
Translation, Adaptation, and Validation of the Modified Thai Version of Champion’s Health Belief Model Scale (MT-CHBMS)

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Between the ages of 40 and 70 years (the recommended age for mammograms);
- No history of breast cancer or any other cancers;
- No pregnancy or breastfeeding.
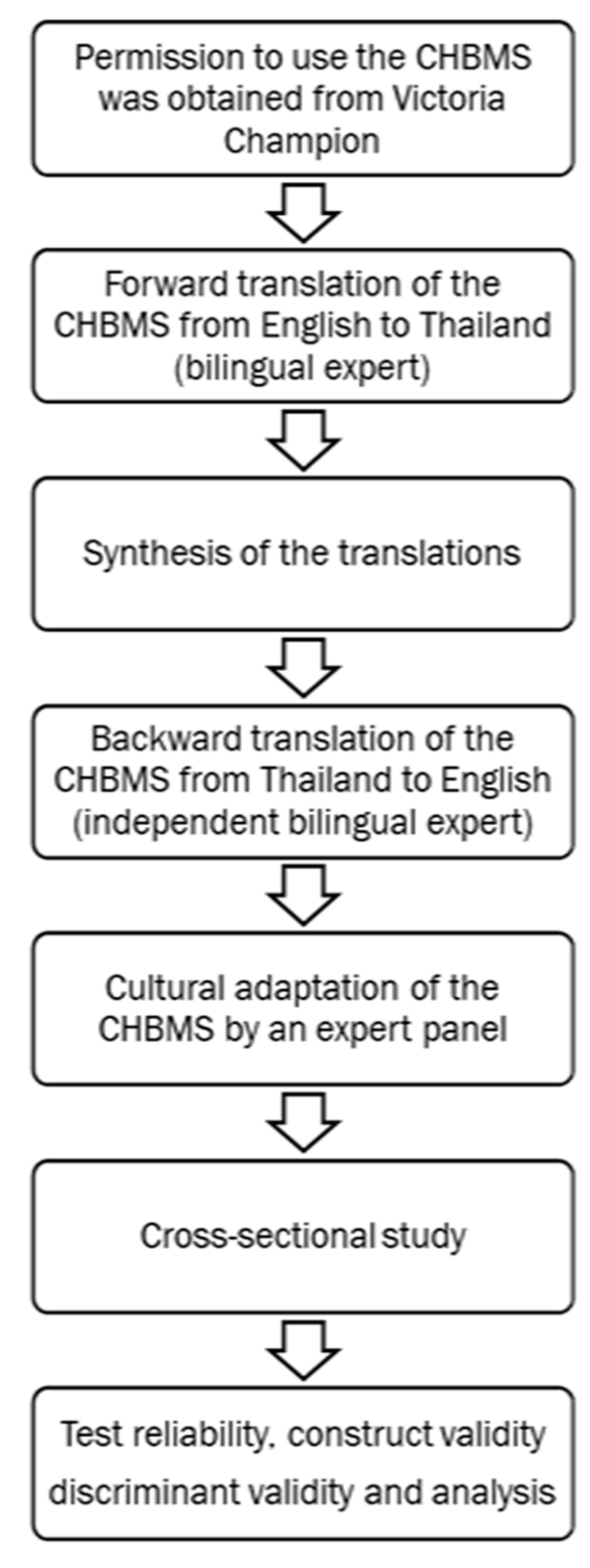
2.2. Development of the Modified Thai Version of CHBMS(MT-CHBMS)
2.2.1. Translation Process
Forward Translation
Synthesis of the Translations
Backward Translation
2.2.2. Modification
2.2.3. The Final MT-CHBMS

2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Respondents
3.2. Exploratory Factor Analysis (EFA)
3.3. Confirmatiory Factor Analysis (CFA)
4. Discussion
4.1. Clinical Implication and Future Research
4.2. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer Key Factors. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 21 December 2022).
- Strategy and Planning Division. Health Information, Public Health Statistics; Strategy and Planning Division: Nonthaburi, Thailand, 2018; Volume 10. [Google Scholar]
- Society, A.C. Cancer Facts and Figures. Available online: www.cancer.org (accessed on 2 September 2022).
- Unit, H.I. Public Health Statistics A.D.2018; Ministry of Public Health: Nonthaburi, Thailand, 2021. [Google Scholar]
- Fontham, E.; Wolf, A.M.D.; Church, T.R.; Etzioni, R.; Flowers, C.R.; Herzig, A.; Guerra, C.E.; Oeffinger, K.C.; Shih, Y.-C.T.; Walter, L.C.; et al. Guideline Update from the American Cancer Society. CA Cancer J. Clin. 2020, 70(5), 321–346. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Recommendations for Breast Cancer Screening in Thailand; National Cancer Institute: Nonthaburi, Thailand, 2012. [Google Scholar]
- Mukem, S.; Sriplung, H.; McNeil, E.; Tangcharoensathien, V. Breast cancer screening among women in Thailand: Analyses of population-based household surveys. J. Med. Assoc. Thai. 2014, 97, 1106–1118. [Google Scholar] [PubMed]
- National Cancer Institute. Hospital-Based Cancer Registry; Cancer Registry Unit, Medical Digital Division National Cancer Institute: Bangkok, Thailand, 2019. [Google Scholar]
- Champion, V.L. Revised Susceptibility, Benefits, and Barriers Scale for Mammography Screening. Res. Nurs. Health 1999, 22, 341–348. [Google Scholar] [CrossRef]
- Marmara, D.; Marmara, V.; Hubbard, G. Maltese Translation and Adaptation of Champion’s Health Belief Model Scale and the Revised Illness Perception Questionnaire for Breast Screening Among Maltese Women. J. Nurs. Meas. 2017, 25, 486–503. [Google Scholar] [CrossRef] [PubMed]
- Medina-Shepherd, R.; Kleier, J.A. Spanish Translation and Adaptation of Victoria Champion’s Health Belief Model Scales for Breast Cancer Screening Mammography. Cancer Nurs. 2010, 33, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Secginli, S.; Nahcivan, N.O. Reliability and Validity of the Breast Cancer Screening Belief Scale Among Turkish Women. Cancer Nurs. 2004, 27, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.-H.; Kim, J.-S.; Song, M.S. Translation and Validation of Champion’s Health Belief Model Scale with Korean Women. Cancer Nurs. 2002, 25, 391–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsa, P.; Kandiah, M.; Mohd, N.M.T.; Hejar, A.R.; Nor, A.M.Z. Reliability and validity of Champion’s Health Belief Model Scale for breast cancer screening among Malaysian women. Singap. Med. J. 2008, 49, 897. [Google Scholar]
- Noman, S.; Shahar, H.; Rahman, H.; Ismail, S.; Aljaberi, M.; Abdulrahman, M. Factor structure and internal reliability of breast cancer screening Champion’s Health Belief Model Scale in Yemeni women in Malaysia: A cross-sectional study. BMC Womens Health 2021, 21, 437. [Google Scholar] [CrossRef] [PubMed]
- Dewi, T.K. Validation of the Indonesian version of Champion’s Health Belief Model Scale for breast self-examination. Psychol. Res. Behav. Manag. 2018, 11, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chotsangsakorn, R.; Thanasilp, S.; Pudtong, N. Predicting Factors of Breast Cancer Screening Behaviors among Menopausal Women. Kuakarun J. Nurs. 2019, 26, 107–120. [Google Scholar]
- Koike, I.; Chompikul, J.; Thepthien, B.O.; Maikhan, N. Determinants of monthly breast self-examination among women in Samut Songkhram Province, Thailand. J. Public Health Dev. 2018, 16, 29–43. [Google Scholar]
- Shen, S.; Zhou, Y.; Xu, Y.; Zhang, B.; Duan, X.; Huang, R.; Li, B.; Shi, Y.; Shao, Z.; Liao, H.; et al. A multi-centre randomised trial comparing ultrasound vs mammography for screening breast cancer in high-risk Chinese women. Br. J. Cancer 2015, 112, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Htay, M.N.N.; Schliemann, D.; Dahlui, M.; Cardwell, C.R.; Loh, S.Y.; Tamin, N.S.B.I.; Somasundaram, S.; Champion, V.; Donnelly, M.; Su, T.T. Validation of the Champion Health Belief Model Scale for an Investigation of Breast Cancer Screening Behaviour in Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 9311. [Google Scholar] [CrossRef] [PubMed]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill Inc.: New York, NY, 1994. [Google Scholar]
- Hu, L.; Bentler, P.M. Evaluating model fit. In Structural Equation Modeling: Concepts, Issues and Applications; Hoyle, R.H., Ed.; Sage: Thousand Oaks, CA, USA, 1995; pp. 76–99. [Google Scholar]
- Hu, L.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to under parameterized model misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cut off criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equatation Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Arbuckle, J. Amos (Version 18.0), Computer Program; SPSS: Chicago, IL, USA, 2009.
- Tennant, A.; Conaghan, P.G. The Rasch measurement model in rheumatology: What is it and why use it? When should it be applied, and what should one look for in a Rasch paper? Arthritis Care Res. 2007, 57, 1358–1362. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | n (%) or Mean ± SD |
|---|---|
| Age (years), mean ± SD | 52.33 ± 7.28 |
| Marital status, n (%) | |
| Married | 17 (13.08) |
| Single | 80 (61.54) |
| Widow | 15 (11.54) |
| Divorced | 18 (13.85) |
| Education, n (%) | |
| - Unlettered | 3 (2.31) |
| - Middle school | 39 (30.00) |
| - High school/technical college | 39 (30.00) |
| - Baccalaureate degree | 37 (28.46) |
| - Master’s degree or higher | 12 (9.23) |
| Monthly income, n (%) | |
| THB < 10,000 | 63 (48.46) |
| THB 10,000–14,999 | 16 (12.31) |
| THB 15,000–19,999 | 1 (0.77) |
| THB 20,000–24,999 | 6 (4.62) |
| THB > 25,000 | 44 (33.85) |
| THB < 10,000 | |
| Health security, n (%) | |
| - Government or state enterprise officer | 54 (41.54) |
| - Social security scheme | 30 (23.08) |
| - Universal coverage scheme | 44 (33.85) |
| - Private health insurance | 0(0) |
| - Self-payment | 2 (1.54) |
| SD = standard deviation |
| Current Study (TM-CHBMS) | Champion’s Study (CHBMS) | |||
|---|---|---|---|---|
| Subscale | Alpha | Mean (SD) | Alpha | Mean (SD) |
| Susceptibility | 0.93 | 2.46 (0.98) | 0.93 | 2.54 (0.81) |
| Seriousness | 0.85 | 3.15 (0.81) | 0.80 | 3.25 (0.68) |
| Benefits—BSE | 0.88 | 4.05 (0.64) | 0.80 | 3.88 (0.52) |
| Barriers—BSE | 0.86 | 3.94 (0.65) | 0.88 | 2.02 (0.60) |
| Confidence | 0.90 | 4.10 (0.69) | 0.88 | 3.31 (0.57) |
| Health motivation | 0.85 | 3.81 (0.75) | 0.83 | 3.78 (0.59) |
| Benefits—mammogram | 0.93 | 25.36 (3.90) | 0.79 | 23.86 (3.17) |
| Barriers—mammogram | 0.74 | 19.05 (3.73) | 0.75 | 11.02 (3.26) |
| Benefits—ultrasound | 0.90 | 24.62 (4.12) | - | - |
| Barriers—ultrasound | 0.79 | 19.05 (3.76) | - | - |
| Items | Factor | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| barb3 | 0.805 | 0.173 | 0.114 | −0.116 | ||||||
| barb4 | 0.801 | 0.130 | −0.131 | |||||||
| barb1 | 0.722 | −0.115 | −0.106 | 0.303 | ||||||
| barb5 | 0.721 | −0.148 | ||||||||
| bau2 | 0.673 | 0.187 | 0.176 | 0.187 | 0.216 | |||||
| barb6 | 0.668 | 0.109 | 0.199 | −0.101 | 0.147 | |||||
| barm2 | 0.664 | 0.187 | 0.139 | |||||||
| barm3 | 0.620 | 0.240 | −0.120 | 0.314 | ||||||
| bau3 | 0.594 | 0.338 | 0.187 | 0.319 | ||||||
| bau4 | 0.534 | 0.234 | 0.194 | −0.142 | 0.315 | |||||
| barm1 | 0.532 | 0.200 | 0.110 | −0.297 | 0.178 | |||||
| barm4 | 0.448 | 0.177 | 0.119 | 0.108 | −0.101 | 0.241 | ||||
| barb2 | 0.359 | −0.143 | −0.126 | −0.168 | 0.245 | −0.284 | 0.290 | |||
| I5 | 0.123 | 0.776 | 0.134 | 0.126 | −0.108 | 0.211 | 0.118 | |||
| I6 | 0.775 | 0.211 | ||||||||
| I11 | 0.760 | 0.158 | 0.195 | −0.141 | ||||||
| I9 | 0.713 | 0.122 | −0.143 | −0.141 | 0.105 | −0.133 | ||||
| I4 | 0.686 | 0.200 | 0.138 | 0.384 | ||||||
| I10 | 0.685 | 0.153 | ||||||||
| I8 | 0.683 | −0.138 | −0.147 | |||||||
| I3 | 0.678 | −0.143 | 0.259 | 0.118 | 0.422 | |||||
| I7 | 0.638 | −0.117 | 0.168 | |||||||
| bm3 | 0.182 | 0.816 | 0.165 | 0.199 | 0.131 | 0.119 | ||||
| bm6 | 0.114 | 0.806 | 0.269 | 0.217 | 0.137 | |||||
| bm2 | 0.141 | 0.104 | 0.767 | 0.272 | 0.175 | 0.169 | 0.114 | |||
| bm4 | 0.168 | 0.165 | 0.740 | 0.229 | 0.255 | 0.221 | ||||
| bm1 | 0.250 | 0.661 | 0.318 | 0.175 | 0.107 | 0.138 | ||||
| bm5 | 0.152 | 0.110 | 0.565 | 0.473 | 0.186 | 0.174 | ||||
| beu1 | 0.134 | 0.288 | 0.822 | 0.247 | 0.181 | |||||
| beu3 | 0.129 | 0.314 | 0.796 | 0.175 | ||||||
| beu2 | −0.105 | 0.177 | 0.788 | 0.148 | 0.219 | 0.117 | ||||
| beu4 | 0.157 | 0.172 | 0.759 | 0.230 | −0.118 | 0.114 | ||||
| beu5 | 0.155 | 0.626 | 0.169 | 0.316 | 0.186 | −0.247 | ||||
| beu6 | 0.113 | 0.382 | 0.477 | 0.206 | ||||||
| M4 | 0.152 | 0.258 | 0.225 | 0.845 | ||||||
| M3 | 0.215 | 0.181 | 0.799 | 0.143 | ||||||
| M2 | 0.166 | 0.108 | 0.270 | 0.736 | ||||||
| M5 | 0.152 | 0.116 | 0.709 | −0.150 | ||||||
| M1 | 0.300 | 0.209 | 0.285 | 0.646 | 0.106 | 0.104 | ||||
| M7 | 0.135 | 0.125 | 0.574 | −0.175 | ||||||
| M6 | 0.158 | 0.386 | 0.254 | −0.120 | ||||||
| S5 | 0.890 | |||||||||
| S4 | 0.870 | 0.213 | −0.118 | |||||||
| S2 | 0.848 | 0.174 | ||||||||
| S3 | −0.116 | 0.819 | 0.151 | −0.151 | ||||||
| S1 | 0.812 | 0.136 | 0.130 | |||||||
| be4 | 0.137 | 0.133 | 0.163 | 0.158 | 0.809 | |||||
| be6 | 0.173 | 0.165 | 0.101 | 0.187 | 0.141 | 0.784 | 0.110 | |||
| be5 | 0.156 | 0.158 | 0.234 | 0.166 | 0.760 | 0.101 | ||||
| be3 | 0.152 | 0.184 | 0.138 | 0.103 | 0.731 | 0.214 | ||||
| beb2 | −0.130 | 0.683 | 0.113 | 0.275 | 0.388 | |||||
| se3 | −0.157 | 0.104 | 0.820 | |||||||
| se2 | 0.110 | 0.102 | 0.104 | 0.733 | ||||||
| se1 | 0.226 | 0.705 | ||||||||
| se4 | −0.213 | 0.165 | 0.112 | 0.688 | ||||||
| se6 | 0.654 | |||||||||
| se7 | −0.180 | 0.161 | 0.517 | −0.102 | ||||||
| se5 | −0.102 | 0.314 | 0.455 | 0.146 | ||||||
| barm5 | 0.248 | 0.103 | 0.558 | |||||||
| bau5 | 0.203 | 0.241 | −0.145 | 0.531 | 0.137 | |||||
| bau1 | 0.487 | −0.113 | 0.117 | −0.151 | 0.490 | −0.102 | ||||
| I2 | 0.530 | 0.111 | 0.531 | |||||||
| I1 | 0.109 | 0.417 | 0.110 | 0.113 | 0.491 | |||||
| beb1 | 0.128 | 0.380 | 0.141 | 0.462 | ||||||
| T-CHBMS | MT-CHBMS | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Estimate | S.E. | Est./S.E. | p-Value | Estimate | S.E. | Est./S.E. | p-Value | ||
| SUS | BY | BY | |||||||
| S1 | 0.832 | 0.032 | 26.29 | <0.001 | 0.832 | 0.032 | 26.094 | <0.001 | |
| S2 | 0.873 | 0.021 | 40.605 | <0.001 | 0.873 | 0.022 | 40.593 | <0.001 | |
| S3 | 0.834 | 0.028 | 29.435 | <0.001 | 0.833 | 0.028 | 29.273 | <0.001 | |
| S4 | 0.903 | 0.022 | 41.627 | <0.001 | 0.902 | 0.022 | 41.585 | <0.001 | |
| S5 | 0.945 | 0.014 | 65.548 | <0.001 | 0.946 | 0.014 | 66.01 | <0.001 | |
| SERIOUSNESS | BY | BY | |||||||
| SE1 | 0.726 | 0.043 | 16.873 | <0.001 | 0.715 | 0.044 | 16.189 | <0.001 | |
| SE2 | 0.752 | 0.051 | 14.614 | <0.001 | 0.764 | 0.05 | 15.302 | <0.001 | |
| SE3 | 0.818 | 0.038 | 21.287 | <0.001 | 0.819 | 0.039 | 21.087 | <0.001 | |
| SE4 | 0.806 | 0.035 | 23.32 | <0.001 | 0.812 | 0.034 | 23.584 | <0.001 | |
| SE5 | 0.532 | 0.06 | 8.83 | <0.001 | 0.518 | 0.062 | 8.32 | <0.001 | |
| SE6 | 0.647 | 0.057 | 11.277 | <0.001 | 0.644 | 0.057 | 11.354 | <0.001 | |
| SE7 | 0.594 | 0.060 | 9.858 | <0.001 | 0.601 | 0.06 | 10.075 | <0.001 | |
| BENEFIT of BSE | BY | BY | |||||||
| BEB1 | 0.589 | 0.045 | 13.243 | <0.001 | 0.566 | 0.049 | 11.664 | <0.001 | |
| BEB2 | 0.629 | 0.051 | 12.393 | <0.001 | 0.604 | 0.056 | 10.766 | <0.001 | |
| BE3 | 0.830 | 0.031 | 26.849 | <0.001 | 0.832 | 0.034 | 24.751 | <0.001 | |
| BE4 | 0.915 | 0.021 | 44.273 | <0.001 | 0.909 | 0.024 | 38.44 | <0.001 | |
| BE5 | 0.944 | 0.020 | 46.91 | <0.001 | 0.961 | 0.022 | 43.35 | <0.001 | |
| BE6 | 0.958 | 0.025 | 37.853 | <0.001 | 0.958 | 0.027 | 36.102 | <0.001 | |
| BENEFIT of MG | BY | BY | |||||||
| BM1 | 0.882 | 0.026 | 33.807 | <0.001 | 0.899 | 0.024 | 37.499 | <0.001 | |
| BM2 | 0.889 | 0.021 | 42.185 | <0.001 | 0.893 | 0.022 | 41.473 | <0.001 | |
| BM3 | 0.991 | 0.016 | 60.245 | <0.001 | 0.977 | 0.017 | 56.99 | <0.001 | |
| BM4 | 0.926 | 0.016 | 59.059 | <0.001 | 0.925 | 0.016 | 58.723 | <0.001 | |
| BM5 | 0.858 | 0.03 | 28.358 | <0.001 | 0.906 | 0.024 | 37.257 | <0.001 | |
| BM6 | 0.953 | 0.014 | 67.414 | <0.001 | 0.953 | 0.014 | 68.123 | <0.001 | |
| BARRIER to BSE | BY | BY | |||||||
| BARB1 | 0.778 | 0.049 | 15.76 | <0.001 | 0.772 | 0.05 | 15.55 | <0.001 | |
| BARB2 | 0.455 | 0.067 | 6.847 | <0.001 | 0.472 | 0.067 | 7.034 | <0.001 | |
| BARB3 | 0.862 | 0.04 | 21.36 | <0.001 | 0.858 | 0.04 | 21.227 | <0.001 | |
| BARB4 | 0.910 | 0.034 | 26.871 | <0.001 | 0.929 | 0.034 | 27.227 | <0.001 | |
| BARB5 | 0.753 | 0.041 | 18.566 | <0.001 | 0.740 | 0.043 | 17.262 | <0.001 | |
| BARB6 | 0.836 | 0.041 | 20.621 | <0.001 | 0.836 | 0.042 | 19.972 | <0.001 | |
| BARRIER to MG | BY | BY | |||||||
| BARM1 | 0.644 | 0.053 | 12.074 | <0.001 | 0.653 | 0.052 | 12.506 | <0.001 | |
| BARM2 | 0.891 | 0.04 | 22.452 | <0.001 | 0.875 | 0.036 | 24.048 | <0.001 | |
| BARM3 | 0.776 | 0.042 | 18.306 | <0.001 | 0.756 | 0.04 | 19.05 | <0.001 | |
| BARM4 | 0.606 | 0.061 | 9.993 | <0.001 | 0.625 | 0.052 | 12.042 | <0.001 | |
| BARM5 | 0.474 | 0.062 | 7.599 | <0.001 | 0.515 | 0.056 | 9.192 | <0.001 | |
| CONFIDENCE | BY | BY | |||||||
| I1 | 0.679 | 0.056 | 12.154 | <0.001 | 0.695 | 0.06 | 11.529 | <0.001 | |
| I2 | 0.756 | 0.040 | 19.062 | <0.001 | 0.752 | 0.042 | 18.022 | <0.001 | |
| I3 | 0.905 | 0.030 | 29.666 | <0.001 | 0.923 | 0.034 | 27.04 | <0.001 | |
| I4 | 0.933 | 0.031 | 29.649 | <0.001 | 0.953 | 0.035 | 26.976 | <0.001 | |
| I5 | 0.739 | 0.045 | 16.376 | <0.001 | 0.740 | 0.047 | 15.612 | <0.001 | |
| I6 | 0.688 | 0.045 | 15.206 | <0.001 | 0.681 | 0.047 | 14.359 | <0.001 | |
| I7 | 0.489 | 0.058 | 8.474 | <0.001 | 0.458 | 0.061 | 7.536 | <0.001 | |
| I8 | 0.652 | 0.051 | 12.809 | <0.001 | 0.641 | 0.054 | 11.879 | <0.001 | |
| I9 | 0.670 | 0.047 | 14.255 | <0.001 | 0.644 | 0.050 | 12.874 | <0.001 | |
| I10 | 0.788 | 0.035 | 22.55 | <0.001 | 0.783 | 0.037 | 20.892 | <0.001 | |
| I11 | 0.776 | 0.042 | 18.354 | <0.001 | 0.767 | 0.045 | 17.022 | <0.001 | |
| MOTIVATION | BY | BY | |||||||
| M1 | 0.88 | 0.034 | 25.653 | <0.001 | 0.910 | 0.035 | 25.709 | <0.001 | |
| M2 | 0.938 | 0.019 | 48.845 | <0.001 | 0.941 | 0.02 | 46.929 | <0.001 | |
| M3 | 0.933 | 0.017 | 56.135 | <0.001 | 0.925 | 0.019 | 49.13 | <0.001 | |
| M4 | 1.028 | 0.016 | 64.794 | <0.001 | 1.029 | 0.016 | 63.697 | <0.001 | |
| M5 | 0.779 | 0.041 | 19.054 | <0.001 | 0.768 | 0.045 | 17.21 | <0.001 | |
| M6 | 0.459 | 0.063 | 7.334 | <0.001 | 0.413 | 0.067 | 6.138 | <0.001 | |
| M7 | 0.719 | 0.044 | 16.288 | <0.001 | 0.716 | 0.047 | 15.286 | <0.001 | |
| BENEFIT OF U | BY | ||||||||
| BEU1 | 0.946 | 0.02 | 47.853 | <0.001 | |||||
| BEU2 | 0.863 | 0.028 | 30.303 | <0.001 | |||||
| BEU3 | 0.931 | 0.021 | 43.747 | <0.001 | |||||
| BEU4 | 0.922 | 0.023 | 39.612 | <0.001 | |||||
| BEU5 | 0.827 | 0.037 | 22.238 | <0.001 | |||||
| BEU6 | 0.809 | 0.036 | 22.385 | <0.001 | |||||
| BARRIER of U | BY | ||||||||
| BAU1 | 0.622 | 0.047 | 13.269 | <0.001 | |||||
| BAU2 | 0.906 | 0.035 | 25.649 | <0.001 | |||||
| BAU3 | 0.880 | 0.027 | 32.853 | <0.001 | |||||
| BAU4 | 0.813 | 0.032 | 25.174 | <0.001 | |||||
| BAU5 | 0.494 | 0.064 | 7.741 | <0.001 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suriyong, P.; Jiraniramai, S.; Wongpakaran, N.; Pinyopornpanish, K.; Angkurawaranon, C.; Jiraporncharoen, W.; Champion, V.L.; Wongpakaran, T. Translation, Adaptation, and Validation of the Modified Thai Version of Champion’s Health Belief Model Scale (MT-CHBMS). Healthcare 2023, 11, 128. https://doi.org/10.3390/healthcare11010128
Suriyong P, Jiraniramai S, Wongpakaran N, Pinyopornpanish K, Angkurawaranon C, Jiraporncharoen W, Champion VL, Wongpakaran T. Translation, Adaptation, and Validation of the Modified Thai Version of Champion’s Health Belief Model Scale (MT-CHBMS). Healthcare. 2023; 11(1):128. https://doi.org/10.3390/healthcare11010128
Chicago/Turabian StyleSuriyong, Patinya, Surin Jiraniramai, Nahathai Wongpakaran, Kanokporn Pinyopornpanish, Chaisiri Angkurawaranon, Wichuda Jiraporncharoen, Victoria L. Champion, and Tinakon Wongpakaran. 2023. "Translation, Adaptation, and Validation of the Modified Thai Version of Champion’s Health Belief Model Scale (MT-CHBMS)" Healthcare 11, no. 1: 128. https://doi.org/10.3390/healthcare11010128