
Diagnostic Performances of Ultrasound-Based Models for Predicting Malignancy in Patients with Adnexal Masses
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. IOTA-LR1 and IOTA-LR2
2.3. IOTA-ADNEX
2.4. IOTA Simple Rules
2.5. MIA2G Test
2.6. Reference Standard
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Chan, W.C.; Ngai, C.H.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.J.; Elcarte, E.; Withers, M.; et al. Worldwide Burden, Risk Factors, and Temporal Trends of Ovarian Cancer: A Global Study. Cancers 2022, 14, 2230. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Tiznobaik, A.; Taheri, S.; Salehiniya, H. Ovarian Cancer in the World: Epidemiology and Risk Factors. Int. J. Womens Health 2019, 11, 287–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of Ovarian Cancer: A Review. Cancer Biol. Med. 2017, 14, 9–32. [Google Scholar] [CrossRef] [Green Version]
- Cancer Stat Facts; SEER Ovarian Cancer: Bethesda, MD, USA, 2022.
- American College of Obstetricians and Gynecologists Committee Opinion No. 716: The Role of the Obstetrician-Gynecologist in the Early Detection of Epithelial Ovarian Cancer in Women at Average Risk. Obstet. Gynecol. 2017, 130, e146–e149. [CrossRef] [Green Version]
- Duran-Ranada, G.M.M.; Anzures, C.U. Diagnostic Accuracy Performance of the International Ovarian Tumour Analysis (IOTA) Simple Rules and Assessment of Different Neoplasias in the Adnexa (ADNEX) Model for Identifying Benign or Malignant Adnexal Masses against Histopathological Diagnosis in P. Philipp. J. Obstet. Gynecol. 2019, 43, 9–21. [Google Scholar]
- Gilarmeza, A.A. Diagnostic Performance of International Ovarian Tumor Analysis (IOTA) Simple Descriptors, Simple Rules and Sassone Scoring System among Patients with Ovarian Disease in a Tertiary Specialty Hospital. Philipp. J. Obstet. Gynecol. 2000, 42, 26–32. [Google Scholar]
- Morales, B.A.R.; Juan, F.S.S. A Retrospective Study on the Accuracy of Sassone, Lerner and IOTA Simple Rules in Determining Malignancy of Ovarian Masses in a Tertiary Hospital Ob-Gyn Ultrasound Diagnostics Unit. Philipp. J. Obstet. Gynecol. 2017, 41, 5–12. [Google Scholar]
- Espiritu-Concepcion, M.A.; Reforma, K.N. Comparative Study on the Diagnostic Accuracy of the Different International Ovarian Tumor Analysis (IOTA) Predictive Model in Discriminating between Benign and Malignant Ovarian New Growths: Logistic Regression 1 and 2 (LR1 and LR2) and Assessment of The. Philipp. J. Obstet. Gynecol. 2019, 43, 1–8. [Google Scholar]
- Velayo, C.L.; Reforma, K.N.; Sicam, R.V.G.; Diwa, M.H.; Sy, A.D.R.; Tantengco, O.A.G. Clinical Performance of a Multivariate Index Assay in Detecting Early-Stage Ovarian Cancer in Filipino Women. Int. J. Environ. Res. Public Health 2022, 19, 9896. [Google Scholar] [CrossRef]
- Velayo, C.L.; Reforma, K.N.; Sicam, R.V.G.; Diwa, M.H.; Sy, A.D.R.; Tantengco, O.A.G. Improving Diagnostic Strategies for Ovarian Cancer in Filipino Women Using Ultrasound Imaging and a Multivariate Index Assay. Cancer Epidemiol. 2022, 81, 102253. [Google Scholar] [CrossRef]
- Bullock, R.G.; Smith, A.; Munroe, D.G.; Ueland, F.R.; Goodrich, S.T.; Pappas, T.C.; Fredericks, T.I.; Bonato, V. Combining A Second-Generation Multivariate Index Assay with Ovarian Imaging Improves the Preoperative Assessment of An Adnexal Mass. J. Surg. Oncol. 2019, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.L.; Herzog, T.J.; Chan, D.W.; Munroe, D.G.; Pappas, T.C.; Smith, A.; Zhang, Z.; Wolf, J. Validation of a Second-Generation Multivariate Index Assay for Malignancy Risk of Adnexal Masses. Am. J. Obstet. Gynecol. 2016, 215, e1–e82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using The ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: Prospective multicentre diagnostic study. BMJ 2014, 349, 5920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmerman, D.; Van Calster, B.; Testa, A.C.; Guerriero, S.; Fischerova, D.; Lissoni, A.A.; Van Holsbeke, C.; Fruscio, R.; Czekierdowski, A.; Jurkovic, D.; et al. Ovarian cancer prediction in adnexal masses using ultrasound-based logistic regression models: A temporal and external validation study by the IOTA group. Ultrasound Obstet. Gynecol. 2010, 36, 226–234. [Google Scholar] [CrossRef]
- Dearking, A.; Aletti, G.; McGree, M.; Weaver, L.; Sommerfield, K.; Cliby, WA. How relevant are ACOG and SGO guidelines for referral of adnexal mass? Obstet. Gynecol. 2007, 110, 841–848. [Google Scholar] [CrossRef]
- Desai, A.; Xu, J.; Aysola, K.; Qin, Y.; Okoli, C.; Hariprasad, R.; Chinemerem, U.; Gates, C.; Reddy, A.; Danner, O.; et al. Epithelial Ovarian Cancer: An Overview. World J. Transl. Med. 2014, 3, 1–8. [Google Scholar] [CrossRef]
- Gubbels, J.A.A.; Claussen, N.; Kapur, A.K.; Connor, J.P.; Patankar, M.S. The Detection, Treatment, and Biology of Epithelial Ovarian Cancer. J. Ovarian Res. 2010, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Lheureux, S.; Braunstein, M.; Oza, A.M. Epithelial Ovarian Cancer: Evolution of Management in the Era of Precision Medicine. CA. Cancer J. Clin. 2019, 69, 280–304. [Google Scholar] [CrossRef] [Green Version]
- Lalwani, N.; Prasad, S.R.; Vikram, R.; Shanbhogue, A.K.; Huettner, P.C.; Fasih, N. Histologic, Molecular, and Cytogenetic Features of Ovarian Cancers: Implications for Diagnosis and Treatment. RadioGraphics 2011, 31, 625–646. [Google Scholar] [CrossRef]
- Tanaka, Y.O.; Okada, S.; Satoh, T.; Matsumoto, K.; Oki, A.; Saida, T.; Yoshikawa, H.; Minami, M. Differentiation of Epithelial Ovarian Cancer Subtypes by Use of Imaging and Clinical Data: A Detailed Analysis. Cancer Imaging 2016, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Labidi-Galy, S.I.; Papp, E.; Hallberg, D.; Niknafs, N.; Adleff, V.; Noe, M.; Bhattacharya, R.; Novak, M.; Jones, S.; Phallen, J.; et al. High Grade Serous Ovarian Carcinomas Originate in the Fallopian Tube. Nat. Commun. 2017, 8, 1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peres, L.C.; Risch, H.; Terry, K.L.; Webb, P.M.; Goodman, M.T.; Wu, A.H.; Alberg, A.J.; Bandera, E.V.; Barnholtz-Sloan, J.; Bondy, M.L.; et al. Racial/Ethnic Differences in the Epidemiology of Ovarian Cancer: A Pooled Analysis of 12 Case-Control Studies. Int. J. Epidemiol. 2018, 47, 460–472. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, L.M.R.; Desoky, H.H.M.; Seifeldein, G.S.; Salah, A.; Amine, M.A.; Hussien, M.T. Sonographic and Doppler Predictors of Malignancy in Ovarian Lesions. Egypt. J. Radiol. Nucl. Med. 2020, 51, 44. [Google Scholar] [CrossRef]
- Jeong, Y.-Y.; Outwater, E.K.; Kang, H.K. Imaging Evaluation of Ovarian Masses. RadioGraphics 2000, 20, 1445–1470. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Kaur, A.; Kaur Mohi, J.; Sibia, P.; Kaur, N. Evaluation of IOTA Simple Ultrasound Rules to Distinguish Benign and Malignant Ovarian Tumours. J. Clin. Diagn. Res. 2017, 11, TC06–TC09. [Google Scholar] [CrossRef]
- Shen-Gunther, J.; Mannel, R.S. Ascites as a Predictor of Ovarian Malignancy. Gynecol. Oncol. 2002, 87, 77–83. [Google Scholar] [CrossRef]
- Rickard, B.P.; Conrad, C.; Sorrin, A.J.; Ruhi, M.K.; Reader, J.C.; Huang, S.A.; Franco, W.; Scarcelli, G.; Polacheck, W.J.; Roque, D.M.; et al. Malignant Ascites in Ovarian Cancer: Cellular, Acellular, and Biophysical Determinants of Molecular Characteristics and Therapy Response. Cancers 2021, 13, 4318. [Google Scholar] [CrossRef]
- Partana, P.; Lee, S.L.; Tan, W.C. Diagnostic Performance of International Ovarian Tumor Analysis Logistic Regression Model LR2 for Adnexal Masses Classification at a Tertiary Gynecology Center in Singapore. J. Clin. Gynecol. Obstet. 2021, 10, 67–72. [Google Scholar] [CrossRef]
- Nunes, N.; Ambler, G.; Foo, X.; Widschwendter, M.; Jurkovic, D. Prospective Evaluation of IOTA Logistic Regression Models LR1 and LR2 in Comparison with Subjective Pattern Recognition for Diagnosis of Ovarian Cancer in an Outpatient Setting. Ultrasound Obstet. Gynecol. 2018, 51, 829–835. [Google Scholar] [CrossRef]
- Testa, A.; Kaijser, J.; Wynants, L.; Fischerova, D.; Van Holsbeke, C.; Franchi, D.; Savelli, L.; Epstein, E.; Czekierdowski, A.; Guerriero, S.; et al. Strategies to Diagnose Ovarian Cancer: New Evidence from Phase 3 of the Multicentre International IOTA Study. Br. J. Cancer 2014, 111, 680–688. [Google Scholar] [CrossRef] [Green Version]
- Nunes, N.; Yazbek, J.; Ambler, G.; Hoo, W.; Naftalin, J.; Jurkovic, D. Prospective Evaluation of the IOTA Logistic Regression Model LR2 for the Diagnosis of Ovarian Cancer. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2012, 40, 355–359. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | All Evaluable Women | ||
|---|---|---|---|
| Overall | Pre-Menopausal | Menopausal | |
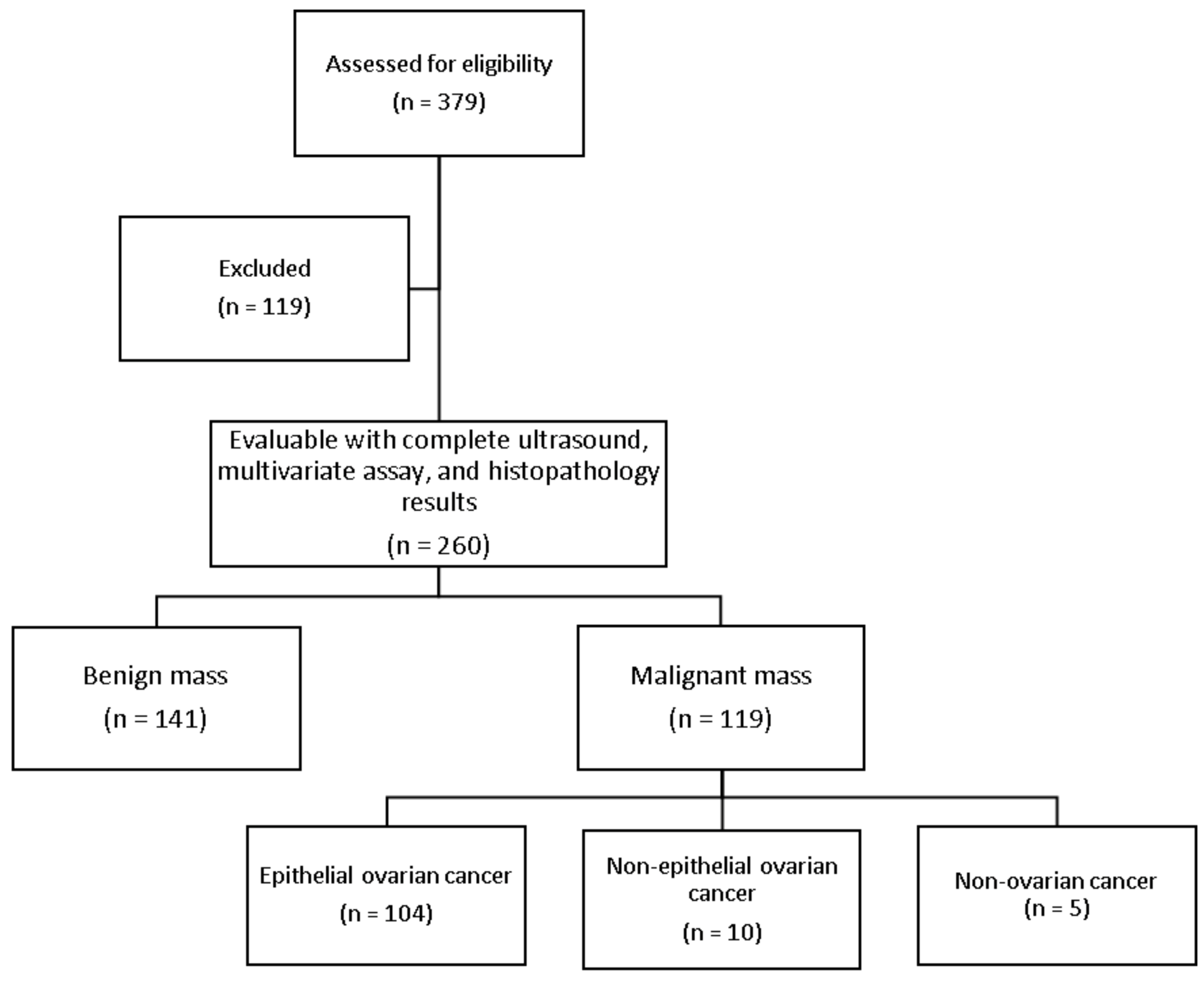
| Number | 260 | 169 | 91 |
| Age in years | |||
| Mean ± SD | 44.21 ± 13.00 | 36.86 ± 9.40 | 57.73 ± 5.86 |
| Median | 45 | 38 | 58 |
| Range | 18 to 78 | 18 to 52 | 42 to 78 |
| Number of pregnancies | |||
| None | 71 (27.31%) | 58 (34.32%) | 13 (14.29%) |
| 1 | 36 (13.85%) | 31 (18.34%) | 5 (5.49%) |
| 2 | 34 (13.08%) | 24 (14.20%) | 10 (10.99%) |
| 3 | 22 (8.46%) | 13 (7.69%) | 9 (9.89%) |
| ≥4 | 85 (32.69%) | 36 (21.30%) | 49 (53.85%) |
| Not specified | 12 (4.62%) | 7 (4.14%) | 5 (5.49%) |
| Pathologic diagnosis, n (%) | |||
| Benign conditions | 141 (54.23%) | 104 (61.54%) | 37 (40.66%) |
| Malignant conditions | 119 (45.77%) | 65 (38.46%) | 54 (59.34%) |
| Epithelial ovarian cancer | 104 (40%) | 55 (32.54%) | 49 (53.85%) |
| Serous | 33 (12.69) | 14 (8.28%) | 19 (20.88%) |
| Mucinous | 46 (17.69%) | 30 (17.75%) | 16 (17.58%) |
| Endometrioid | 3 (1.15%) | 1 (0.59%) | 2 (2.20%) |
| Clear cell | 8 (3.08%) | 5 (2.96%) | 3 (3.30%) |
| Seromucinous | 2 (0.77%) | - | 2 (2.20%) |
| Brenner | 1 (0.38%) | - | 1 (1.10%) |
| Mesonephric-like adenocarcinoma | 2 (0.77%) | 1 (0.59%) | 1 (1.10%) |
| Mixed | 8 (3.08%) | 3 (1.78%) | 5 (5.49%) |
| Metastasis (ovarian epithelial in origin) | 1 (0.38%) | 1 (0.59%) | - |
| Non-epithelial ovarian | 10 (3.85%) | 7 (4.14%) | 3 (3.30%) |
| Sex cord stromal | 4 (1.54%) | 3 (1.78%) | 1 (1.10%) |
| Germ cell | 3 (1.15%) | 3 (1.78%) | - |
| Other | 3 (1.15%) | 1 (0.59%) | 2 (2.20%) |
| Non-ovarian cancer | 5 (1.92%) | 3 (1.78%) | 2 (2.20%) |
| Stage, n (%) | 119 | 65 | 54 |
| Low malignant potential | 26 (21.85%) | 15 (23.08%) | 11 (20.37%) |
| I | 50 (42.02%) | 32 (49.23%) | 18 (33.33%) |
| II | 4 (3.36%) | 1 (1.54%) | 3 (5.56%) |
| III | 21 (17.65%) | 7 (10.77%) | 14 (25.93%) |
| IV | 10 (8.40%) | 4 (6.15%) | 6 (11.11%) |
| Descriptors | Malignant | Benign | Accuracy |
|---|---|---|---|
| Ascites | |||
| Present | 34 | 10 | 63.5% (57.3–69.3%) |
| Absent | 85 | 131 | |
| Solid components | |||
| Present | 34 | 10 | 63.5% (57.3–69.3%) |
| Absent | 85 | 131 | |
| Papillae with blood flow | |||
| Present | 61 | 7 | 75% (69.3–80.1%) |
| Absent | 58 | 134 | |
| Irregular cyst walls | |||
| Present | 65 | 15 | 73.5% (67.7–78.7%) |
| Absent | 54 | 126 | |
| Acoustic shadows | |||
| Present | 2 | 28 | 44.2% (38.1–50.5%) |
| Absent | 117 | 113 | |
| Moderate to Strong flow | |||
| Present | 49 | 11 | 68.5% (62.4–74.1%) |
| Absent | 70 | 127 | |
| Criteria | LR1 | LR2 | ADNEX | Simple Rules |
|---|---|---|---|---|
| Number | 259 | 260 | 260 | 260 |
| Sensitivity | ||||
| % | 87.4% | 79.8% | 93.3% | 85.7% |
| 95% CI | 80.1–92.8% | 71.5–86.6% | 87.2–97.1% | 78.1–91.5% |
| Specificity | ||||
| % | 78.6% | 84.4% | 62.4% | 70.2% |
| 95% CI | 70.8–85.1% | 77.3–90% | 53.9–70.4% | 61.9–77.6% |
| Positive PV | ||||
| % | 77.6% | 81.2% | 67.7% | 70.8% |
| 95% CI | 69.6–84.4% | 72.9–87.8% | 59.9–74.8% | 62.7–78.1% |
| Negative PV | ||||
| % | 88% | 83.2% | 91.7% | 85.3% |
| 95% CI | 81.0–93.1% | 76.1–88.9% | 84.2–96.3% | 77.6–91.2% |
| Accuracy | ||||
| % | 82.6% | 82.3% | 76.5% | 77.3% |
| n/N | 214/259 | 214/260 | 199/260 | 201/260 |
| 95% CI | 77.5–87% | 77.1–86.7% | 70.9–81.6% | 71.7–82.3% |
| AUROC | 0.83 | 0.82 | 0.78 | 0.78 |
| 95% CI | 0.78–0.88 | 0.77–0.87 | 0.73–0.82 | 0.73–0.83 |
| Criteria | LR1 | LR2 | ADNEX | Simple Rules | ||||
|---|---|---|---|---|---|---|---|---|
| MIA2G | CA-125 | MIA2G | CA-125 | MIA2G | CA-125 | MIA2G | CA-125 | |
| Sensitivity | ||||||||
| % | 95.8% | 91.6% | 94.1% | 86.6% | 97.5% | 94.1% | 96.6% | 93.3% |
| 95% CI | 90.5–98.6% | 85.1–95.9% | 88.3–97.6% | 79.1–92.1% | 92.8–99.5% | 88.3–97.6% | 91.6–99.1% | 87.2–97.1% |
| Specificity | ||||||||
| % | 40% | 58.6% | 40.4% | 62.4% | 34% | 50.4% | 34% | 52.5% |
| 95% CI | 31.8–48.6% | 49.9–66.8% | 32.3–49% | 53.9–70.4% | 26.3–42.5% | 41.8–58.9% | 26.3–42.5% | 43.9–60.9% |
| Positive PV | ||||||||
| % | 57.6% | 65.3% | 57.1% | 66% | 55.5% | 61.5% | 55.3% | 62.4% |
| 95% CI | 50.4–64.6% | 57.5–72.5% | 49.9–64.2% | 58–73.4% | 48.5–62.4% | 54.1- 68.6% | 48.3–62.2% | 54.8–69.5% |
| Negative PV | ||||||||
| % | 91.8% | 89.1% | 89.1% | 84.6% | 94.1% | 91% | 92.3% | 90.2% |
| 95% CI | 81.9–97.3% | 80.9–94.7% | 78.8–95.5% | 76.2–90.9% | 83.8–98.8% | 82.4–96.3% | 81.5–97.9% | 81.7–95.7% |
| Accuracy | ||||||||
| % | 65.6% | 73.7% | 65% | 73.5% | 63.1% | 70.4% | 62.7% | 71.2% |
| n/N | 170/259 | 191/259 | 169/260 | 191/260 | 164/260 | 183/260 | 163/260 | 185/260 |
| 95% CI | 59.5–71.4% | 67.9–79% | 58.9–70.8% | 67.7–78.7% | 56.9–69% | 64.4–75.9% | 56.5–68.6% | 65.2–76.6% |
| AUROC | 0.68 | 0.75 | 0.67 | 0.74 | 0.66 | 0.72 | 0.65 | 0.73 |
| 95% CI | 0.63–0.72 | 0.70–0.80 | 0.63–0.72 | 0.69–0.80 | 0.62–0.70 | 0.68–0.77 | 0.61–0.70 | 0.68–0.78 |
| Criteria | LR1 | LR2 | ADNEX | Simple Rules | ||||
|---|---|---|---|---|---|---|---|---|
| MIA2G | CA-125 | MIA2G | CA-125 | MIA2G | CA-125 | MIA2G | CA-125 | |
| Sensitivity | ||||||||
| % | 84% | 73.9% | 78.2% | 71.4% | 88.2% | 77.3% | 81.5% | 70.6% |
| 95% CI | 76.2–90.1% | 65.1–81.6% | 69.6–85.2% | 62.4–79.3% | 81–93.4% | 68.7–84.5% | 73.4–88% | 61.5–78.6% |
| Specificity | ||||||||
| % | 80.7% | 86.4% | 85.8% | 88.7% | 70.2% | 78.7% | 78% | 84.4% |
| 95% CI | 73.2–86.9% | 79.6–91.6% | 78.9–91.1% | 82.2–93.4% | 61.9–77.6% | 71–85.2% | 70.3–84.5% | 77.3–90% |
| Positive PV | ||||||||
| % | 78.7% | 82.2% | 82.3% | 84.2% | 71.4% | 75.4% | 75.8% | 79.2% |
| 95% CI | 70.6–85.5% | 73.7–89% | 74–88.8% | 75.6–90.7% | 63.4–78.6% | 66.8–82.8% | 67.4–82.9% | 70.3–86.5% |
| Negative PV | ||||||||
| % | 85.6% | 79.6% | 82.3% | 78.6% | 87.6% | 80.4% | 83.3% | 77.3% |
| 95% CI | 78.4–91.1% | 72.3–85.7% | 75.2–88.1% | 71.4–84.7% | 80.1–93.1% | 72.8–86.7% | 75.9–89.3% | 69.8–83.6% |
| Accuracy | ||||||||
| % | 82.2% | 80.7% | 82.3% | 80.8% | 78.5% | 78.1% | 79.6% | 78.1% |
| n/N | 213/259 | 209/259 | 214/260 | 210/260 | 204/260 | 203/260 | 207/260 | 203/260 |
| 95% CI | 77–86.7% | 75.4–85.3% | 77.1–86.7% | 75.4–85.4% | 73–83.3% | 72.5–83% | 74.2–84.3% | 72.5–83% |
| AUROC | 0.82 | 0.80 | 0.82 | 0.80 | 0.79 | 0.78 | 0.80 | 0.77 |
| 95% CI | 0.78–0.87 | 0.75–0.85 | 0.77–0.87 | 0.75–0.85 | 0.74–0.84 | 0.73–0.83 | 0.75–0.85 | 0.72–0.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velayo, C.L.; Reforma, K.N.; Sicam, R.V.G.; Diwa, M.H.; Sy, A.D.R.; Tantengco, O.A.G. Diagnostic Performances of Ultrasound-Based Models for Predicting Malignancy in Patients with Adnexal Masses. Healthcare 2023, 11, 8. https://doi.org/10.3390/healthcare11010008
Velayo CL, Reforma KN, Sicam RVG, Diwa MH, Sy ADR, Tantengco OAG. Diagnostic Performances of Ultrasound-Based Models for Predicting Malignancy in Patients with Adnexal Masses. Healthcare. 2023; 11(1):8. https://doi.org/10.3390/healthcare11010008
Chicago/Turabian StyleVelayo, Clarissa L., Kareen N. Reforma, Renee Vina G. Sicam, Michele H. Diwa, Alvin Duke R. Sy, and Ourlad Alzeus G. Tantengco. 2023. "Diagnostic Performances of Ultrasound-Based Models for Predicting Malignancy in Patients with Adnexal Masses" Healthcare 11, no. 1: 8. https://doi.org/10.3390/healthcare11010008