
Sulphurous Crenotherapy Is Effective at Reducing Pain and Disability in Overweight/Obese Patients Affected by Chronic Low Back Pain from Spine Osteoarthritis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
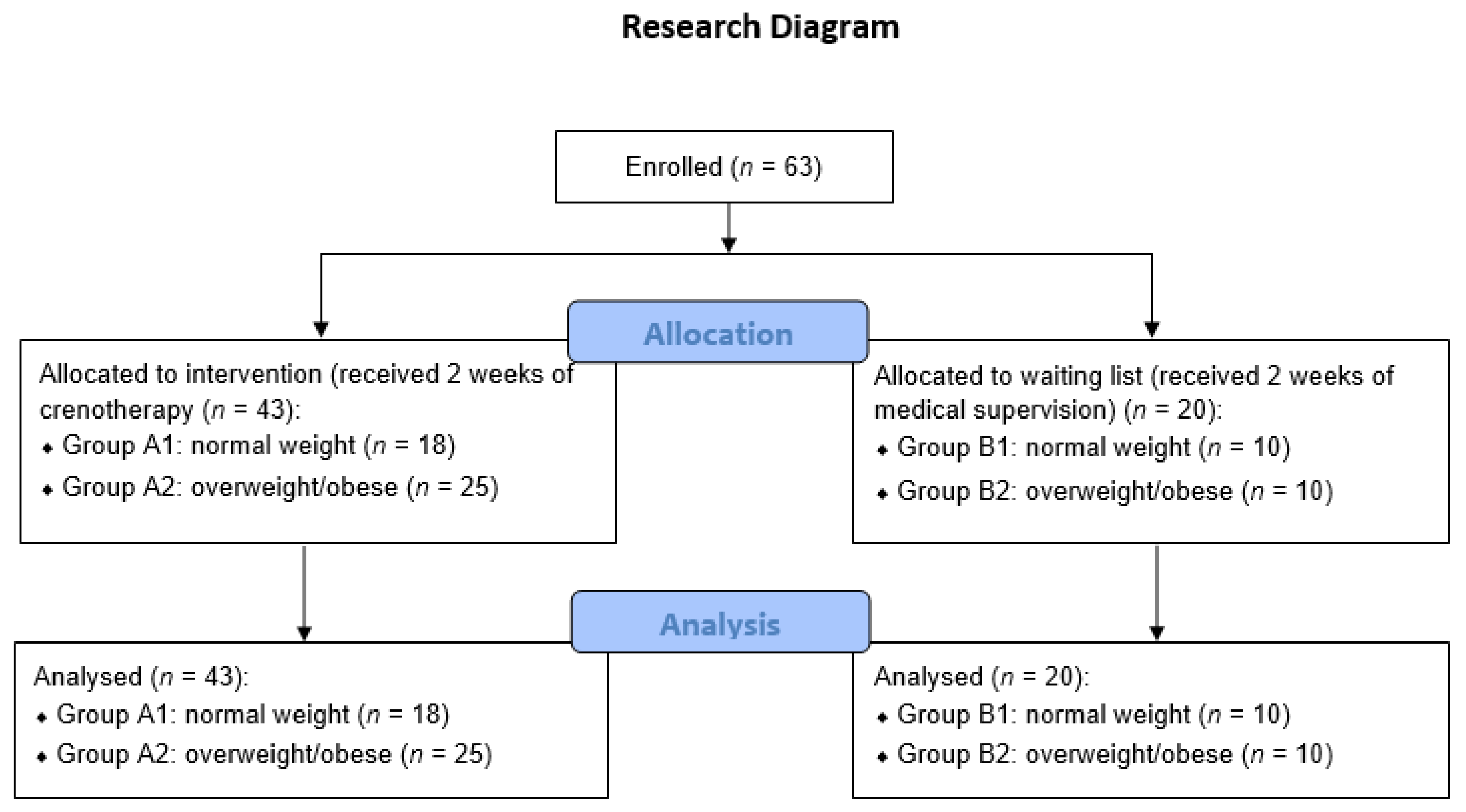
2.1. Study Population and Study Design
2.2. Sulphurous Crenotherapy
2.3. Control Groups
2.4. Ethical Issues
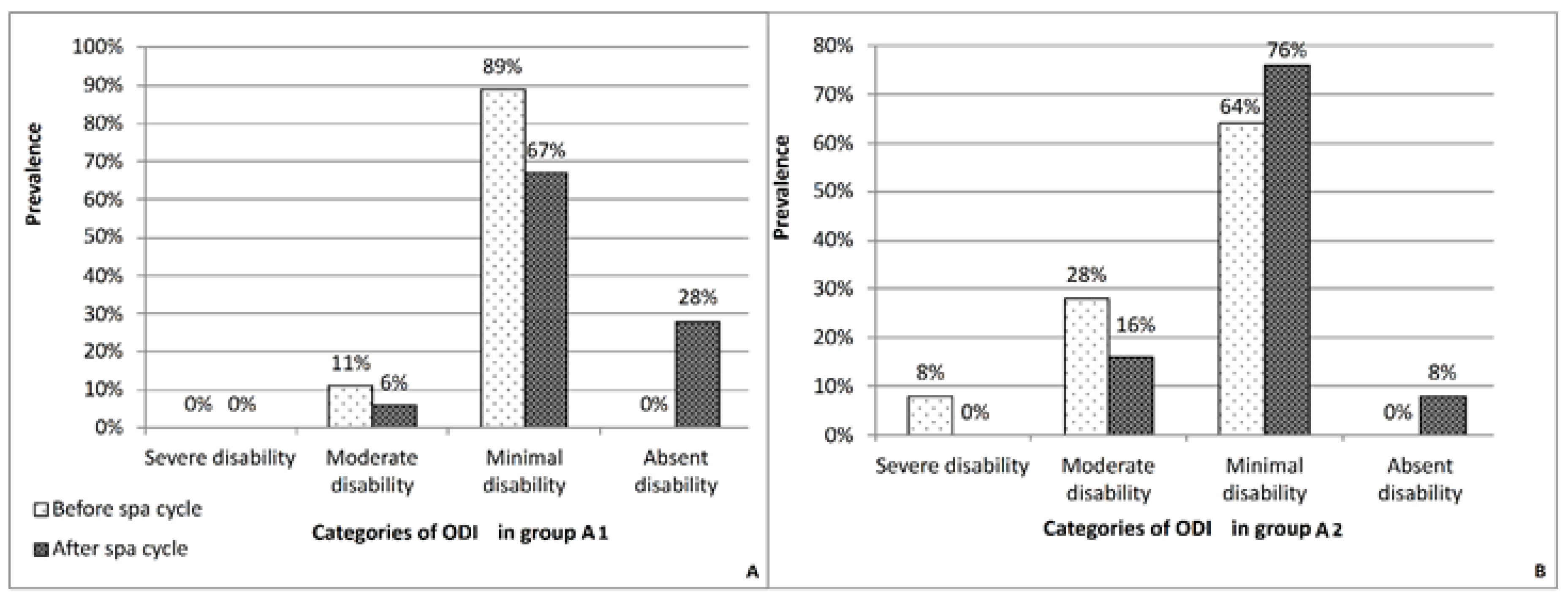
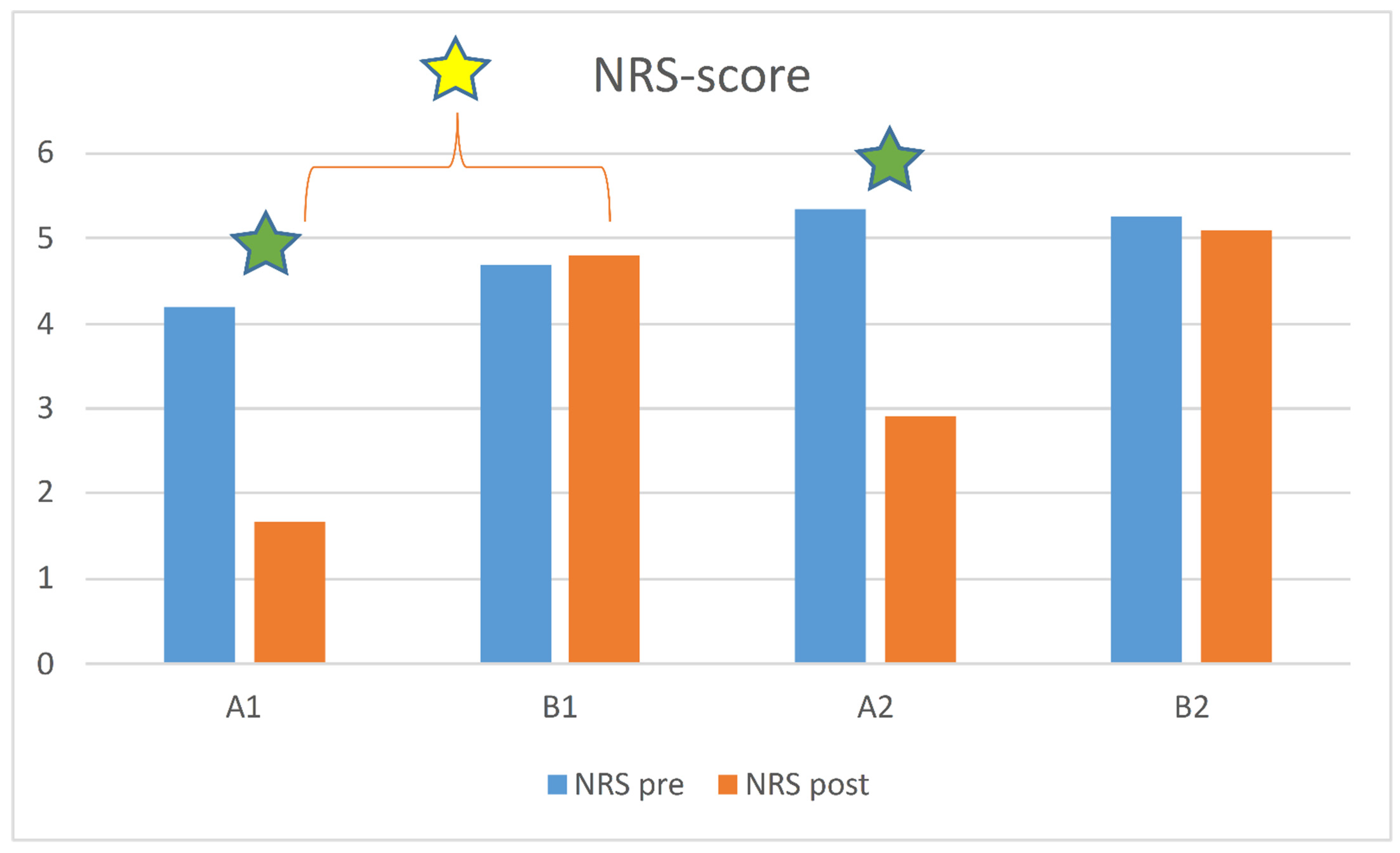
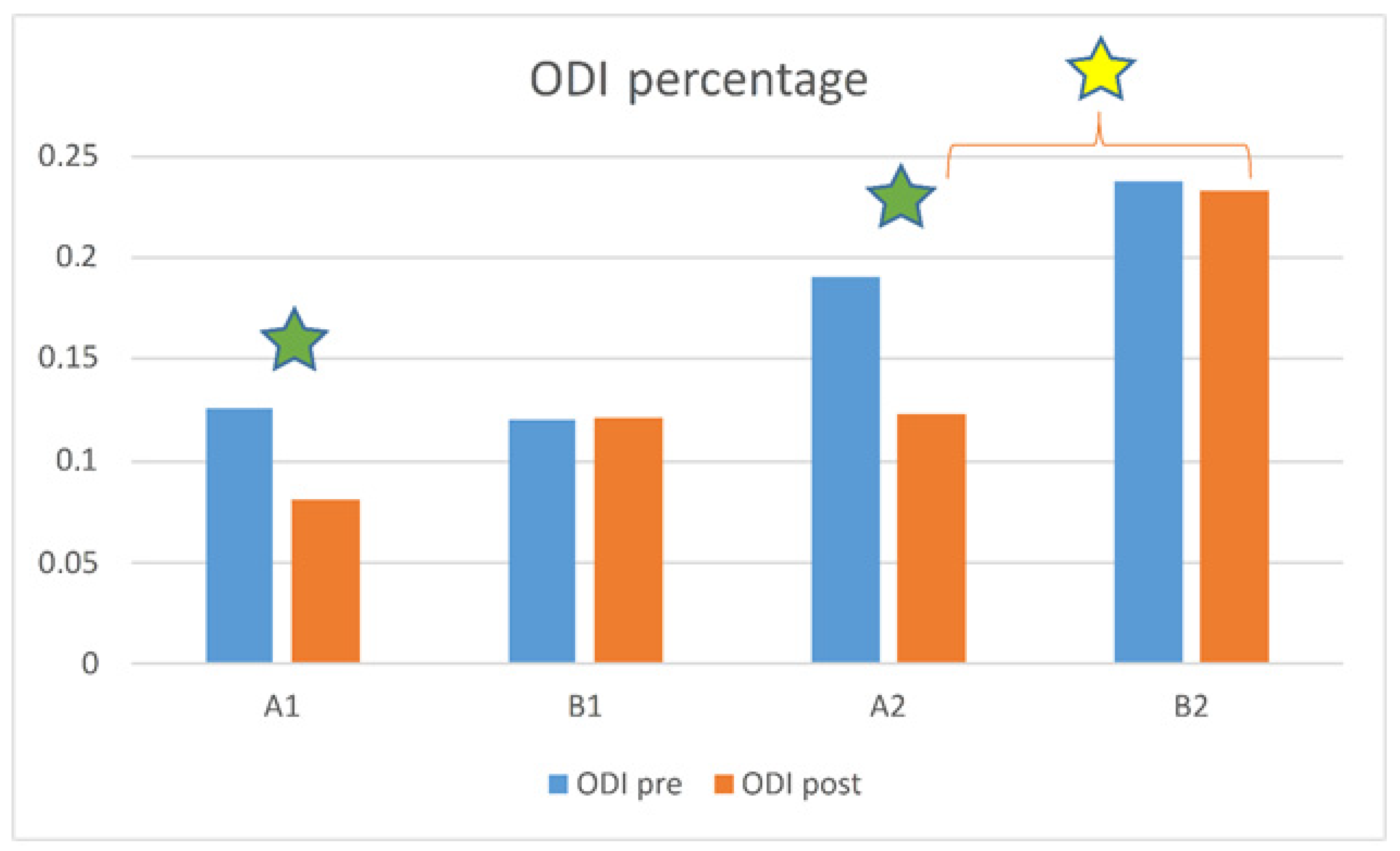
2.5. Measurements
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef]
- Shiri, R.; Karppinen, J.; Leino-Arjas, P.; Solovieva, S.; Viikari-Juntura, E. The association between obesity and low back pain: A meta-analysis. Am. J. Epidemiol. 2010, 171, 135–154. [Google Scholar] [CrossRef] [PubMed]
- Janke, E.A.; Collins, A.; Kozak, A.T. Overview of the relationship between pain and obesity: What do we know? Where do we gonext? J. Rehabil. Res. Dev. 2007, 44, 245–262. [Google Scholar] [CrossRef]
- Øiestad, B.E.; Hilde, G.; Tveter, A.T.; Peat, G.G.; Thomas, M.J.; Dunn, K.M.; Grotle, M. Risk factors for episodes of back pain in emerging adults. A systematic review. Eur. J. Pain 2020, 24, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Heuch, I.; Heuch, I.; Hagen, K.; Zwart, J.A. Body mass index as a risk factor for developing chronic low back pain: A follow-up in the Nord-Trøndelag Health Study. Spine 2013, 38, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Johannes, C.B.; Le, T.K.; Zhou, X.; Johnston, J.A.; Dworkin, R.H. The prevalence of chronic pain in United States adults: Results of an Internet-based survey. J. Pain 2010, 11, 1230–1239. [Google Scholar] [CrossRef]
- Elgaeva, E.E.; Tsepilov, Y.; Freidin, M.B.; Williams, F.M.K.; Aulchenko, Y.; Suri, P. ISSLS Prize in Clinical Science 2020. Examining causal effects of body mass index on back pain: A Mendelian randomization study. Eur. Spine J. 2020, 29, 686–691. [Google Scholar] [CrossRef]
- Webb, R.; Brammah, T.; Lunt, M.; Urwin, M.; Allison, T.; Symmons, D. Prevalence and predictors of intense, chronic, and disabling neck and back pain in the UK general population. Spine 2003, 28, 1195–1202. [Google Scholar] [CrossRef]
- Smuck, M.; Kao, M.C.; Brar, N.; Martinez-Ith, A.; Choi, J.; Tomkins-Lane, C.C. Does physical activity influence the relationship between low back pain and obesity? Spine J. 2014, 14, 209–216. [Google Scholar] [CrossRef]
- Heo, M.; Allison, D.; Faith, M.S.; Zhu, S.; Fontaine, K.R. Obesity and quality of life: Mediating effects of pain and comorbidities. Obes. Res. 2003, 11, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Arranz, L.-I.; Rafecas, M.; Alegre, C. Effects of Obesity on Function and Quality of Life in Chronic Pain Conditions. Curr. Rheumatol. Rep. 2014, 16, 390. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Iosa, M.; Paolucci, T.; Fusco, A.; Alcuri, R.; Spadini, E.; Saraceni, V.M.; Paolucci, S. Efficacy of perceptive rehabilitation in the treatment of chronic nonspecific low back pain through a new tool: A randomized clinical study. Clin. Rehabil. 2012, 26, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Paolucci, T.; Morone, G.; Iosa, M.; Fusco, A.; Alcuri, R.; Matano, A.; Bureca, I.; Saraceni, V.M.; Paolucci, S. Psychological features and outcomes of the Back School treatment in patients with chronic non-specific low back pain. A randomized controlled study. Eur. J. Phys. Rehabil. Med. 2012, 48, 245–253. [Google Scholar]
- Morone, G.; Paolucci, T.; Alcuri, M.R.; Vulpiani, M.C.; Matano, A.; Bureca, I.; Paolucci, S.; Saraceni, V.M. Quality of life improved by multidisciplinary back school program in patıents with chronic non-specific low back pain: A single blind randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2011, 47, 533–541. [Google Scholar]
- White, A.P.; Arnold, P.M.; Norvell, D.C.; Ecker, E.; Fehlings, M.G. Pharmacologic management of chronic low back pain: Synthesis of the evidence. Spine 2011, 36 (Suppl. 21), S131–S143. [Google Scholar] [CrossRef]
- Paans, N.; van den Akker-Scheek, I.; Van der Meer, K.; Bulstra, S.K.; Stevens, M. The effects of exercise and weight loss in overweight patients with hip osteo-arthritis: Design of a prospective cohort study. BMC Musculoskelet. Disord. 2009, 10, 24. [Google Scholar] [CrossRef]
- Hayden, J.A.; Wilson, M.N.; Stewart, S.; Cartwright, J.L.; Smith, A.O.; Riley, R.D.; Van Tulder, M.; Bendix, T.; Cecchi, F.; Costa, L.O.P.; et al. Exercise treatment effect modifiers in persistent low back pain: An individual participant data meta-analysis of 3514 participants from 27 randomized controlled trials. Br. J. Sports Med. 2020, 54, 1277–1278. [Google Scholar] [CrossRef]
- Gutenbrunner, C.; Bender, T.; Cantista, P.; Karagülle, Z. A proposal for a worldwide definition of health resort medicine, balneology, medical hydrology and climatology. Int. J. Biometeorol. 2010, 54, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Li, C.; Xiao, Y.; Sharma, M.; Zhang, F.; Zhao, Y. Effectiveness of spa therapy for patients with chronic low back pain: An updated systematic review and meta-analysis. Medicine 2019, 98, e17092. [Google Scholar] [CrossRef]
- Rubinstein, S.M.; van Middelkoop, M.; Kuijpers, T.; Ostelo, R.; Verhagen, A.P.; de Boer, M.R.; Koes, B.W.; van Tulder, M.W. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur. Spine J. 2010, 19, 1213–1228. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.; Conti, V.; Corbi, G.; Marongiu, F.; Marongiu, M.B.; Filippelli, A. Sulphurous mud-bath therapy for treatment of Chronic Low Back Pain caused by Lumbar Spine Osteoarthritis. Intern. Emerg. Med. 2019, 14, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Karagülle, M.; Kardeş, S.; Karagülle, M.Z. Real-life effectiveness of spa therapy in rheumatic and musculoskeletal diseases: A retrospective study of 819 patients. Int. J. Biometereol. 2017, 61, 1945–1956. [Google Scholar] [CrossRef] [PubMed]
- Guillemin, F.; Virion, J.M.; Escudier, P.; De Talancé, N.; Weryha, G. Effect on osteoarthritis of spa therapy at Bourbonne-les-Bains. Jt. Bone Spine 2001, 68, 499–503. [Google Scholar] [CrossRef]
- Kardeş, S.; Karagülle, M.; Geçmen, İ.; Adıgüzel, T.; Yücesoy, H.; Karagülle, M.Z. Outpatient balneological treatment of osteoarthritis in older persons: A retrospective study. Z. Gerontol. Geriatr. 2019, 52, 164–171. [Google Scholar] [CrossRef]
- Costantino, M. Sulphur mud-bath treatment in osteoarthrosis: Therapeutic activity and efficiency on the quality of life. Clin. Ter. 2006, 157, 525–529. [Google Scholar] [PubMed]
- Costantino, M.; Lampa, E. Long-term effects of sulphureous well mud-therapy: Epidemiological study. Med. Clin. Term. 2002, 14, 347–361. [Google Scholar]
- Costantino, M.; Lampa, E. Therapeutic and adverse drug effects of mud-balneotherapy for rheumatic diseases over the medium-term: An epidemiological study. Ig. Mod. 2001, 116, 21–36. [Google Scholar]
- Masiero, S.; Vittadini, F.; Ferroni, C.; Bosco, A.; Serra, R.; Frigo, A.C.; Frizziero, A. The role of thermal balneotherapy in the treatment of obese patient with knee osteoarthritis. Int. J. Biometeorol. 2018, 62, 243–252. [Google Scholar] [CrossRef]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies Comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for Assessment of Pain Intensity in Adults: A Systematic Literature Review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Monticone, M.; Baiardi, P.; Ferrari, S.; Foti, C.; Mugnai, R.; Pillastrini, P.; Carla, V.; Gustavo, Z. Development of the Italian version of the Oswestry Disability Index (ODI-I): A cross-cultural adaptation, reliability, and validity study. Spine 2009, 34, 2090–2095. [Google Scholar] [CrossRef] [PubMed]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 15, 2940–2952. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, A.; Stickley, A.; Garin, N.; Miret, M.; Ayuso-Mateos, J.L.; Leonardi, M.; Koskinen, S.; Galas, A.; Haro, J.M. The association between obesity and back pain in nine countries: A cross-sectional study. BMC Public Health 2015, 15, 123. [Google Scholar] [CrossRef]
- Hozumi, J.; Sumitani, M.; Matsubayashi, Y.; Abe, H.; Oshima, Y.; Chikuda, H.; Takeshita, K.; Yamada, Y. Relationship between Neuropathic Pain and Obesity. Pain Res. Manag. 2016, 2016, 2487924. [Google Scholar] [CrossRef] [PubMed]
- Samartzis, D.; Karppinen, J.; Cheung, J.P.Y.; Lotz, J. Disk degeneration and low back pain: Are they fat-related conditions? Glob. Spin J. 2013, 3, 133–144. [Google Scholar] [CrossRef]
- Walsh, T.P.; Arnold, J.B.; Evans, A.M.; Yaxley, A.; Damarell, R.A.; Shanahan, E.M. The association between body fat and musculoskeletal pain: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2018, 19, 233. [Google Scholar] [CrossRef]
- Husky, M.M.; Farin, F.F.; Compagnone, P.; Fermanian, C.; Kovess-Masfety, V. Chronic back pain and its association with quality of life in a large French population survey. Health Qual. Life Outcomes 2018, 16, 195. [Google Scholar] [CrossRef]
- Bultink, I.E.M.; Vis, M.; van der Horst-Bruinsma, I.E.; Lems, W.F. Inflammatory rheumatic disorders and bone. Curr. Rheumatol. Rep. 2012, 14, 224–230. [Google Scholar] [CrossRef]
- Gandhi, R.; Razak, F.; Davey, J.R.; Mahomed, N.N. Metabolic syndrome and the functional outcomes of hip and knee arthroplasty. J. Rheumatol. 2010, 37, 1917–1922. [Google Scholar] [CrossRef]
- Scalabrino, A.; Galassi, A.; Pierallini, F.; Gigli, P.; Pieraccini, A.; Mignani, E.; Ciappei, G.C.; Teofoli, p.; Mancini, A.; Lotti, T. A single mud-bath treatment induces increased levels of circulating endogeneous opioids. Current 1994, 2, 5–10. [Google Scholar]
- Costantino, M.; Filippelli, A.; Quenau, P.; Nicolas, J.P.; Coiro, V. Sulphur mineral water and SPA therapy in osteoarthritis. Therapie 2012, 67, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.; Filippelli, A. Knee osteoarthritis and SPA therapy: Assessment of joint function and quality of life. Clin. Ter. 2011, 162, e51-7. [Google Scholar]
- Caraglia, M.; Beninati, S.; Giuberti, G.; D’Alessandro, A.M.; Lentini, A.; Abbruzzese, A.; Bove, G.; Landolfi, F.; Rossi, F.; Lampa, E.; et al. Alternative therapy of earth elements increases the chondroprotective effects of chondroitin-sulfate in mice. Exp. Mol. Med. 2005, 37, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.; Giampaolo, C.; Filippelli, A. Effects of drinking SPA therapy on oxidative stress. Clin. Ter. 2012, 163, e13-7. [Google Scholar]
- Braga, P.C.; Ceci, C.; Marabini, L.; Nappi, G. The antioxidant activity of sulphurous thermal water protects against oxidative DNA damage: A comet assay investigation. Drug Res. 2013, 63, 198–202. [Google Scholar] [CrossRef]
- Costantino, M.; Conti, V.; Corbi, G.; Filippelli, A. Hydropinotherapy with Sulphurous Mineral Water as Complementary Treatment to Improve Glucose Metabolism, Oxidative Status, and Quality of Life. Antioxidants 2021, 10, 1773. [Google Scholar] [CrossRef]
- Karagülle, M.; Karagülle, M.Z. Effectiveness of balneotherapy and spa therapy for the treatment of chronic low back pain: A review on latest evidence. Clin. Rheumatol. 2015, 34, 207–214. [Google Scholar] [CrossRef]
- Nguyen, M.; Revel, M.; Dougados, M. Prolonged effects of 3 week therapy in a spa resort on lumbar spine, knee and hip osteoarthritis: Follow-up after 6 months. A randomized controlled trial. Br. J. Rheumatol. 1997, 36, 77–81. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) Mean ± SD | Range Age (Years) | Median | Female % | Male % | BMI * Mean ± SD | |
|---|---|---|---|---|---|---|
| Study group (n = 43) | 63 ± 8.8 | 41–81 | 62 | 58 | 42 | 27.7 ± 4.7 |
| A1 subgroup (n = 18) | 63 ± 8.9 | 44–81 | 62 | 37 | 33 | 23.7 ± 0.97 |
| A2 subgroup (n = 25) | 62 ± 8.9 | 41–77 | 61 | 52 | 48 | 30.6 ± 4.2 |
| Control group (n = 20) | 63 ± 11 | 46–83 | 62 | 60 | 40 | 26.6 ± 5.3 |
| B1 subgroup (n = 10) | 61 ± 8.8 | 47–80 | 59 | 70 | 30 | 22.3 ± 1.9 |
| B2 subgroup (n = 10) | 65.5 ± 13.2 | 46–83 | 65.5 | 50 | 50 | 30.8 ± 3.9 |
| Total NRS Score | |||
|---|---|---|---|
| Subgroup (n) | Before | After | p-Value |
| A1 (18) | 4.2 ± 2.7 | 1.7 ± 1.9 | <0.001 |
| A2 (25) | 5.36 ± 3.0 | 2.92 ± 2.4 | 0.0005 |
| B1 (10) | 4.7 ± 3.1 | 4.8 ± 3.0 | 0.4 |
| B2 (10) | 5.3 ± 2.7 | 5.1 ± 2.7 | 0.1 |
| Subgroup (n) | Total ODI Score | Mean ± SD | p-Value (Wilcoxon Test) |
|---|---|---|---|
| Before | After | ||
| A1 (18) | 13% ± 0.08 | 8% ± 0.08 | p < 0.001 |
| B1 (10) | 12.05% ± 0.1 | 12.10% ± 0.1 | p > 0.05 |
| A2 (25) | 19% ± 0.13 | 12% ± 0.10 | p = 0.001 |
| B2 (10) | 23.8% ± 0.1 | 23.3% ± 0.1 | p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costantino, M.; Conti, V.; Corbi, G.; Ciancarelli, I.; Morone, G.; Filippelli, A. Sulphurous Crenotherapy Is Effective at Reducing Pain and Disability in Overweight/Obese Patients Affected by Chronic Low Back Pain from Spine Osteoarthritis. Healthcare 2022, 10, 1800. https://doi.org/10.3390/healthcare10091800
Costantino M, Conti V, Corbi G, Ciancarelli I, Morone G, Filippelli A. Sulphurous Crenotherapy Is Effective at Reducing Pain and Disability in Overweight/Obese Patients Affected by Chronic Low Back Pain from Spine Osteoarthritis. Healthcare. 2022; 10(9):1800. https://doi.org/10.3390/healthcare10091800
Chicago/Turabian StyleCostantino, Maria, Valeria Conti, Graziamaria Corbi, Irene Ciancarelli, Giovanni Morone, and Amelia Filippelli. 2022. "Sulphurous Crenotherapy Is Effective at Reducing Pain and Disability in Overweight/Obese Patients Affected by Chronic Low Back Pain from Spine Osteoarthritis" Healthcare 10, no. 9: 1800. https://doi.org/10.3390/healthcare10091800