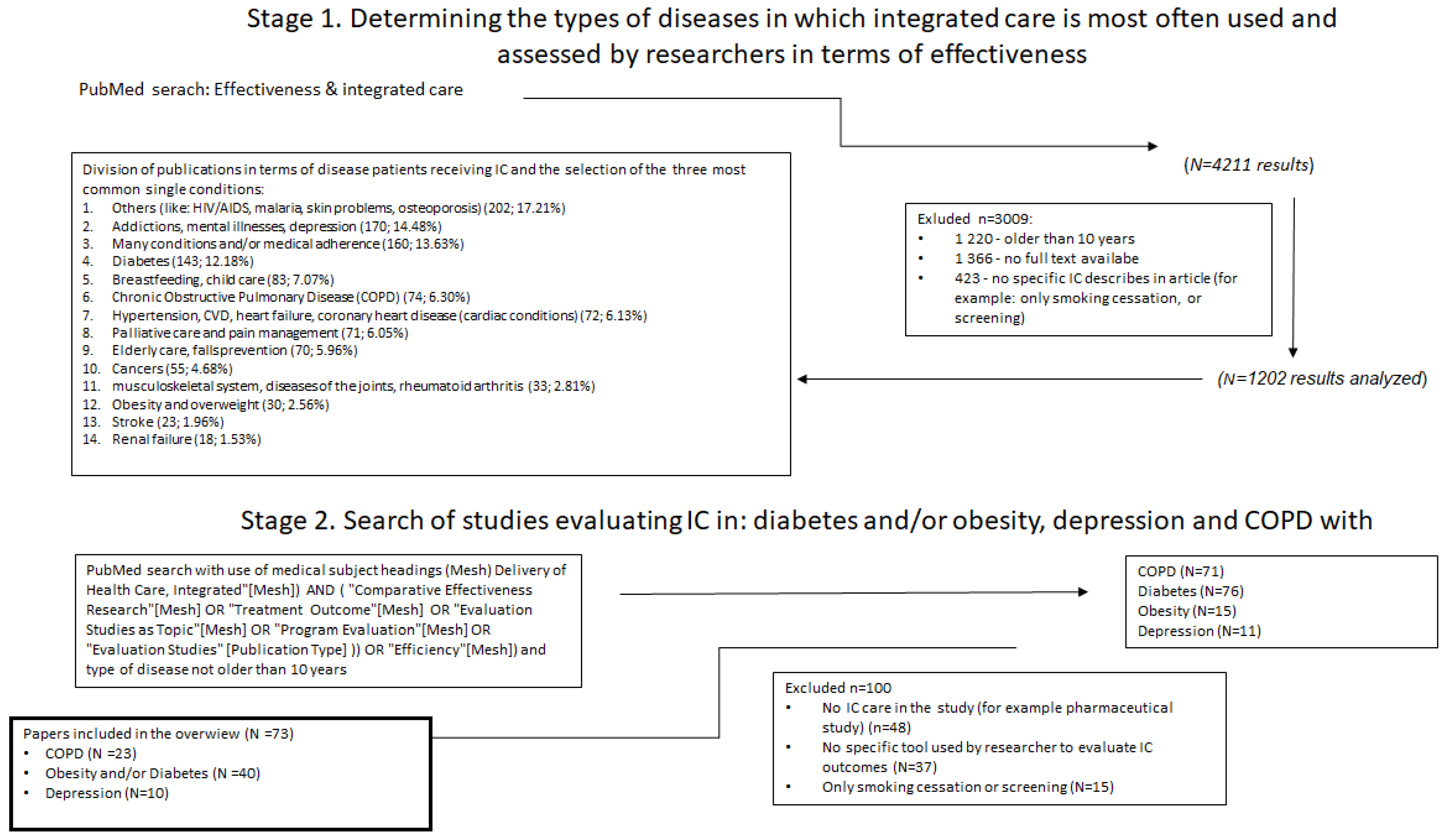
2. Material and Methods
- What types of PROMs and PREMs are used to describe the effectiveness of IC programs? Are there differences in the use of PROMs and PREMs depending on the type of disease and the country?
- 2.
- The patients suffering from one of three chronic diseases: COPD, obesity/diabetes or depression, who received integrated care.
- 3.
- The intervention discussed was integrated care, which was assessed by researchers in terms of its effectiveness.
3. Results
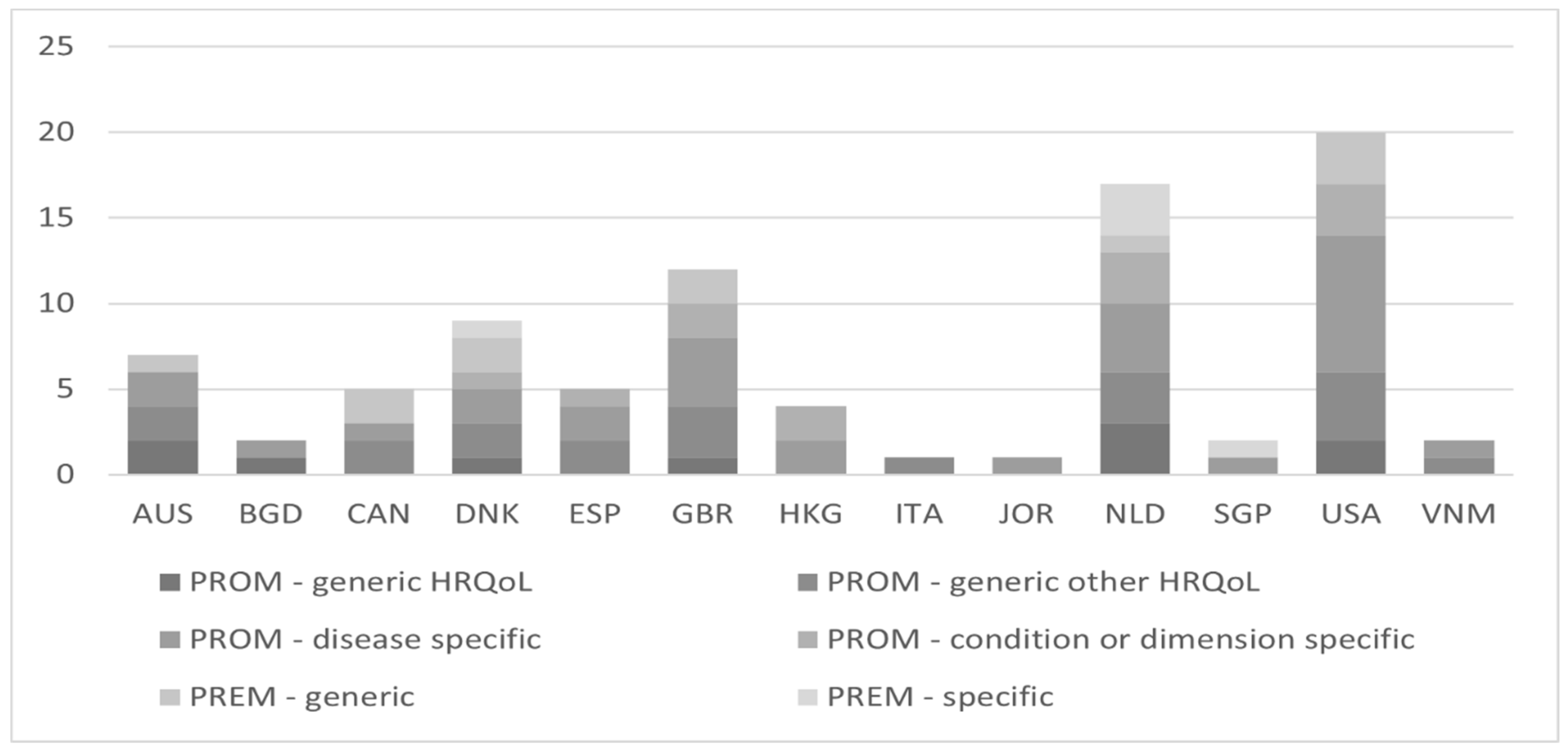
3.1. General Characteristics of the Studies
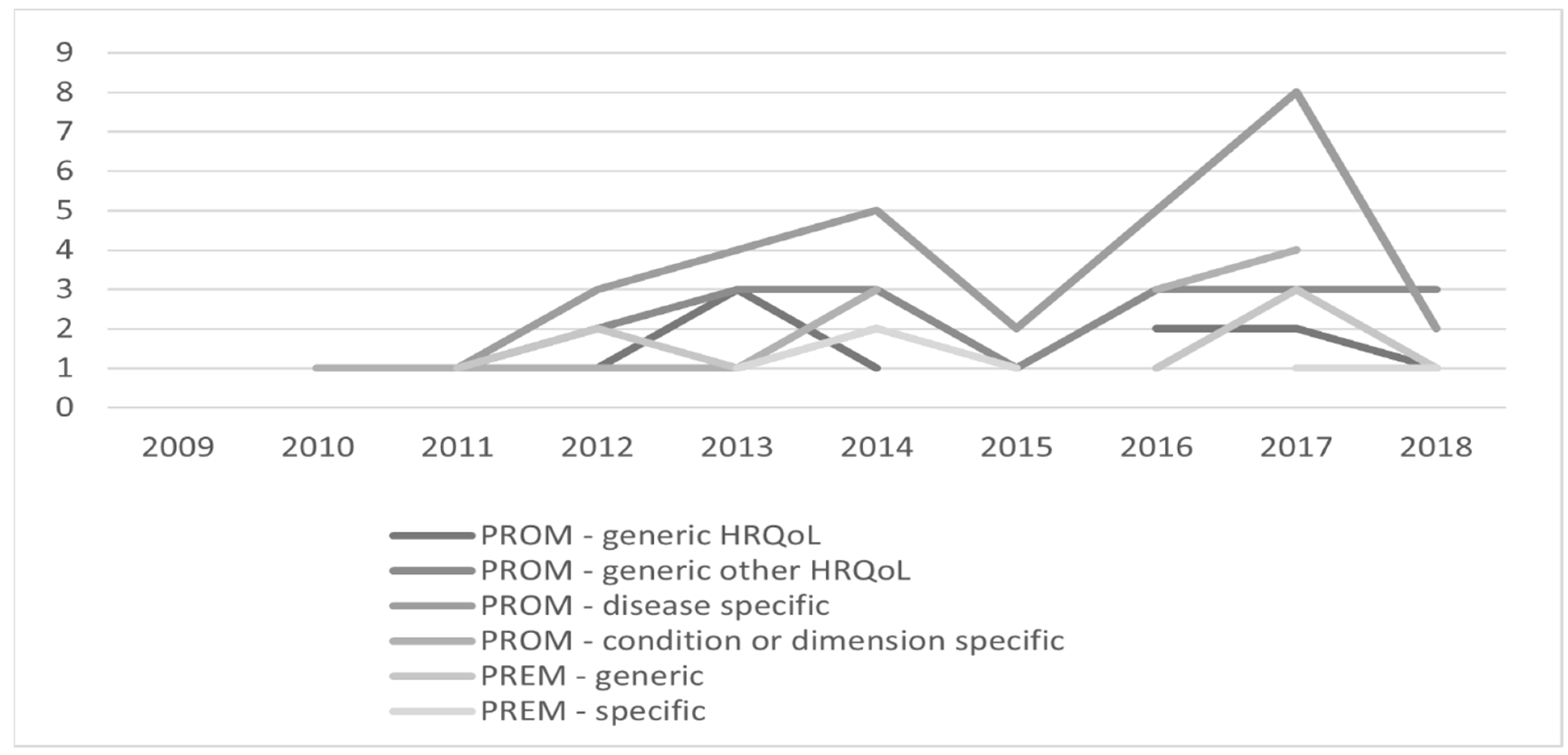
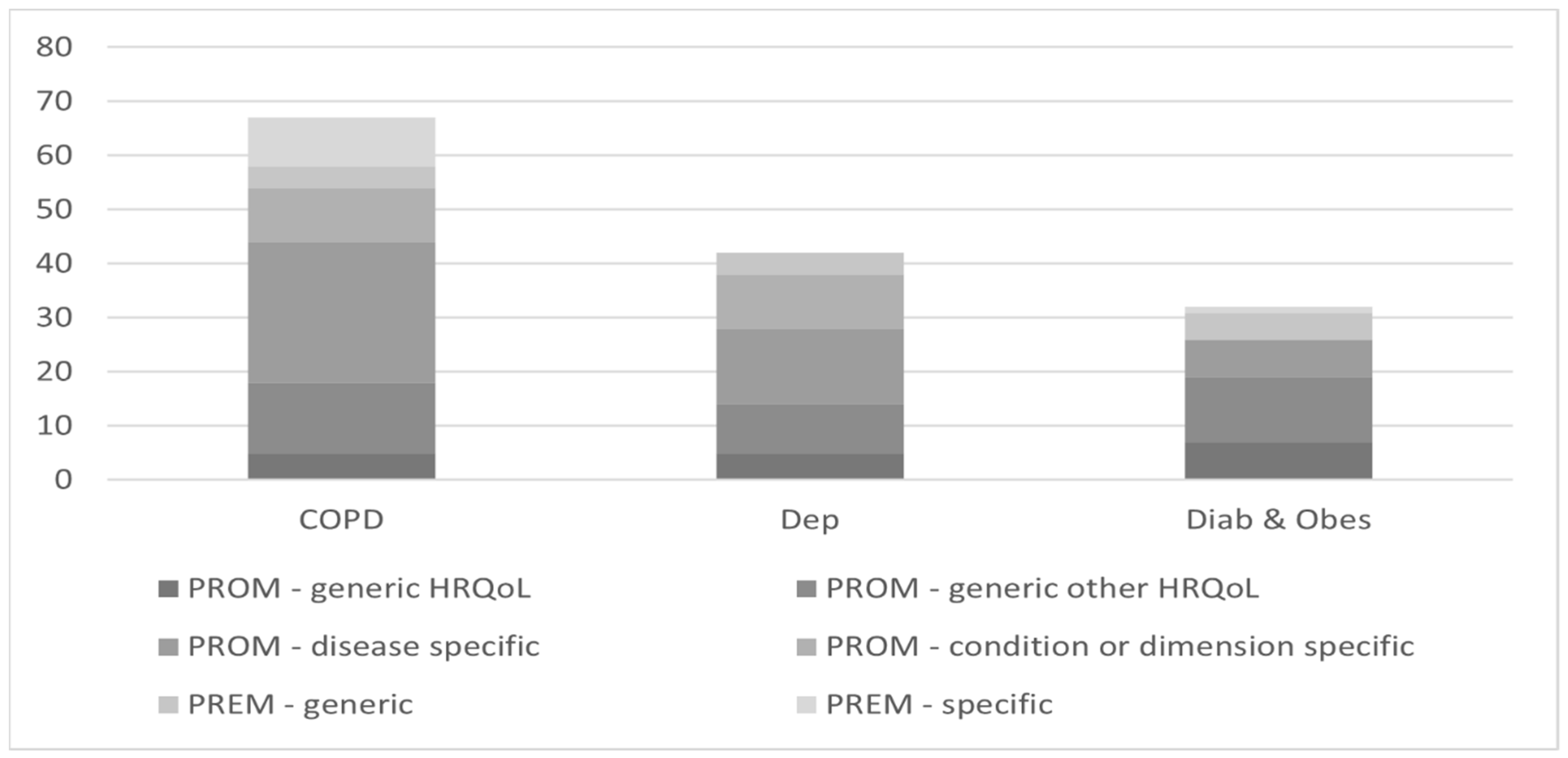
3.2. Outcomes Measures Used in Studies
3.3. PROMs and PREMs in Evaluation of IC
4. Discussion
5. Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
References
- EUnetHTA. Endpoints Used for Relative Effectiveness Assessment of Pharmaceuticals: Clinical Endpoints. Available online: https://www.eunethta.eu/wp-content/uploads/2018/01/Clinical-endpoints.pdf2015 (accessed on 30 April 2021).
- Field, J.; Holmes, M.M.; Newell, D. PROMs data: Can it be used to make decisions for individual patients? A narrative review. Patient Relat. Outcome Meas. 2019, 10, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Organisation for Economic Co-Operation and Development. Measuring What Matters: The Patient-Reported Indicator Surveys. Available online: https://www.oecd.org/health/health-systems/Measuring-what-matters-the-Patient-Reported-Indicator-Surveys.pdf2019 (accessed on 14 December 2022).
- Goodwin, N. Understanding Integrated Care. Int. J. Integr. Care 2016, 16, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contandriapoulos, A.P.; Denis, J.L.; Touati, N.; Rodriguez, C. The integration of health care: Dimensions and implementation. In Groupe de Recherche Interdisciplinaire en Santé; Working Paper N04–01; Université de Montréal: Montréal, QC, Canada, 2003. [Google Scholar]
- Lemmens, L.C.; Molema, C.C.; Versnel, N.; Baan, C.A.; de Bruin, S.R. Integrated care programs for patients with psychological comorbidity: A systematic review and meta-analysis. J. Psychosom. Res. 2015, 79, 580–594. [Google Scholar] [CrossRef] [PubMed]
- Weldring, T.; Smith, S.M. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv. Insights 2013, 6, 61–68. [Google Scholar]
- Williams, K.; Sansoni, J.; Morris, D.; Grootemaat, P.; Thompson, C. Patient-reported outcome measures. Literature review. Aust. Comm. Saf. Qual. Health Care 2016. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/PROMs-Literature-Review-December-2016.pdf (accessed on 1 December 2022).
- Desomer, A.; van den Heede, K.; Triemstra, M.; Paget, J.; De Boer, R.; Kohn, L.; Cleemput, I. Use of Patient-Reported Outcome and Experience Measures in Patient Care and Policy–Short report. Health Services Research (HSR) Brussels: Belgian Health Care Knowledge Centre (KCE). 2018. Available online: https://kce.fgov.be/en/use-of-patient-reported-outcome-and-experience-measures-in-patient-care-and-policy (accessed on 15 April 2021).
- Fitzpatrick, R.; Davey, C.; Buxton, M.; Jones, D. Evaluating patient-based outcome measures for use in clinical trials. Health Technol. Asses. 1998, 14, 74. [Google Scholar] [CrossRef] [Green Version]
- Doyle, C.; Lennox, L.; Bell, D. A systematic review of evidenceon the links between patient experienceand clinical safety and effectiveness. BMJ Open 2013, 3, 21–29. [Google Scholar] [CrossRef]
- Bandurska, E.; Ciećko, W.; Zarzeczna-Baran, M. Wykorzystanie wskaźników efektywności pochodzących od pacjentów w opiece zdrowotnej. [Use of patient-reported outcomes measures in healthcare]. Bezpieczeństwo Pacjentów I Pers. Med. 2019, 3, 226–231. [Google Scholar]
- Valderas, J.M.; Kotzeva, A.; Espallargues, M.; Guyatt, G.; Ferrans, C.; Halyard, M.Y.; Revicki, D.A.; Symonds, T.; Parada, A.; Alonso, J.; et al. The impact of measuring patient-reported outcomes in clinical practice: A systematic review of the literature. Qual. Life Res. 2008, 17, 179–193. [Google Scholar] [CrossRef]
- Griggs, C.; Schneider, J.; Kazis, L.; Ryan, C. Patient-reported outcome measures a stethoscope for the patient history. Ann. Surg. 2017, 265, 1066–1067. [Google Scholar] [CrossRef]
- Steuten, L.; Vrijhoef, B.; Severens, H.; van Merode, F.; Spreeuwenberg, C. Are we measuring what matters in health technology assessment of disease management? Systematic literature review. Int. J. Technol. Assess 2006, 22, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Gutierrez, R.; McCoy, R. Measuring What Matters in Diabetes. JAMA 2019, 21, 1865–1866. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, J.; Meadows, K. The effectiveness of the use of patient-based measures of health in routine practice in improving the process and outcomes of patient care: A literature review. J. Eval. Clin. Pr. 1999, 5, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Solberg, L.; Asche, S.; Butler, J.; Carrell, D.; Norton, C.; Jarvik, J.; Smith-Bindman, R.; Tillema, J.; Whi, R. It Is Time to Ask Patients What Outcomes Are Important to Them. Am. J. Acc. Care 2015, 4, 48–54. [Google Scholar]
- Afolabi, G.; Stevens, R.; Turner, M.; Harvey, M.; Norman, L.; Dogan, S.; Gray, W. Development of a Pulmonary Rehabilitation Service for People With COPD. A tiered model of integrated care. J. Cardiopulm. Rehabil. Prev. 2013, 13, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Alshabanat, A.; Otterstatter, M.; Sin, D.; Rempel, C.; van Eeden, S.; FitzGerald, J. Impact of a COPD comprehensive case management program on hospital length of stay and readmission rates. Int. J. Chronic Obstr. Pulm. Dis. 2017, 21, 961–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balaban, R.; Zhang, F.; Vialle-Valentin, C.; Galbraith, A.; Burns, M.; Larochelle, M.; Ross-Degan, D. Impact of a Patient Navigator Program on Hospital-Based and Outpatient Utilization Over 180 Days in a Safety-Net Health System. J. Gen. Intern. Med. 2017, 32, 981–989. [Google Scholar] [CrossRef]
- Carron, T.; Bridevaux, P.; Lörvall, K.; Parmentier, R.; Moix, J.; Beytrison, V.; Pernet, R.; Rey, C.; Roberfroid, P.; Chhajed, P.; et al. Feasibility, acceptability and effectiven ess of integrated care for COPD patients: A mixed methods evaluation of a pilot community-based programme. Swiss Med. Wkly. 2017, 147, w14567. [Google Scholar]
- Henoch, I.; Strang, S.; Löfdahl, C.; Ekberg-Jansson, A. Management of COPD, equal treatment across age, gender, and social situation? A register study. Int. J. Chronic Obs. 2016, 11, 2681–2690. [Google Scholar] [CrossRef] [Green Version]
- Davis, E.; Marra, C.; Gamble, J.; Farrell, J.; Lockyer, J.; FitzGerald, M.; Abu-Ashour, W.; Gillis, C.; Hawboldt, J. Effectiveness of a pharmacist-driven intervention in COPD (EPIC): Study protocol for a randomized controlled trial. Trials 2016, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Esteban, C.; Moraza, J.; Iriberri, M.; Aguirre, U.; Goiria, B.; Quintana, J.; Aburto, M.; Capelastegiu, A. Outcomes of a telemonitoring-based program (telEPOC) in frequently hospitalized COPD patients. Int. J. Chronic Obstr. 2016, 11, 2919–2930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillis, D.; Demmons, J.; Rocker, G. Expanding the INSPIRED COPD Outreach Program™ to the emergency department: A feasibility assessment. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1597–1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garner, A.; Hodson, M.; Ketsetzis, G.; Pulle, L.; Yorek, J.; Bhowmik, A. An analysis of the economic and patient o utcome impact of an integrated COPD service in east London. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1653–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, C.; Alonso, A.; Garcia-Aymerich, J.; Serra, I.; Marti, D.; Rodriguez-Roisin, R.; Narsavage, G.; Gomez, M.; Roca, J. Effectiveness of community-based integrated care in frail COPD patients: A randomised controlled trial. Int. J. Chronic Obstr. Pulm. Dis. 2015, 25, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Hogg, L.; Garrod, R.; Thorton, H.; McDonnell, L.; Bellas, H.; White, P. Effectiveness, Attendance, and Completion of an Integrated, System-Wide Pulmonary Rehabilitation Service for COPD: Prospective Observational Study. COPD: J. Chronic Obstr. Pulm. Dis. 2012, 9, 546–554. [Google Scholar] [CrossRef]
- Jain, V.; Allison, R.; Beck, S.; Jain, R.; Mills, P.; McCurley, S. Van Gundy, K.; Peterson, M. Impact of an integrated disease management program in reducing exacerbations in patients with severe asthma and COPD. Respir. Med. 2014, 108, 1794–1800. [Google Scholar] [CrossRef] [Green Version]
- Jarab, A.; AlQudah, S.; Khdour, M.; Shamssain, M.; Mukattash, T. Impact of pharmaceutical care on health outcomes in pati ents with COPD. Int. J. Clin. Pharm. 2012, 34, 53–62. [Google Scholar] [CrossRef]
- Ko, F.; Ngai, J.; Ng, S.; Chang, K.; Cheung, R.; Leung, M.; Pun, M.; Hui, D. COPD care programme can reduce readmissions and in-patient bed days. Respir. Med. 2014, 108, 1771–1778. [Google Scholar] [CrossRef] [Green Version]
- Ko, F.; Cheung, R.; Rainer, T.; Lum, C.; Wong, I.; Hui, D. Comprehensive care programme for patients with chronic obstructive pulmonary disease:a randomised controlled trial. Thorax 2017, 72, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Koolen, E.; van der Wees, G.; Dekhuijzen, R.; Heijdra, Y.; van Hul, A. Evaluation of the COPDnet integrated care model in patients with COPD: The study protocol. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2237–2244. [Google Scholar] [CrossRef] [Green Version]
- Kruis, A.; Boland, M.; Assendelft, W.; Gussekloo, J.; Tsiachristas, A.; Stijnen, T.; Blom, C.; Sont, J.; Rutten-van Mölken, M.; Chavannes, N. Effectiveness of integrated disease management for primary care chronic obstructive pulmonary disease patients: Results of cluster randomised trial. BMJ 2014, 349, g5392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruis, A.; von Adrichem, J.; Erkelens, M.; Scheepers, H.; Veen, H.; Muris, J.; Chavannes, N. Sustained effects of integrated COPD management on health status and exercise capacity in primary care patients. Int. J. Chronic Obstr. Pulm. Dis. 2010, 5, 407–413. [Google Scholar]
- Luk, E.; Hutchinson, A.; Tacey, M.; Irving, L.; Khan, F. COPD: Health Care Utilisation Patterns with Different Disease Management Interventions. Lung 2017, 195, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Pinnock, H.; Hanley, J.; McCloughan, L.; Todd, A.; Krishan, A.; Lewis, S.; Stoddart, A.; van del Pol, M.; MacNee, A.; Sheikh, A.; et al. Effectiveness of telemonitoring integrated into existing clinical services on hospital admission for exacerbation of chronic obstructive pulmonary disease: Researcher blind, multicentre, randomised controlled trial. BMJ 2013, 347, f6070. [Google Scholar] [CrossRef] [Green Version]
- Titova, E.; Steinshamn, S.; Indredavik, B.; Henriksen, A. Long term effects of an integrated care intervention on hospital utilization in patients with severe COPD: A single centre controlled study. Respir. Res. 2015, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Tan, W.; See, R.; Yu, W.; Kwek, L.; Toh, M.; Chee, T.; Chua, S. A matched-group study protocol to evaluate the implementation of an Integrated Care Pathway programme for chronic obstructive pulmonary disease in Singapore. BMJ Open 2015, 5, e005655. [Google Scholar] [CrossRef]
- Aponte, J.; Jackson, T.; Wyka, K.; Ikechi, C. Health effectiveness of community health workers as a diabetes self-management intervention. Diabetes Vasc. Dis. Res. 2017, 14, 316–326. [Google Scholar] [CrossRef] [Green Version]
- Barcelo, A.; Cafiero, E.; de Boer, M.; Mesa, A.; Lopez, M.; Jimenez, R.; Esqueda, A.; Martinez, J.; Holgiun, E.; Meiners, M.; et al. Using collaborative learning to improve diabetes care and outcomes: The VIDA project. Prim. Care Diabetes 2010, 4, 145–153. [Google Scholar] [CrossRef]
- Beauregard, M.; Provost, S.; Pineault, R.; Grimard, D.; Perez, J.; Fournier, M. Effects on patients of variations in the implementation of a cardiometabolic risk intervention program in Montréal. Health Promot. Chronic Dis. Prev. Can. Res. 2018, 2, 64–77. [Google Scholar] [CrossRef] [Green Version]
- Benedict, A.; Spence, M.; Sie, J.; Chin, H.; Ngo, C.; Salmingo, J.; Vidaurreta, A.; Rashid, N. Evaluation of a Pharmacist-Managed Diabetes Program in a Primary Care Setting Within an Integrated Health Care System. J. Manag. Care Spec. Pharm. 2018, 24, 114–122. [Google Scholar] [CrossRef]
- Chen, S.; Hou, X.; Sun, Y.; Hu, G.; Zhou, X.; Xue, H.; Chen, P.; Wu, J.; Bao, Y.; Jia, W. A seven-year study on an integrated hospital-community diabetes management program in Chinese patients with diabetes. Prim. Care Diabetes 2018, 12, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Chwastiak, J.; Jackson, S.; Russo, J.; Kiefer, M.; Belyeu, B.; Mertens, K.; Chew, L.; Lin, E. A collaborative care team to integrate behavioral health care and treatment of poorly-controlled type 2 diabetes in an urban safety net primary care clinic. Gen. Hosp. Psychiatry 2017, 44, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.; Aquilino, A.; Cortese, F.; Scicchitano, P.; Sassara, P.; Mola, E.; Rollo, R.; Caldarola, P.; Giorgino, F.; Pomo, V.; et al. Feasibility and effectiveness of a disease and care management model in the primary health care system for patients with heart failure and diabetes (Project Leonardo). Vasc. Health Risk Manag. 2010, 6, 297–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva Marinhoa, M.; Fontbonneb, A.; Mary, J.; Barbosaa, V.; de Melo Rodriguesc, H.; de Carvalhoa, E.; de Souza, W.V.; Cesse, E.A. The impact of an intervention to improve diabetes management in primary healthcare professionals’ practices in Brazil. Prim. Care Diabetes 2017, 11, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Fottrell, E.; Jennings, H.; Kuddus, A.; Ahmed, N.; Morrison, J.; Akter, K.; Shaha, S.; Nahar, B.; Nahar, T.; Haghparast-Bidgoli, H.; et al. The effect of community groups and mobile phone messages on the prevention and control of diabetes in rural Bangladesh: Study protocol for a three-arm cluster randomised controlled trial. Trials 2016, 17, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gucciardi, E.; Fortugno, M.; Horodezny, S.; Lou, W.; Sidani, S.; Espin, S.; Webster, F.; Shah, B. Will Mobile Diabetes Education Teams (MDETs) in primary care improve patient care processes and health outcomes? Study pprotocol for a randomized controlled trial. Trials 2012, 13, 1–10. [Google Scholar] [CrossRef]
- Harris, M.; Breaves, F.; Patterson, S.; Jones, J.; Pappas, Y.; Majeed, A.; Car, J. The North West London Integrated Care Pilot Innovative Srategies to Improve Care Coordination for Older Adults and People With Diabetes. J. Ambul. Care Manag. 2012, 35, 216–225. [Google Scholar] [CrossRef]
- Huckfeldt, P.; Meeker, D.; Peters, A.; Guterman, J.; Diaz, G.; Goldman, D. Diabetes Management for Low-Income Patients In Los Angeles: Two Strategies Improved Disease Control In The Short Term. Health Aff. 2012, 31, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Huque, R.; Nasreen, S.; Ahmed, F.; Hicks, J.; Walley, J.; Newell, J.; Elsey, H. Integrating a diabetes and hypertension case management package within primary health care: A mixed methods feasibility study in Bangladesh. BMC Health Serv. Res. 2018, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Husted, G.; Thorsteinsson, B.; Esbensen, B.; Gluud, C.; Winkel, P.; Hommel, E.; Elsey, H. Effect of guided self-determination youth intervention integrated into outpatient visits versus treatment as usual on glycemic control and life skills: A randomized clinical trial in adolescents with type 1 diabetes. Trials 2014, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Jansink, R.; Braspenning, J.; Keizer, E.; Van der Weijden, T.; Elwyn, G.; Grol, R. No identifiable Hb1Ac or lifestyle chang e after a comprehensive diabetes programme including motivational interviewing: A cluster randomised trial. Scand. J. Prim. Health 2013, 31, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, I.; Pirabhahar, S.; Williamson, P.; Raghunath, V.; Brennan, F.; O'Sullivan, A.; Youssef, G.; Lane, C.; Jacobson, G.; Feldman, P.; et al. Connect CKD-virtual medical consulting: A web-based chronic kidney disease, hypertension and diabetes integrated care program. Nephrology 2018, 23, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Kornelius, E.; Chiou, J.; Yang, Y.; Lu, Y.; Peng, C.; Huang, C. The Diabetes Shared Care Program and Risks of Cardiovascular Events in Type 2 Diabetes. Am. J. Med. 2015, 128, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Ku, G.; Kegels, G. Integrating chronic care with primary care activities: Enriching healthcare staff knowledge and skills and improving glycemic control of a cohort of people with diabetes through the First Line Diabetes Care Project in the Philippines. Glob. Health Action 2014, 7, 25286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Labhardt, N.; Balo, J.; Ndam, M. Task shifting to non-physician clinicians for integrated management of hypertension and diabetes in rural Cameroon: A programme assessment at two years. BMC Health Serv. Res. 2010, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liddy, C.; Johnston, S.; Nash, K.; Ward, N.; Irving, H. Health coaching in primary care: A feasibility model for diabetes care. BMC Prim. Care 2014, 15, 1–8. [Google Scholar] [CrossRef]
- Lien, A.; Jiang, Y.; Mou, C.; Sun, M.; Gau, B.; Yen, H. Integrative traditional Chinese medicine therapy reduces the risk of diabetic ketoacidosis in patients with type 1 diabetes mellitus. J. Ethnopharmacol. 2016, 191, 324–330. [Google Scholar] [CrossRef]
- MacRury, S.; Stephen, K.; Main, F.; Gorman, J.; Jones, S.; Macfarlane, D. Reducing Amputations in People with Diabetes (RAPID): Evaluation of a New Care Pathway. Int. J. Environ. Res. Public Health 2018, 15, 999. [Google Scholar] [CrossRef] [Green Version]
- Newlyn, N.; MaGrath, R.; Fulcher, G. Evaluation of the performance and outcomes for the first year of a diabetes rapid access clinic. Med. J. Aust. 2016, 205, 172. [Google Scholar] [CrossRef]
- Salant, T.; Slavin, S.; Baumrin, E.; Bordeu, M.; Rowley, M.; Brackett, E.; Severin, P.; Behforouz, H. Lessons in Translation Insights From a Collaboration Integrating Community Health Workers Into Diabetes Care. J. Ambul. Care Manag. 2013, 36, 156–165. [Google Scholar] [CrossRef]
- Seidu, S.; Bodicoat, D.; Davies, M.; Daly, H.; Stribling, B.; Farooqi, A.; Brady, E.; Khunti, K. Evaluating the impact of an enhanced primary care diabetes service on diabetes outcomes: A before–after study. Prim. Care Diabetes 2017, 11, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Turnacilar, M.; Sancar, M.; Apikoglu-Rabus, S.; Hursitoglu, M.; Izzettin, F. Improvement of diabetes indices of care by a short pharmaceutical care program. Pharm. World Sci. 2009, 31, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Rümenapf, G.; Geiger, S.; Schneider, B.; Amendt, K.; Wilhelm, N.; Morbach, S.; Nagel, N. Readmissions of patients with diabetes mellitus and foot ulcers after infra-popliteal bypass surgery–attacking the problem by an integrated case management model. Vasa 2013, 42, 56–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermunt, P.; Milder, I.; Wielaard, F.; Baan, C.; Schelfhout, J.; Westert, G.; van Oers, H. Implementation of a lifestyle intervention for type 2 diabetes prevention in Dutch primary care: Opportunities for intervention delivery. BMC Fam. Pract. 2012, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.; Harris, B.; Roberts, A. Evaluation of a community diabetes initiative: Integrating diabetes. Prim. Care Diabetes 2015, 9, 203–210. [Google Scholar] [CrossRef]
- Webb, E.; Rheeder, P. A cluster-randomized trial to estimate the effect of mobile screening and treatment feedback on HbA1c and diabetes-related complications in Tshwane primary health care clinics, South Africa. Prim. Care Diabetes 2017, 11, 546–554. [Google Scholar] [CrossRef]
- Yang, G.; Yuan, S.; Fu, H.; Wan, G.; Zhu, L.; Yuan, M.; Lv, Y.; Zhang, J.; Du, X.; Li, Y.; et al. Influence of educational attainments on long term glucose control and morbid events in patients with type 2 diabetes receiving integrated care from 15 China urban communities: The Beijing Community Diabetes Study 11. Prim. Care Diabetes 2015, 9, 473–481. [Google Scholar] [CrossRef]
- Zhang, J.; Burridge, L.; Baxter, K.; Donald, M.; Foster, M.; Hollingworth, S.; Ware, R.; Russell, A.; Lackson, C. A new model of integrated p rimary-secondary care for complex diabetes in the community: Study protocol for a randomised controlled trial. Trials 2013, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bennett, W.; Gadzune, K.; Appel, L.; Clark, J. Insights from the POWER Practice-Based Weight Loss Trial: A Focus Group Study on the PCP’s Role in Weight Management. J. Gen. Intern. Med. 2013, 29, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Brunisholz, K.; Joy, E.; Hashibe, M.; Gren, L.; Savitz, L.; Hamilton, S.; Cannon, W.; Huynh, K.; Schafer, T.; Newman, L.; et al. Stepping Back to Move Forward: Evaluating the Effectiveness of a Diabetes Prevention Program Within a Large Integrated Healthcare Delivery System. J. Healthc. Qual. 2017, 39, 278–293. [Google Scholar] [CrossRef]
- Van Eeghen, C.; Littenberg, B.; Kessler, R. Chronic care coordination by integrating care through a team-based, population-driven approach: A case study. Transl. Behav. Med. 2018, 8, 468–480. [Google Scholar] [CrossRef]
- Gross, S.; Augustyn, M.; Henderson, J.; Baig, K.; Williams, C.; Ajao, B.; Bell-Waddy, P.; Paige, D. Integrating Obstetrical Care and WIC Nutritional Services to Address Maternal Obesity and Postpartum Weight Retention. Matern. Child. Health J. 2018, 22, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.; Frerichs, L.; Story, M.; Jones, J.; Gaskin, K.; Apple, A.; Skinner, A.; Armstrong, S. An Integrated Clinic-Community Partnership for Child Obesity Treatment: A Randomized Pilot Trial. Pediatrics 2018, 141, 1. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.; Jastrzab, R.; Tate, J.; Johnson, K.; Hall-Lipsy, E.; Martin, R.; Taylor, A.; Warholak, T. Evaluation of an Academic-Community Partnership to Implement MTM Services in Rural Communities to Improve Pharmaceutical Care for Patients with Diabetes and/or Hypertension. J. Manag. Care Spec. Pharm. 2018, 24, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Prestes, M.; Gayarre, M.; Elgart, J.; Gonzalez, L.; Rucci, E.; Gagliardino, J. Multistrategic approach to improve quality of care of people with diabetes at the primary care level: Study design and baseline data. Prim. Care Diabetes 2017, 11, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Wake, M.; Lycett, K.; Sabin, M.; Gunn, J.; Gibbons, K.; Hutton, C.; McCallum, Z.; York, E.; Stringer, M.; Wittert, G. A shared-care model of obesity treatment for 3–10 year old children: Protocol for the HopSCOTCH randomised controlled trial. BMC Pediatr. 2012, 12, 1–9. [Google Scholar] [CrossRef]
- Angstman, K.; Doganer, Y.; Dejesus, R.; Rohrer, J. Increased medical cost metrics for patients 50 years of age and older in the collaborate care model of treatment for depression. Psychogeriatrics 2016, 16, 102–106. [Google Scholar] [CrossRef]
- Unützer, J.; Chan, Y.; Hafer, E.; Knaster, J.; Shields, A.; Powers, D.; Veith, R. Quality Improvement with Pay-for-Performance Incentives in In tegrated Behavioral Health Care. Am. J. Public Health 2012, 102, e41–e45. [Google Scholar] [CrossRef]
- Hepner, K.; Hunter, S.; Paddock, S.; Zhou, A.; Watkins, K. Training Addiction Counselors to Implement CBT for Depression. Adm. Policy Ment. Health Ment. Health Serv. Res. 2011, 38, 313–323. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.; Goldsmith, C.; Jones, W.; Oanh, P.; Nguyen, V. The effectiveness of a Supported Self-management task-shifting intervention for adult depression in Vietnam communities: Study protocol for a randomized controlled trial. Trials 2017, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Poulsen, R.; Hoff, A.; Fisker, J.; Hjorthøj, C.; Eplov, L. Integrated mental health care and vocational rehabilitation to improve retu rn to work rates for people on sick leave because of depression and anxiety (the Danish IBB IS trial): Study protocol for a randomized controlled trial. Trials 2017, 18, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Salisbury, C.; O’Cathain, A.; Edwards, L.; Thomas, C.; Gaunt, D.; Hollinghurst, S.; Nicholl, J.; Large, S.; Yardley, L.; Lewis, G.; et al. Effectiveness of an integrated telehealth service for patients with depression: A pragmatic randomised controlled trial of a complex intervention. Lancet Psychiatry 2016, 3, 515–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, K.; Eghaneyan, B.; Killian, M.; Cabassa, L.; Trivedi, M. Measurement, Education and Tracking in Integrated Care (METRIC): Use of a culturally adapted education tool versus standard education to increase engagement in depression treatment among Hispanic patients: Study protocol for a randomized control trial. Trials 2017, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Von Korff, M.; Katon, W.; Lin, E.; Ciechanowski, P.; Peterson, D.; Ludman, E.; Young, B.; Rutter, C. Functional outcomes of multi-condition collaborative care and successful ageing: Results of randomised trial. BMJ 2014, 343. [Google Scholar] [CrossRef] [Green Version]
- Wagner, G.; Ngo, V.; Glick, P.; Obuku, E.; Musisi, S.; Akena, D. INtegration of DEPression Treatment into HIV Care i n Uganda (INDEPTH-U ganda): Study protocol for a randomized controlled trial. Trials 2014, 15, 343. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Haomiao, J.; Vidyanti, I.; Lee, P.; Eli, K.; Wu, S. Collaborative Depression Care Among Latino Patients in Diabetes Disease Management, Los Angeles, 2011–2013. Prev. Chronic Dis. 2014, 11, E148. [Google Scholar] [CrossRef]
- Porter, M. Value-based health care delivery. Ann. Surg. 2008, 248, 503–509. [Google Scholar] [CrossRef]
- Morris, M.; Atkinson, V.; Woods, J.; Myles, P.; Hodge, A.; Jones, C.; Lloyd, D.; Rovtar, V.; Clifford, A.; Brusco, N. Patient Judgement of Change with Elective Surgery Correlates with Patient Reported Outcomes and Quality of Life. Healthcare 2022, 10, 999. [Google Scholar] [CrossRef]
- Gentry, S.; Badrinath, P. Defining Health in the Era of Value-based Care: Lessons from England of Relevance to Other Health Systems. Cureus 2017, 9, e1079. [Google Scholar] [CrossRef] [Green Version]
- Zipfel, N.; van der Nat, P.; Rensing, B.; Daeter, E.; Westert, G.; Groenewoud, A. The implementation of change model adds value to value-based healthcare: A qualitative study. BMC Health Serv. Res. 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Baxter, S.; Johnson, M.; Chambers, D.; Sutton, A.; Goyder, E.; Booth, A. The effects of integrated care: A systematic review of UK and international evidence. BMC Health Serv. Res. 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, S.; Damery, S.; Combes, G. The effectiveness of integrated care interventions in improving patient quality of life (QoL) for patients with chronic conditions. An overview of the systematic review evidence. Health Qual. Life Outcomes 2017, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bandurska, E.; Damps-Konstańska, I.; Popowski, P.; Jedrzejczyk, T.; Janowiak, P.; Swietnicka, K.; Zarzeczna-Baran, M.; Jassem, E. Cost-Effectiveness Analysis of Integrated Care in Management of Advanced Chronic Obstructive Pulmonary Disease (COPD). Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 2879–2885. [Google Scholar] [CrossRef] [PubMed]
- Lavallee, D.; Chenok, K.; Love, R.; Petersen, C.; Holve, E.; Segal, C.; Franklin, P. Incorporating Patient-Reported Outcomes into Health Care To Engage Patients And Enhance Care. Health Aff. 2016, 35, 575–582. [Google Scholar] [CrossRef]
- De Faoite, D. The advantages of electronic patient-reported measures and an example digital platform to collect ePROs after total knee arthroplasty. Med. Access Point Care 2018, 2. [Google Scholar] [CrossRef]
- OECD. Putting People at the Centre of Health Care. PaRIS Survey of Patients with Chronic Conditions. 2019. Available online: https://www.oecd.org/health/health-systems/PaRIS-survey-Patients-with-Chronic-Conditions-June-2019.pdf (accessed on 20 April 2022).
- Miedany, Y. Adopting patient-centered care in standard practice: PROMs moving toward disease-specific era. Clin. Exp. Rheumat. 2014, 32, S40–S46. [Google Scholar]
- Coelho, A.; de Bienassis, K.; Klazinga, N.; Santo, S.; Frade, P.; Costa, A.; Gaspar, T. Mental Health Patient-Reported Outcomes and Experiences Assessment in Portugal. Int. J. Env. Res. Public Health 2022, 19, 11153. [Google Scholar] [CrossRef]
- Hodson, M.; Andrew, S.; Roberts, C. Towards an understanding of PREMs and PROMs in COPD. Breathe 2013, 9, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Jayakumar, P.; Phil, D.; Teunis, T.; Vranceanu, A.; Lamb, S.; Ring, D.; Gwilym, S. Relationship Between Magnitude of Limitations and Patient Experience During Recovery from Upper-Extremity Fracture. JB JS Open Access 2019, 4, 1–7. [Google Scholar] [CrossRef]
- Black, N.; Varaganum, M.; Hutchings, A. Relationship between patient reported experience (PREMs) and patient reported outcomes (PROMs) in elective surgery. BMJ Qual. Saf. 2014, 23, 534–542. [Google Scholar] [CrossRef]
- Kingsley, C.; Patel, S. Patient-reported outcome measures and patient-reported experience measures. BJA Educ. 2017, 17, 137–144. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elements of IC | N | Percent |
|---|---|---|
| Education (incl. education for staff members), self-management, support after discharge | 56 | 76.7 |
| Community-based or home-based care, also a hospital community-based type of care | 35 | 47.9 |
| Support of additional specialists, multispecialty team | 35 | 47.9 |
| Treatment or action plan, treatment coordination, adherence | 35 | 47.9 |
| Others (for example, IT services, home oxygen service, smoking cessation) | 33 | 45.2 |
| Pulmonary rehabilitation | 12 | 52.2 * |
| Total Number of Instruments Used | N | Percent |
|---|---|---|
| <5 | 21 | 28.8 |
| 6 to 10 | 26 | 35.6 |
| 11 to 15 | 13 | 17.8 |
| 15 to 20 | 2 | 2.7 |
| >20 | 5 | 6.8 |
| n/a | 6 | 8.2 |
| Total | 73 | 100.0 |
| Author (First) | Year | Country (ISO 3166-1) | Population | Disease | PROMS | PREMS | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Generic | Disease Specific | Condition or Dimension Specific | Generic | Disease or Condition Specific | ||||||
| HRQoL | Other than HRQoL | |||||||||
| Afolabi [19] | 2013 | GBR | 199 | COPD | CRQ | |||||
| CAT | ||||||||||
| Carron [22] | 2017 | CHE | 57 | COPD | SF-36 | CAT | mMRC | PACIC | ||
| Number of COPD exacerbations reported by patients | ||||||||||
| CRQ | ||||||||||
| SEM-CD | ||||||||||
| Henoch [23] | 2016 | CHE | 7810 | COPD | Exercise capacity (Likert scale) | CCQ | mMRC | |||
| Davis [24] | 2016 | CAN | 140 | COPD | MMAS-8 | SGRQ | ||||
| Esteban [25] | 2016 | ESP | 119 | COPD | HADS | SGRQ | mMRC | |||
| LCADL | ||||||||||
| Gillis [26] | 2017 | CAN | 174 | COPD | CTM-3 | |||||
| Expectations (single open-ended question) | ||||||||||
| “Helpfulness” of care (Likert scale) | ||||||||||
| Garner [27] | 2017 | GBR | n/a | COPD | CAT | Place of death | ||||
| Hernandez [28] | 2015 | ESP | 155 | COPD | HADS | mMRC | ||||
| IADL | ||||||||||
| Hogg [29] | 2012 | GBR | 1114 | COPD | HADS | CRQ-SR | ||||
| Jarab [31] | 2012 | JOR | 106 | COPD | CSES | |||||
| SGRQ | ||||||||||
| Ko [32] | 2014 | HKG | 185 | COPD | SGRQ | mMRC | ||||
| Ko [33] | 2017 | HKG | 180 | COPD | SGRQ | mMRC | ||||
| Koolen [34] | 2018 | NLD | n/a | COPD | PAM | CCQ | CQIAC | |||
| MSQ | NCSI | CSPAM | ||||||||
| PCRS | ||||||||||
| CPSET | ||||||||||
| PACIC | ||||||||||
| Kruis [35] | 2014 | NLD | 1086 | COPD | EQ-5L | IPAQ | CCQ | mMRC | PACIC | |
| SF-36 | SMAS-30 | SGRQ | ||||||||
| Kruis [36] | 2010 | NLD | 1086 | COPD | EQ-5L | IPAQ | CCQ | mMRC | PACIC | |
| SF-36 | SMAS-30 | SGRQ | ||||||||
| Pinnock [38] | 2013 | GBR | 128 | COPD | HADS | SGRQ | ||||
| SECD-6 | ||||||||||
| LINQ | ||||||||||
| Wu [40] | 2015 | SGP | 62 | COPD | CAT | PACIC | ||||
| Aponte [41] | 2017 | USA | 180 | Diab and Obes | DKQ | |||||
| Beauregard [43] | 2018 | CAN | 1185 | Diab and Obes | Enquête québécoise sur l’activité physique et la santé | |||||
| Chwastiak [46] | 2017 | USA | 151 | Diab and Obes | PHQ-9 | |||||
| Ciccone [47] | 2010 | ITA | 1160 | Diab and Obes | SF-12 | |||||
| Fottrell [49] | 2016 | BGD | Diab and Obes | EQ-5L | SRQ | |||||
| Gucciardi [50] | 2012 | CAN | 1200 | Diab and Obes | Patients’ experiences and views (in-depth interviews) | |||||
| Husted [54] | 2014 | DNK | 71 | Diab and Obes | TSRQ-21 | PCD | HCCQ | PAID-20 | ||
| WHO5 | ||||||||||
| Jansink [55] | 2013 | NLD | 940 | Diab and Obes | VAS scale | |||||
| Vermunt [68] | 2012 | NLD | 925 | Diab and Obes | Satisfaction about program (Likert scale) | |||||
| Zhang [72] | 2013 | AUS | 456 | Diab and Obes | SF-12 | HADS | DQoL-brief | CSQ-8 | ||
| SMAS-30 | ||||||||||
| van Eeghen [75] | 2018 | USA | 20 | Diab and Obes | PHQ-9 | Satisfaction about program (Likert scale) | ||||
| Hoffman [77] | 2018 | USA | 97 | Diab and Obes | Sizing Me Up | FFQ | ||||
| IPAQ | ||||||||||
| PMI | ||||||||||
| PAQ | ||||||||||
| Wake [80] | 2012 | AUS | 120 | Diab and Obes | PedsQL | PCSC | BPQ | |||
| SDQ | ||||||||||
| Unützer [82] | 2012 | USA | 7977 | Dep | PHQ-9 | |||||
| Hepner [83] | 2011 | USA | 113 | Dep | Satisfaction about program (Likert scale) | |||||
| Murphy [84] | 2017 | VNM | n/a | Dep | WHODAS | SRQ-20 | ||||
| CAGE | ||||||||||
| Poulsen [85] | 2017 | DNK | n/a | Dep | EQ-5L | WSAS | BDI-II | PSS | CSQ-8 | |
| Flanagan QOLS | IPQ | BAI | KES | |||||||
| GSS | 4DSQ | RTW-SE | ||||||||
| SPS | ||||||||||
| Salisbury [86] | 2016 | GBR | 609 | Dep | EQ-5L | HeiQ | PHQ-9 | GAD-7 | Care coordination (Haggerty) | |
| MMAS-8 | ||||||||||
| eHEALs | ||||||||||
| Sanchez [87] | 2017 | USA | 11895 | Dep | PAQ | PHQ-9 | GAD-7 | |||
| DKM | SCMHC | |||||||||
| SD | LSAS | |||||||||
| Von Korff [88] | 2011 | USA | 214 | Dep | Quality of life (Likert scale) | WHODAS | SLC-20 | SDS | ||
| Wagner [89] | 2014 | USA | n/a | Dep | PHQ-9 | |||||
| MOS-HIV | ||||||||||
| Wu [90] | 2014 | USA | 964 | Dep | SF-12 | PHQ-9 | SDS | Satisfaction about program (Likert scale) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandurska, E. The Voice of Patients Really Matters: Using Patient-Reported Outcomes and Experiences Measures to Assess Effectiveness of Home-Based Integrated Care—A Scoping Review of Practice. Healthcare 2023, 11, 98. https://doi.org/10.3390/healthcare11010098
Bandurska E. The Voice of Patients Really Matters: Using Patient-Reported Outcomes and Experiences Measures to Assess Effectiveness of Home-Based Integrated Care—A Scoping Review of Practice. Healthcare. 2023; 11(1):98. https://doi.org/10.3390/healthcare11010098
Chicago/Turabian StyleBandurska, Ewa. 2023. "The Voice of Patients Really Matters: Using Patient-Reported Outcomes and Experiences Measures to Assess Effectiveness of Home-Based Integrated Care—A Scoping Review of Practice" Healthcare 11, no. 1: 98. https://doi.org/10.3390/healthcare11010098