
Comparison of the Psychological Impact of COVID-19 on Self-Employed Private Healthcare Workers with Respect to Employed Public Healthcare Workers: Three-Wave Study during the COVID-19 Pandemic in Spain
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
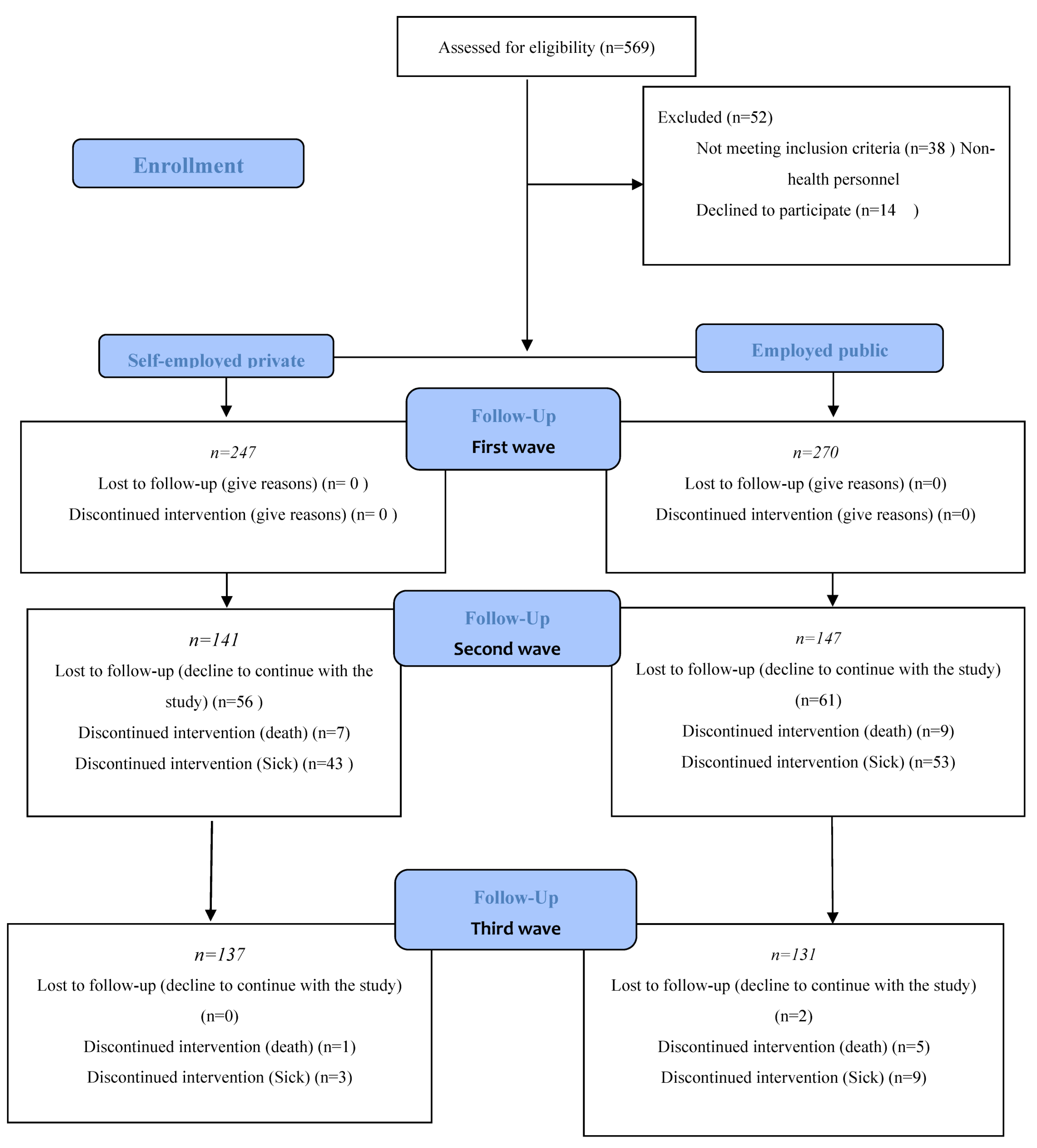
2.2. Sample
2.3. Procedure and Sampling Technique
2.4. Questionnaire
- Sociodemographic variables: age, sex.
- Academic education.
- Social security system for professional activity: self-employed or salaried employee.
- Relationship status: single, married, divorced, domestic partner, widow.
2.5. Statistical Analysis
3. Results
Characteristics of the Study Sample
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Parikhani, A.B.; Bazaz, M.; Bamehr, H.; Fereshteh, S.; Amiri, S.; Salehi-Vaziri, M.; Arashkia, A.; Azadmanesh, K. The Inclusive Review on SARS-CoV-2 Biology, Epidemiology, Diagnosis, and Potential Management Options. Curr. Microbiol. 2021, 78, 1099–1114. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Consumer Affairs and Social Welfare—Profesionales-Situación Actual Coronavirus. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/situacionActual.htm (accessed on 27 October 2021).
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Actualización no 324. Enfermedad por el coronavirus (CO-VID-19). Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/ (accessed on 15 August 2022).
- FDA Briefing Document, Pfizer-BioNTech COVID-19 Vaccine. Vaccines and Related Biological Products Advisory Committee Meeting. 10 December 2020. Available online: https://www.fda.gov/media/144245/download (accessed on 15 August 2022).
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. COVID-19: Pfizer BioNTech vaccine reduced cases by 94% in Israel, shows peer reviewed study. BMJ 2021, 372, n567. [Google Scholar] [CrossRef]
- EMA Recommends COVID-19 Vaccine Moderna for Authorisation in the EU. European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-moderna-authorisation-eu (accessed on 7 March 2021).
- EMA Recommends COVID-19 Vaccine AstraZeneca for Authorisation in the EU. European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-astrazeneca-authorisation-eu (accessed on 7 March 2021).
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef]
- Vilar-Palomo, S.; Pabón-Carrasco, M.; Gonzalez-Elena, M.; Ramírez-Baena, L.; Rodríguez-Gallego, I.; Castro-Méndez, A. Assessment of the Anxiety Level of Andalusian Podiatrists during the COVID-19 Pandemic: The Increase Phase. Healthcare 2020, 8, 432. [Google Scholar] [CrossRef]
- Pandey, A.; Sharma, C.; Chapagain, R.H.; Devkota, N.; Ranabhat, K.; Pant, S.; Adhikari, K. Stress, Anxiety, Depression and Their Associated Factors among Health Care Workers during COVID-19 Pandemic in Nepal. J. Nepal Health Res. Counc. 2021, 18, 655–660. [Google Scholar] [CrossRef]
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to Sars-Cov-2 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef]
- Evanoff, B.A.; Strickland, J.R.; Dale, A.M.; Hayibor, L.; Page, E.; Duncan, J.G.; Kannampallil, T.; Gray, D.L. Work-Related and Personal Factors Associated With Mental Well-Being During the COVID-19 Response: Survey of Health Care and Other Workers. J. Med. Internet Res. 2020, 22, e21366. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; de Los Santos, J.A.A. Fear of COVID-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 2021, 29, 395–403. [Google Scholar] [CrossRef] [PubMed]
- García-Iglesias, J.J.; Gómez-Salgado, J.; Martín-Pereira, J.; Fagundo-Rivera, J.; Ayuso-Murillom, D.; Martínez-Riera, J.R.; Ruiz-Frutos, C. Impacto del SARS-CoV-2 (COVID-19) en la salud mental de los profesionales sanitarios: Una revisión sistemá-tica [Impact of SARS-CoV-2 (COVID-19) on the mental health of healthcare professionals: A systematic review.]. Rev. Esp. Salud Publica 2020, 94, e202007088. (In Spanish) [Google Scholar] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Mensi, S.; Di Marco, A.; Siracusano, A.; Di Lorenzo, G. Mental Health Outcomes Among Healthcare Workers and the General Population During the COVID-19 in Italy. Front. Psychol. 2020, 11, 608986. [Google Scholar] [CrossRef] [PubMed]
- Rathod, S.; Pallikadavath, S.; Young, A.H.; Graves, L.; Rahman, M.M.; Brooks, A.; Soomro, M.; Rathod, P.; Phiri, P. Psychological impact of COVID-19 pandemic: Protocol and results of first three weeks from an international cross-section survey—Focus on health professionals. J. Affect. Disord. Rep. 2020, 1, 100005. [Google Scholar] [CrossRef]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public–A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef]
- Sischka, P.E.; Schmidt, A.F.; Steffgen, G. COVID-19 countermeasures at the workplace, psychological well-being, and mental health—A nationally representative latent class analysis of Luxembourgish employees. Curr. Psychol. 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual Huerta, J. Global pandemic, COVID-19 and podiatry. Rev. Esp. Pod. 2020, 31, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Official Gazette of the State. Royal Decree 463/2020 of 14 March, Declaring a State of Alarm for the Management of the Health Crisis Situation Caused by the COVID-19. 2020, 25390–25400. Available online: https://www.boe.es/eli/es/rd/2020/03/14/463 (accessed on 20 December 2022).
- Chatzittofis, A.; Karanikola, M.; Michailidou, K.; Constantinidou, A. Impact of the COVID-19 Pandemic on the Mental Health of Healthcare Workers. Int. J. Environ. Res. Public Health 2021, 18, 1435. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research In-volving Human Subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Brug, J.; Aro, A.R.; Oenema, A.; De Zwart, O.; Richardus, J.H.; Bishop, G.D. SARS Risk Perception, Knowledge, Precautions, and Information Sources, the Netherlands. Emerg. Infect. Dis. 2004, 10, 1486–1489. [Google Scholar] [CrossRef]
- Bults, M.; Beaujean, D.J.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A. Perceived Risk, Anxiety, and Behavioural Responses of the General Public during the Early Phase of the Influenza A (H1N1) Pandemic in the Nether-lands: Results of Three Consecutive Online Surveys. BMC Public Health 2011, 11, 2. [Google Scholar] [CrossRef] [Green Version]
- De Zwart, O.; Veldhuijzen, I.K.; Elam, G.; Aro, A.R.; Abraham, T.; Bishop, G.D.; Richardus, J.H.; Brug, J. Avian Influenza Risk Perception, Europe and Asia. Emerg. Infect. Dis. 2007, 13, 290–293. [Google Scholar] [CrossRef]
- Cano-Vindel, A.; Miguel-Tobal, J.J. Assessing Anxiety from an Interactive and Multidimensional Approach: The Anxiety Situations and Responses Inventory-ISRA. Psicol. Contemp. 1999, 6, 14–21. [Google Scholar]
- Cano-Vindel, A.; Muñoz-Navarro, R.; Morettic, L.S.; Medrano, L.A. Pyschometric properties of the Brief Inventory of Situations and Responses of Anxiety (ISRA-B). Anxiety Stress 2020, 26, 155–166. [Google Scholar]
- He, K.; Stolarski, A.; Whang, E.; Kristo, G. Addressing General Surgery Residents’ Concerns in the Early Phase of the COVID-19 Pandemic. J. Surg. Educ. 2020, 77, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Z.; Han, M.F.; Luo, T.D.; Ren, A.K.; Zhou, X.P. Mental health survey of 230 medical staff in a tertiary infectious disease hospital for COVID-19. Chin. J. Ind. Hyg. Occup. Dis. 2020, 38, E001. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Bohlken, J.; Sch€omig, F.; Lemke, M.R.; Pumberger, M.; Riedel-Heller, S.G. COVID-19 pandemic: Stress experience of healthcare workers. Psychiat Prax. 2020, 47, 190–197. [Google Scholar]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Gorini, A.; Fiabane, E.; Sommaruga, M.; Barbieri, S.; Sottotetti, F.; La Rovere, M.T.; Tremoli, E.; Gabanelli, P. Mental health and risk perception among Italian healthcare workers during the second month of the Covid-19 pandemic. Arch. Psychiatr. Nurs. 2020, 34, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Honkonen, T.; Ahola, K.; Pertovaara, M.; Isometsä, E.; Kalimo, R.; Nykyri, E.; Aromaa, A.; Lönnqvist, J. The association between burnout and physical illness in the general population—Results from the Finnish Health 2000 Study. J. Psychosom. Res. 2006, 61, 59–66. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and pref-erences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Chang, B.P. Can hospitalization be hazardous to your health? A nosocomial based stress model for hospitalization. Gen. Hosp. Psychiatry 2019, 60, 83–89. [Google Scholar] [CrossRef]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Category (n = 517) | Subcategories | % (n = 247) | % (n = 270) | p Value (ES) |
|---|---|---|---|---|
| Self-Employed Private | Employed Public | |||
| Gender $ | Men | 32.00 (n = 79) | 24.10 (n = 65) | 0.029 ** |
| Women | 68.00 (n = 168) | 75.90 (n = 205) | (0.460) & | |
| Professional category $ | Podiatrists | 44.54 (n = 110) | ||
| Physiotherapists | 55.46 (n = 137) | |||
| Doctors | 15.6 (n = 42) | |||
| Nurses | 61.1 (n = 165) | 0.001 *** | ||
| Auxiliary Nurses | 13.3 (n = 36) | (0.510) & | ||
| Other | 10.0 (n = 27) | |||
| Employment situation $ | Private Clinics | 100 (n = 247) | ||
| Hospital | 60.0 (n = 162) | |||
| Primary Care | 32.2 (n = 87) | 0.001 *** | ||
| Nursing Homes | 7.8 (n = 21) | (0.502) & | ||
| Marital status $ | Single | 27.9 (n = 69) | 27.0 (n = 73) | |
| Married/Domestic Partner | 65.2 (n = 161) | 66.7 (n = 180) | 0.941 | |
| Divorced/Widow | 6.9 (n = 17) | 6.3 (n = 17) | (0.214) & | |
| Children < 18 years old in the home $ | Yes | 46.5 (n = 115) | 40.4 (n = 109) | 0.001 *** |
| No | 53.5 (n = 132) | 59.6 (n = 161) | (0.415) & | |
| Risk of contracting the disease due to my age or presence of previous pathologies. $ | Very High | 5.6 (n = 14) | 0.9 (n = 2) | |
| High | 15.6 (n = 39) | 19.7 (n = 53) | ||
| Medium | 26.5 (n = 65) | 28.5 (n = 77) | 0.001 *** | |
| Low | 22.5 (n = 55) | 32.8 (n = 89) | (0.578) & | |
| Very Low | 29.8 (n = 74) | 18.0 (n = 49) | ||
| COVID-19 is harmful to my health $ | Very High | 39.6 (n = 98) | 10.1 (n = 27) | |
| High | 22.7 (n = 56) | 28.0 (n = 76) | ||
| Medium | 24.8 (n = 61) | 38.7 (n = 104) | 0.001 *** | |
| Low | 9.8 (n = 24) | 20.4 (n = 55) | (0.578) & | |
| Very Low | 3.2 (n = 8) | 2.8 (n = 8) | ||
| Very High | 18.5 (n = 46) | 1.1 (n = 3) | ||
| High | 26.0 (n = 64) | 36.3 (n = 98) | ||
| Perceived likelihood of becoming infected $ | Medium | 35.2 (n = 87) | 37.9 (n = 102) | 0.001 *** |
| Low | 16.9 (n = 42) | 22.8 (n = 62) | (0.503) & | |
| Very Low | 3.3 (n = 8) | 1.8 (n = 5) | ||
| Perceived severity $ | Very High | 9.4 (n = 23) | 11.2 (n = 30) | |
| High | 21.5 (n = 53) | 27.3 (n = 74) | ||
| Medium | 42.7 (n = 105) | 38.9 (n = 105) | 0.014 ** | |
| Low | 20.2 (n = 50) | 19.2 (n = 52) | (0.512) & | |
| Very Low | 6.3 (n = 16) | 3.5 (n = 9) | ||
| Very High | 24.6 (n = 61) | 0.0 (n = 0) | ||
| Severity of COVID-19 $ | High | 45.6 (n = 113) | 28.7 (n = 77) | |
| Medium | 25.6 (n = 63) | 33.3 (n = 90) | 0.001*** | |
| Low | 3.1 (n = 8) | 27.1 (n = 74) | (0.622) & | |
| Very Low | 1.0 (n = 2) | 10.9 (n = 29) | ||
| Media (SD) | Media (SD) | p value | ||
| Perceived anxiety (ASRI) total first wave £ | 19.2 (10.17) | 27.31 (11.89) | 0.001 *** (0.645) # | |
| Perceived anxiety (ASRI) total second wave £ | 16.79 (10.72) | 26.02 (10.88) | 0.001 *** (0.617) # | |
| Perceived anxiety (ASRI) total third wave £ | 18.45 (10.66) | 25.83 (11.13) | 0.001 *** (0.627) # | |
| Cognitive (ASRI) first wave £ | 8.84 (2.87) | 10.50 (3.38) | 0.001 *** (0.573) # | |
| Cognitive (ASRI) second wave £ | 8.15 (3.50) | 9.91 (3.35) | 0.001 *** (0.548) # | |
| Cognitive (ASRI) third wave £ | 8.23 (3.28) | 9.71 (2.96) | 0.001 *** (0.564) # | |
| Physiological (ASRI) first wave £ | 4.43 (4.45) | 8.96 (5.52) | 0.001 *** (0.594) # | |
| Physiological (ASRI) second wave £ | 3.70 (4.37) | 8.52 (5.03) | 0.001 *** (0.542) # | |
| Physiological (ASRI) third wave £ | 4.61 (4.67) | 8.55 (5.25) | 0.001 *** (0.532) # | |
| Motor (ASRI) first wave | 4.56 (3.12) | 5.36 (3.28) | 0.006 ** (0.518) # | |
| Motor (ASRI) second wave | 3.92 (2.94) | 5.22 (2.93) | 0.001 *** (0.567) # | |
| Motor (ASRI) third wave | 4.28 (2.84) | 5.16 (3.26) | 0.023 ** (0.509) # |
| First Wave | Self-Employed Private | Employed Public | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | |
| χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | |||
| Gender † | 3175 (0.001 ***) | 0.06 & | 3355.5 (0.003 ***) | 3344 (0.002 ***) | 3381.5 (0.003 ***) | 5265.5 (0.011 **) | 0.09 & | 5371 (0.018 **) | 4910 (0.001 ***) | 6121 (0.321) |
| Employment situation † | 3.678 (0.287) | 0.04 # | 0.627 (0.428) | 2.31 (0.128) | 4.30 (0.038 *) | 3.678 (0.298) | 0.04 # | 0.610 (0.894) | 8.43 (0.0.38 *) | 0.72 (0.868) |
| Severity of COVID-19 † | 20.30 (0.001 ***) | 0.23 $ | 31.3 (0.001 ***) | 18.6 (0.001 **) | 13.01 (0.011 **) | 8.56 (0.033 **) | 0.17& | 10.2 (0.017 **) | 8.12 (0.043 *) | 1.29 (0.729) |
| Risk of contracting the disease because of my age or presence of previous pathologies † | 21.31 (0.001 ***) | 0.14 & | 25.77 (0.001 ***) | 15.36 (0.001 ***) | 14.34 (0.001 ***) | 17.96 (0.001 ***) | 0.16 & | 22.55 (0.001 ***) | 11.00 (0.001 ***) | 17.98 (0.001 ***) |
| COVID-19 is harmful for my health † | 16.70 (0.002 ***) | 0.14 & | 17.81 (0.005 **) | 13.58 (0.009 **) | 15.56 (0.004 **) | 18.70 (0.001 ***) | 0.15 & | 21.21 (0.001 ***) | 16.58 (0.001 ***) | 15.06 (0.003 **) |
| Perceived susceptibility † | 56.19 (0.001 ***) | 0.31 $ | 53.96 (0.001 ***) | 44.69 (0.001 ***) | 37.40 (0.001 ***) | 58.19 (0.001 ***) | 0.32 $ | 51.96 (0.001 ***) | 47.69 (0.001 ***) | 39.40 (0.001 ***) |
| Perceived possibility of getting infected † | 35.77 (0.001 ***) | 0.23 $ | 29.61 (0.001 ***) | 28.02 (0.001 ***) | 26.81 (0.001 ***) | 37.77 (0.001 ***) | 0.23 $ | 32.11 (0.001 ***) | 29.82 (0.001 ***) | 28.01 (0.001 ***) |
| Second Wave | Self-Employed Private | Employed Public | ||||||||
| Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | |
| χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | |||
| Gender † | 1597 (0.017 *) | 0.07 & | 1610.5 (0.019*) | 1687 (0.041 *) | 1759.5 (0.093) | 1539(0.178) | 0.05 # | 1371(0.030) | 1607(0.307) | 1667(0.461) |
| Employment situation † | 0.184 (0.668) | 0.03 # | .420 (0.517) | 0.062 (0.803) | 0.066 (0.798) | 8.26 (0.041 *) | 0.07 & | 9.89 (0.019) | 6.59 (0.086) | 5.59(0.133) |
| Severity of COVID-19 † | 1.79 (0.617) | 0.07 & | 4.35 (0.226) | 1.59 (0.661) | 9.43 (0.815) | 1.67 (0.642) | 0.04 # | 1.81 (0.611) | 1.77 (0.620) | 3.21 (0.360) |
| Risk of contracting the disease because of my age or presence of previous pathologies † | 24.60 (0.001 ***) | 0.14 & | 29.50 (0.001 ***) | 19.86 (0.001 ***) | 15.80 (0.001 ***) | 1.35 (0.903) | 0.12 & | 0.365 (0.985) | 1.04 (0.903) | 3.29 (0.511) |
| COVID-19 is harmful for my health † | 18.15 (0.001 ***) | 0.13 & | 21.67 (0.001 ***) | 15.90 (0.001 ***) | 13.50 (0.011 **) | 18.02 (0.001 ***) | 0.11 & | 20.47 (0.001 ***) | 14.91 (0.004 **) | 13.57 (0.011 **) |
| Perceived susceptibility † | 34.83 (0.001 ***) | 0.27 $ | 42.17 (0.001 ***) | 28.23 (0.001 ***) | 16.53 (0.002 **) | 1.79 (0.774) | 0.04 # | 1.80 (0.772) | 1.65 (0.779) | 0.943 (0.918) |
| Perceived possibility of getting infected † | 19.80 (0.001 ***) | 0.20 $ | 14.94 (0.005 **) | 14.20 (0.007 **) | 15.39 (0.004 **) | 3.54 (0.471) | 0.03 # | 0.625 (0.960) | 5.16 (0.270) | 4.15 (0.386) |
| Third Wave | Self-Employed Private | Employed Public | ||||||||
| Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | Perceived Anxiety (ASRI) Total | ES | Cognitive (ASRI) | Physiological (ASRI) | Motor (ASRI) | |
| χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | χ2 o u (p) | |||
| Gender † | 1294.5 (0.001 ***) | 0.06 & | 1330.5 (0.001 ***) | 1271 (0.001 ***) | 1638.5 (0.059) | 1260(0.101) | 0.03 # | 1385 (0.330) | 1230 (0.071) | 1233 (0.073) |
| Employment situation † | 1.283 (0.257) | 0.05 # | 0.707 (0.400) | 0.504 (0.478) | 3.39 (0.066) | 0.477 (0.924) | 0.04 # | 2.00 (0.572) | 0.637 (0.888) | 0.201 (0.977) |
| Severity of COVID-19 † | 19.98 (0.001 ***) | 0.21 $ | 26.47 (0.001 ***) | 14.44 (0.006 **) | 13.60 (0.009 **) | 3.49 (0.479) | 0.14 & | 5.24(0.263) | 2.39 (0.664) | 4.88 (0.299) |
| Risk of contracting the disease because of my age or presence of previous pathologies † | 17.53 (0.001 ***) | 0.14 & | 20.92 (0.001 ***) | 9.43 (0.050 *) | 19.18 (0.001 ***) | 3.07 (0.546) | 0.12 & | 4.98 (0.288) | 3.78 (0.436) | 2.54 (0.637) |
| COVID-19 is harmful for my health † | 19.59 (0.001 ***) | 0.17 & | 28.67 (0.001 ***) | 13.73 (0.008 **) | 10.60 (0.031 **) | 19.04 (0.001 ***) | 0.16 & | 26.17 (0.001 ***) | 12.61 (0.008 **) | 9.62 (0.031 **) |
| Perceived susceptibility † | 47.01 (0.001 ***) | 0.30 $ | 59.52 (0.001 ***) | 35.91 (0.001 ***) | 22.71 (0.001 ***) | 3.52 (0.475) | 0.04 # | 2.64 (0.620) | 3.63 (0.458) | 4.62 (0.329) |
| Perceived possibility of getting infected † | 4.30 (0.366) | 0.05 # | 6.37 (0.173) | 3.02 (0.553) | 7.81 (0.099) | 1.36 (0.850) | 0.05 # | 0.731 (0.947) | 1.75 (0.781) | 2.65 (0.617) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pabón-Carrasco, M.; Vilar-Palomo, S.; Gonzalez-Elena, M.L.; Romero-Castillo, R.; Ponce-Blandon, J.A.; Castro-Méndez, A. Comparison of the Psychological Impact of COVID-19 on Self-Employed Private Healthcare Workers with Respect to Employed Public Healthcare Workers: Three-Wave Study during the COVID-19 Pandemic in Spain. Healthcare 2023, 11, 134. https://doi.org/10.3390/healthcare11010134
Pabón-Carrasco M, Vilar-Palomo S, Gonzalez-Elena ML, Romero-Castillo R, Ponce-Blandon JA, Castro-Méndez A. Comparison of the Psychological Impact of COVID-19 on Self-Employed Private Healthcare Workers with Respect to Employed Public Healthcare Workers: Three-Wave Study during the COVID-19 Pandemic in Spain. Healthcare. 2023; 11(1):134. https://doi.org/10.3390/healthcare11010134
Chicago/Turabian StylePabón-Carrasco, Manuel, Samuel Vilar-Palomo, María Luisa Gonzalez-Elena, Rocío Romero-Castillo, José Antonio Ponce-Blandon, and Aurora Castro-Méndez. 2023. "Comparison of the Psychological Impact of COVID-19 on Self-Employed Private Healthcare Workers with Respect to Employed Public Healthcare Workers: Three-Wave Study during the COVID-19 Pandemic in Spain" Healthcare 11, no. 1: 134. https://doi.org/10.3390/healthcare11010134