
Parameters of Iliopsoas Plane Immediately Caudal to the Indirect Tendon of Rectus Femoris in Axial Plane Measured on Magnetic Resonance Images in an Adult Eastern Asian Population
 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
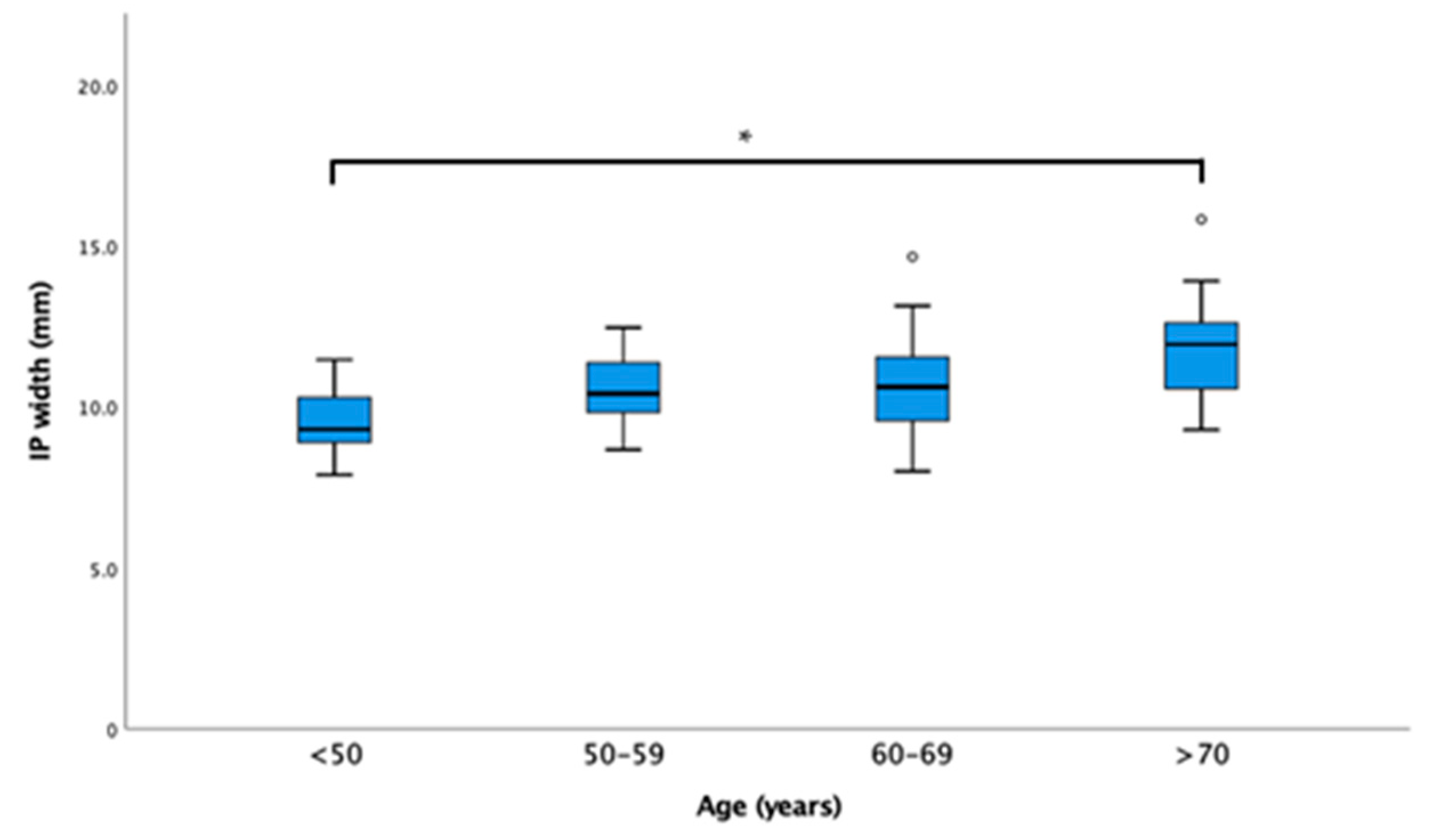
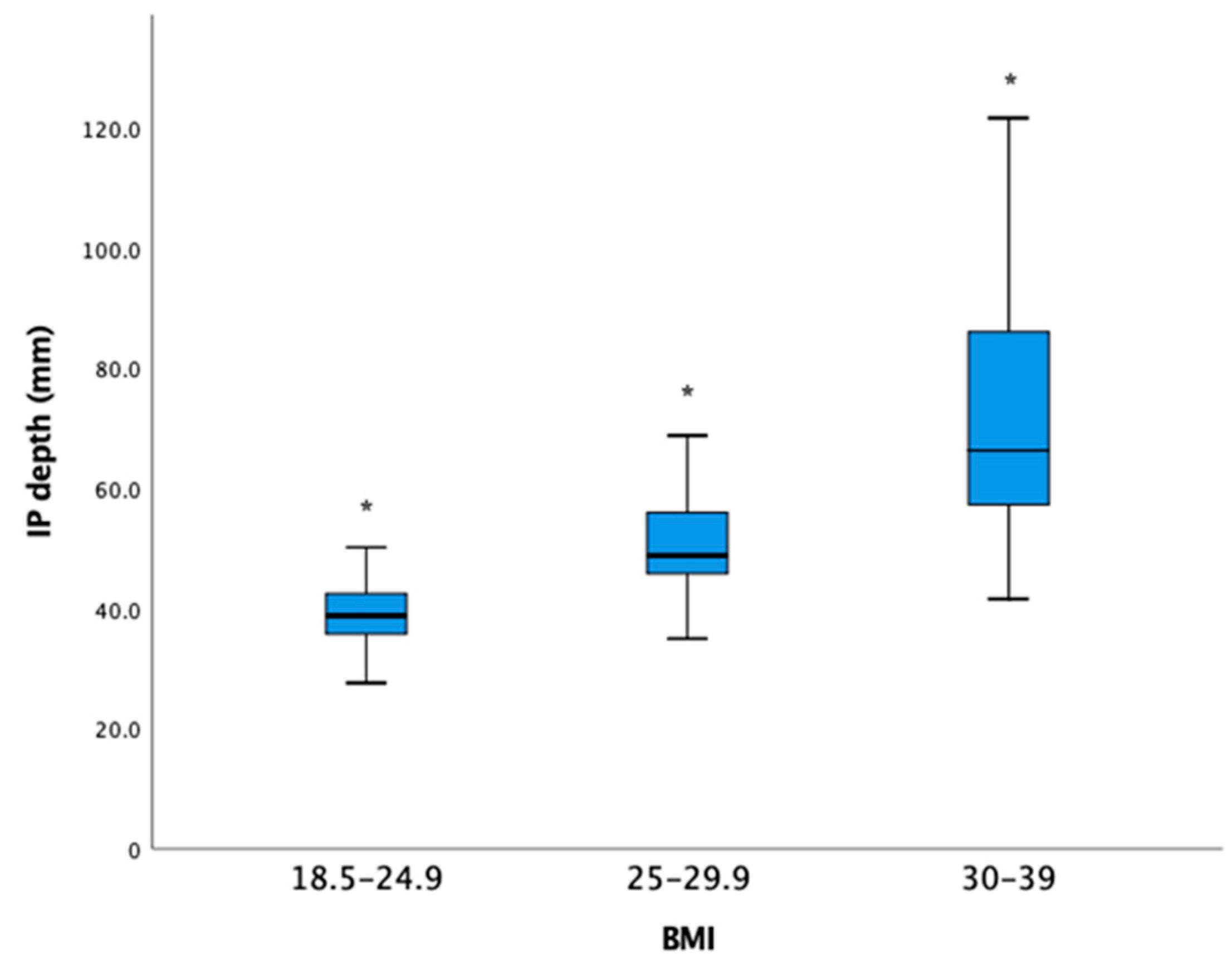
Appendix A. IP Width with the Age Subgroups and IP Depth with the BMI Subgroups Are Shown Here as Boxplots


Appendix B
References
- Nielsen, N.D.; Greher, M.; Moriggl, B.; Hoermann, R.; Nielsen, T.D.; Borglum, J.; Bendtsen, T.F. Spread of injectate around hip articular sensory branches of the femoral nerve in cadavers. Acta Anaesthesiol. Scand. 2018, 62, 1001–1006. [Google Scholar] [CrossRef]
- Short, A.J.; Barnett, J.J.G.; Gofeld, M.; Baig, E.; Lam, K.; Agur, A.M.R.; Peng, P.W.H. Anatomic Study of Innervation of the Anterior Hip Capsule: Implication for Image-Guided Intervention. Reg. Anesth. Pain Med. 2018, 43, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.D.; Madsen, M.N.; Østergaard, H.K.; Bjørn, S.; Pedersen, E.M.; Nielsen, T.D.; Søballe, K.; Børglum, J.; Bendtsen, T.F. An iliopsoas plane block does not cause motor blockade-A blinded randomized volunteer trial. Acta Anaesthesiol. Scand. 2019, 64, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Chan, W.S.; Ng, T.K.; Sham, P. Ultrasound-Guided Pericapsular Hip Joint Alcohol Neurolysis for the Treatment of Hip Pain: A Case Report of a Novel Approach. A&A Pract. 2018, 11, 60–62. [Google Scholar] [CrossRef]
- Ng, T.K.T.; Lin, J.A.; Sasaki, S. A Preliminary Analysis of a Modified Anterior Approach to 2 Hip Pericapsular Neurolysis for Inoperable Hip Fracture. Healthcare 2022, 9, 1002. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, S.R.; Chou, Y.; Chan, S.M.; Hou, J.D.; Lin, J.A. Pericapsular Nerve Group Block and Iliopsoas Plane Block: A Scoping Review of Quadriceps Weakness after Two Proclaimed Motor-Sparing Hip Blocks. Healthcare 2022, 10, 1565. [Google Scholar] [CrossRef] [PubMed]
- Moraux, A.; Wawer, R.; Lefevbre, G.; Cotten, H.; Demondion, X.; Cotten, A. An anatomical study of the indirect tendon of the rectus femoris using ultrasonography. Eur. Radiol. 2015, 25, 3614–3619. [Google Scholar] [CrossRef]
- Girón-Arango, L.; Peng, P.W.H.; Chin, K.J.; Brull, R.; Perlas, A. Pericapsular Nerve Group (PENG) Block for Hip Fracture. Reg. Anesth. Pain Med. 2018, 43, 859–863. [Google Scholar] [CrossRef]
- Laumonerie, P.; Dalmas, Y.; Tibbo, M.E.; Robert, S.; Durant, T.; Caste, T.; Vialla, T.; Tiercelin, J.; Gracia, G.; Chaynes, P. Sensory Innervation of the Hip Joint and Referred Pain: A Systematic Review of the Literature. Pain Med. 2021, 22, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.D.; Bendtsen, T.F. Motor-sparing regional analgesia for hip-derived pain. Reg. Anesth. Pain Med. 2019, 44, 415. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | IP Width (mm) | IP Depth (mm) | Needle-Beam Angle (Degrees) | |
|---|---|---|---|---|
| Age, years/old | ||||
| <50 | 6 (12) | 9.5 ± 1.2 | 42.1 ± 9.9 | 86.6 ± 1.0 |
| 50–59 | 11 (23) | 10.5 ± 1.2 | 54.9 ± 24.3 | 84.2 ± 8.5 |
| 60–69 | 21 (44) | 10.7 ± 1.6 | 48.3 ± 12.5 | 84.5 ± 9.2 |
| >70 | 10 (21) | 12.0 ± 1.9 | 45.5 ± 11.0 c | 81.9 ± 5.4 |
| p value a | 0.023 | 0.372 | 0.754 | |
| Gender, n | ||||
| Female | 21 (44) | 10.3 ± 1.4 | 53.5 ± 21.1 | 83.6 ± 8.2 |
| Male | 27 (56) | 11.1 ± 1.8 | 44.5 ± 7.6 c | 84.6 ± 8.6 |
| p value b | 0.076 | 0.051 | 0.677 | |
| BMI, kg/m2 | ||||
| 18.5–24.9 | 19 (40) | 11.2 ± 1.6 | 38.9 ± 5.8 | 85.4 ± 9.5 |
| 25–29.9 | 22 (46) | 10.5 ± 1.7 | 50.1 ± 8.0 | 83.4 ± 8.1 |
| 30–39 | 7 (14) | 10.5 ± 1.3 | 73.2 ± 27.8 c | 83.3 ± 6.0 |
| p value a | 0.323 | <0.001 d | 0.736 |
| R Square (Adjusted R) | Sig | |
|---|---|---|
| 0.150 (0.132) | IP width = 6.977 + 0.061 ∗ age | 0.007 |
| 0.573 (0.563) | IP depth = −31.24 + 3.064 ∗ BMI | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeoh, S.-R.; Chou, Y.; Yang, J.-H.; Chuang, C.-W.; Chan, S.-M.; Chen, S.-Y.; Hou, J.-D.; Lin, J.-A. Parameters of Iliopsoas Plane Immediately Caudal to the Indirect Tendon of Rectus Femoris in Axial Plane Measured on Magnetic Resonance Images in an Adult Eastern Asian Population. Healthcare 2023, 11, 69. https://doi.org/10.3390/healthcare11010069
Yeoh S-R, Chou Y, Yang J-H, Chuang C-W, Chan S-M, Chen S-Y, Hou J-D, Lin J-A. Parameters of Iliopsoas Plane Immediately Caudal to the Indirect Tendon of Rectus Femoris in Axial Plane Measured on Magnetic Resonance Images in an Adult Eastern Asian Population. Healthcare. 2023; 11(1):69. https://doi.org/10.3390/healthcare11010069
Chicago/Turabian StyleYeoh, Shang-Ru, Yen Chou, Jin-Han Yang, Ching-Wei Chuang, Shun-Ming Chan, Se-Yi Chen, Jin-De Hou, and Jui-An Lin. 2023. "Parameters of Iliopsoas Plane Immediately Caudal to the Indirect Tendon of Rectus Femoris in Axial Plane Measured on Magnetic Resonance Images in an Adult Eastern Asian Population" Healthcare 11, no. 1: 69. https://doi.org/10.3390/healthcare11010069