
Acute Pain Management Pearls: A Focused Review for the Hospital Clinician

Abstract
:1. Introduction
- Uncontrolled pain worsens patient outcomes and healthcare costs—adopt a consistent, systematic, and holistic approach to acute pain management.
- Not every patient is an ideal candidate for every medication, but every patient in pain is a candidate for multimodal analgesia optimization.
- There are tremendous benefits to employing anti-inflammatories and few good reasons to withhold them in the management of acute pain.
- Gabapentinoids have a complex risk/benefit ratio and decision-making should be nuanced.
- Low-dose ketamine is a powerful analgesic even in opioid-tolerant patients and is generally well-tolerated with appropriate institutional protocols.
- Empiric opioid regimens should include consideration of optimal agent selection, dosing, route of administration, and supportive therapies.
- Pain regimens should be evaluated and adjusted at least daily through multidimensional pain assessments to optimize efficacy and safety endpoints.
- Patients with opioid tolerance, chronic pain, and/or opioid use disorder require higher opioid doses and more supportive therapies.
- When used for acute pain, patient-specific plans for opioid tapering and harm reduction should be developed and supported across the care continuum.
- Methadone and buprenorphine should almost always be continued throughout acute pain episodes, but naltrexone must be stopped.
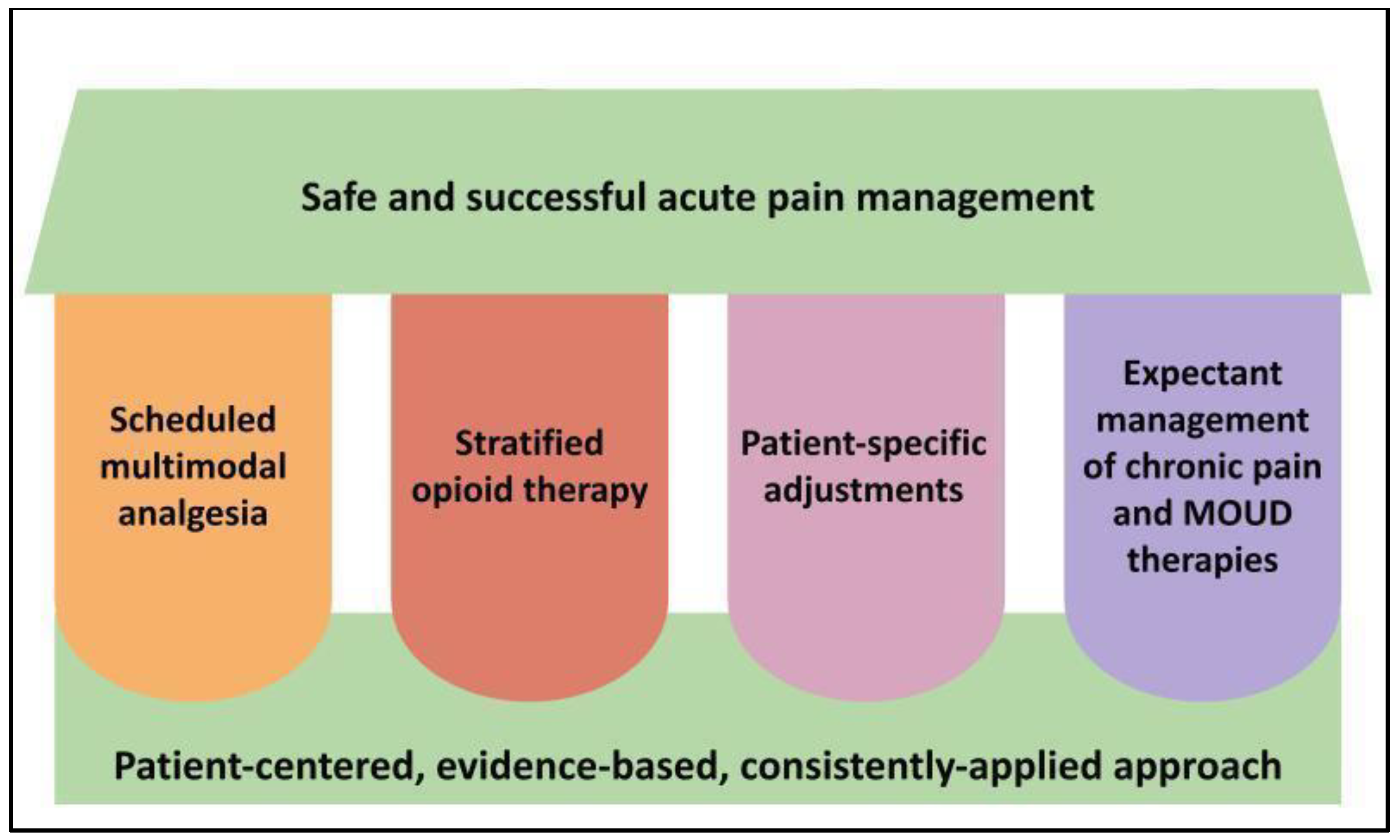
2. Clinical Pearl #1: Uncontrolled Pain Worsens Patient Outcomes and Healthcare Costs—Adopt a Consistent, Systematic, and Holistic Approach to Acute Pain Management
KEY CONSIDERATION: Opioid avoidance in acute painful conditions is an ill-advised goal as it is neither patient-centered nor evidenced-based; rather, multimodal analgesia and opioid stewardship should integrate into a patient-specific, data-driven approach to inpatient acute pain management.
3. Clinical Pearl #2: Not Every Patient Is an Ideal Candidate for Every Medication, but Every Patient in Pain Is a Candidate for Multimodal Analgesia Optimization
KEY CONSIDERATION: Multimodal analgesia should be balanced and thoughtful, utilizing complementary mechanisms to improve pain control with less high-risk drug exposure, as opposed to overmedicating without regard to cumulative risks or patient-specific factors.
- Acetaminophen
- Anti-inflammatories
- Neuropathic agents- gabapentinoids, serotonin reuptake inhibitors, anticonvulsants
- Corticosteroids
- NMDA antagonists
- Central alpha adrenergic agonists
- Systemic anesthetics (e.g., intravenous lidocaine, inhaled anesthetics)
- Topical agents- lidocaine, anti-inflammatories, capsaicin
- Regional anesthetic modalities in concert with a specialist pain service (e.g., peripheral nerve blocks, neuraxial blocks)
- Physical therapy, cognitive/behavioral therapies, thermotherapies, and other nonpharmacologic modalities
4. Clinical Pearl #3: There Are Tremendous Benefits to Employing Anti-Inflammatories and Few Good Reasons to Withhold Them in the Management of Acute Pain
KEY CONSIDERATION: NSAIDs target an important source of pain instead of just interfering with the perception of pain, making them among the most effective and important analgesics available in acute pain management.
5. Clinical Pearl #4: Gabapentinoids Have a Complex Risk/Benefit Ratio and Decision-Making Should Be Nuanced
KEY CONSIDERATION: Gabapentanioids are heavily renally eliminated and require dose adjustment in altered kidney function. Patients undergoing dialysis who are apt to miss appointments or who are unable to tolerate a complete hemodialysis session are at risk for drug accumulation and adverse events.
KEY CONSIDERATION: Gabapentinoids are narcotics with dose-dependent adverse effects, which may include respiratory depression, especially with concomitant CNS depressants or in high-risk patients.
6. Clinical Pearl #5: Low-Dose Ketamine Is a Powerful Analgesic even in Opioid-Tolerant Patients and Is Generally Well-Tolerated with Appropriate Institutional Protocols
KEY CONSIDERATION: Among available nonopioid analgesics, ketamine has the strongest evidence supporting improved pain control and opioid-sparing properties in patients with preexisting opioid tolerance. It may also interrupt the pathological processes of central sensitization and opioid-induced hyperalgesia, conferring benefit in severe or difficult-to-treat pain.
KEY CONSIDERATION: Collaborative, evidence-based institutional protocols and prescriber/staff education are essential to the safe use of analgesic-dose ketamine in hospitalized patients. With appropriate provider knowledge (and/or availability of specialist consultation) and standardized procedures, low-dose ketamine can be safely employed for acute pain management by general practitioners on general medical/surgical inpatient units.
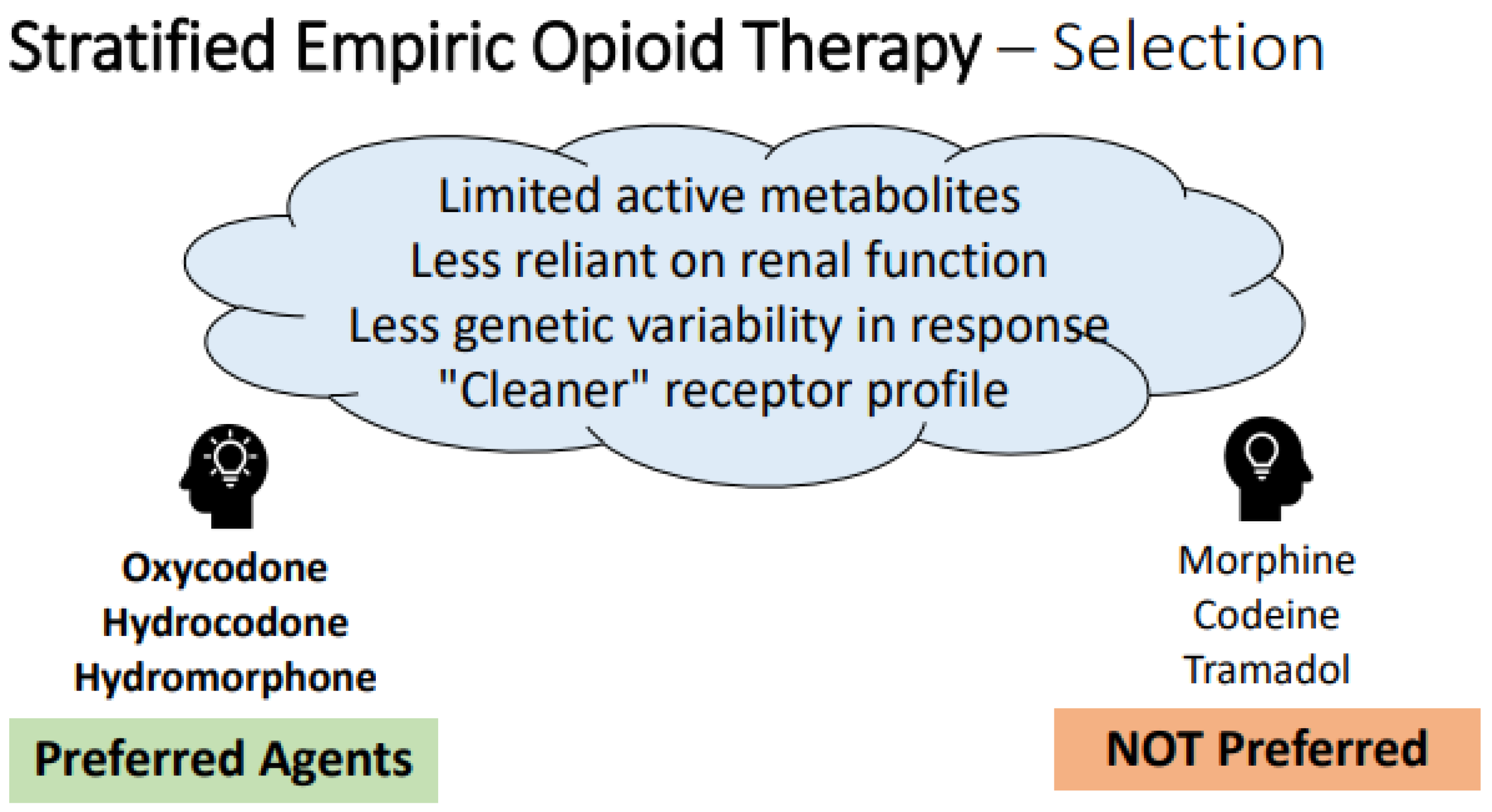
7. Clinical Pearl #6: Empiric Opioid Regimens should include Consideration of Optimal Agent Selection, Dosing, Route of Administration, and Supportive Therapies
7.1. Opioid Agent Selection
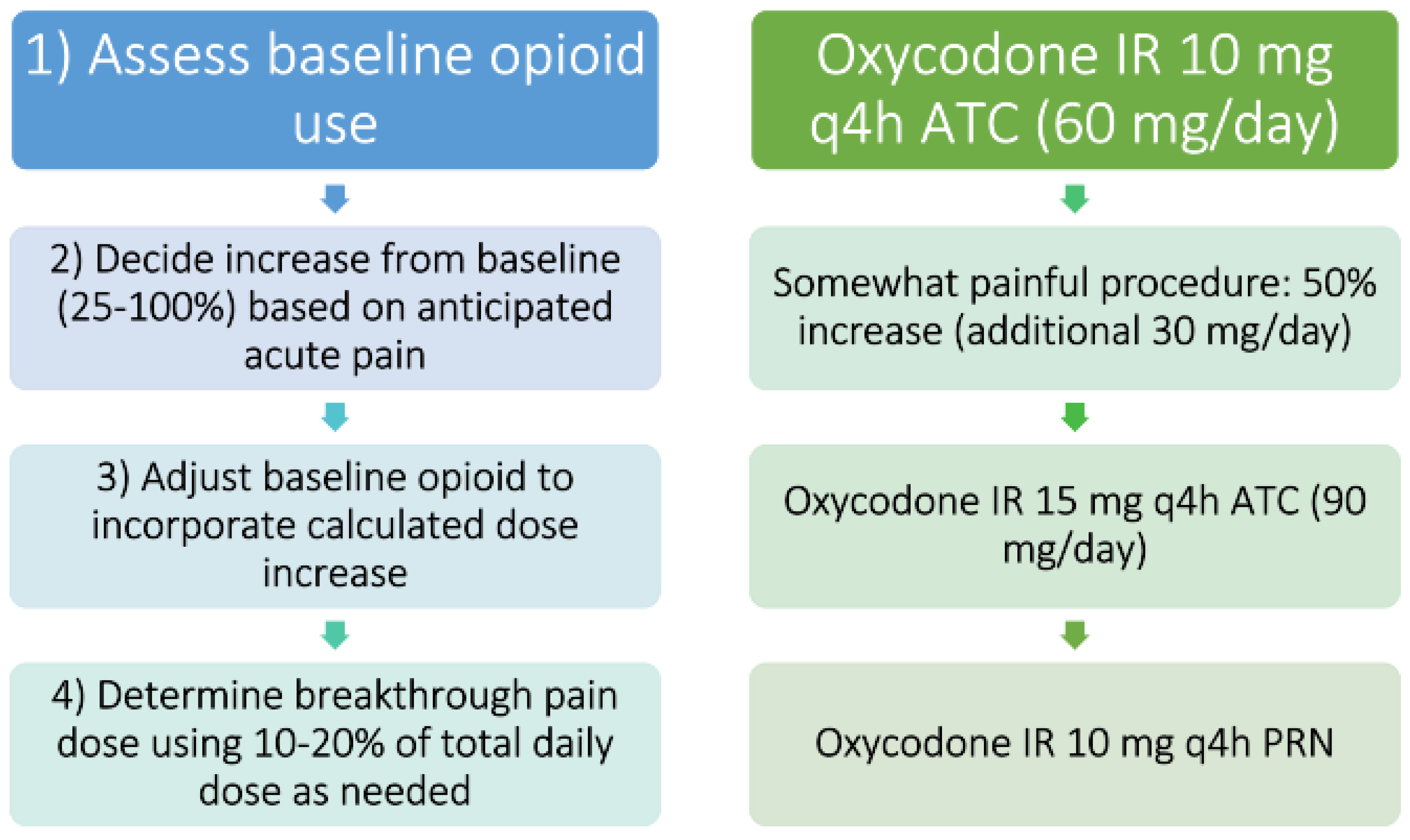
7.2. Empiric Opioid Dosing
7.3. Opioid Routes of Administration
KEY CONSIDERATION: The route of opioid administration should be tailored to patient status and degree of need for rapid onset, with the enteral route being the safest and easiest when possible. The sublingual route of administration also offers a fast onset of action.
KEY CONSIDERATION: The subcutaneous route of administration for opioids is a valued option in unique situations; the intramuscular route of administration should be avoided.
7.4. Supportive Therapies to Be Co-Prescribed with Opioids
KEY CONSIDERATION: Always begin a scheduled stimulant bowel regimen when initiating opioid therapy; as-needed laxatives or docusate alone are not sufficient to prevent opioid-induced bowel dysfunction.
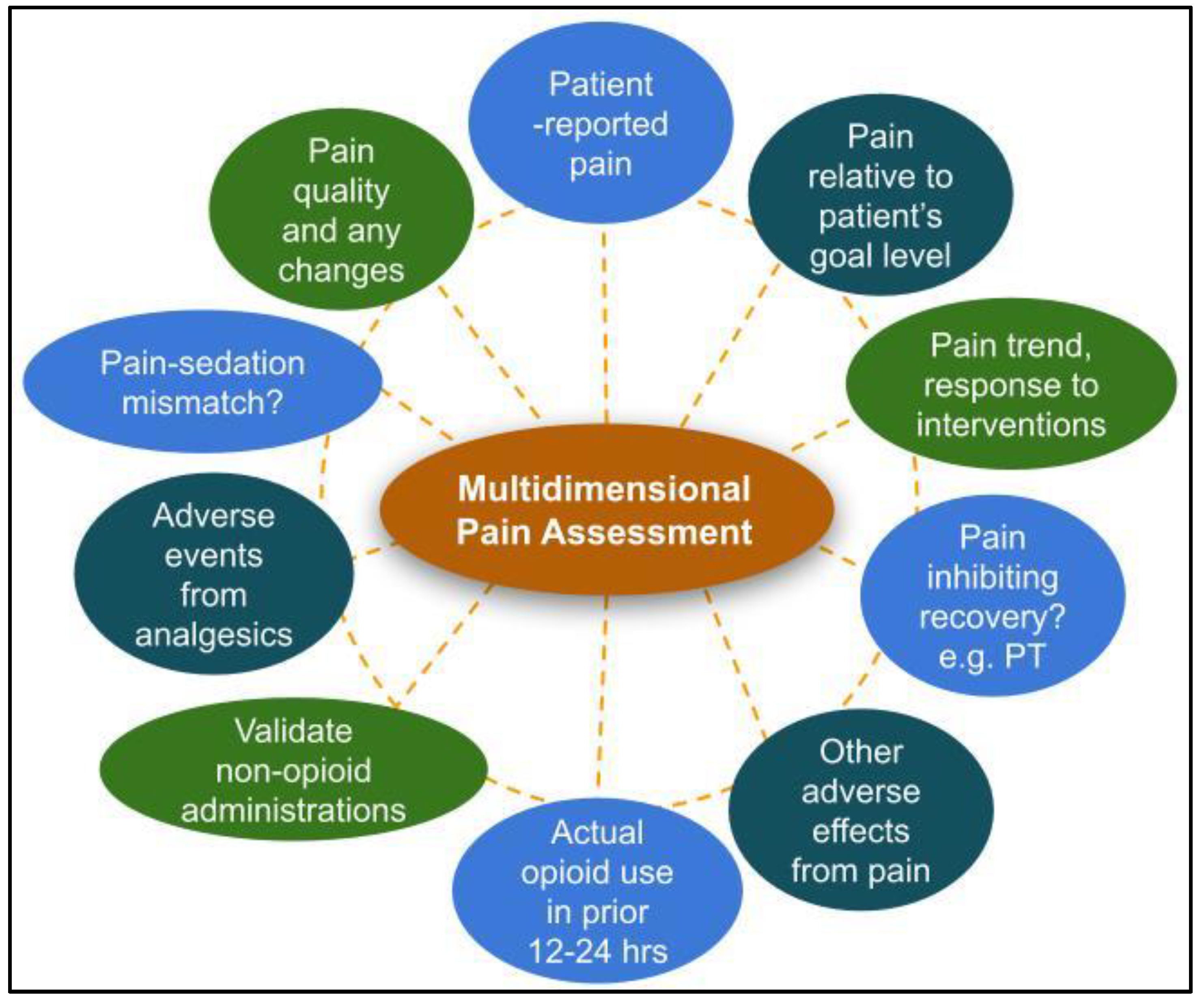
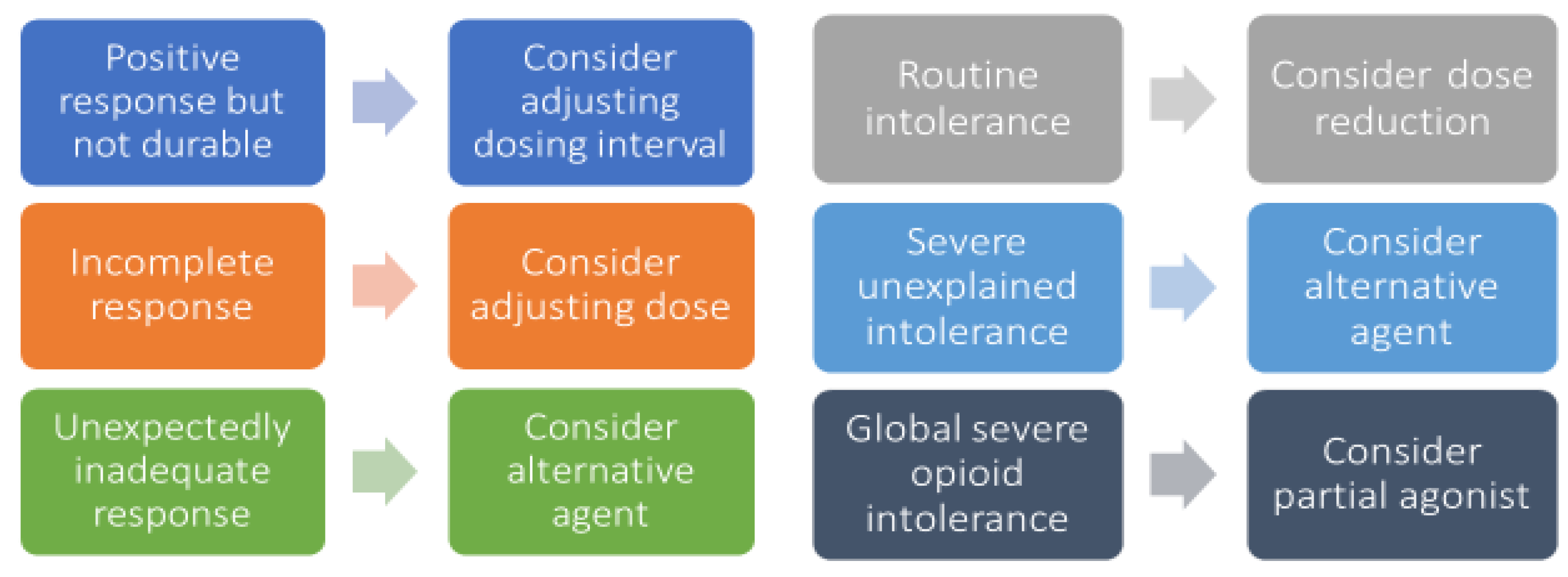
8. Clinical Pearl #7: Pain Regimens Should Be Evaluated and Adjusted at Least Daily through Multidimensional Pain Assessments to Optimize Efficacy and Safety Endpoints
KEY CONSIDERATION: Assessing for drug efficacy and adverse effects at the expected time to peak after drug administration is the best way to determine whether the selected dose is right for the patient. Carefully assess the nature of breakthrough pain in order to determine the best approach to regimen adjustments.
9. Clinical Pearl #8: Patients with Opioid Tolerance, Chronic Pain, and/or Opioid Use Disorder Require Higher Opioid Doses and More Supportive Therapies to Achieve Positive Outcomes
KEY CONSIDERATION: A relationship of mutual trust and respect is vital to manage the patient’s pain. Chronic pain comes with complex psychological impacts that can inform the patient’s physical pain experience and can affect treatment response.
10. Clinical Pearl #9: When Used for Acute Pain, Patient-Specific Plans for Opioid Tapering and Harm Reduction Should Be Developed and Supported across the Care Continuum
KEY CONSIDERATION: Opioid tapering goals and regimens must be patient-specific and prospectively, collaboratively discussed with the patient and other care team members in order to be safe and successful. Pre-discharge patient counseling on the pain management plan and opioid safety are essential.
KEY CONSIDERATION: Co-prescribing take-home naloxone is evidenced-based harm reduction and should be widely considered by hospital providers prescribing opioids at discharge, alongside appropriate educational and continuity of care efforts.
11. Clinical Pearl #10: Methadone and Buprenorphine Should Almost Always Be Continued throughout Acute Pain Episodes, but Naltrexone Must Be Stopped
KEY CONSIDERATION: Buprenorphine/naloxone combination products DO NOT have to be changed to buprenorphine-only products during acute painful episodes due to the low bioavailability of naloxone.
KEY CONSIDERATION: Methadone and buprenorphine should be continued during acute painful episodes, including surgical encounters, alongside opioid-tolerant doses of as-needed pain medications within multimodal analgesic regimens.
KEY CONSIDERATION: The duration of analgesia from buprenorphine and methadone is shorter than their duration of reducing cravings and withdrawal symptoms- splitting the home dose throughout the day should be considered as part of the multimodal analgesic regimen during periods of acute pain. The patient’s usual dosing regimen can then be resumed once acute pain has subsided and/or at hospital discharge.
KEY CONSIDERATION: Naltrexone-containing products must be stopped prior to any scheduled elective procedures to ensure adequate pain management for patients. Patients who have naltrexone interrupted will rapidly lose their tolerance to opioids and should be monitored closely when opioid therapies are needed.
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, R.J.; Reid, M.C.; Liu, L.L.; Chused, A.E.; Evans, A.T. The Barriers to High-Quality Inpatient Pain Management: A Qualitative Study. Am. J. Hosp. Palliat. Med. 2015, 32, 594–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinatra, R. Causes and consequences of inadequate management of acute pain. Pain Med. 2010, 11, 1859–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baratta, J.L.; Schwenk, E.S.; Viscusi, E.R. Clinical consequences of inadequate pain relief: Barriers to optimal pain management. Plast. Reconstr. Surg. 2014, 134, 15S–21S. [Google Scholar] [CrossRef]
- Glare, P.; Aubrey, K.R.; Myles, P.S. Transition from acute to chronic pain after surgery. Lancet 2019, 393, 1537–1546. [Google Scholar] [CrossRef]
- Kane-Gill, S.L.; Rubin, E.C.; Smithburger, P.L.; Buckley, M.S.; Dasta, J.F. The cost of opioid-related adverse drug events. J. Pain Palliat. Care Pharmacother. 2014, 28, 282–293. [Google Scholar] [CrossRef]
- Bicket, M.C.; Long, J.J.; Pronovost, P.J.; Alexander, G.C.; Wu, C.L. Prescription Opioid Analgesics Commonly Unused After Surgery: A Systematic Review. JAMA Surg. 2017, 152, 1066–1071. [Google Scholar] [CrossRef]
- Brat, G.A.; Agniel, D.; Beam, A.; Yorkgitis, B.; Bicket, M.; Homer, M. Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: Retrospective cohort study. BMJ 2018, 360, j5790. [Google Scholar] [CrossRef] [Green Version]
- Kent, M.L.; Hurley, R.W.; Oderda, G.M.; Gordon, D.B.; Sun, E.; Mythen, M. American Society for Enhanced Recovery and Perioperative Quality Initiative-4 Joint Consensus Statement on Persistent Postoperative Opioid Use: Definition, Incidence, Risk Factors, and Health Care System Initiatives. Anesth. Analg. 2019, 129, 543. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps, Inconsistencies, and Recommendations. Available online: https://www.hhs.gov/ash/advisory-committees/pain/reports/index.html (accessed on 15 September 2022).
- McPherson, M.L. Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing; Bethesda, M.D., Ed.; American Society of Health-System Pharmacists, 2019, 2nd ed. Available online: https://play.google.com/store/books/details?id=1g9uDwAAQBAJ (accessed on 15 September 2022).
- Hyland, S.J.; Brockhaus, K.K.; Vincent, W.R.; Spence, N.Z.; Lucki, M.M.; Howkins, M.J. Perioperative Pain Management and Opioid Stewardship: A Practical Guide. Healthcare 2021, 9, 333. [Google Scholar] [CrossRef]
- Dunwoody, C.J.; Krenzischek, D.A.; Pasero, C.; Rathmell, J.P.; Polomano, R.C. Assessment, physiological monitoring, and consequences of inadequately treated acute pain. J. Perianesth. Nurs. 2008, 23, S15–S27. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.; Chin, K.J. Advances in regional anaesthesia and acute pain management: A narrative review. Anaesthesia 2020, 75 (Suppl. 1), e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Memtsoudis, S.G.; Cozowicz, C.; Bekeris, J.; Bekere, D.; Liu, J.; Soffin, E.M. Anaesthetic care of patients undergoing primary hip and knee arthroplasty: Consensus recommendations from the International Consensus on Anaesthesia-Related Outcomes after Surgery group (ICAROS) based on a systematic review and meta-analysis. Br. J. Anaesth. 2019, 123, 269–287. [Google Scholar] [CrossRef] [PubMed]
- Oderda, G.M.; Senagore, A.J.; Morland, K.; Iqbal, S.U.; Kugel, M.; Liu, S. Opioid-related respiratory and gastrointestinal adverse events in patients with acute postoperative pain: Prevalence, predictors, and burden. J. Pain Palliat. Care Pharmacother. 2019, 33, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.T.; Ingram, S.L.; Henderson, G.; Chavkin, C.; von Zastrow, M.; Schulz, S. Regulation of μ-opioid receptors: Desensitization, phosphorylation, internalization, and tolerance. Pharmacol. Rev. 2013, 65, 223–254. [Google Scholar] [CrossRef] [Green Version]
- Cao, D.-N.; Li, F.; Wu, N.; Li, J. Insights into the mechanisms underlying opioid use disorder and potential treatment strategies. Br. J. Pharmacol. 2021. [Google Scholar] [CrossRef]
- Bicket, M.C.; White, E.; Pronovost, P.J.; Wu, C.L.; Yaster, M.; Alexander, G.C. Opioid Oversupply After Joint and Spine Surgery: A Prospective Cohort Study. Anesth. Analg. 2019, 128, 358–364. [Google Scholar] [CrossRef]
- Chou, R.; Gordon, D.B.; de Leon-Casasola, O.A.; Rosenberg, J.M.; Bickler, S.; Brennan, T. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J. Pain 2016, 17, 131–157. [Google Scholar] [CrossRef] [Green Version]
- Desai, K.; Carroll, I.; Asch, S.M.; Seto, T.; McDonald, K.M.; Curtin, C. Utilization and effectiveness of multimodal discharge analgesia for postoperative pain management. J. Surg. Res. 2018, 228, 160–169. [Google Scholar] [CrossRef]
- Uritsky, T.J.; Busch, M.E.; Chae, S.G.; Genord, C. Opioid Stewardship: Building on Antibiotic Stewardship Principles. J. Pain Palliat. Care Pharmacother. 2021, 34, 181–183. [Google Scholar] [CrossRef]
- Weingarten, T.N.; Taenzer, A.H.; Elkassabany, N.M.; Le Wendling, L.; Nin, O.; Kent, M.L. Safety in Acute Pain Medicine-Pharmacologic Considerations and the Impact of Systems-Based Gaps. Pain Med. 2018, 19, 2296–2315. [Google Scholar] [CrossRef] [PubMed]
- Wick, E.C.; Grant, M.C.; Wu, C.L. Postoperative Multimodal Analgesia Pain Management With Nonopioid Analgesics and Techniques: A Review. JAMA Surg. 2017, 152, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Helander, E.M.; Menard, B.L.; Harmon, C.M.; Homra, B.K.; Allain, A.V.; Bordelon, G.J. Multimodal Analgesia, Current Concepts, and Acute Pain Considerations. Curr. Pain Headache Rep. 2017, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Beverly, A.; Kaye, A.D.; Ljungqvist, O.; Urman, R.D. Essential Elements of Multimodal Analgesia in Enhanced Recovery After Surgery (ERAS) Guidelines. Anesthesiol. Clin. 2017, 35, e115–e143. [Google Scholar] [CrossRef]
- Kaye, A.D.; Urman, R.D.; Rappaport, Y.; Siddaiah, H.; Cornett, E.M.; Belani, K. Multimodal analgesia as an essential part of enhanced recovery protocols in the ambulatory settings. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, S40–S45. [Google Scholar] [CrossRef]
- Dwyer, J.P.; Jayasekera, C.; Nicoll, A. Analgesia for the cirrhotic patient: A literature review and recommendations. J. Gastroenterol. Hepatol. 2014, 29, 1356–1360. [Google Scholar] [CrossRef] [Green Version]
- Ohnuma, T.; Raghunathan, K.; Ellis, A.R.; Whittle, J.; Pyati, S.; Bryan, W.E. Effects of acetaminophen, NSAIDs, gabapentinoids, and their combinations on postoperative pulmonary complications after total hip or knee arthroplasty. Pain Med. 2020, 21, 2385–2393. [Google Scholar] [CrossRef]
- Agrawal, S.; Khazaeni, B. Acetaminophen Toxicity; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28722946 (accessed on 15 September 2022).
- Lopes-Júnior, L.C.; Rosa, G.S.; Pessanha, R.M.; Schuab, S.I.P.D.C.; Nunes, K.Z.; Amorim, M.H.C. Efficacy of the complementary therapies in the management of cancer pain in palliative care: A systematic review. Rev. Lat. Am. Enfermagem. 2020, 28, e3377. [Google Scholar] [CrossRef]
- Kaye, A.D.; Granier, A.L.; Garcia, A.J.; Carlson, S.F.; Fuller, M.C.; Haroldson, A.R. Non-Opioid Perioperative Pain Strategies for the Clinician: A Narrative Review. Pain Ther. 2020, 9, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.-S.; Chen, K.-H.; Chen, I.-F.; Huang, S.K.; Tzeng, P.-C.; Yeh, M.-L. The Efficacy of Acupuncture in Post-Operative Pain Management: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0150367. [Google Scholar] [CrossRef]
- Liang, J.; Tian, X.; Yang, W. Application of Music Therapy in General Surgical Treatment. Biomed. Res. Int. 2021, 2021, 6169183. [Google Scholar] [CrossRef] [PubMed]
- Yu, R.; Zhuo, Y.; Feng, E.; Wang, W.; Lin, W.; Lin, F. The effect of musical interventions in improving short-term pain outcomes following total knee replacement: A meta-analysis and systematic review. J. Orthop. Surg. Res. 2020, 15, 465. [Google Scholar] [CrossRef] [PubMed]
- Kühlmann, A.Y.R.; de Rooij, A.; Kroese, L.F.; van Dijk, M.; Hunink, M.G.M.; Jeekel, J. Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br. J. Surg. 2018, 105, 773–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Petrini, M.A. Effects of music therapy on pain, anxiety, and vital signs in patients after thoracic surgery. Complement. Ther. Med. 2015, 23, 714–718. [Google Scholar] [CrossRef]
- Matsota, P.; Christodoulopoulou, T.; Smyrnioti, M.E.; Pandazi, A.; Kanellopoulos, I.; Koursoumi, E. Music’s use for anesthesia and analgesia. J. Altern. Complement. Med. 2013, 19, 298–307. [Google Scholar] [CrossRef]
- Fan, M.; Chen, Z. A systematic review of non-pharmacological interventions used for pain relief after orthopedic surgical procedures. Exp. Ther. Med. 2020, 20, 36. [Google Scholar] [CrossRef]
- Oxford League Table of Analgesic Efficacy. Available online: http://www.bandolier.org.uk/booth/painpag/Acutrev/Analgesics/lftab.html (accessed on 28 February 2021).
- Pogatzki-Zahn, E.M.; Segelcke, D.; Schug, S.A. Postoperative pain-from mechanisms to treatment. Pain Rep. 2017, 2, e588. [Google Scholar] [CrossRef]
- Arias, J.-I.; Aller, M.-A.; Arias, J. Surgical inflammation: A pathophysiological rainbow. J. Transl. Med. 2009, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; Huh, Y.; Ji, R.-R. Roles of inflammation, neurogenic inflammation, and neuroinflammation in pain. J. Anesth. 2019, 33, 131–139. [Google Scholar] [CrossRef]
- Mammoto, T.; Fujie, K.; Taguchi, N.; Ma, E.; Shimizu, T.; Hashimoto, K. Short-term effects of early postoperative celecoxib administration for pain, sleep quality, and range of motion after total knee arthroplasty: A randomized controlled trial. J. Arthroplast. 2021, 36, 526–531. [Google Scholar] [CrossRef]
- Chang, R.W.; Tompkins, D.M.; Cohn, S.M. Are NSAIDs safe? Assessing the risk-benefit profile of nonsteroidal anti-inflammatory drug use in postoperative pain management. Am. Surg. 2020, 87, 872879. [Google Scholar] [CrossRef] [PubMed]
- Sheth, K.R.; Bernthal, N.M.; Ho, H.S.; Bergese, S.D.; Apfel, C.C.; Stoicea, N. Perioperative bleeding and non-steroidal anti-inflammatory drugs: An evidence-based literature review, and current clinical appraisal. Medicine 2020, 99, e20042. [Google Scholar] [CrossRef] [PubMed]
- Fillingham, Y.A.; Hannon, C.P.; Roberts, K.C. AAHKS Anesthesia & Analgesia Clinical Practice Guideline Workgroup, Hamilton WG, Della Valle CJ. Nonsteroidal Anti-Inflammatory Drugs in Total Joint Arthroplasty: The Clinical Practice Guidelines of the American Association of Hip and Knee Surgeons, American Society of Regional Anesthesia and Pain Medicine, American Academy of Orthopaedic Surgeons, Hip Society, and Knee Society. J. Arthroplast. 2020, 35, 2704–2708. [Google Scholar] [CrossRef]
- Debono, B.; Wainwright, T.W.; Wang, M.Y.; Sigmundsson, F.G.; Yang, M.M.H.; Smid-Nanninga, H. Consensus statement for perioperative care in lumbar spinal fusion: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Spine J. 2021, 21, 729–752. [Google Scholar] [CrossRef]
- Martinez, L.; Ekman, E.; Nakhla, N. Perioperative Opioid-sparing Strategies: Utility of Conventional NSAIDs in Adults. Clin. Ther. 2019, 41, 2612–2628. [Google Scholar] [CrossRef]
- Maslin, B.; Lipana, L.; Roth, B.; Kodumudi, G.; Vadivelu, N. Safety Considerations in the Use of Ketorolac for Postoperative Pain. Curr. Drug. Saf. 2017, 12, 67–73. [Google Scholar] [CrossRef]
- Gobble, R.M.; Hoang, H.L.T.; Kachniarz, B.; Orgill, D.P. Ketorolac does not increase perioperative bleeding: A meta-analysis of randomized controlled trials. Plast. Reconstr. Surg. 2014, 133, 741–755. [Google Scholar] [CrossRef]
- Cassinelli, E.H.; Dean, C.L.; Garcia, R.M.; Furey, C.G.; Bohlman, H.H. Ketorolac use for postoperative pain management following lumbar decompression surgery: A prospective, randomized, double-blinded, placebo-controlled trial. Spine 2008, 33, 1313–1317. [Google Scholar] [CrossRef]
- Devin, C.J.; McGirt, M.J. Best evidence in multimodal pain management in spine surgery and means of assessing postoperative pain and functional outcomes. J. Clin. Neurosci. 2015, 22, 930–938. [Google Scholar] [CrossRef]
- Jamjittrong, S.; Matsuda, A.; Matsumoto, S.; Kamonvarapitak, T.; Sakurazawa, N.; Kawano, Y. Postoperative non-steroidal anti-inflammatory drugs and anastomotic leakage after gastrointestinal anastomoses: Systematic review and meta-analysis. Ann. Gastroenterol. Surg. 2020, 4, 64–75. [Google Scholar] [CrossRef]
- Modasi, A.; Pace, D.; Godwin, M.; Smith, C.; Curtis, B. NSAID administration post colorectal surgery increases anastomotic leak rate: Systematic review/meta-analysis. Surg. Endosc. 2019, 33, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Tang, S.R.; Young, C.J. Nonsteroidal anti-inflammatory drugs and anastomotic dehiscence after colorectal surgery: A meta-analysis. ANZ J. Surg. 2018, 88, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Stacy, Z.A.; Dobesh, P.P.; Trujillo, T.C. Cardiovascular risks of cyclooxygenase inhibition. Pharmacotherapy 2006, 26, 919–938. [Google Scholar] [CrossRef] [PubMed]
- Schug, S.A.; Parsons, B.; Li, C.; Xia, F. The safety profile of parecoxib for the treatment of postoperative pain: A pooled analysis of 28 randomized, double-blind, placebo-controlled clinical trials and a review of over 10 years of postauthorization data. J. Pain Res. 2017, 10, 2451–2459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanelli, A.; Ghisi, D.; Aprile, P.L.; Lapi, F. Cardiovascular and cerebrovascular risk with nonsteroidal anti-inflammatory drugs and cyclooxygenase 2 inhibitors:Latest evidence and clinical implications. Ther. Adv. Drug. Saf. 2017, 8, 173–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheiman, J.M.; Hindley, C.E. Strategies to optimize treatment with NSAIDs in patients at risk for gastrointestinal and cardiovascular adverse events. Clin. Ther. 2010, 32, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Massoth, C.; Zarbock, A.; Meersch, M. Risk Stratification for Targeted AKI Prevention After Surgery: Biomarkers and Bundled Interventions. Semin. Nephrol. 2019, 39, 454–461. [Google Scholar] [CrossRef]
- Goren, O.; Matot, I. Perioperative acute kidney injury. Br. J. Anaesth. 2015, 115 (Suppl. 2), ii3–ii14. [Google Scholar] [CrossRef] [Green Version]
- Meersch, M.; Schmidt, C.; Zarbock, A. Perioperative Acute Kidney Injury: An Under-Recognized Problem. Anesth. Analg. 2017, 125, 1223–1232. [Google Scholar] [CrossRef]
- Khan, D.A.; Knowles, S.R.; Shear, N.H. Sulfonamide Hypersensitivity: Fact and Fiction. J. Allergy Clin. Immunol. Pract. 2019, 7, 2116–2123. [Google Scholar] [CrossRef]
- Wulf, N.R.; Matuszewski, K.A. Sulfonamide cross-reactivity: Is there evidence to support broad cross-allergenicity? Am. J. Health Syst. Pharm. 2013, 70, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Brackett, C.C. Sulfonamide allergy and cross-reactivity. Curr. Allergy Asthma. Rep. 2007, 7, 41–48. [Google Scholar] [CrossRef]
- Yska, J.P.; Gertsen, S.; Flapper, G.; Emous, M.; Wilffert, B.; van Roon, E.N. NSAID Use after Bariatric Surgery: A Randomized Controlled Intervention Study. Obes. Surg. 2016, 26, 2880–2885. [Google Scholar] [CrossRef] [PubMed]
- Abou Zeid, H.; Kallab, R.; Najm, M.A.; Jabbour, H.; Noun, R.; Sleilati, F. Safety and Efficacy of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Used for Analgesia After Bariatric Surgery: A Retrospective Case-Control Study. Obes. Surg. 2019, 29, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Thorell, A.; MacCormick, A.D.; Awad, S.; Reynolds, N.; Roulin, D.; Demartines, N. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2065–2083. [Google Scholar] [CrossRef] [Green Version]
- Yurashevich, M.; Pedro, C.; Fuller, M.; Habib, A.S. Intra-operative ketorolac 15 mg versus 30 mg for analgesia following cesarean delivery: A retrospective study. Int. J. Obstet. Anesth. 2020, 44, 116–121. [Google Scholar] [CrossRef]
- Motov, S.; Yasavolian, M.; Likourezos, A.; Pushkar, I.; Hossain, R.; Drapkin, J. Comparison of Intravenous Ketorolac at Three Single-Dose Regimens for Treating Acute Pain in the Emergency Department: A Randomized Controlled Trial. Ann. Emerg. Med. 2017, 70, 177–184. [Google Scholar] [CrossRef]
- Motov, S.; Masoudi, A.; Drapkin, J.; Sotomayor, C.; Kim, S.; Butt, M. Randomized Trial Comparing 3 Doses of Oral Ibuprofen for Management of Pain in Adult EM Patients. J. Emerg. Med. 2020, 59, 759–760. [Google Scholar] [CrossRef]
- Patel, A.S.; Abrecht, C.R.; Urman, R.D. Gabapentinoid Use in Perioperative Care and Current Controversies. Curr. Pain Headache Rep. 2022, 26, 139–144. [Google Scholar] [CrossRef]
- Fudin, J.; Persico, A. Analgesic Polypharmacy Is a Likely Link to Increased Hospital Admissions. Am. J. Nephrol. 2020, 51, 421–423. [Google Scholar] [CrossRef]
- Goodman, C.W.; Brett, A.S. Gabapentinoids for Pain: Potential Unintended Consequences. Am. Fam. Physician 2019, 100, 672–675. [Google Scholar] [PubMed]
- Liu, B.; Liu, R.; Wang, L. A meta-analysis of the preoperative use of gabapentinoids for the treatment of acute postoperative pain following spinal surgery. Medicine 2017, 96, e8031. [Google Scholar] [CrossRef] [PubMed]
- Kharasch, E.D.; Clark, J.D.; Kheterpal, S. Perioperative Gabapentinoids: Deflating the Bubble. Anesthesiology 2020, 133, 251–254. [Google Scholar] [CrossRef]
- Waddy, S.P.; Becerra, A.Z.; Ward, J.B.; Chan, K.E.; Fwu, C.-W.; Eggers, P.W. Concomitant Use of Gabapentinoids with Opioids Is Associated with Increased Mortality and Morbidity among Dialysis Patients. Am. J. Nephrol. 2020, 51, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Aschenbrenner, D.S. New Warning for Gabapentinoids. Am. J. Nurs. 2020, 120, 22. [Google Scholar] [CrossRef]
- Verret, M.; Lauzier, F.; Zarychanski, R.; Perron, C.; Savard, X.; Pinard, A.-M. Perioperative Use of Gabapentinoids for the Management of Postoperative Acute Pain: A Systematic Review and Meta-analysis. Anesthesiology 2020, 133, 265–279. [Google Scholar] [CrossRef]
- Baos, S.; Rogers, C.A.; Abbadi, R.; Alzetani, A.; Casali, G.; Chauhan, N. Effectiveness, cost-effectiveness and safety of gabapentin versus placebo as an adjunct to multimodal pain regimens in surgical patients: Protocol of a placebo controlled randomised controlled trial with blinding (GAP study). BMJ Open 2020, 10, e041176. [Google Scholar] [CrossRef]
- Schwenk, E.S.; Pradhan, B.; Nalamasu, R.; Stolle, L.; Wainer, I.W.; Cirullo, M. Ketamine in the Past, Present, and Future: Mechanisms, Metabolites, and Toxicity. Curr. Pain Headache Rep. 2021, 25, 57. [Google Scholar] [CrossRef]
- Hurth, K.P.; Jaworski, A.; Thomas, K.B.; Kirsch, W.B.; Rudoni, M.A.; Wohlfarth, K.M. The Reemergence of Ketamine for Treatment in Critically Ill Adults. Crit. Care Med. 2020, 48, 899–911. [Google Scholar] [CrossRef]
- Schwenk, E.S.; Viscusi, E.R.; Buvanendran, A.; Hurley, R.W.; Wasan, A.D.; Narouze, S. Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg. Anesth. Pain Med. 2018, 43, 456–466. [Google Scholar] [CrossRef]
- Cohen, S.P.; Bhatia, A.; Buvanendran, A.; Schwenk, E.S.; Wasan, A.D.; Hurley, R.W. Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Chronic Pain From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg. Anesth. Pain Med. 2018, 43, 521–546. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.A.; Hedrick, T.L.; Jayaram, J.; Argoff, C.; Gulur, P.; Holubar, S.D. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Management of Patients on Preoperative Opioid Therapy. Anesth. Analg. 2019, 129, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Natoli, S. The multiple faces of ketamine in anaesthesia and analgesia. Drugs Context 2021, 10, 2020-12-8. [Google Scholar] [CrossRef]
- Kreutzwiser, D.; Tawfic, Q.A. Expanding Role of NMDA Receptor Antagonists in the Management of Pain. CNS Drugs 2019, 33, 347–374. [Google Scholar] [CrossRef] [PubMed]
- Radvansky, B.M.; Shah, K.; Parikh, A.; Sifonios, A.N.; Le, V.; Eloy, J.D. Role of ketamine in acute postoperative pain management: A narrative review. Biomed. Res. Int. 2015, 2015, 749837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balzer, N.; McLeod, S.L.; Walsh, C.; Grewal, K. Low-dose Ketamine For Acute Pain Control in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2021, 28, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Bowers, K.J.; McAllister, K.B.; Ray, M.; Heitz, C. Ketamine as an Adjunct to Opioids for Acute Pain in the Emergency Department: A Randomized Controlled Trial. Acad. Emerg. Med. 2017, 24, 676–685. [Google Scholar] [CrossRef] [Green Version]
- Brinck, E.C.; Tiippana, E.; Heesen, M.; Bell, R.F.; Straube, S.; Moore, R.A. Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2018, 12, CD012033. [Google Scholar] [CrossRef]
- Stoker, A.D.; Rosenfeld, D.M.; Buras, M.R.; Alvord, J.M.; Gorlin, A.W. Evaluation of Clinical Factors Associated with Adverse Drug Events in Patients Receiving Sub-Anesthetic Ketamine Infusions. J. Pain Res. 2019, 12, 3413–3421. [Google Scholar] [CrossRef] [Green Version]
- Schwenk, E.S.; Goldberg, S.F.; Patel, R.D.; Zhou, J.; Adams, D.R.; Baratta, J.L. Adverse Drug Effects and Preoperative Medication Factors Related to Perioperative Low-Dose Ketamine Infusions. Reg. Anesth. Pain Med. 2016, 41, 482–487. [Google Scholar] [CrossRef]
- Kugler, N.W.; Carver, T.W.; Juul, J.; Peppard, W.J.; Boyle, K.; Drescher, K.M. Ketamine infusion for pain control in elderly patients with multiple rib fractures: Results of a randomized controlled trial. J. Trauma Acute Care Surg. 2019, 87, 1181–1188. [Google Scholar] [CrossRef]
- Motov, S.; Mann, S.; Drapkin, J.; Butt, M.; Likourezos, A.; Yetter, E. Intravenous subdissociative-dose ketamine versus morphine for acute geriatric pain in the Emergency Department: A randomized controlled trial. Am. J. Emerg. Med. 2019, 37, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Lovett, S.; Reed, T.; Riggs, R.; Lew, G.; Koch, E.; Durazo-Arvizu, R.A. A randomized, noninferiority, controlled trial of two doses of intravenous subdissociative ketamine for analgesia in the emergency department. Acad. Emerg. Med. 2021, 28, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Motov, S.; Mai, M.; Pushkar, I.; Likourezos, A.; Drapkin, J.; Yasavolian, M. A prospective randomized, double-dummy trial comparing IV push low dose ketamine to short infusion of low dose ketamine for treatment of pain in the ED. Am. J. Emerg. Med. 2017, 35, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.J.; Kim, Y.I.; Koo, Y.H.; Oh, H.-C.; Kang, H. Perioperative magnesium for postoperative analgesia: An umbrella review of systematic reviews and updated meta-analysis of randomized controlled trials. J. Pers. Med. 2021, 11, 1273. [Google Scholar] [CrossRef]
- Wheeler, K.E.; Grilli, R.; Centofanti, J.E.; Martin, J.; Gelinas, C.; Szumita, P.M. Adjuvant Analgesic Use in the Critically Ill: A Systematic Review and Meta-Analysis. Crit. Care Explor. 2020, 2, e0157. [Google Scholar] [CrossRef]
- Smith, H.S. The metabolism of opioid agents and the clinical impact of their active metabolites. Clin. J. Pain 2011, 27, 824–838. [Google Scholar] [CrossRef]
- Puntillo, F.; Giglio, M.; Varrassi, G. The Routes of Administration for Acute Postoperative Pain Medication. Pain Ther. 2021, 10, 909–925. [Google Scholar] [CrossRef]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 110, 888–896. [Google Scholar] [CrossRef]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Klein, T.E.; Caudle, K.E. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin. Pharmacol. Ther. 2014, 95, 376–382. [Google Scholar] [CrossRef]
- Ren, Z.-Y.; Xu, X.-Q.; Bao, Y.-P.; He, J.; Shi, L.; Deng, J.-H. The impact of genetic variation on sensitivity to opioid analgesics in patients with postoperative pain: A systematic review and meta-analysis. Pain Physician 2015, 18, 131–152. [Google Scholar]
- Coller, J.K.; Christrup, L.L.; Somogyi, A.A. Role of active metabolites in the use of opioids. Eur. J. Clin. Pharmacol. 2009, 65, 121–139. [Google Scholar] [CrossRef] [PubMed]
- Overholser, B.R.; Foster, D.R. Opioid pharmacokinetic drug-drug interactions. Am. J. Manag. Care 2011, 17 (Suppl. 11), S276–S287. [Google Scholar] [PubMed]
- Davison, S.N. Clinical Pharmacology Considerations in Pain Management in Patients with Advanced Kidney Failure. Clin. J. Am. Soc. Nephrol. 2019, 14, 917–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miotto, K.; Cho, A.K.; Khalil, M.A.; Blanco, K.; Sasaki, J.D.; Rawson, R. Trends in Tramadol: Pharmacology, Metabolism, and Misuse. Anesth. Analg. 2017, 124, 44–51. [Google Scholar] [CrossRef]
- “Weak” opioid analgesics. Codeine, dihydrocodeine and tramadol: No less risky than morphine. Prescrire Int. 2016, 25, 45–50.
- Brennan, M.J. The clinical implications of cytochrome p450 interactions with opioids and strategies for pain management. J Pain Symptom Manag. 2012, 44, S15–S22. [Google Scholar] [CrossRef]
- Baldo, B.A.; Pham, N.H. Histamine-releasing and allergenic properties of opioid analgesic drugs: Resolving the two. Anaesth. Intensive Care 2012, 40, 216–235. [Google Scholar] [CrossRef] [Green Version]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef] [Green Version]
- Washington State Agency Medical Directors’ Group (AMDG). AMDG—Interagency Guidelines. Available online: https://www.agencymeddirectors.wa.gov/guidelines (accessed on 1 December 2020).
- Wood, C. Effect of sublingual versus intravenous opioid administration on total opioid administration in patients following total knee arthroplasty. In Proceedings of the Great Lakes Pharmacy Residency Conference, West Lafayette, IN, USA, 20 April 2019; Pursue University: West Lafayette, IN, USA. [Google Scholar]
- Sorrel, D.C. (Ed.) Access Device Standards. Oncology Nursing Society (ONS), Pittsburgh, PA. 2017. Available online: https://www.ons.org/access-device-standards (accessed on 31 October 2022).
- Woelk, C.J. The hand that writes the opioid. Can. Fam. Physician. 2007, 53, 1015–1017. [Google Scholar]
- Alvaro, D.; Caraceni, A.T.; Coluzzi, F.; Gianni, W.; Lugoboni, F.; Marinangeli, F. What to do and what not to do in the management of opioid-induced constipation: A Choosing Wisely report. Pain Ther. 2020, 9, 657–667. [Google Scholar] [CrossRef]
- Gonzales, L.K.; Delmastro, M.A.; Boyd, D.M.; Sterling, M.L.; Aube, P.A.; Le, R.N. Adjusting Bowel Regimens When Prescribing Opioids in Women Receiving Palliative Care in the Acute Care Setting. Am. J. Hosp. Palliat. Care 2016, 33, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Müller-Lissner, S.; Bassotti, G.; Coffin, B.; Drewes, A.M.; Breivik, H.; Eisenberg, E. Opioid-induced constipation and bowel dysfunction: A clinical guideline. Pain Med. 2017, 18, 1837–1863. [Google Scholar] [CrossRef] [PubMed]
- Drewes, A.M.; Munkholm, P.; Simrén, M.; Breivik, H.; Kongsgaard, U.E.; Hatlebakk, J.G. Definition, diagnosis and treatment strategies for opioid-induced bowel dysfunction-Recommendations of the Nordic Working Group. Scand. J. Pain 2016, 11, 111–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warden, V.; Hurley, A.C.; Volicer, L. Development and psychometric evaluation of the Pain Assessment in Advanced Dementia (PAINAD) scale. J. Am. Med. Dir. Assoc. 2003, 4, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ahlers, S.J.G.M.; van der Veen, A.M.; van Dijk, M.; Tibboel, D.; Knibbe, C.A.J. The use of the Behavioral Pain Scale to assess pain in conscious sedated patients. Anesth. Analg. 2010, 110, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Wong-Baker FACES Pain Rating Scale. Wong-Baker FACES Foundation [Internet]. 8 June 2015. Available online: https://wongbakerfaces.org/ (accessed on 31 October 2022).
- List of Clinically Tested and Validated Pain Scales. Practical Pain Management [Internet]. 29 April 2019. Available online: https://www.practicalpainmanagement.com/resource-centers/opioid-prescribing-monitoring/list-clinically-tested-validated-pain-scales (accessed on 31 October 2022).
- Swarm, R.A.; Paice, J.A.; Anghelescu, D.L.; Are, M.; Bruce, J.Y.; Buga, S. Adult Cancer Pain, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 977–1007. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Fanciullo, G.J.; Fine, P.G.; Adler, J.A.; Ballantyne, J.C.; Davies, P. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J. Pain 2009, 10, 113–130. [Google Scholar] [CrossRef] [Green Version]
- The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update. J. Addict. Med. 2020, 14, 1–91. [CrossRef]
- Words Matter—Terms to Use and Avoid When Talking About Addiction. In: National Institute on Drug Abuse [Internet]. 29 November 2021. Available online: https://nida.nih.gov/nidamed-medical-health-professionals/health-professions-education/words-matter-terms-to-use-avoid-when-talking-about-addiction (accessed on 24 October 2022).
- Huxtable, C.A.; Roberts, L.J.; Somogyi, A.A.; MacIntyre, P.E. Acute pain management in opioid-tolerant patients: A growing challenge. Anaesth. Intensive Care 2011, 39, 804–823. [Google Scholar] [CrossRef] [Green Version]
- Genord, C.; Frost, T.; Eid, D. Opioid exit plan: A pharmacist’s role in managing acute postoperative pain. J. Am. Pharm. Assoc. 2017, 57, S92–S98. [Google Scholar] [CrossRef] [Green Version]
- Li, W.T.; Bell, K.L.; Yayac, M.; Barmann, J.A.; Star, A.M.; Austin, M.S. A postdischarge multimodal pain management cocktail following total knee arthroplasty reduces opioid consumption in the 30-day postoperative period: A group-randomized trial. J. Arthroplasty 2021, 36, 164–172. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, R.; Pattullo, G. Management of postsurgical pain in the community. Aust. Prescr. 2020, 43, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Loomis, E.A.; McNaughton, D.; Genord, C. A Quality Improvement Initiative Addressing Safe Opioid Prescribing and Disposal Postcesarean Delivery. Pain Manag. Nurs. 2022, 23, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Hite, M.; Dippre, A.; Heldreth, A.; Cole, D.; Lockett, M.; Klauber-DeMore, N. A Multifaceted Approach to Opioid Education, Prescribing, and Disposal for Patients with Breast Cancer Undergoing Surgery. J. Surg. Res. 2021, 257, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Patient Counseling. Michigan OPEN [Internet]. Available online: https://michigan-open.org/prescribing-recommendations/patient-counseling/ (accessed on 22 December 2020).
- Helpful Materials for Patients. The Centers for Disease Control and Prevention (CDC) [Internet]. 18 August 2021. Available online: https://www.cdc.gov/opioids/patients/materials.html (accessed on 24 October 2022).
- Prescribing Recommendations. Michigan OPEN [Internet]. Available online: https://michigan-open.org/prescribing-recommendations/ (accessed on 14 September 2020).
- Dr. Robert Bree Collaborative and Washington State Agency Medical Directors’ Group. Prescribing Opioids for Postoperative Pain—Supplemental Guidance. July 2018. Available online: http://www.agencymeddirectors.wa.gov/Files/FinalSupBreeAMDGPostopPain091318wcover.pdf (accessed on 15 September 2022).
- Overton, H.N.; Hanna, M.N.; Bruhn, W.E.; Hutfless, S.; Bicket, M.C.; Makary, M.A. Opioid-Prescribing Guidelines for Common Surgical Procedures: An Expert Panel Consensus. J. Am. Coll. Surg. 2018, 227, 411–418. [Google Scholar] [CrossRef]
- Thiels, C.A.; Ubl, D.S.; Yost, K.J.; Dowdy, S.C.; Mabry, T.M.; Gazelka, H.M. Results of a Prospective, Multicenter Initiative Aimed at Developing Opioid-prescribing Guidelines After Surgery. Ann. Surg. 2018, 268, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.V.; Stucke, R.S.; Billmeier, S.E.; Kelly, J.L.; Barth, R.J., Jr. Guideline for Discharge Opioid Prescriptions after Inpatient General Surgical Procedures. J. Am. Coll. Surg. 2018, 226, 996–1003. [Google Scholar] [CrossRef]
- Brummett, C.M.; Waljee, J.F.; Goesling, J.; Moser, S.; Lin, P.; Englesbe, M.J. New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults. JAMA Surg. 2017, 152, e170504. [Google Scholar] [CrossRef]
- El Moheb, M.; Mokhtari, A.; Han, K.; van Erp, I.; Kongkaewpaisan, N.; Jia, Z. Pain or No Pain, We Will Give You Opioids: Relationship Between Number of Opioid Pills Prescribed and Severity of Pain after Operation in US vs Non-US Patients. J. Am. Coll. Surg. 2020, 231, 639–648. [Google Scholar] [CrossRef]
- Varley, P.R.; Zuckerbraun, B.S. Opioid Stewardship and the Surgeon. JAMA Surg. 2018, 153, e174875. [Google Scholar] [CrossRef]
- Kelley-Quon, L.I.; Kirkpatrick, M.G.; Ricca, R.L.; Baird, R.; Harbaugh, C.M.; Brady, A. Guidelines for Opioid Prescribing in Children and Adolescents After Surgery: An Expert Panel Opinion. JAMA Surg. 2021, 156, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Berna, C.; Kulich, R.J.; Rathmell, J.P. Tapering Long-term Opioid Therapy in Chronic Noncancer Pain: Evidence and Recommendations for Everyday Practice. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2015; Volume 90, pp. 828–842. [Google Scholar] [CrossRef]
- Compton, P.; Aronowitz, S.V.; Klusaritz, H.; Anderson, E. Acute pain and self-directed discharge among hospitalized patients with opioid-related diagnoses: A cohort study. Harm Reduct. J. 2021, 18, 131. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; King, A.B.; Geiger, T.M.; Grant, M.C.; Grocott, M.P.W.; Gupta, R. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Opioid Minimization in Opioid-Naïve Patients. Anesth. Analg. 2019, 129, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Compton, P. Acute Pain Management for Patients Receiving Medication-Assisted Therapy. AACN Adv. Crit. Care 2019, 30, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Nolan, S.; Beaulieu, T.; Shalansky, S.; Ti, L. Inappropriate opioid prescribing practices: A narrative review. Am. J. Health Syst. Pharm. 2019, 76, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Parhami, I.; Massey, J.; Trimzi, I.; Huckshorn, K.; Gallucci, G. Risks Associated with Co-Prescribing Opioids and Benzodiazepines and Delaware’s Prescription Drug Monitoring Program. Del. Med. J. 2015, 87, 270–274. [Google Scholar]
- Babalonis, S.; Walsh, S.L. Warnings Unheeded:The Risks of Co-Prescribing Opioids and Benzodiazepines. Pain Clin. Updates 2015, 23, 1–7. [Google Scholar]
- Kerensky, T.; Walley, A.Y. Opioid overdose prevention and naloxone rescue kits: What we know and what we don’t know. Addict. Sci. Clin. Pract. 2017, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- White, N.D. Increasing Naloxone Access and Use to Prevent Opioid Overdose Death and Disability. Am. J. Lifestyle Med. 2019, 13, 33–35. [Google Scholar] [CrossRef]
- Klimas, J.; Egan, M.; Tobin, H.; Coleman, N.; Bury, G. Development and process evaluation of an educational intervention for overdose prevention and naloxone distribution by general practice trainees. BMC Med. Educ. 2015, 15, 206. [Google Scholar] [CrossRef] [Green Version]
- McAuley, A.; Aucott, L.; Matheson, C. Exploring the life-saving potential of naloxone: A systematic review and descriptive meta-analysis of take home naloxone (THN) programmes for opioid users. Int. J. Drug Policy 2015, 26, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services; Office of the Surgeon General. U.S. Surgeon General’s Advisory on Naloxone and Opioid Overdose. HHS.Gov [Internet]. 3 April 2018. Available online: https://www.hhs.gov/surgeongeneral/reports-and-publications/addiction-and-substance-misuse/advisory-on-naloxone/index.html (accessed on 25 October 2022).
- The Lancet. Take-home naloxone: A life saver in opioid overdose. Lancet 2019, 393, 296. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.; Bratberg, J.P.; Davis, C.S.; Green, T.C.; Walley, A.Y. Prescribe to Prevent: Overdose Prevention and Naloxone Rescue Kits for Prescribers and Pharmacists. J. Addict. Med. 2016, 10, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Prescribe to Prevent. Available online: https://prescribetoprevent.org/ (accessed on 29 October 2022).
- How to Respond to an Opioid Overdose. HHS.Gov [Internet]. 18 April 2018. Available online: https://www.hhs.gov/opioids/treatment/overdose-response/index.html (accessed on 29 October 2022).
- Veazie, S.; Mackey, K.; Peterson, K.; Bourne, D. Managing Acute Pain in Patients Taking Medication for Opioid Use Disorder: A Rapid Review. J. Gen. Intern. Med. 2020, 35, 945–953. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.N.; Quaye, A.N.-A.; Wilens, T.E. Opioid use disorders: Perioperative management of a special population. Anesth. Analg. 2018, 127, 539. [Google Scholar] [CrossRef] [PubMed]
- Koller, G.; Schwarzer, A.; Halfter, K.; Soyka, M. Pain management in opioid maintenance treatment. Expert Opin. Pharm. 2019, 20, 1993–2005. [Google Scholar] [CrossRef]
- Lau, F.; Gardiner, M. Oxycodone/naloxone: An unusual adverse drug reaction. Aust. Fam. Physician 2017, 46, 42–43. [Google Scholar]
- Lembke, A.; Ottestad, E.; Schmiesing, C. Patients Maintained on Buprenorphine for Opioid Use Disorder Should Continue Buprenorphine Through the Perioperative Period. Pain Med. 2019, 20, 425–428. [Google Scholar] [CrossRef] [Green Version]
- Houchard, G.; Kullgren, J.; Saphire, M.; Porter, K.; Abel, S. Hospital Opioid Requirements Following Continuation Versus Discontinuation of Buprenorphine for Addiction—A Retrospective Cohort Study. J Pain Palliat. Care Pharm. 2019, 33, 98–106. [Google Scholar] [CrossRef]
- Quaye, A.; Potter, K.; Roth, S.; Acampora, G.; Mao, J.; Zhang, Y. Perioperative Continuation of Buprenorphine at Low-Moderate Doses Was Associated with Lower Postoperative Pain Scores and Decreased Outpatient Opioid Dispensing Compared with Buprenorphine Discontinuation. Pain Med. 2020, 21, 1955–1960. [Google Scholar] [CrossRef]
- Macintyre, P.E.; Russell, R.A.; Usher, K.A.N.; Gaughwin, M.; Huxtable, C.A. Pain relief and opioid requirements in the first 24 hours after surgery in patients taking buprenorphine and methadone opioid substitution therapy. Anaesth. Intensive Care 2013, 41, 222–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohan, L.; Potru, S.; Barreveld, A.M.; Sprintz, M.; Lane, O.; Aryal, A. Buprenorphine management in the perioperative period: Educational review and recommendations from a multisociety expert panel. Reg. Anesth. Pain Med. 2021, 46, 840–859. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Azargive, S.; Weissman, J.S.; Shanthanna, H.; Hanlon, J.G.; Samman, B. Perioperative Pain and Addiction Interdisciplinary Network (PAIN) clinical practice advisory for perioperative management of buprenorphine: Results of a modified Delphi process. Br. J. Anaesth. 2019, 123, e333–e342. [Google Scholar] [CrossRef] [PubMed]
- Alford, D.P.; Compton, P.; Samet, J.H. Acute pain management for patients receiving maintenance methadone or buprenorphine therapy. Ann. Intern. Med. 2006, 144, 127–134. [Google Scholar] [CrossRef]
- Sudakin, D. Naltrexone: Not Just for Opioids Anymore. J. Med. Toxicol. 2016, 12, 71–75. [Google Scholar] [CrossRef]
- Simpson, G.K.; Jackson, M. Perioperative management of opioid-tolerant patients. BJA Educ. 2017, 17, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Harrison, T.K.; Kornfeld, H.; Aggarwal, A.K.; Lembke, A. Perioperative Considerations for the Patient with Opioid Use Disorder on Buprenorphine, Methadone, or Naltrexone Maintenance Therapy. Anesth. Clin. 2018, 36, 345–359. [Google Scholar] [CrossRef]
- Sen, S.; Arulkumar, S.; Cornett, E.M.; Gayle, J.A.; Flower, R.R.; Fox, C.J. New pain management options for the surgical patient on methadone and buprenorphine. Curr. Pain Headache Rep. 2016, 20, 16. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concern | Evidence | Recommendation |
|---|---|---|
| Bleeding/antiplatelet effects | Bleeding times and perioperative bleeding events are not significantly affected by NSAIDs at usual doses; GI complications from NSAID-induced prostaglandin inhibition are not increased by short-term use (<7 days); These risks may be further mitigated by using a COX-2 selective agent since antiplatelet effects are mediated by COX-1 inhibition | Do not withhold NSAIDs in acute pain due to bleeding concerns as long as usual analgesic doses and short-term durations are employed; selective COX-2 inhibitors or concomitant gastroprotective agents may be considered in patients at high GI bleed risk |
| Wound healing issues or orthopedic/spinal nonunion after fracture or fusion surgery | Older data from animal and limited retrospective studies suggested these concerns, however more recent and higher quality prospective studies have not replicated | NSAIDs, especially COX-2 selective agents, appear efficacious and safe for short-term use in orthopedic and spinal surgery and should be routinely considered based on risks/benefits |
| Anastomotic leak after GI surgery | Some studies have suggested increased risk of anastomotic leakage with nonselective NSAIDS, but selective COX-2 inhibitors were not associated with this risk in recent meta-analyses | Do not withhold COX-2 selective NSAIDs in GI surgery patients |
| MACE after cardiac surgery | COX-2 selective inhibitors have been associated with increased rates of MACE after cardiac surgery, likely due to an unfavorable effect on pro-thrombotic pathways | COX-2 selective agents should be avoided in cardiac surgery, however, nonselective NSAIDs have been used safely in cardiac surgery, and COX-2 selective agents have been used safely in patients with cardiac disease undergoing noncardiac surgery |
| Sulfa allergy | While some NSAIDs contain a sulfur-containing moiety, these are not structurally the same as sulfa antibiotics; patients with sulfa allergies have been found to be no more likely to have allergic reactions to NSAIDs than patients without sulfa allergies | Do not withhold NSAIDs, including celecoxib, in patients with sulfa (sulfonamide antibiotic) allergies |
| Gastritis/pouchitis in patients s/p bariatric surgery | Patients s/p bariatric surgery should avoid chronic NSAID exposure, however, short-term use is supported by current guidelines as safe and beneficial | Do not withhold short-term NSAIDs in acute pain in patients s/p bariatric surgery; use of a COX-2 selective agent and/or temporary PPI therapy may be considered to decrease GI risk |
| Kidney injury | NSAIDs inhibit prostaglandin-dependent mechanisms of preserving renal perfusion and GFR in times of decreased renal blood flow, increasing risk for acute and chronic kidney injury in at-risk populations | All NSAIDs and COX-2 inhibitors should generally be avoided in patients with AKI or CKD |
| Large doses must be used for analgesia | The maximum effective analgesic dose of ketorolac is approximately 10–15 mg and is approximately 400 mg for ibuprofen based on available dose-finding studies, though higher doses may confer additional anti-inflammatory benefit | When using NSAIDs primarily to treat pain, doses should generally not exceed their analgesic ceiling in order to limit adverse effects |
| Pain Scale 1 | Description | Intended Population |
|---|---|---|
| Visual Analog Scale | numerical scale rating 1–10 | adults who are able to self-report pain |
| Wong-Baker Faces | scale utilizing facial expressions linked to pain severity | patients age 3 and above |
| Pain Assessment in Advanced Dementia (PAINAD) | utilizes non-verbal cues to assess pain | patients with dementia, unable to self-report |
| Behavioral Pain Scale | observational assessment | critically ill, sedated patients |
| Defense and Veterans Pain Rating Scale (DVPRS) | combination graphic and numerical tool | adults who are able to self-report pain |
| Formulation/Route of Administration | Time to Peak1—Assess for Efficacy and Adverse Effects | Additional Considerations |
|---|---|---|
| Intravenous | 10–15 min | |
| Subcutaneous | 30 min | |
| Immediate release oral | 60 min | |
| Immediate release sublingual | 15–30 min | Assess patient ability to hold medication under the tongue |
| Regimen Component | Approach for Opioid-Naïve | Approach for Opioid-Tolerant |
|---|---|---|
| Goals of opioid tapering | Limit excess exposure to opioids and opioid-related adverse events once pain is improving, limit conversion to persistent opioid use if not otherwise indicated by patient condition, limit quantity of unused opioids | More complex and patient-specific, may entail tapering back to previous chronic pain or MOUD regimen (or reevaluating chronic regimen in concert with applicable prescriber), limiting opioid-related adverse events, avoiding relapse of OUD, limiting long-term adverse events related to chronic opioid exposure |
| Dose reduction at each step of taper | Consider decreasing daily dose by 20–25% | More gradual reductions may be needed at each step |
| Frequency of tapering | Every 1–2 days once pain is improving | Less frequent reductions are likely to be needed, consider every 2–7 days once acute pain improving |
| Total duration of taper | Most patients can successfully taper off opioids within 3–7 days after a major scheduled surgery, assuming multimodal and enhanced recovery techniques are used concurrently | Longer tapers will be needed, may take weeks to months to be successful depending on patient-specific circumstances |
| Other considerations | Consider reducing dose before lengthening dosing interval to help maintain smoother pain control without large peaks/valleys of analgesic effect | More multimodal therapies, psychosocial support, monitoring, and coordination of care often needed |
| Medication | Mechanism of Action | Acute Pain Strategies |
|---|---|---|
| Buprenorphine | Partial mu-opioid agonist, kappa-opioid antagonist | Continue home regimen; Split home regimen into TID dosing for same TDD |
| Methadone | Full mu-opioid agonist, NMDA antagonist | Continue home regimen; Split home regimen into TID dosing for same TDD |
| Naltrexone (IM) | Mu-opioid antagonist | Stop IM dose 30 days prior to painful procedure and until patient has been opioid-free for 3 days afterward; Multimodal therapies to treat painful crisis, consider ketamine and regional anesthesia |
| Naltrexone (PO) | Mu-opioid antagonist | Stop therapy 72 h prior to painful and until patient has been opioid-free for 3 days afterward; Multimodal therapies to treat painful crisis, consider ketamine and regional anesthesia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyland, S.J.; Wetshtein, A.M.; Grable, S.J.; Jackson, M.P. Acute Pain Management Pearls: A Focused Review for the Hospital Clinician. Healthcare 2023, 11, 34. https://doi.org/10.3390/healthcare11010034
Hyland SJ, Wetshtein AM, Grable SJ, Jackson MP. Acute Pain Management Pearls: A Focused Review for the Hospital Clinician. Healthcare. 2023; 11(1):34. https://doi.org/10.3390/healthcare11010034
Chicago/Turabian StyleHyland, Sara J., Andrea M. Wetshtein, Samantha J. Grable, and Michelle P. Jackson. 2023. "Acute Pain Management Pearls: A Focused Review for the Hospital Clinician" Healthcare 11, no. 1: 34. https://doi.org/10.3390/healthcare11010034