
Assessment of the Efficiency of Non-Invasive Diagnostic Imaging Modalities for Detecting Myocardial Ischemia in Patients Suspected of Having Stable Angina

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- Intermediate-to-high risk of major CAD events was expected from the results of the initial evaluation.
- The result of CCTA as an additional test was inconclusive.
- Coronary artery stenosis of uncertain functional significance was detected on CCTA.
- (1)
- CMRI (rest and stress perfusion MRI).
- (2)
- SPECT.
- (3)
- SE.
- (4)
- FFRCT (recent guidelines offered class 2a recommendations for FFRCT as a sequential or an add-on testing) [10].
- (5)
- PET.
2.2. Literature Search
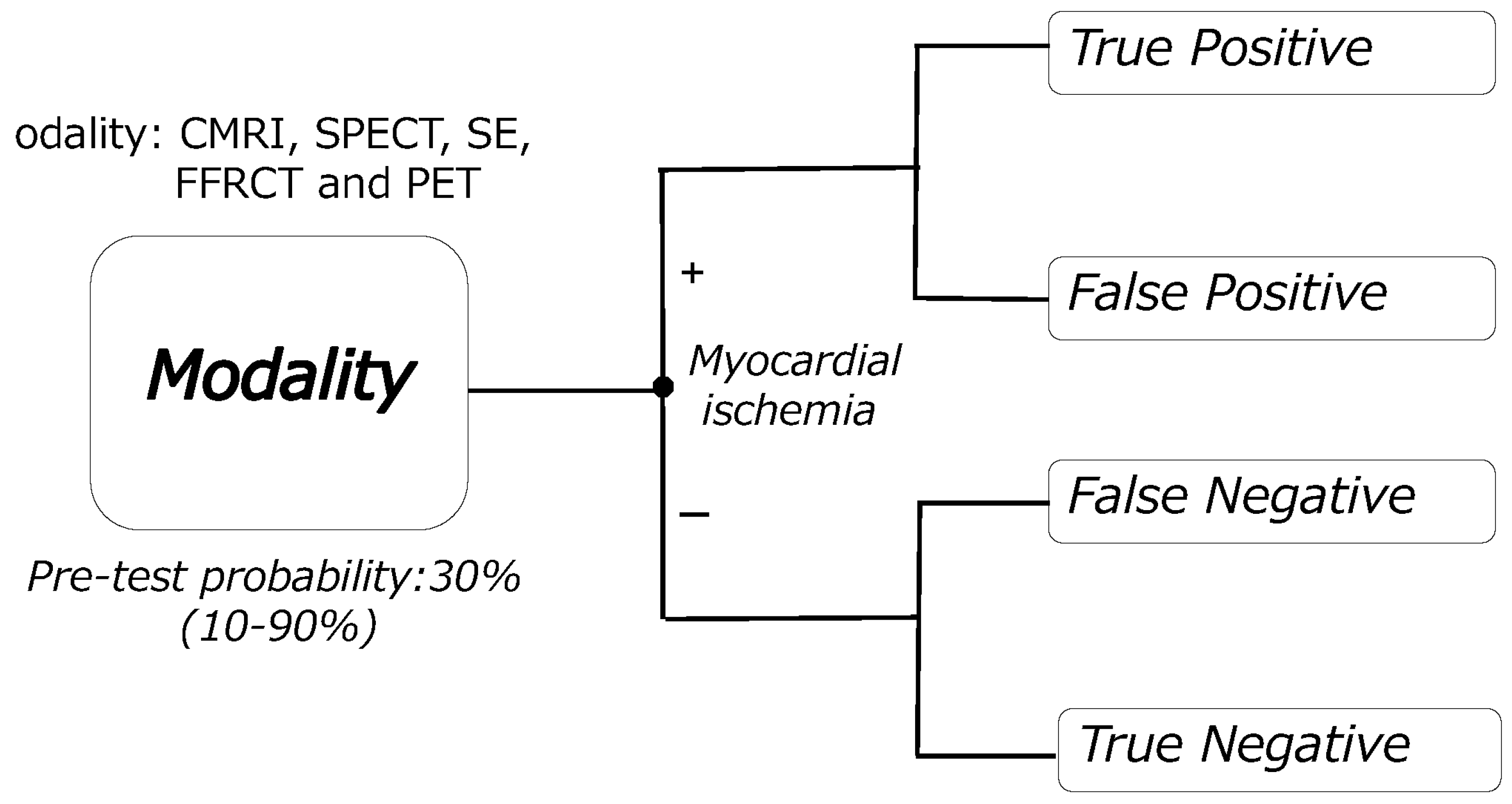
2.3. Definition of Efficiencies for Detecting Myocardial Ischemia
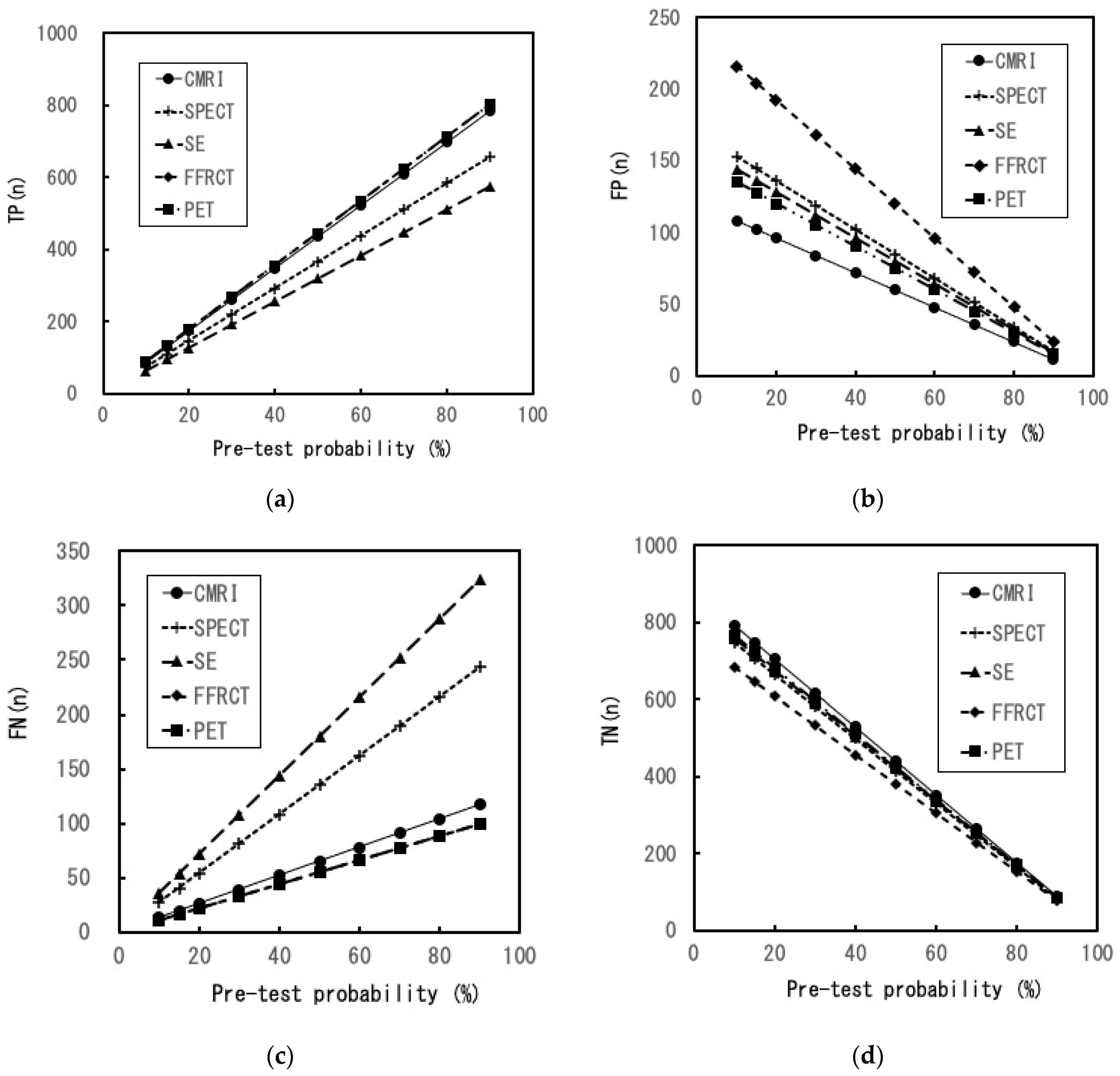
- (a)
- The number of true positive (TP), false positive (FP), false negative (FN), and true negative (TN) results per 1000 patients.
- (b)
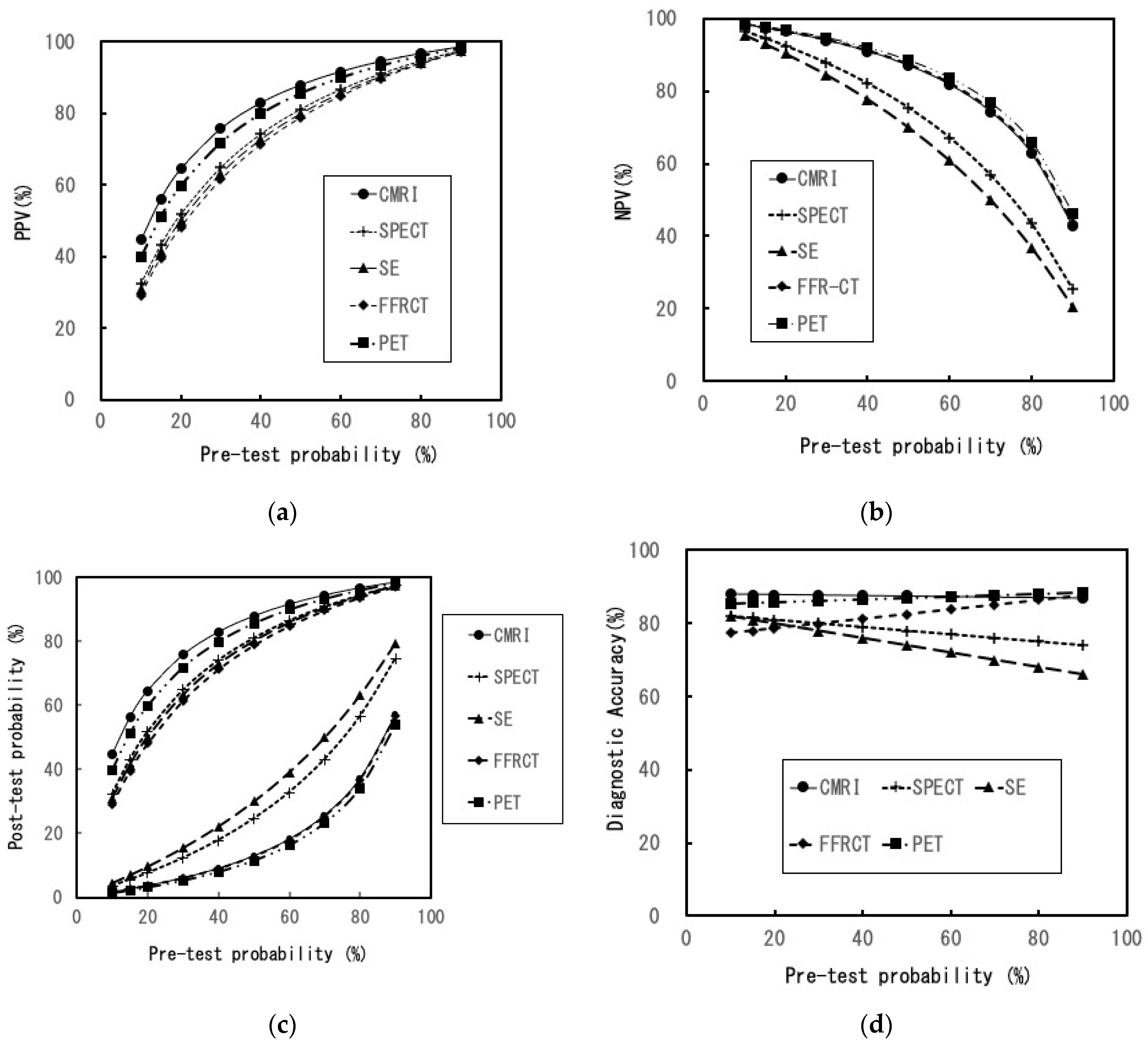
- Positive predictive value (PPV) = post-test probability (post-TP (for positive results)).
- (c)
- Negative predictive value (NPV).
- (d)
- Post-TP (for negative results) [18].
- (e)
- Diagnostic accuracy (DA).
- (f)
- Number needed to diagnose (NND) [19].
2.4. Calculation of Efficiencies
2.5. Sensitivity Analyses
2.6. Statistical Analysis
3. Results
3.1. Selected Literature
3.2. Efficiencies at the Basic Settings
3.3. Changes in Efficiencies in the Sensitivity Analyses
4. Discussion
- The maximum and minimum probabilities of a positive test result and having actual ischemia were 76% (CMRI) and 61% (FFRCT), respectively.
- The maximum and minimum probabilities of a negative test result and having no actual ischemia were 95% (PET) and 84% (SE), respectively.
- Despite a negative test result, the minimum and maximum probabilities of existing actual ischemia were 5.3% (PET) and 15.5% (SE), respectively.
- PET generated the best TP and NPV and the least FN among the five imaging modalities.
- CMRI generated the best DA, PPV, and TN and the least FP among the five imaging modalities.
- FFRCT generated the best TP and the least FN among the five imaging modalities but produced more FP results than did the rest.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- van Waardhuizen, C.N.; Khanji, M.Y.; Genders, T.S.S.; Ferket, B.S.; Fleischmann, K.E.; Hunink, M.G.M.; Petersen, S.E. Comparative cost-effectiveness of non-invasive imaging tests in patients presenting with chronic stable chest pain with suspected coronary artery disease: A systematic review. Eur. Heart J. Qual. Care Clin. Outcomes 2016, 2, 245–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewey, M.; Siebes, M.; Kachelriess, M.; Kofoed, K.F.; Maurovich-Horvat, P.; Nikolaou, K.; Bai, W.; Kofler, A.; Manka, R.; Kozerke, S.; et al. Clinical quantitative cardiac imaging for the assessment of myocardial ischaemia. Nat. Rev. Cardiol. 2020, 17, 427–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, P.H.; de Lemos, J.A. Diagnosis and Management of Stable Angina: A Review. JAMA J. Am. Med. Assoc. 2021, 325, 1765–1778. [Google Scholar] [CrossRef] [PubMed]
- Mordi, I.R.; Badar, A.A.; Irving, R.J.; Weir-McCall, J.R.; Houston, J.G.; Lang, C.C. Efficacy of noninvasive cardiac imaging tests in diagnosis and management of stable coronary artery disease. Vasc. Health Risk Manag. 2017, 13, 427–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balfour, P.C., Jr.; Gonzalez, J.A.; Kramer, C.M. Non-invasive assessment of low-and intermediate-risk patients with chest pain. Trends Cardiovasc Med. 2017, 27, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Jiang, B.; Cai, W.; Lv, X.; Liu, H. Diagnostic Performance and Clinical Utility of Myocardial Perfusion MRI for Coronary Artery Disease with Fractional Flow Reserve as the Standard Reference: A Meta-analysis. Heart Lung Circ. 2016, 25, 1031–1038. [Google Scholar] [CrossRef]
- Dai, N.; Zhang, X.; Zhang, Y.; Hou, L.; Li, W.; Fan, B.; Zhang, T.; Xu, Y. Enhanced diagnostic utility achieved by myocardial blood analysis: A meta-analysis of noninvasive cardiac imaging in the detection of functional coronary artery disease. Int. J. Cardiol. 2016, 221, 665–673. [Google Scholar] [CrossRef]
- Wu, W.; Pan, D.R.; Foin, N.; Pang, S.; Ye, P.; Holm, N.; Ren, X.M.; Luo, J.; Nanjundappa, A.; Chen, S.L. Noninvasive fractional flow reserve derived from coronary computed tomography angiography for identification of ischemic lesions: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 29409. [Google Scholar] [CrossRef] [Green Version]
- Ding, A.; Qiu, G.; Lin, W.; Hu, L.; Lu, G.; Long, X.; Hong, X.; Chen, Y.; Luo, X.; Tang, Q.; et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in ischemia-causing coronary stenosis: A meta-analysis. Jpn. J. Radiol. 2016, 34, 795–808. [Google Scholar] [CrossRef]
- Gulati, M.; Levy, P.D.; Mukherjee, D.; Amsterdam, E.; Bhatt, D.L.; Birtcher, K.K.; Blankstein, R.; Boyd, J.; Bullock-Palmer, R.P.; Conejo, T.; et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 30, e368–e454. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feger, S.; Ibes, P.; Napp, A.E.; Lembcke, A.; Laule, M.; Dreger, H.; Bokelmann, B.; Davis, G.K.; Roditi, G.; Diez, I.; et al. Clinical pre-test probability for obstructive coronary artery disease: Insights from the European DISCHARGE pilot study. Eur. Radiol. 2021, 31, 1471–1481. [Google Scholar] [CrossRef] [PubMed]
- Petitti, D.B. Meta-Analysis, Decision Analysis, and Cost-Effectiveness Analysis: Methods for Quantitative Synthesis in Medicine; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Zhuang, B.; Wang, S.; Zhao, S.; Lu, M. Computed tomography angiography-derived fractional flow reserve (CT-FFR) for the detection of myocardial ischemia with invasive fractional flow reserve as reference: Systematic review and meta-analysis. Eur. Radiol. 2020, 30, 712–725. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.S.; Rodriguez-Guadarrama, Y.; Rua, T.; Bui, K.H.; Buylova Gola, A.; Chiribiri, A.; McCrone, P.; Plein, S.; Pennington, M. Cost-effectiveness in diagnosis of stable angina patients: A decision-analytical modelling approach. Open Heart 2022, 9, e001700. [Google Scholar] [CrossRef]
- Chong, A.B.; Taylor, M.; Schubert, G.; Vassar, M. Interventional Radiology Clinical Practice Guideline Recommendations for Neurovascular Disorders Are Not Based on High-Quality Systematic Reviews. AJNR Am. J. Neuroradiol. 2017, 38, 759–765. [Google Scholar] [CrossRef] [Green Version]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA J. Am. Med. Assoc. 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Sox, H.; Stern, S.; Owens, D.; Abrams, H.L. Assessment of Diagnostic Technology in Health Care. In Assessment of Diagnostic Technology in Health Care: Rationale, Methods, Problems, and Directions: Monograph of the Council on Health Care Technology; National Academies Press: Washington, DC, USA, 1989. [Google Scholar]
- Larner, A.J. Number Needed to Diagnose, Predict, or Misdiagnose: Useful Metrics for Non-Canonical Signs of Cognitive Status? Dement. Geriatr. Cogn. Dis. Extra 2018, 8, 321–327. [Google Scholar] [CrossRef]
- Hsu, J.; Brozek, J.L.; Terracciano, L.; Kreis, J.; Compalati, E.; Stein, A.T.; Fiocchi, A.; Schunemann, H.J. Application of GRADE: Making evidence-based recommendations about diagnostic tests in clinical practice guidelines. Implement Sci. 2011, 6, 62. [Google Scholar] [CrossRef] [Green Version]
- Bing, R.; Singh, T.; Dweck, M.R.; Mills, N.L.; Williams, M.C.; Adamson, P.D.; Newby, D.E. Validation of European Society of Cardiology pre-test probabilities for obstructive coronary artery disease in suspected stable angina. Eur. Heart J. Qual Care Clin. Outcomes 2020, 6, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Ullah, W.; Roomi, S.; Abdullah, H.M.; Mukhtar, M.; Ali, Z.; Ye, P.; Haas, D.C.; Figueredo, V.M. Diagnostic Accuracy of Cardiac Magnetic Resonance Versus Fractional Flow Reserve: A Systematic Review and Meta-Analysis. Cardiol. Res. 2020, 11, 145–154. [Google Scholar] [CrossRef]
- Pontone, G.; Guaricci, A.I.; Palmer, S.C.; Andreini, D.; Verdecchia, M.; Fusini, L.; Lorenzoni, V.; Guglielmo, M.; Muscogiuri, G.; Baggiano, A.; et al. Diagnostic performance of non-invasive imaging for stable coronary artery disease: A meta-analysis. Int. J. Cardiol. 2020, 300, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Yu, S.Q.; Lu, M.J.; Zhao, S.H. Comparison of diagnostic accuracy of stress myocardial perfusion imaging for detecting hemodynamically significant coronary artery disease between cardiac magnetic resonance and nuclear medical imaging: A meta-analysis. Int. J. Cardiol. 2019, 293, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Ballo, H.; Juarez-Orozco, L.E.; Saraste, A.; Kolh, P.; Rutjes, A.W.S.; Juni, P.; Windecker, S.; Bax, J.J.; Wijns, W. The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina: A meta-analysis focused on post-test disease probability. Eur. Heart J. 2018, 39, 3322–3330. [Google Scholar] [CrossRef] [PubMed]
- Kiaos, A.; Tziatzios, I.; Hadjimiltiades, S.; Karvounis, C.; Karamitsos, T.D. Diagnostic performance of stress perfusion cardiac magnetic resonance for the detection of coronary artery disease: A systematic review and meta-analysis. Int. J. Cardiol. 2018, 252, 229–233. [Google Scholar] [CrossRef]
- Danad, I.; Szymonifka, J.; Twisk, J.W.R.; Norgaard, B.L.; Zarins, C.K.; Knaapen, P.; Min, J.K. Diagnostic performance of cardiac imaging methods to diagnose ischaemia-causing coronary artery disease when directly compared with fractional flow reserve as a reference standard: A meta-analysis. Eur. Heart J. 2017, 38, 991–998. [Google Scholar] [CrossRef] [Green Version]
- Takx, R.A.; Blomberg, B.A.; El Aidi, H.; Habets, J.; de Jong, P.A.; Nagel, E.; Hoffmann, U.; Leiner, T. Diagnostic accuracy of stress myocardial perfusion imaging compared to invasive coronary angiography with fractional flow reserve meta-analysis. Circulation. Cardiovasc. Imaging 2015, 8, e002666. [Google Scholar] [CrossRef] [Green Version]
- Tang, C.X.; Wang, Y.N.; Zhou, F.; Schoepf, U.J.; Assen, M.V.; Stroud, R.E.; Li, J.H.; Zhang, X.L.; Lu, M.J.; Zhou, C.S.; et al. Diagnostic performance of fractional flow reserve derived from coronary CT angiography for detection of lesion-specific ischemia: A multi-center study and meta-analysis. Eur. J. Radiol. 2019, 116, 90–97. [Google Scholar] [CrossRef]
- Hamon, M.; Geindreau, D.; Guittet, L.; Bauters, C.; Hamon, M. Additional diagnostic value of new CT imaging techniques for the functional assessment of coronary artery disease: A meta-analysis. Eur. Radiol. 2019, 29, 3044–3061. [Google Scholar] [CrossRef]
- Celeng, C.; Leiner, T.; Maurovich-Horvat, P.; Merkely, B.; de Jong, P.; Dankbaar, J.W.; van Es, H.W.; Ghoshhajra, B.B.; Hoffmann, U.; Takx, R.A.P. Anatomical and Functional Computed Tomography for Diagnosing Hemodynamically Significant Coronary Artery Disease: A Meta-Analysis. JACC. Cardiovasc. Imaging 2019, 12, 1316–1325. [Google Scholar] [CrossRef]
- Panchal, H.B.; Veeranki, S.P.; Bhatheja, S.; Barry, N.; Mahmud, E.; Budoff, M.; Lavine, S.J.; Mamudu, H.M.; Paul, T.K. Fractional flow reserve using computed tomography for assessing coronary artery disease: A meta-analysis. J. Cardiovasc. Med. 2016, 17, 694–700. [Google Scholar] [CrossRef]
- Gonzalez, J.A.; Lipinski, M.J.; Flors, L.; Shaw, P.W.; Kramer, C.M.; Salerno, M. Meta-Analysis of Diagnostic Performance of Coronary Computed Tomography Angiography, Computed Tomography Perfusion, and Computed Tomography-Fractional Flow Reserve in Functional Myocardial Ischemia Assessment Versus Invasive Fractional Flow Reserve. Am. J. Cardiol. 2015, 116, 1469–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, S.B.; Jing, X.D.; Wang, J.; Huang, C.; Xia, S.; Du, J.L.; Liu, Y.J.; She, Q. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in coronary artery disease: A systematic review and meta-analysis. Int. J. Cardiol. 2015, 184, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, F.; Yadollahie, M. Number needed to misdiagnose: A measure of diagnostic test effectiveness. Epidemiology 2013, 24, 170. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.P.; Seo, J.K.; Hwang, I.C.; Park, J.B.; Park, E.A.; Lee, W.; Paeng, J.C.; Lee, H.J.; Yoon, Y.E.; Kim, H.L.; et al. Coronary computed tomography angiography vs. myocardial single photon emission computed tomography in patients with intermediate risk chest pain: A randomized clinical trial for cost-effectiveness comparison based on real-world cost. Eur. Heart J. Cardiovasc Imaging 2019, 20, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Bertoldi, E.G.; Stella, S.F.; Rohde, L.E.; Polanczyk, C.A. Long-term Cost-Effectiveness of Diagnostic Tests for Assessing Stable Chest Pain: Modeled Analysis of Anatomical and Functional Strategies. Clin. Cardiol. 2016, 39, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Shaw, L.J.; Marwick, T.H.; Berman, D.S.; Sawada, S.; Heller, G.V.; Vasey, C.; Miller, D.D. Incremental cost-effectiveness of exercise echocardiography vs. SPECT imaging for the evaluation of stable chest pain. Eur. Heart J. 2006, 27, 2448–2458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckert, D.; Witzel, S.; Cieslik, M.; Tibi, R.; Rottbauer, W.; Bernhardt, P. Magnetic resonance Adenosine perfusion imaging as Gatekeeper of invasive coronary intervention (MAGnet): Study protocol for a randomized controlled trial. Trials 2017, 18, 358. [Google Scholar] [CrossRef] [PubMed]
- Ko, B.S.; Wong, D.T.; Cameron, J.D.; Leong, D.P.; Leung, M.; Meredith, I.T.; Nerlekar, N.; Antonis, P.; Crossett, M.; Troupis, J.; et al. 320-row CT coronary angiography predicts freedom from revascularisation and acts as a gatekeeper to defer invasive angiography in stable coronary artery disease: A fractional flow reserve-correlated study. Eur. Radiol. 2014, 24, 738–747. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Reference Standard (Invasive FFR) | |||
|---|---|---|---|
| Myocardial Ischemia (+) | Myocardial Ischemia (−) | ||
| Index Test | Positive | TP = Sensitivity × PTP × 1000 | FP = (1 − Specificity) × (1 − PTP) × 1000 |
| Negative | FN = (1 − Sensitivity) × PTP × 1000 | TN = Specificity × (1 − PTP) × 1000 | |
| Author (Reference) | Year | Modality | FFR Threshold | No. of Studies | No. of Patients | Sensitivity (95% CI) | Specificity (95% CI) | PRISMA Score |
|---|---|---|---|---|---|---|---|---|
| Ullah [22] | 2020 | CMRI | 0.75−0.8 | 17 | 1886 | 0.86 (0.79−0.91) | 0.86 (0.82−0.90) | 15 |
| Pontone [23] | 2020 | CMRI | 0.75−0.8 | NA | 1085 | 0.87 (0.84−0.90) | 0.88 (0.85−0.90) | 18 |
| Yang [24] | 2019 | CMRI | 0.75−0.8 | 7 | 718 | 0.87 (0.73−0.94) | 0.87 (0.82−0.90) | - |
| Knuuti [25] | 2018 | CMRI | 0.8 | 5 | 588 | 0.89 (0.85−0.92) | 0.87 (0.83−0.91) | - |
| Kiaos [26] | 2018 | CMRI | 0.75−0.8 | 6 | 516 | 0.90 (0.85−0.93) | 0.85 (0.80−0.89) | - |
| Danad [27] | 2017 | CMRI | 0.75−0.8 | 2 | 70 | 0.90 (0.75−0.97) | 0.94 (0.79−0.99) | - |
| Jiang [6] | 2016 | CMRI | 0.75−0.8 | 12 | 1041 | 0.87 (0.83−0.90) | 0.87 (0.84−0.90) | - |
| Dai [7] | 2016 | CMRI | 0.75−0.8 | 15 | 1054 | 0.88 (0.85−0.91) | 0.84 (0.79−0.87) | 17 |
| Takx [28] | 2015 | CMRI | 0.75−0.8 | 10 | 798 | 0.89 (0.86−0.92) | 0.87 (0.83−0.90) | - |
| Pontone [23] | 2020 | SPECT | 0.75−0.8 | NA | 682 | 0.71 (0.66–0.76) | 0.79 (0.74–0.83) | - |
| Yang [24] | 2019 | SPECT | 0.75−0.8 | 8 | 842 | 0.72 (0.52−0.86) | 0.79 (0.71−0.85) | 17 |
| Knuuti [25] | 2018 | SPECT | 0.8 | 5 | 740 | 0.73 (0.62–0.82) | 0.83 (0.71–0.90) | 18 |
| Danad [27] | 2017 | SPECT | 0.75−0.8 | 3 | 110 | 0.70 (0.59–0.80) | 0.78 (0.68–0.87) | - |
| Dai [7] | 2016 | SPECT | 0.75−0.8 | 15 | 1142 | 0.78 (0.71–0.84) | 0.79 (0.70-.087) | 17 |
| Takx [28] | 2015 | SPECT | 0.75−0.8 | 8 | 553 | 0.74 (0.67–0.79) | 0.79 (0.74–0.83) | - |
| Knuuti [25] | 2018 | PET | 0.8 | 4 | 709 | 0.89 (0.82–0.93) | 0.85 (0.81–0.88) | 18 |
| Dai [7] | 2016 | PET | 0.8 | 4 | 609 | 0.90 (0.8–0.95) | 0.84 (0.81–0.90) | 17 |
| Takx [28] | 2015 | PET | 0.8 | 2 | 224 | 0.84(0.75–0.91) | 0.87 (0.80–0.92) | 17 |
| Pontone [23] | 2020 | SE | 0.75−0.8 | NA | 361 | 0.64 (0.56–0.71) | 0.84 (0.78–0.89) | 18 |
| Danad [27] | 2017 | SE | 0.75−0.8 | 2 | 115 | 0.77 (0.61–0.88) | 0.75 (0.63–0.85) | - |
| Dai [7] | 2016 | SE | 0.75−0.8 | 6 | 359 | 0.69 (0.57–0.80) | 0.77 (0.62–0.87) | 17 |
| Takx [28] | 2015 | SE | 0.75 | 4 | 177 | 0.69 (0.56–0.79) | 0.84 (0.75–0.90) | 17 |
| Pontone [23] | 2020 | FFRCT | 0.8 | NA | 664 | 0.90 (0.86–0.94) | 0.69 (0.64–0.74) | - |
| Zhuang [14] | 2020 | FFRCT | 0.8 | 7 | 1013 | 0.89 (0.85–0.92) | 0.71 (0.61–0.80) | 17 |
| Tang [29] | 2019 | FFRCT | 0.8 | 17 | 1418 | 0.90 (0.86–0.92) | 0.78 (0.68–0.86) | 14 |
| Hamon [30] | 2019 | FFRCT | 0.8 | 8 | 823 | 0.88 (0.84–0.91) | 0.72 (0.68–0.76) | - |
| Celeng [31] | 2019 | FFRCT | 0.8 | 10 | 1069 | 0.89 (0.85–0.92) | 0.76 (0.69–0.82) | 18 |
| Danad [27] | 2017 | FFRCT | 0.75 | 3 | 609 | 0.90 (0.85–0.93) | 0.71 (0.65–0.75) | - |
| Ding [9] | 2016 | FFRCT | 0.8 | 4 | 662 | 0.90 (0.86–0.93) | 0.73 (0.68–0.77) | - |
| Dai [7] | 2016 | FFRCT | 0.8 | 4 | 662 | 0.90 (0.85–0.93) | 0.75 (0.62–0.85) | - |
| Panchal [32] | 2016 | FFRCT | 0.8 | 4 | 662 | 0.90 (0.85–0.93) | 0.72 (0.67–0.76) | - |
| Wu [8] | 2016 | FFRCT | 0.8 | 5 | 833 | 0.89 (0.85–0.93) | 0.76 (0.64–0.84) | - |
| Gonzalez [33] | 2015 | FFRCT | 0.8 | 4 | 662 | 0.90 (0.85–0.93) | 0.72 (0.67–0.76) | - |
| Deng [34] | 2015 | FFRCT | NA | 4 | 662 | 0.90 (0.85–0.93) | 0.72 (0.67–0.76) | - |
| CMRI | SPECT | PET | SE | FFRCT | |
|---|---|---|---|---|---|
| Number of TP (n) | 261 | 219 | 267 | 192 | 267 |
| Number of FP (n) | 84 | 119 | 105 | 112 | 168 |
| Number of FN (n) | 39 | 81 | 33 | 108 | 33 |
| Number of TN (n) | 616 | 581 | 595 | 588 | 532 |
| Positive predictive value † (%) (95% CI) | 76 (71−80) | 65 (59−70) | 72 (67−76) | 63 (57−69) | 61 (57−66) |
| Negative predictive value (%) (95% CI) | 94 (92−96) | 88 (85−90) | 95 (93−96) | 84 (82−87) | 94 (92−96) |
| Post-test probability ‡ (%) (95% CI) | 6.0 (4.3−8.1) | 12.2 (9.8−15.0) | 5.3 (3.6−7.3) | 15.5 (12.9−18.4) | 5.8 (4.1−8.1) |
| Diagnostic accuracy (%) (95% CI) | 88 (86−90) | 80 (77−82) | 86 (84−88) | 78 (75−81) | 80 (77−82) |
| Number needed to diagnose (95% CI) | 1.33 (1.24−1.47) | 1.79 (1.57−2.10) | 1.35 (1.25−1.49) | 2.08 (1.78−2.54) | 1.54 (1.40−1.74) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwata, K.; Ogasawara, K. Assessment of the Efficiency of Non-Invasive Diagnostic Imaging Modalities for Detecting Myocardial Ischemia in Patients Suspected of Having Stable Angina. Healthcare 2023, 11, 23. https://doi.org/10.3390/healthcare11010023
Iwata K, Ogasawara K. Assessment of the Efficiency of Non-Invasive Diagnostic Imaging Modalities for Detecting Myocardial Ischemia in Patients Suspected of Having Stable Angina. Healthcare. 2023; 11(1):23. https://doi.org/10.3390/healthcare11010023
Chicago/Turabian StyleIwata, Kunihiro, and Katsuhiko Ogasawara. 2023. "Assessment of the Efficiency of Non-Invasive Diagnostic Imaging Modalities for Detecting Myocardial Ischemia in Patients Suspected of Having Stable Angina" Healthcare 11, no. 1: 23. https://doi.org/10.3390/healthcare11010023