

The Patient Flow Effect of Pandemic Policies: A Hybrid Simulation Study in a Norwegian Emergency Department



Abstract
:1. Introduction
- How does the introduction of COVID-19-contaminated patients affect the patient flow in an emergency department?
- What effect does adding a waiting zone and extra treatment rooms have on patient flow in an emergency department?
2. Materials and Methods
2.1. Case and Data Description
2.2. Simulation Modeling Methodology
2.2.1. The Introduced Interventions in This Case
- Pre-triageThe pre-triage is an intervention in the form of a physical building in front of the ED entrance. In broad lines, patients must undergo screening by answering questions concerning the risk of contamination and taking a rapid antigen test.
- Fast-trackingThey are expediting contaminated patients to treatment rooms. Patients that are found to have the risk of being contaminated are expedited directly to their designated treatment room. Other patients have to go by the normal procedure, wait in the waiting room and perhaps go through the triage; patients with the risk of being contaminated will be sent directly to their treatment room.
- Extra treatment rooms:To balance out the demand implications that the interventions put on the ED, they chose to increase the capacity of the ED by four rooms, each with its own bed. The balancing of capacity was performed by increasing the number of treatment rooms, which was 13 before the pandemic. The emergency department manager opens up four extra treatment rooms when needed.
- Waiting zoneAnother balancing intervention is the introduction of a waiting zone. The waiting zone is an area dedicated to non-contaminated patients who have received treatment and whose condition has stabilized. The need for treatment is reduced; thus, they can be placed in a new location. The policies of using the waiting zone for a patient are first that there are no more treatment rooms left over for a newly admitted patient and that the patient has received at least 2 h of care in their initial treatment room.
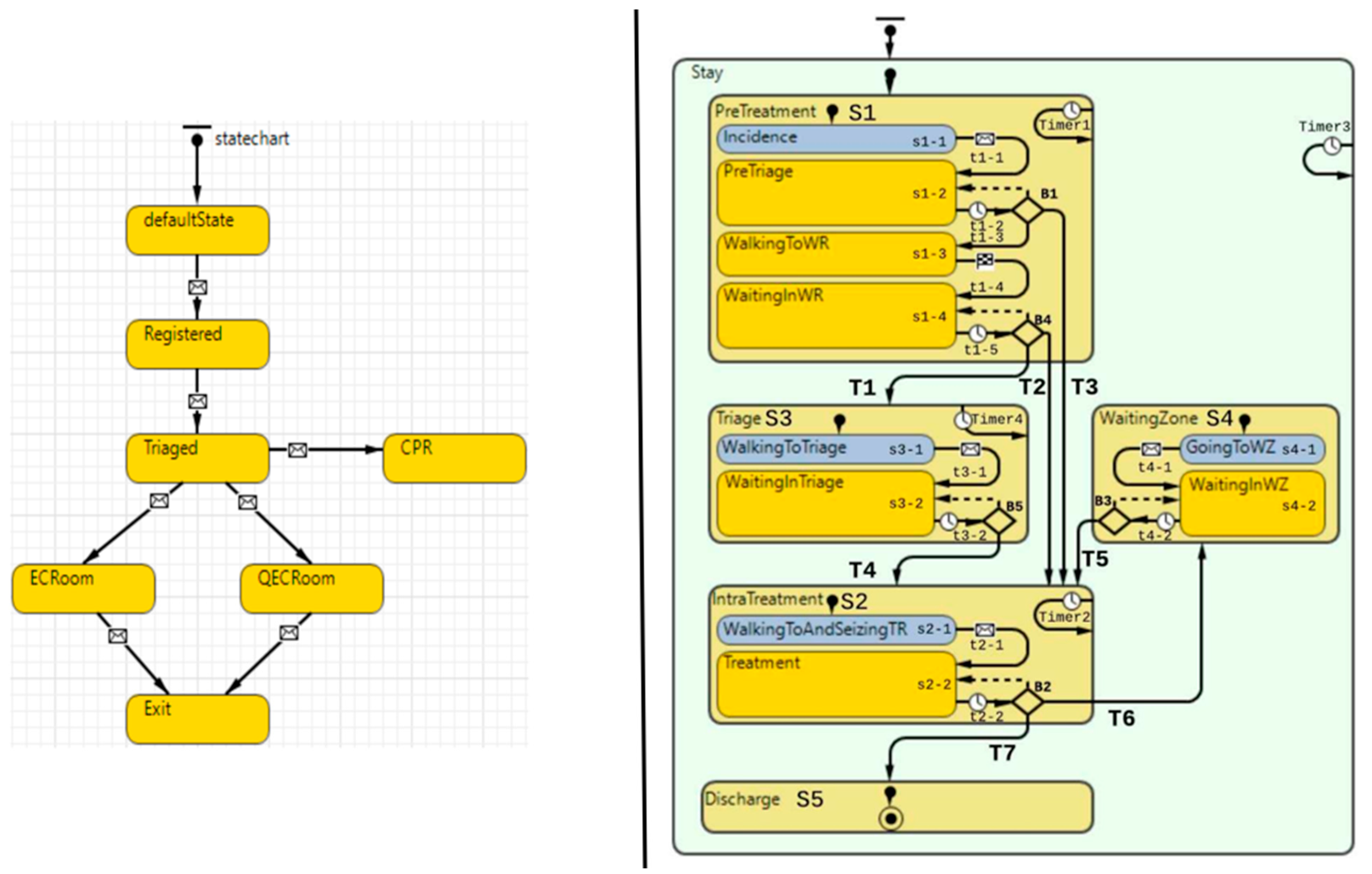
2.3. Simulation Model
2.4. Scenario Design
2.4.1. Patient Flow Indicators
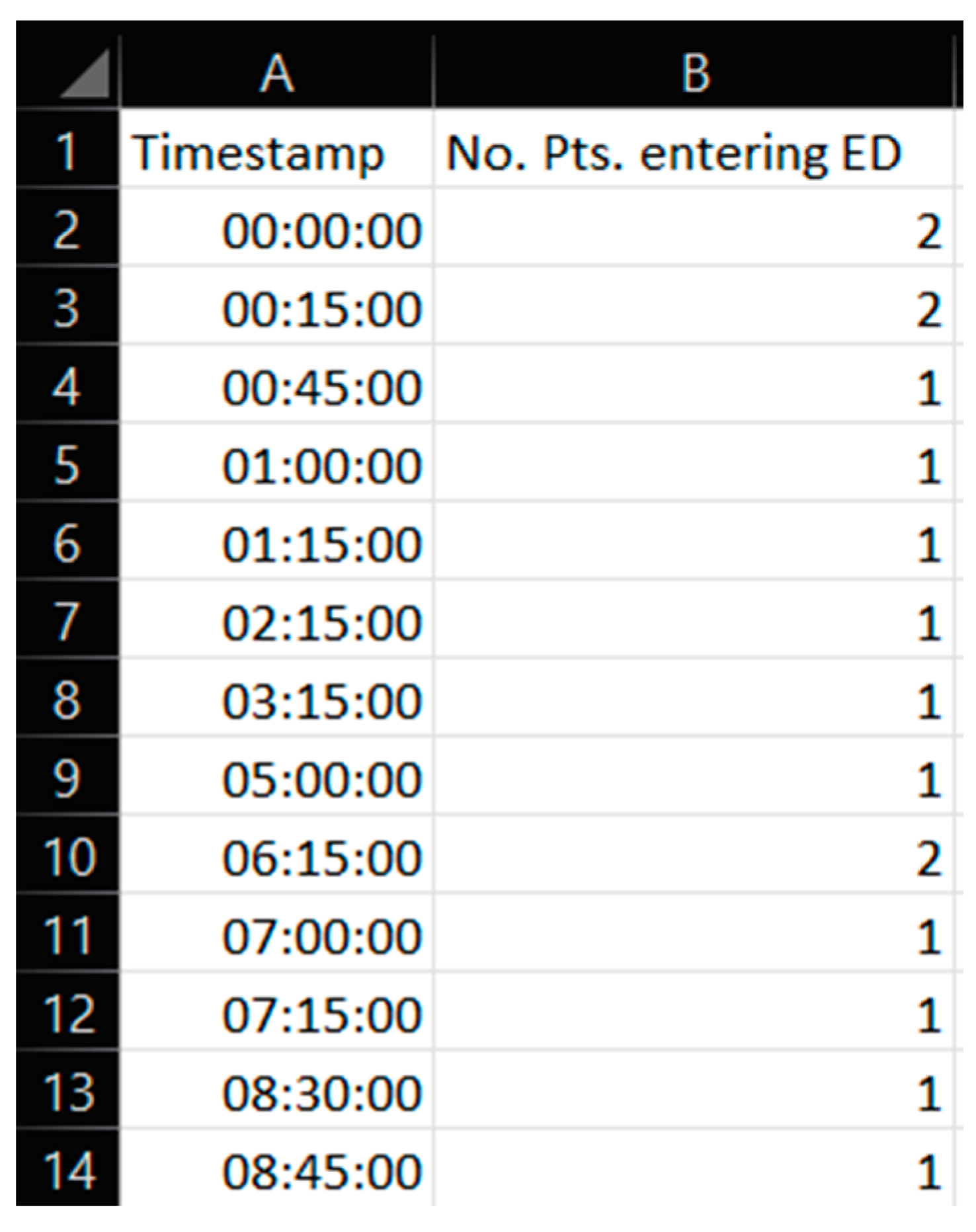
2.4.2. The Data
3. Results and Discussions
3.1. Presentation and Discussion of Simulation Results for Sc.1–Sc.5
3.1.1. Scenario 1: The Base Case Scenario
3.1.2. Scenario 2: Pandemic: Introducing the Virus-Suspicious Patients, but No Interventions
3.1.3. Scenario 3: Pandemic and Introducing Extra Treatment Rooms
3.1.4. Scenario 4: Pandemic and Introducing the Waiting Zone as the Only Intervention
3.1.5. Scenario 5: Pandemic and Using Extra Treatment Rooms and the Waiting Zone
3.1.6. Effect on Time to Treatment (TtT)
- When no interventions are introduced, and patients are routed through the ED according to contamination status, TtT for ordinary patients is much higher for ordinary than for contaminated patients.
- Introducing an extra treatment room (ET) causes a drop in TtT for both ordinary (Ord) and contaminated (Con) patients
- However, introducing the waiting zone (WZ), in addition to the extra treatment room, causes a further drop in TtT for contaminated (Con) patients but an increase in TtT for ordinary (Ord) patients.
3.1.7. Summary of the Simulation Outputs
3.2. General Discussion
3.2.1. Research Contribution
3.2.2. Further Work
- Cleaning and disinfection time: When looking at the numerical output portrayed in Table 4, we can see the indicator of how many times a room was seized. Under pandemic conditions, a treatment room must be sanitized between each patient visit. This will not only need resources, but it will also take time. Different scenarios gave different seizing times, particularly Sc.4 and Sc.5, which included the waiting zone to be utilized. Implementing time for sanitization could reveal a further “cost” of including a waiting zone in the ED.
- Optimization of the number of extra treatment rooms: The results that are shown in Section 3.1. show favorable patient flow outcomes when including the extra treatment rooms. In order to make the model reflect the actual patient flow interventions that the case ED implemented, scenarios Sc.3 and Sc.5 included four treatment rooms. Since treatment rooms showed such an overall improvement in patient flow, it would be fruitful to investigate the optimal number of extra treatment rooms to add.
- Classification error: Similar to any classification system, pre-triage prescreening may be vulnerable to false positives and false negatives. Here, the risk associated with false negatives might have a devastating impact on a department filled with compromised patients. Such a case could imply contagious patients admitted to the waiting room.
- Studying the effect of the increased patient contamination rate on the patient flow: Given the results disclosed in this present article, an immediately succeeding logical step could be to investigate differential outcomes with an incremental increase of the patient contamination rate. Such a granular approach could evaluate and inform the intervention efficacy under different patient contamination rates and investigate and inform at which levels the non-contaminated patients have to suffer too great of a burden.
- Intra-hospital contamination: As shown in the literature on the current pandemic, we know that the pathogen is highly transmissible. There could be a risk of intradepartmental virus transmission if a patient is near another patient. Additionally, the screening may not be accurate, and patients might be contaminated. This is quite easy to implement in an agent-based model such as the one used in the present paper. Such an endeavor was pursued in the research of [33]. However, it is not clear if an actual patient flow moving across the physical layout was taken into consideration
4. Conclusions
- The suspected COVID-19 patient requires prioritization over the ordinary patient to the level that ordinary patients must leave the treatment room for suspected COVID-19 patients;
- It increases the occupancy rate for treatment rooms and leads to more frequent seizing and releasing operations for treatment rooms due to the prioritization and random arrival rate of suspected COVID-19 patients;
- It increases the need for additional services for treatment rooms and waiting zones;
- It increases the lead time, treatment time, and waiting time for the patients not found to be contaminated.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 1 | Day 2 † | |
|---|---|---|
| (Sc. 1) |  |  |
| (Sc. 2) |  |  |
| (Sc. 3) |  |  |
| (Sc. 4) |  |  |
| (Sc. 5) |  |  |
 | ||
References
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.-C.; Wang, C.-B.; Bernardini, S. The COVID-19 Pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Martellucci, C.A.; Flacco, M.E.; Cappadona, R.; Bravi, F.; Mantovani, L.; Manzoli, L. SARS-CoV-2 Pandemic: An Overview. Adv. Biol. Regul. 2020, 77, 100736. [Google Scholar] [CrossRef] [PubMed]
- Helse Stavanger, S. Koronavirus—Rutiner for Medarbeidere. Available online: https://helse-stavanger.no/om-oss/for-ansatte/koronavirus-rutiner-for-ansatte (accessed on 7 October 2022).
- Gro, F. Håndteringen av COVID-19-Pandemien. 31. Available online: https://www.regjeringen.no/contentassets/dee8c25ba49f4e21add931746e04f7fb/regjeringens-strategi-og-beredskapsplan.pdf (accessed on 10 June 2022).
- Capalbo, C.; Aceti, A.; Simmaco, M.; Bonfini, R.; Rocco, M.; Ricci, A.; Napoli, C.; Rocco, M.; Alfonsi, V.; Teggi, A.; et al. The Exponential Phase of the COVID-19 Pandemic in Central Italy: An Integrated Care Pathway. Int. J. Environ. Res. Public Health 2020, 17, 3792. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, P.A.; Provost, L.P.; Kotagal, U.R.; Luther, K.; Anderson, A. Institute for Healthcare Improvement: Achieving Hospital-Wide Patient Flow; Institute for Healthcare Improvement: Cambridge, MA, USA, 2017. [Google Scholar]
- McHugh, M.; VanDyke, K.; McClelland, M.; Moss, D. Improving Patient Flow and Reducing Emergency Department Crowding: A Guide for Hospitals. 48. Available online: https://www.ahrq.gov/research/findings/final-reports/ptflow/index.html (accessed on 11 August 2022).
- Mohiuddin, S.; Busby, J.; Savović, J.; Richards, A.; Northstone, K.; Hollingworth, W.; Donovan, J.L.; Vasilakis, C. Patient Flow within UK Emergency Departments: A Systematic Review of the Use of Computer Simulation Modelling Methods. BMJ Open 2017, 7, e015007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanbrabant, L.; Braekers, K.; Ramaekers, K.; Van Nieuwenhuyse, I. Simulation of Emergency Department Operations: A Comprehensive Review of KPIs and Operational Improvements. Comput. Ind. Eng. 2019, 131, 356–381. [Google Scholar] [CrossRef]
- Bansal, K.; Kumar, S. Mutational Cascade of SARS-CoV-2 Leading to Evolution and Emergence of Omicron Variant. Virus Res. 2022, 315, 198765. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, P.; Ray, P.K. Patient Flow Modelling and Performance Analysis of Healthcare Delivery Processes in Hospitals: A Review and Reflections. Comput. Ind. Eng. 2014, 78, 299–312. [Google Scholar] [CrossRef]
- Aljahany, M.; Alassaf, W.; Alibrahim, A.A.; Kentab, O.; Alotaibi, A.; Alresseeni, A.; Algarni, A.; Algaeed, H.A.; Aljaber, M.I.; Alruwaili, B.; et al. Use of In Situ Simulation to Improve Emergency Department Readiness for the COVID-19 Pandemic. Prehosp. Disaster Med. 2021, 36, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Salmon, A.; Rachuba, S.; Briscoe, S.; Pitt, M. A Structured Literature Review of Simulation Modelling Applied to Emergency Departments: Current Patterns and Emerging Trends. Oper. Res. Health Care 2018, 19, 1–13. [Google Scholar] [CrossRef]
- Castanheira-Pinto, A.; Gonçalves, B.S.; Lima, R.M.; Dinis-Carvalho, J. Modeling, Assessment and Design of an Emergency Department of a Public Hospital through Discrete-Event Simulation. Appl. Sci. 2021, 11, 805. [Google Scholar] [CrossRef]
- Hamza, N.; Majid, M.A.; Hujainah, F. SIM-PFED: A Simulation-Based Decision Making Model of Patient Flow for Improving Patient Throughput Time in Emergency Department. IEEE Access 2021, 9, 103419–103439. [Google Scholar] [CrossRef]
- Tavakoli, M.; Tavakkoli-Moghaddam, R.; Mesbahi, R.; Ghanavati-Nejad, M.; Tajally, A. Simulation of the COVID-19 Patient Flow and Investigation of the Future Patient Arrival Using a Time-Series Prediction Model: A Real-Case Study. Med. Biol. Eng. Comput. 2022, 60, 969–990. [Google Scholar] [CrossRef]
- Al-Shareef, A.S.; Al Jabarti, A.; Babkair, K.A.; Jamajom, M.; Bakhsh, A.; Aga, S.S. Strategies to Improve Patient Flow in the Emergency Department during the COVID-19 Pandemic: A Narrative Review of Our Experience. Emerg. Med. Int. 2022, 2022, 2715647. [Google Scholar] [CrossRef]
- Bovim, T.R.; Gullhav, A.N.; Andersson, H.; Dale, J.; Karlsen, K. Simulating Emergency Patient Flow during the COVID-19 Pandemic. J. Simul. 2021, 1–15. [Google Scholar] [CrossRef]
- Louhab, Z.; Boufera, F. Modelling and Simulation of Patient Flow in the Emergency Department During the COVID-19 Pandemic Using Hierarchical Coloured Petri Net. Int. J. Open Source Softw. Process. IJOSSP 2022, 13, 1–15. [Google Scholar] [CrossRef]
- Terning, G.; Brun, E.C.; El-Thalji, I. Modeling Patient Flow in an Emergency Department under COVID-19 Pandemic Conditions: A Hybrid Modeling Approach. Healthcare 2022, 10, 840. [Google Scholar] [CrossRef] [PubMed]
- Helse Stavanger, S. Nøkkeltall 2019/2020. Available online: https://helse-stavanger.no/om-oss/nokkeltall-20192020 (accessed on 28 November 2020).
- Suh, H. Om Oss. Available online: https://helse-stavanger.no/om-oss (accessed on 7 February 2019).
- Minge, A. Hun Skal Hele Tiden Være Orakelet og ta Raske og Rette Avgjørelse. Denne Dagen Varte Pausen i 30 Sekunder. Stavanger Aftenblad 2020. Available online: https://www.aftenbladet.no/magasin/i/EWgGxa/hun-skal-hele-tiden-vaere-orakelet-og-ta-raske-og-rette-avgjoerelse-den (accessed on 3 June 2020).
- Gallagher Healthcare What Are the Different Types of Hospitals? Available online: https://www.gallaghermalpractice.com/blog/post/what-are-the-different-types-of-hospitals (accessed on 14 February 2019).
- Randers, J. (Ed.) Elements of the Systems Dynamics Method; Productivity Press: Cambridge, MA, USA, 1980; ISBN 978-0-915299-39-3. [Google Scholar]
- Terning, G.; Brun, E. Systemic Conceptual Modeling of Patient Flow in a Hospital Emergency Department: A Case Example. In Proceedings of the System Dynamics Society Record of the 38th International Conference of the System Dynamics Society, Bergen, Norway, 19–24 July 2020; University of Stavanger: Stavanger, Norway, 2021; Volume 38. [Google Scholar]
- Brailsford, S.C. Hybrid Simulation in Healthcare: New Concepts and New Tools. In Proceedings of the 2015 Winter Simulation Conference (WSC), Huntington Beach, CA, USA, 6–9 December 2015; pp. 1645–1653. [Google Scholar]
- Lättilä, L.; Hilletofth, P.; Lin, B. Hybrid Simulation Models—When, Why, How? Expert Syst. Appl. 2010, 37, 7969–7975. [Google Scholar] [CrossRef]
- Borshchev, A. The Big Book of Simulation Modeling: Multimethod Modeling with Anylogic 6; AnyLogic North America: Chicago, IL, USA, 2013; ISBN 978-0-9895731-7-7. [Google Scholar]
- Ronen, B.; Pliskin, J.S.; Pass, S. The Hospital and Clinic Improvement Handbook: Using Lean and the Theory of Constraints for Better Healthcare Delivery; Oxford University Press: Oxford, UK; New York, NY, USA, 2018; ISBN 978-0-19-084345-8. [Google Scholar]
- Asgary, A.; Najafabadi, M.M.; Karsseboom, R.; Wu, J. A Drive-through Simulation Tool for Mass Vaccination during COVID-19 Pandemic. Healthcare 2020, 8, 469. [Google Scholar] [CrossRef] [PubMed]
- Gul, M.; Guneri, A.F. A Comprehensive Review of Emergency Department Simulation Applications for Normal and Disaster Conditions. Comput. Ind. Eng. 2015, 83, 327–344. [Google Scholar] [CrossRef]
- Ferrer, J.; Salmon, M.; Temime, L. Nosolink: An Agent-Based Approach to Link Patient Flows and Staff Organization with the Circulation of Nosocomial Pathogens in an Intensive Care Unit. Procedia Comput. Sci. 2013, 18, 1485–1494. [Google Scholar] [CrossRef]







| Sc. No. | Explanation | Model and Resource Configuration | |||
|---|---|---|---|---|---|
| PCR [%] | P.T. | E.Tr. | WZ | ||
| Sc. 1 | Base case, pre pandemic operation: This scenario sets the emergency department operation to the pre-pandemic situation, like it was during the time of data gathering. The extra treatment rooms and the waiting zone is not in use and none of the patients will be treated as being virus suspicious. Regular path of patient flow will be followed. This is before any implementation of any novel resources into the ED. | 0 | |||
| Sc. 2 | Scenario simulating situation during pandemic operation. However, no extra resources are introduced, only the new policies are introduced, channeling and expediting the contaminated patients according to the policies. Thus, the E.Tr. and WZ is not in use for this scenario. P.T. is necessarily introduced as it functions as the mechanism of sorting contaminated patients from the non-contaminated patients. | 20 | ✓ | ||
| Sc. 3 | Scenario simulating situation during pandemic operation with E.Tr. introduced. This scenario is made in order to isolate out the effect of the waiting zone that. Otherwise, all else is equal as Sc.2. | 20 | ✓ | ✓ | |
| Sc. 4 | Scenario simulating pandemic operation with WZ introduced: The operation is set up as the case organization during the m, with the only change of excluding the extra treatment. Doing this, we can see how the operation of the ED would be without these four extra treatment rooms used. | 20 | ✓ | ✓ | |
| Sc. 5 | Scenario simulating pandemic operation. The operation is set up as the case organization during the pandemic situation. Doing this, we cans see the combined effect of the two policies. | 20 | ✓ | ✓ | ✓ |
| Abbreviation | Description and Explanation | Unit |
|---|---|---|
| Resources: | ||
| PT | Pre-Triage: A resource introduced for questionnaire and test of the admitted patients before entering the ED. From here patients are treated as either ordinary patients or contaminated patients. | - |
| Tri. | Triage: The place where patients normally, i.e. when not found to be contagious, will go after being admitted to the ED. Patients will wait here until a treatment room is available. | |
| E.TR. | Extra treatment rooms: These are treatment rooms put in addition to the existing treatment rooms in the ED. These are used to accommodate the other adverse effect that the pandemic pose to the ED. | - |
| WZ | Waiting Zone: A dedicated area for ordinary patients whenever they have to leave their treatment room to make room for a contaminated patient. | - |
| Model inputs: | ||
| OP | Ordinary patients: Non-contaminated patients that in the pre-triage were not found to be carriers of pathogens. | # |
| CP | Contaminated patients: Patients that in the pre-triage were found to be contagious and carriers of pathogens and thus risk of | # |
| PCR | Patient contamination rate: A variable that is dependent on spread of infectious decease in the general population. In this study it is set to 0% and 20% according to the scenario design. | % |
| Patient flow indicators: | ||
| TTT | Time to Treatment: The patient flow indicator calculates how long time on average it takes before the treatment of a patient gets started. Values are given in number of hours per patient. | Hours per patient [h/pt] |
| ALOS | Average length of stay—Calculates how long is the average time spent in the emergency department, from point of entry until | Hours per patient [h/pt] |
| Crowding | The crowding indicator tracks how many patient are prevalent in the department at any given time and whenever threshold is passed, the time duration the threshold has been surpassed is divided on the total running time. Crowding is based on the case organization own framework of managing patient flow; ‘Plan for high activity’. Which has defined three crowding levels relevant for the ED: 15, 25 and 30 patients each of which has their specifically tailored modus operandi. | % |
| Peak crowding | This indicator shows how many patients are prevalent on the busiest time of the day and it also keeps the time stamp of when this peak occurred | # & Time |
| Time start use/Time in use | This patient flow indicator shows when relevant resources (i.e. E.TR, Tri. and WZ) was first to be used by a patient during that day. A reading in the Tr.-column at ‘11:00’ means that the triage that day was not used until 11:00. Second value shows the percentage amount of that day this resource has been used at least by one patient. | Time |
| Time full | This patient flow indicator counts how long the different resources has been at their maximal capacity. | Time & % |
| Time in WR | This patient flow indicator calculates the average time patients use in the waiting room. | h |
| Times TR blockedfor con. | This measures counts the amount of times contaminated patients cannot get access to a treatment room. | # |
| Times TR seized | This measure counts how many times a treatment room is seized. | # |
| Day 1 | Day 2 † | |
|---|---|---|
| Real data |  |  |
| Scenario No. | Time to Treatment [h/pt] | ALOS [h/pt] | Crowding [%] (Time Value Passed [When]) | Peak Crowding ED [#] (Time of Peak [When]) | Time Start Use [When] (Time in Use [%]) | Time Full [When] (Time Full [%]) | Time in WR (h/pt) | Times TR Blocked for Cont. (#) | Times TR Seized [#] (Times WZ Seized [#]) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day | Tot. | Ord. | Con. | Tot. | Ord. | Con. | >15 | >25 | >30 | ED | E. TR | Tri. | WZ | E. TR | Tri. | WZ | ||||
| 1 | 1 | 0.674 | 0.674 | null | 2.699 | 2.699 | null | 42.379 (10:45) | 20.182 (14:45) | 0 (null) | 26 (14:45) | null (0.0) | 11:00 (52.876) | null (0.0) | null (0.0) | 14:19 (4.697) | null (0) | 0.034 | 0 | 124 (0) |
| 2 | 1.096 | 1.096 | null | 3.121 | 3.121 | null | 58.518 (11:45) | 39.051 (14:45) | 26.606 (15:00) | 39 (17:15) | null (0.0) | 11:33 (63.199) | null (0.0) | null (0) | 12:48 (39.280) | null (0) | 0.259 | 0 | 138 (0) | |
| 2 | 1 | 0.896 | 1.038 | 0.178 | 3.004 | 3.063 | 2.708 | 47.207 (10:45) | 7.749 (14:15) | 0 (null) | 29 (14:45) | null (0) | 11:00 (58.642) | null (0) | null (0) | 14:18 (10.745) | null (0) | 0.069 | 13 | 124 (0) |
| 2 | 1.124 | 1.372 | 0.255 | 3.261 | 3.397 | 2.785 | 60.883 (11:45) | 41.164 (14:45) | 32.268 (15:00) | 43 (19:30) | null (0) | 11:33 (64.901) | null (0) | null (0) | 13:18 (40.597) | null (0) | 0.261 | 18 | 132 (0) | |
| 3 | 1 | 0.203 | 0.231 | 0.054 | 2.311 | 2.258 | 2.585 | 29.420 (10:45) | 0 (null) | 0 (null) | 24 (14:45) | 11:00 (46.275) | 12:03 (21.252) | null (0) | 11:00 (28.675) | null (0) | null (0) | 0.028 | 3 | 124 (0) |
| 2 | 0.714 | 0.878 | 0.212 | 2.865 | 2.905 | 2.743 | 47.828 (11:45) | 23.168 (13:15) | 7.106 (15:15) | 35 (17:30) | 11:33 (59.467) | 12:18 (45.931) | null (0) | 11:48 (48.140) | 15:18 (10.606) | null (0) | 0.081 | 22 | 146 (0) | |
| 4 | 1 | 0.979 | 1.181 | 0.030 | 3.094 | 3.208 | 2.560 | 53.000 (10:45) | 7.777 (14:15) | 0 (null) | 30 (15:45) | null (0) | 11:00 (60.379) | 11:00 (16.165) | null (0) | 14:18 (12.496) | null (0) | 0.084 | 2 | 140 (16) |
| 2 | 1.212 | 1.604 | 0.039 | 3.367 | 3.633 | 2.568 | 61.392 (11:45) | 43.797 (13:15) | 35.687 (15:00) | 46 (17:30) | null (0) | 11:33 (64.683) | 11:45 (26.540) | null (0) | 13:03 (39.153) | null (0) | 0.259 | 8 | 158 (25) | |
| 5 | 1 | 0.210 | 0.245 | 0.029 | 2.320 | 2.273 | 2.561 | 29.543 (10:45) | 0 (null) | 0 (null) | 25 (14:45) | 11:00 (46.277) | 12:03 (21.085) | 12:15 (4.964) | 11:00 (31.066) | null (0) | null (0) | 0.029 | 1 | 130 (6) |
| 2 | 0.845 | 1.134 | 0.033 | 3.006 | 3.164 | 2.563 | 49.997 (11:45) | 26.996 (13:00) | 11.996 (15:15) | 39 (17:30) | 11:33 (66.143) | 11:33 (66.143) | 12:15 (21.178) | 11:48 (51.553) | 15:03 (17.136) | null (0) | 0.147 | 5 | 168 (22) | |
| Key Patient Flow Indicator | Day 1 | Day 2 |
|---|---|---|
| Time to treatment (TtT) | 0.674 | 1.096 |
| Average length of stay (ALOS) | 2.699 | 3.121 |
| Crowding > 15% | 42,379 | 58,518 |
| Peak crowding | 26 | 39 |
| Times treatment room (TR) is blocked | 0 | 0 |
| Day 1 | Day 2 † | |
|---|---|---|
| (Sc. 1) |  |  |
 | ||
| Key Patient Flow Indicator | Day 1 | Day 2 | ||||
|---|---|---|---|---|---|---|
| Patient Type: | All | Ord | Con | All | Ord | Con |
| Time to treatment (TtT) | 0.896 | 1.038 | 0.178 | 1.124 | 1.372 | 0.255 |
| Average length of stay (ALOS) | 3.004 | 2.063 | 2.708 | 3.261 | 3.397 | 2785 |
| Crowding > 15% | 47.207 | 60.883 | ||||
| Peak crowding | 29 | 43 | ||||
| Times treatment room (TR) is blocked | 13 | 18 | ||||
| Day 1 | Day 2 † | |
|---|---|---|
| (Sc. 1) |  |  |
| (Sc. 2) |  |  |
 | ||
| Key Patient Flow Indicator | Day 1 | Day 2 | ||||
|---|---|---|---|---|---|---|
| Patient Group: | All | Ord | Con | All | Ord | Con |
| Time to treatment (TtT) | 0.203 | 0.231 | 0.054 | 0.714 | 0.878 | 0.212 |
| Average length of stay (ALOS) | 2.311 | 2.258 | 2.585 | 2.865 | 2.905 | 2.743 |
| Crowding > 15% | 29.420 | 47.828 | ||||
| Peak crowding | 24 | 35 | ||||
| Times treatment room (TR) is blocked | 3 | 22 | ||||
| Times TR seized | 124 | 146 | ||||
| Day 1 | Day 2† | |
|---|---|---|
| (Sc. 2) |  |  |
| (Sc. 3) |  |  |
 | ||
| Key Patient Flow Indicator | Day 1 | Day 2 | ||||
|---|---|---|---|---|---|---|
| Patient Group: | All | Ord | Con | All | Ord | Con |
| Time to treatment (TtT) | 0.979 | 1.181 | 0.030 | 1.212 | 1.604 | 0.039 |
| Average length of stay (ALOS) | 3.094 | 3.208 | 2.560 | 3.367 | 3.633 | 2.568 |
| Crowding > 15% | 53.000 | 61.392 | ||||
| Peak crowding | 30 | 46 | ||||
| Times treatment room (TR) is blocked | 2 | 8 | ||||
| Times TR seized | 140 | 158 | ||||
| Day 1 | Day 2 † | |
|---|---|---|
| (Sc. 2) |  |  |
| (Sc. 4) |  |  |
 | ||
| Key Patient Flow Indicator | Day 1 | Day 2 | ||||
|---|---|---|---|---|---|---|
| Patient Group: | All | Ord | Con | All | Ord | Con |
| Time to treatment (TtT) | 0.210 | 0.245 | 0.029 | 0.845 | 1.134 | 0.033 |
| Average length of stay (ALOS) | 2.320 | 2.273 | 2.561 | 3.006 | 3.164 | 2.563 |
| Crowding > 15% | 29.543 | 49.997 | ||||
| Peak crowding | 25 | 39 | ||||
| Times treatment room (TR) is blocked | 1 | 5 | ||||
| Times TR seized | 130 | 168 | ||||
| Day 1 | Day 2 † | |
|---|---|---|
| (Sc. 2) |  |  |
| (Sc. 5) |  |  |
 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terning, G.; Brun, E.C.; El-Thalji, I. The Patient Flow Effect of Pandemic Policies: A Hybrid Simulation Study in a Norwegian Emergency Department. Healthcare 2023, 11, 1. https://doi.org/10.3390/healthcare11010001
Terning G, Brun EC, El-Thalji I. The Patient Flow Effect of Pandemic Policies: A Hybrid Simulation Study in a Norwegian Emergency Department. Healthcare. 2023; 11(1):1. https://doi.org/10.3390/healthcare11010001
Chicago/Turabian StyleTerning, Gaute, Eric Christian Brun, and Idriss El-Thalji. 2023. "The Patient Flow Effect of Pandemic Policies: A Hybrid Simulation Study in a Norwegian Emergency Department" Healthcare 11, no. 1: 1. https://doi.org/10.3390/healthcare11010001