
Cognitive Benefits of Exercise: Is There a Time-of-Day Effect?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Measures
2.3.1. The International Physical Activity Questionnaire
2.3.2. The Borg Scale
2.3.3. The d2 Test of Attention
2.4. Procedure
3. Results
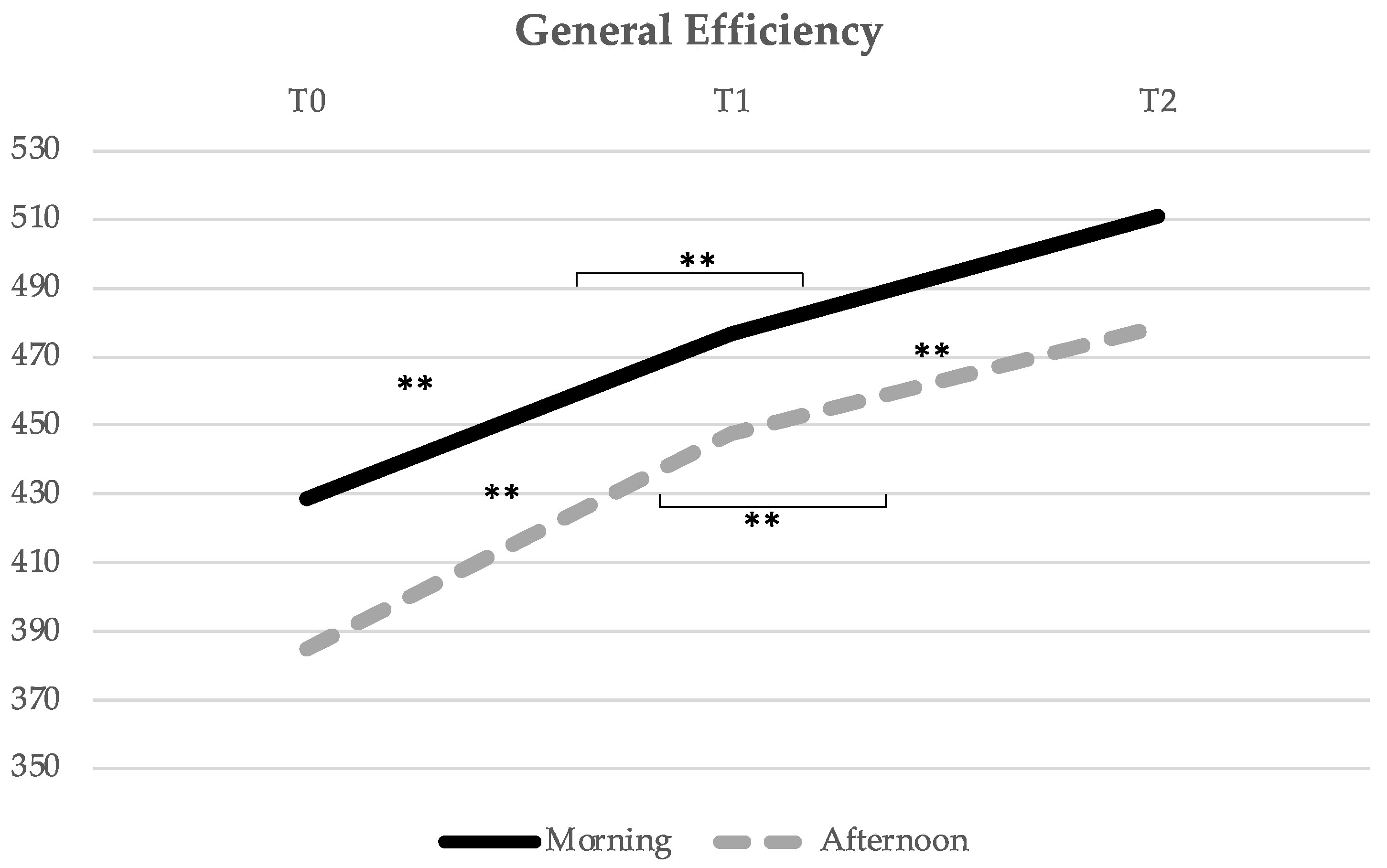
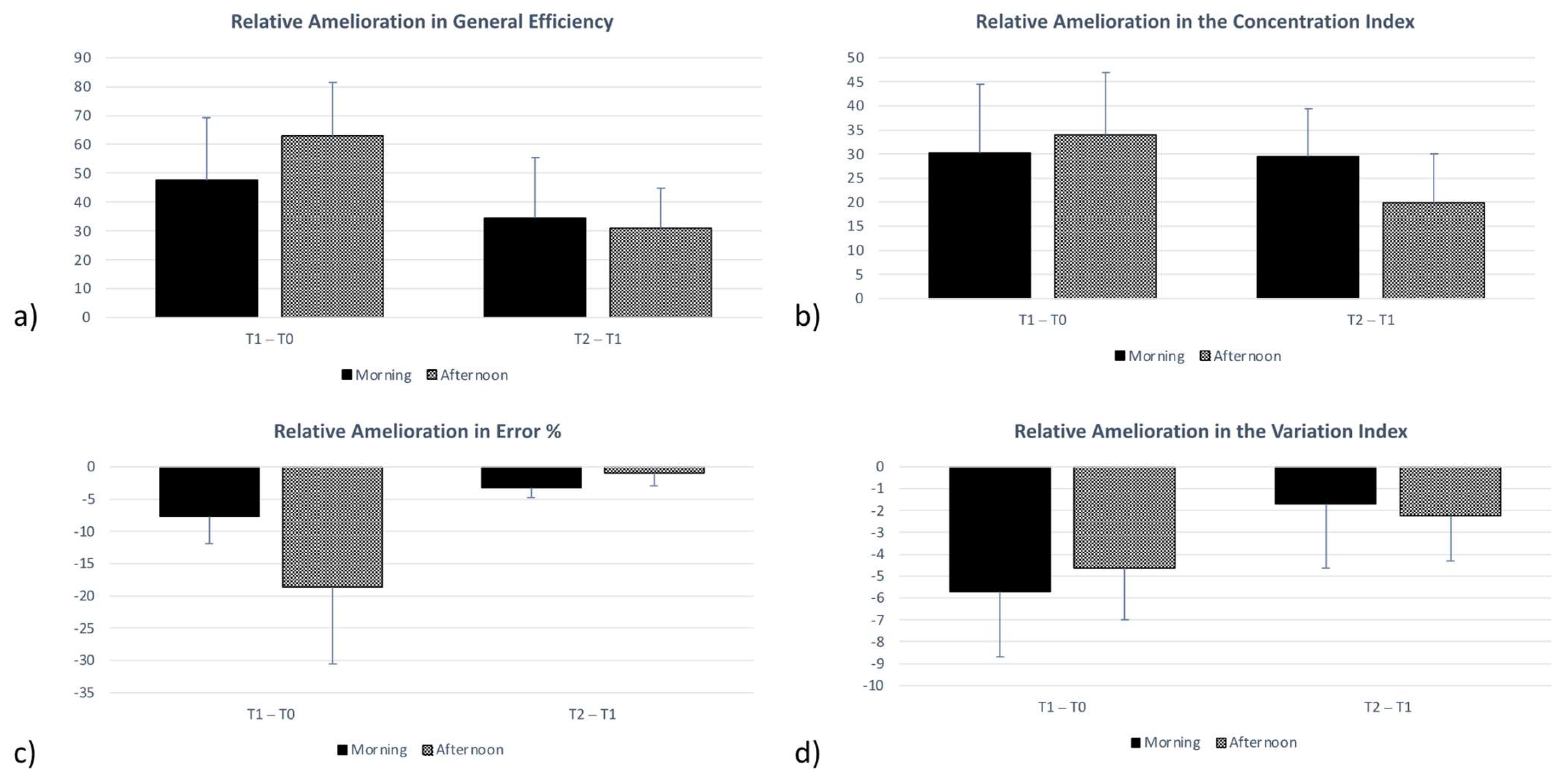
3.1. General Efficiency
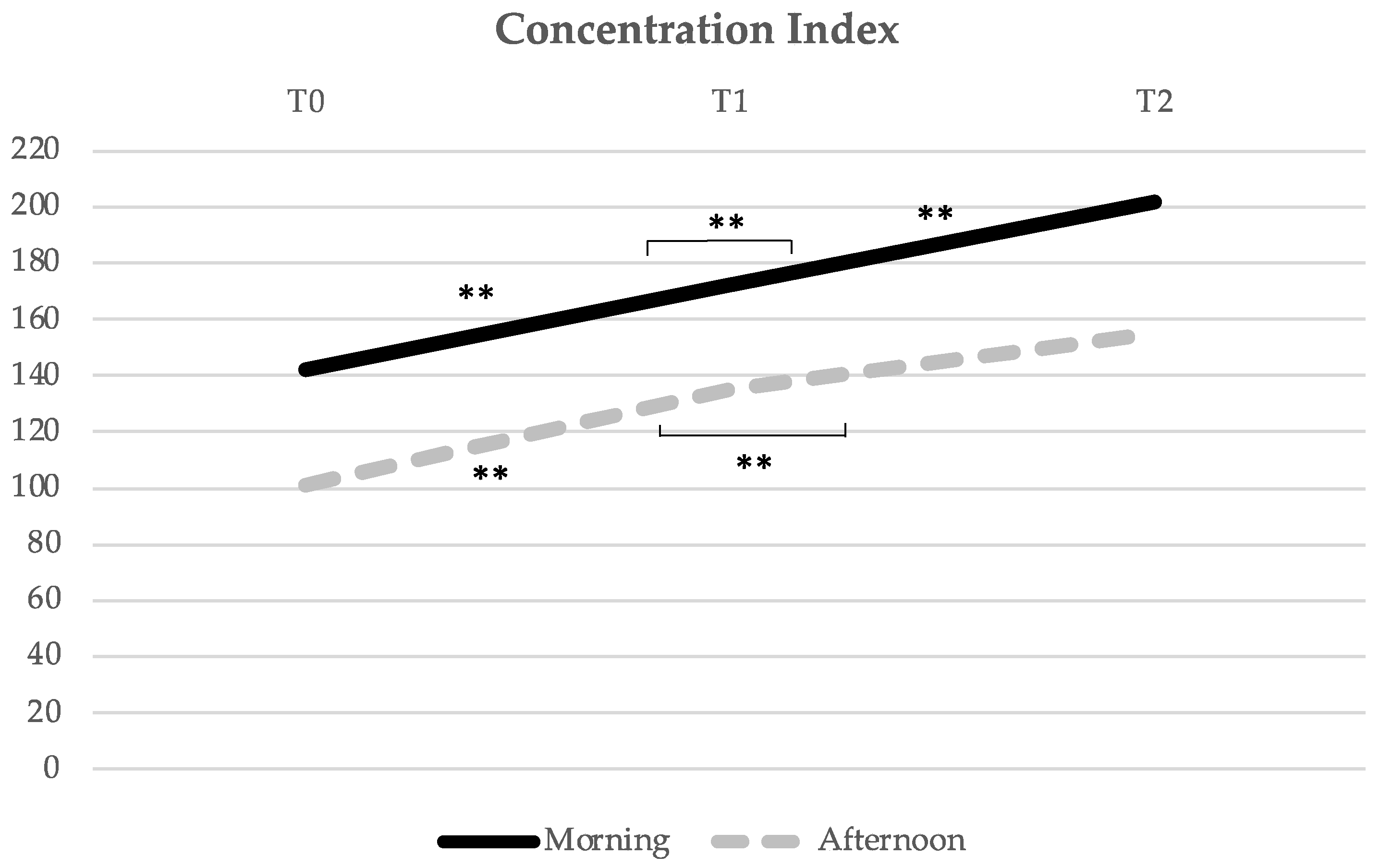
3.2. Concentration Index
3.3. Error Percentage
3.4. Variation Index
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ludyga, S.; Gerber, M.; Pühse, U.; Looser, V.N.; Kamijo, K. Systematic review and meta-analysis investigating moderators of long-term effects of exercise on cognition in healthy individuals. Nat. Hum. Behav. 2020, 4, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical activity, cognition, and brain outcomes: A review of the 2018 physical activity guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of physical activity on neurocognitive function: A review at multiple levels of analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Ogoh, S.; Tsukamoto, H.; Hirasawa, A.; Hasegawa, H.; Hirose, N.; Hashimoto, T. The effect of changes in cerebral blood flow on cognitive function during exercise. Physiol. Rep. 2014, 2, e12163. [Google Scholar] [CrossRef]
- Abreu, M.A.; Frade, I. Running against the schedule: Are children exercising at the right time? A comment on the Portuguese education system. Pressing 2020, 12, 33–40. [Google Scholar] [CrossRef]
- Chan, J.S.Y.; Liu, G.; Liang, D.; Deng, K.; Wu, J.; Yan, J.H. Special issue–therapeutic benefits of physical activity for mood: A systematic review on the effects of exercise intensity, duration, and modality. J. Psychol. Interdiscip. Appl. 2019, 153, 102–125. [Google Scholar] [CrossRef]
- Buecker, S.; Simacek, T.; Ingwersen, B.; Terwiel, S.; Simonsmeier, B.A. Physical activity and subjective well-being in healthy individuals: A meta-analytic review. Health Psychol. Rev. 2021, 15, 574–592. [Google Scholar] [CrossRef]
- Andersen, M.H.; Ottesen, L.; Thing, L.F. The social and psychological health outcomes of team sport participation in adults: An integrative review of research. Scand. J. Public Health 2019, 47, 832–850. [Google Scholar] [CrossRef]
- Fernandes, R.M.; Correa, M.G.; dos Santos, M.A.R.; Almeida, A.P.C.P.S.C.; Fagundes, N.C.F.; Maia, L.C.; Lima, R.R. The effects of moderate physical exercise on adult cognition: A systematic review. Front. Physiol. 2018, 9, 667. [Google Scholar] [CrossRef]
- Chen, Z.; Lan, W.; Yang, G.; Li, Y.; Ji, X.; Chen, L.; Zhou, Y.; Li, S. Exercise intervention in treatment of neuropsychological diseases: A review. Front. Psychol. 2020, 11, 569206. [Google Scholar] [CrossRef]
- Haverkamp, B.F.; Wiersma, R.; Vertessen, K.; van Ewijk, H.; Oosterlaan, J.; Hartman, E. Effects of physical activity interventions on cognitive outcomes and academic performance in adolescents and young adults: A meta-analysis. J. Sports Sci. 2020, 38, 2637–2660. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Blumenthal, J.A.; Hoffman, B.M.; Cooper, H.; Strauman, T.A.; Welsh-Bohmer, K.; Browndyke, J.N.; Sherwood, A. Aerobic exercise and neurocognitive performance: A meta-analytic review of randomized controlled trials. Psychosom. Med. 2010, 72, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.V. Selective sustained attention: A developmental foundation for cognition. Curr. Opin. Psychol. 2019, 29, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Tomporowski, P.D. Effects of acute bouts of exercise on cognition. Acta Psychologica 2003, 112, 297–324. [Google Scholar] [CrossRef]
- Alves, C.R.R.; Tessaro, V.H.; Teixeira, L.A.C.; Murakava, K.; Roschel, H.; Gualano, B.; Takito, M.Y. Influence of acute high-intensity aerobic interval exercise bout on selective attention and short-term memory tasks. Percept. Motor Skills 2014, 118, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Brisswalter, J.; Collardeau, M.; René, A. Effects of acute physical exercise characteristics on cognitive performance. Sports Med. 2002, 32, 555–566. [Google Scholar] [CrossRef]
- Oliveira, P.A.; Araújo, D.; Abreu, A.M. Proneness for exercise, cognitive and psychophysiological consequences of action observation. Psychol. Sport Exerc. 2014, 15, 39–47. [Google Scholar] [CrossRef]
- Chtourou, H.; Souissi, N. The effect of training at a specific time of day: A review. J. Strength Cond. Res. 2012, 26, 1984–2005. [Google Scholar] [CrossRef]
- Elghoul, Y.; Frikha, M.; Abdelmlak, S.; Chtourou, H.; Dammak, K.; Chamari, K.; Souissi, N. Time-of-day effect on dart-throwing performance and the perception of the difficulty of the task in 9–10 year-old boys. Biol. Rhythm Res. 2014, 45, 523–532. [Google Scholar] [CrossRef]
- Teo, W.; Newton, M.J.; McGuigan, M.R. Circadian rhythms in exercise performance: Implications for hormonal and muscular adaptation. J. Sports Sci. Med. 2011, 10, 600–606. [Google Scholar]
- Xu, S.; Akioma, M.; Yuan, Z. Relationship between circadian rhythm and brain cognitive functions. Front. Optoelectron. 2021, 14, 278–287. [Google Scholar] [CrossRef]
- Sato, S.; Basse, A.L.; Schönke, M.; Chen, S.; Samad, M.; Altıntaş, A.; Laker, R.C.; Dalbram, E.; Barrès, R.; Baldi, P.; et al. Time of exercise specifies the impact on muscle metabolic pathways and systemic energy homeostasis. Cell Metab. 2019, 30, 92–110.e4. [Google Scholar] [CrossRef]
- Wheeler, M.J.; Green, D.J.; Ellis, K.A.; Cerin, E.; Heinonen, I.; Naylor, L.H.; Larsen, R.; Wennberg, P.; Boraxbekk, C.J.; Lewis, J.; et al. Distinct effects of acute exercise and breaks in sitting on working memory and executive function in older adults: A three-arm, randomised cross-over trial to evaluate the effects of exercise with and without breaks in sitting on cognition. Br. J. Sports Med. 2020, 54, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Pahwa, A.R.; Miller, D.J.; Caplan, J.B.; Collins, D.F. Performance on an associative memory test decreases 8 hr after cardiovascular exercise. J. Sport Exerc. Psychol. 2020, 42, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Haitani, T.; Tanaka, F.; Yamagishi, T.; Kawakami, Y.; Shibata, S.; Kumano, H. Effects of the time-of-day (morning vs. afternoon) of implementing a combined physical and cognitive exercise program on cognitive functions and mood of older adults: A randomized controlled study. Adv. Gerontol. Uspekhi Gerontol. 2020, 33, 595–599. [Google Scholar] [CrossRef]
- Facer-Childs, E.R.; Boiling, S.; Balanos, G.M. The effects of time of day and chronotype on cognitive and physical performance in healthy volunteers. Sports Med. Open 2018, 4, 47. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Bakker, A.; Cai, J.; English, L.; Kaiser, G.; Mesa, V.; Van Dooren, W. Beyond small, medium, or large: Points of consideration when interpreting effect sizes. Educ. Stud. Math. 2019, 102, 1–8. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrance Erlbaum Associates, Publishers: New York, NY, USA, 1988. [Google Scholar]
- Abraham, W.T.; Russell, D.W. Statistical power analysis in psychological research. Soc. Personal. Psychol. Compass 2008, 2, 283–301. [Google Scholar] [CrossRef]
- Kokkinos, P.F.; Giannelou, A.; Manolis, A.; Pittaras, A. Physical activity in the prevention and management of high blood Pressure. Hell. J. Cardiol. 2009, 50, 52–59. [Google Scholar]
- Whelton, P.K.; Carey, R.M. The 2017 american college of cardiology/ american heart association clinical practice guideline for high blood pressure in adults. JAMA Cardiol. 2018, 3, 352–353. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.M.; Monteiro, C.P.; Rando, B. The impact of action observation on the intention for action engagement. Int. J. Sport Exerc. Psychol. 2022, 1–18. [Google Scholar] [CrossRef]
- Úbeda-Colomer, J.; Monforte, J.; Devís-Devís, J. Physical activity of university students with disabilities: Accomplishment of recommendations and differences by age, sex, disability and weight status. Public Health 2019, 166, 69–78. [Google Scholar] [CrossRef] [PubMed]
- World MedicaL Association Helsinki. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Booth, M. Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 2000, 71, 114–120. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–11. [Google Scholar]
- Bangsbo, J.; Iaia, F.M.; Krustrup, P. The yoyo intermittent recovery test: A useful tool for evaluation of physical performance in intermittent sports. Sport. Med. 2008, 38, 37–51. [Google Scholar] [CrossRef]
- Castillo, D.; Raya-González, J.; Sarmento, H.; Clemente, F.M.; Yanci, J. Effects of including endurance and speed sessions within small-sided soccer games periodization on physical fitness. Biol. Sport 2021, 38, 291–299. [Google Scholar] [CrossRef]
- Brickenkamp, R. d2 Teste de Atenção; Hogrefe Publishing: Göttingen, Germany, 2007; pp. 11–112. [Google Scholar]
- Williams, N. Borg rating of perceived exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef]
- Lavelle, G.; Noorkoiv, M.; Theis, N.; Korff, T.; Kilbride, C.; Baltzopoulos, V.; Shortland, A.; Levin, W.; Ryan, J.M. Validity of the international physical activity questionnaire short form (ipaq-sf) as a measure of physical activity (pa) in young people with cerebral palsy: A cross-sectional study. Physiotherapy 2020, 107, 209–215. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Expert Rev. Cardiovasc. Ther. 2019, 17, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Aamot, I.L.; Forbord, S.H.; Karlsen, T.; Støylen, A. Does rating of perceived exertion result in target exercise intensity during interval training in cardiac rehabilitation? A study of the borg scale versus a heart rate monitor. J. Sci. Med. Sport 2014, 17, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Cabral, L.L.; Nakamura, F.Y.; Stefanello, J.M.F.; Pessoa, L.C.V.; Smirmaul, B.P.C.; Pereira, G. Initial validity and reliability of the portuguese borg rating of perceived exertion 6–20 scale. Meas. Phys. Educ. Exerc. Sci. 2020, 24, 103–114. [Google Scholar] [CrossRef]
- Guidetti, L.; Sgadari, A.; Buzzachera, C.F.; Broccatelli, M.; Utter, A.C.; Goss, F.L.; Baldari, C. Validation of the omni-cycle scale of perceived exertion in the elderly. J. Aging Phys. Act. 2011, 19, 214–224. [Google Scholar] [CrossRef]
- Pageaux, B. Perception of effort in exercise science: Definition, measurement and perspectives. Eur. J. Sport Sci. 2016, 16, 885–894. [Google Scholar] [CrossRef]
- Moore, R.D.; Romine, M.W.; O’Connor, P.J.; Tomporowski, P.D. The influence of exercise-induced fatigue on cognitive function. J. Sports Sci. 2012, 30, 841–850. [Google Scholar] [CrossRef]
- Fery, Y.A.; Ferry, A.; Hope, A.V.; Rieu, M. Effect of physical exhaustion on cognitive functioning. Percept. Mot. Skills 1997, 84, 291–298. [Google Scholar] [CrossRef]
- Brickenkamp, R.; Zilmer, E. D2–Test of Attention; Hogrefe & Huber Publishers: Göttingen, Germany, 1998. [Google Scholar]
- Lindemann-Matthies, P.; Benkowitz, D.; Hellinger, F. Associations between the naturalness of window and interior classroom views, subjective well-being of primary school children and their performance in an attention and concentration test. Landsc. Urban Plan. 2021, 214, 104146. [Google Scholar] [CrossRef]
- Lozano, J.H.; Capote, E.; Fernández, M.P. Convergent validity of the measures of attention and impulsivity in the trees: Simple visual discrimination test (divisa-uam). An. de Psicol. 2015, 31, 74–83. [Google Scholar] [CrossRef]
- Spitzer, U.S.; Hollmann, W. Experimental observations of the effects of physical exercise on attention, academic and prosocial performance in school settings. Trends Neurosci. Educ. 2013, 2, 1–6. [Google Scholar] [CrossRef]
- Tilp, M.; Scharf, C.; Payer, G.; Presker, M.; Fink, A. Physical exercise during the morning school-break improves basic cognitive functions. Mind Brain Educ. 2020, 14, 24–31. [Google Scholar] [CrossRef]
- García, G.C.; Secchi, J.D. Test course navette de 20metros con etapas de un minuto. Una idea original que perdura hace 30 años. Apunt. Med. l’Esport 2014, 49, 93–103. [Google Scholar] [CrossRef]
- Krustrup, P.; Mohr, M.; Amstrup, T.; Rysgaard, T.; Johansen, J.; Steensberg, A.; Pedersen, P.K.; Bangsbo, J. The yo-yo intermittent recovery test: Physiological response, reliability, and validity. Med. Sci. Sports Exerc. 2003, 35, 697–705. [Google Scholar] [CrossRef]
- Higino, W.P. Fatores Determinantes no Desempenho do TesteYyo-yo Intermitente Recuperativo Nível 1 (YYIR1); Universidade de São Paulo: São Paulo, Brazil, 2013. [Google Scholar]
- Bagchi, A.; Nimkar, N.; Yeravdekar, R. Development of norms for cardiovascular endurance test for youth aged 18–25 years. Indian J. Public Health Res. Dev. 2019, 10, 1486–1491. [Google Scholar] [CrossRef]
- Eskandarifard, E.; Silva, R.; Nobari, H.; Clemente, F.M.; Pérez-Gómez, J.; Figueiredo, A.J. Maturational effect on physical capacities and anabolic hormones in under-16 elite footballers: A cross-sectional study. Sport Sci. Health 2022, 18, 297–305. [Google Scholar] [CrossRef]
- Sapolsky, R.M.; Romero, L.M.; Munck, A.U. How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocr. Rev. 2000, 21, 55–89. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Rampinini, E.; Maffiuletti, N.A.; Castagna, C.; Bizzini, M.; Wisløff, U. Effects of aerobic training on the exercise-induced decline in short-passing ability in junior soccer players. Appl. Physiol. Nutr. Metab. 2008, 33, 1192–1198. [Google Scholar] [CrossRef]
- Aloui, K.; Abedelmalek, S.; Chtourou, H.; Wong, D.P.; Boussetta, N.; Souissi, N. Effects of time-of-day on oxidative stress, cardiovascular parameters, biochemical markers, and hormonal response following level-1 yo-yo intermittent recovery test. Physiol. Int. 2017, 104, 77–90. [Google Scholar] [CrossRef]
- Chen, Y.S.; Liao, C.J.; Lu, W.A.; Kuo, C.D. Sympathetic enhancement in futsal players but not in football players after repeated sprint ability test. BMJ Open Sport Exerc. Med. 2015, 1, 1–10. [Google Scholar] [CrossRef]
- Ferrari Bravo, D.; Impellizzeri, F.M.; Rampinini, E.; Castagna, C.; Bishop, D.; Wisloff, U. Sprint vs. Interval training in football. Int. J. Sports Med. 2008, 29, 668–674. [Google Scholar] [CrossRef]
- Oliveira, R.S.; Leicht, A.S.; Bishop, D.; Barbero-Álvarez, J.C.; Nakamura, F.Y. Seasonal changes in physical performance and heart rate variability in high level futsal players. Int. J. Sports Med. 2013, 34, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Castagna, C.; Krustrup, P.; Póvoas, S. Yo-Yo intermittent tests are a valid tool for aerobic fitness assessment in recreational football. Eur. J. Appl. Physiol. 2020, 120, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Geertsen, S.S.; Thomas, R.; Larsen, M.N.; Dahn, I.M.; Andersen, J.N.; Krause-Jensen, M.; Korup, V.; Nielsen, C.M.; Wienecke, J.; Ritz, C.; et al. Motor skills and exercise capacity are associated with objective measures of cognitive functions and academic performance in preadolescent children. PLoS ONE 2016, 11, e0161960. [Google Scholar] [CrossRef] [PubMed]
- Mazzoccante, R.; Corrêa, H.; Sousa, I.; Ramos, I.; Melo, G. The relationship between the number of weekly physical education classes with morphological, physical, motor and executive functions profiles: A cross-sectional study physical education class morphological, physical, motor and executive functions. Cuad. Psicol. del Deport. 2022, 22, 171–185. [Google Scholar] [CrossRef]
- Mazzoccante, R.P.; De Luca Corrêa, H.; De Santana, F.S.; Câmara, M.A.; De Sousa, B.R.C.; De Sousa, I.R.C.; Ferreira, A.P.; De Melo, G.F. Attention and executive function are predicted by anthropometric indicators, strength, motor performance, and aerobic fitness in children aged 6–10 years. Hum. Mov. 2020, 21, 40–48. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular effects and benefits of exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef]
- Zhou, S.; Chen, S.; Liu, X.; Zhang, Y.; Zhao, M.; Li, W. Physical activity improves cognition and activities of daily living in adults with alzheimer’s disease: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2022, 19, 1216. [Google Scholar] [CrossRef]
- Anders, J.P.V.; Kraemer, W.J.; Newton, R.U.; Post, E.M. Acute effects of high-intensity resistance exercise on cognitive function. J. Sports Sci. Med. 2021, 20, 391–397. [Google Scholar] [CrossRef]
- Chang, H.; Kim, K.; Jung, Y.-J.; Kato, M. Effects of acute high-intensity resistance exercise on cognitive function and oxygenation in prefrontal cortex. J. Exerc. Nutr. Biochem. 2017, 21, 1–8. [Google Scholar] [CrossRef]
- Jarraya, S.; Jarraya, M.; Chtourou, H.; Souissi, N. Diurnal Variations on cognitive performances in handball goalkeepers. Biol. Rhythm Res. 2014, 45, 93–101. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | ||||||
|---|---|---|---|---|---|---|
| Morning (n = 27) | Afternoon (n = 29) | |||||
| Freq | % | Freq | % | |||
| Gender | Female | 15 | 55.6% | 20 | 69.0% | X2 = 1.073 p = 0.300 |
| Male | 12 | 44.4% | 9 | 31.0% | ||
| Age | 18–32 23.37 ± 4.09 | 17–33 21.93 ± 3.33 | t = 1.446 p = 0.154 | |||
| IPAQ MET_minWeek | 340.00–2754.00 1460.13 ± 493.48 | 325.00–2807.50 1228.00 ± 602.33 | t = 1.571 p = 0.122 | |||
| Group | n | Mean | Std. Deviation | Independent Sample t-Test | |
|---|---|---|---|---|---|
| Gen_PerformT1-T0 | Morning | 27 | 47.74 | 110.95 | t = −0.546 p = 0.587 |
| Afternoon | 29 | 63.07 | 99.05 | ||
| Gen_PerformT2-T1 | Morning | 27 | 34.33 | 109.07 | t = 0.137 p = 0.891 |
| Afternoon | 29 | 30.93 | 74.07 | ||
| Gen_PerformT2-T0 | Morning | 27 | 82.07 | 103.69 | t = −0.492 p = 0.625 |
| Afternoon | 29 | 94.00 | 76.43 | ||
| Conc_IndexT1-T0 | Morning | 27 | 30.30 | 73.38 | t = −0.190 p = 0.850 |
| Afternoon | 29 | 33.93 | 69.90 | ||
| Conc_IndexT2-T1 | Morning | 27 | 29.56 | 51.31 | t = −0.681 p = 0.499 |
| Afternoon | 29 | 19.90 | 54.61 | ||
| Conc_IndexT2-T0 | Morning | 27 | 59.85 | 83.88 | t = 0.326 p = 0.746 |
| Afternoon | 29 | 53.83 | 48.68 | ||
| Erro%_T1-T0 | Morning | 27 | −7.67 | 21.88 | t = 0.839 p = 0.405 |
| Afternoon | 29 | −18.60 | 64.29 | ||
| Error%_T2-T1 | Morning | 27 | −3.26 | 8.00 | t = −0.904 p = 0.370 |
| Afternoon | 29 | −1.01 | 10.37 | ||
| Error%_T2-T0 | Morning | 27 | −10.93 | 20.51 | t = 0.679 p = 0.500 |
| Afternoon | 29 | −19.61 | 63.41 | ||
| Variation_IndexT1-T0 | Morning | 27 | −5.70 | 15.62 | t = −0.277 p = 0.783 |
| Afternoon | 29 | −4.66 | 12.64 | ||
| Variation_IndexT2-T1 | Morning | 27 | −1.70 | 15.27 | t = 0.151 p = 0.880 |
| Afternoon | 29 | −2.24 | 11.18 | ||
| Variation_IndexT2-T0 | Morning | 27 | −7.41 | 14.93 | t = −0.150 p = 0.881 |
| Afternoon | 29 | −6.90 | 10.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maeneja, R.; Ferreira, I.S.; Silva, C.R.; Abreu, A.M. Cognitive Benefits of Exercise: Is There a Time-of-Day Effect? Healthcare 2022, 10, 1766. https://doi.org/10.3390/healthcare10091766
Maeneja R, Ferreira IS, Silva CR, Abreu AM. Cognitive Benefits of Exercise: Is There a Time-of-Day Effect? Healthcare. 2022; 10(9):1766. https://doi.org/10.3390/healthcare10091766
Chicago/Turabian StyleMaeneja, Reinaldo, Inês S. Ferreira, Cláudia R. Silva, and Ana Maria Abreu. 2022. "Cognitive Benefits of Exercise: Is There a Time-of-Day Effect?" Healthcare 10, no. 9: 1766. https://doi.org/10.3390/healthcare10091766