



Comparison of Digital Interactive Case-Based Educational Resource with Virtual Role Play in Dental Undergraduates in Clinical Oral Medicine/Oral Pathology Education

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of Case Scenarios
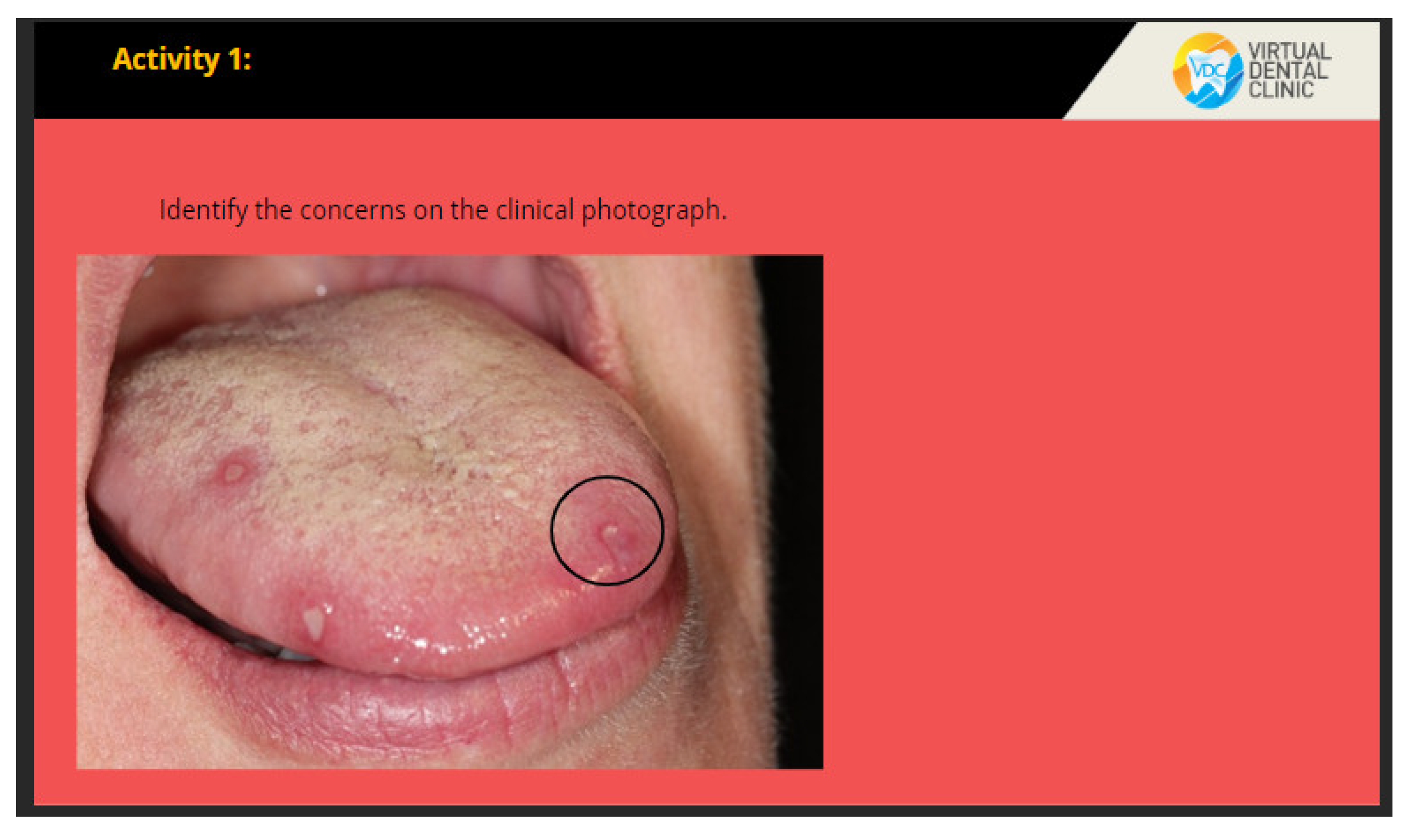
2.3. Virtual Oral Medicine Clinic (VOMC)
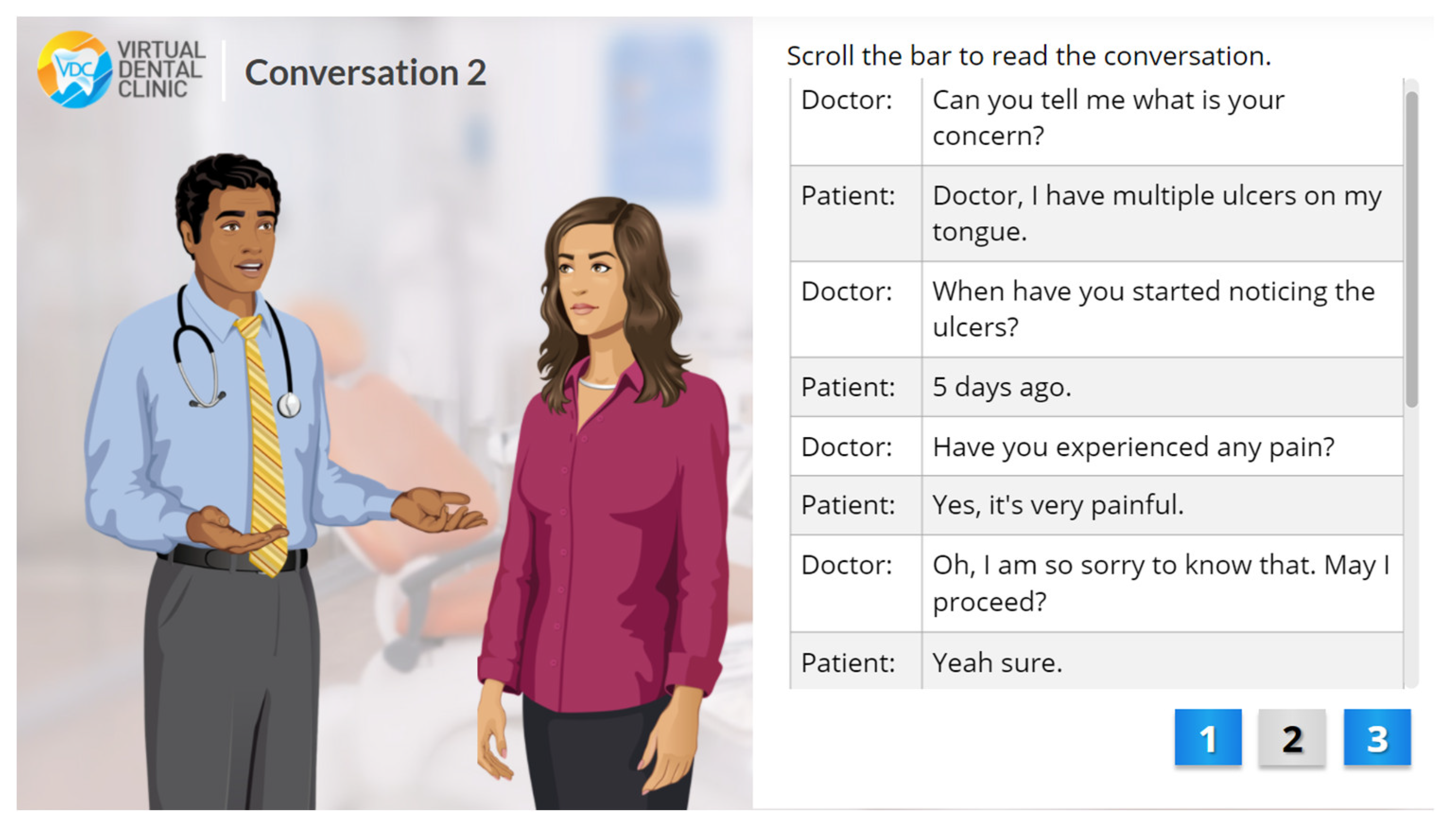
2.4. Virtual Role Play Activity
2.5. Learning Evaluation
2.6. Student’s Feedback
2.6.1. Online Questionnaire
2.6.2. Focus Group Discussion
2.7. Data Analysis
3. Results
3.1. Learning Evaluation
3.2. Student’s Feedback
3.2.1. Feedback Questionnaire
3.2.2. Focus Group Discussion
- (1) flexibility, (2) organization of content, (3) interactivity, and (4) element of personalization.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pokhrel, S.; Chhetri, R. A Literature Review on Impact of COVID-19 Pandemic on Teaching and Learning. High Educ. Future 2021, 8, 133–141. [Google Scholar] [CrossRef]
- Car, J.; Carlstedt-Duke, J.; Tudor Car, L.; Posadzki, P.; Whiting, P.; Zary, N.; Digital Health Education Collaboration. Digital education in health professions: The need for overarching evidence synthesis. J. Med. Internet Res. 2019, 21, e12913. [Google Scholar] [CrossRef] [PubMed]
- Moazami, F.; Bahrampour, E.; Azar, M.R.; Jahedi, F.; Moattari, M. Comparing two methods of education (virtual versus traditional) on learning of Iranian dental students: A post-test only design study. BMC Med. Educ. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.; Schmidt, A.; Wöstmann, B.; Krämer, N.; Schulz-Weidner, N. Students’ and lecturers’ perspective on the implementation of online learning in dental education due to SARS-CoV-2 (COVID-19): A cross-sectional study. BMC Med. Educ. 2020, 20, 354. [Google Scholar] [CrossRef]
- Zary, N.; Johnson, G.; Boberg, J.; Fors, U.G. Development, implementation and pilot evaluation of a Web-based Virtual Patient Case Simulation environment—Web-SP. BMC Med Educ. 2006, 6, 10. [Google Scholar] [CrossRef]
- Eagles, J.M.; Calder, S.A.; Nicoll, K.S.; Sclare, P.D. Using simulated patients in education about alcohol misuse. Acad. Med. 2001, 76, 395–410. [Google Scholar] [CrossRef]
- Gordon, J.A.; Wilkerson, W.M.; Shaffer, D.W.; Armstrong, E.G. “Practicing” medicine without risk: Students’ and educators’ responses to high-fidelity patient simulation. Acad. Med. 2001, 76, 469–472. [Google Scholar] [CrossRef]
- Eshach, H.; Bitterman, H. From case-based reasoning to problem-based learning. Acad. Med. 2003, 78, 491–496. [Google Scholar] [CrossRef]
- Norman, G. Research in clinical reasoning: Past history and current trends. Med. Educ. 2005, 39, 418–427. [Google Scholar] [CrossRef]
- Wu, Y.-J.A.; Lan, Y.-J.; Huang, S.-B.P.; Lin, Y.-T.R. Enhancing Medical Students’ Communicative Skills in a 3D Virtual World. J. Educ. Techno. Soc. 2019, 22, 18–32. [Google Scholar]
- Vuchkova, J.; Maybury, T.; Farah, C. Digital interactive learning of oral radiographic anatomy. Eur. J. Dent. Educ. 2011, 16, e79–e87. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.C.; Anderson, O.R.; Lal, S. Assessment of a Novel Module for Training Dental Students in Child Abuse Recognition and Reporting. J. Dent. Educ. 2014, 78, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Soltanimehr, E.; Bahrampour, E.; Imani, M.M.; Rahimi, F.; Almasi, B.; Moattari, M. Effect of virtual versus traditional education on theoretical knowledge and reporting skills of dental students in radiographic interpretation of bony lesions of the jaw. BMC Med. Educ. 2019, 19, 233. [Google Scholar] [CrossRef]
- Hakami, Z. Comparison between Virtual and Traditional Learning Methods for Orthodontic Knowledge and Skills in Dental Students: A Quasi-Experimental Study. Healthcare 2021, 9, 1092. [Google Scholar] [CrossRef]
- Aly, M.; Elen, J.; Willems, G. Instructional Multimedia Program versus Standard Lecture: A Comparison of Two Methods for Teaching the Undergraduate Orthodontic Curriculum. Eur. J. Dent. Educ. 2004, 8, 43–46. [Google Scholar] [CrossRef]
- Bains, M.; Reynolds, P.A.; McDonald, F.; Sherriff, M. Effectiveness and Acceptability of Face-to-Face, Blended and e-Learning: A Randomised Trial of Orthodontic Undergraduates. Eur. J. Dent. Educ. 2011, 15, 110–117. [Google Scholar] [CrossRef]
- Menon, R.K.; Seow, L.L. Development of an Online Asynchronous Clinical Learning Resource (“Ask the Expert”) in Dental Education to Promote Personalized Learning. Healthcare 2021, 9, 1420. [Google Scholar] [CrossRef]
- Omar, H.; Khan, S.; Toh, C. Structured student-generated videos for first-year students at a dental school in malaysia. J. Dent. Educ. 2013, 77, 640–647. [Google Scholar] [CrossRef]
- Ayn, C.; Robinson, L.; Nason, A.; Lovas, J. Determining recommendations for improvement of communication skills training in dental education: A scoping review. J. Dent. Educ. 2017, 81, 479–488. [Google Scholar] [CrossRef]
- Agboola Sogunro, O. Efficacy of role-playing pedagogy in training leaders: Some reflections. J. Manag. Dev. 2004, 23, 355–371. [Google Scholar] [CrossRef]
- Kasabah, S.; Reddy, P.; Kashyap, B. Role plays a teaching strategy for dental students: An institutional study. Int. J. Adv. Appl. 2016, 3, 31–35. [Google Scholar] [CrossRef]
- Al-Khalifa, K.S.; Nazir, M.A. Evaluation of dental students’ responses to roleplay videos in a professionalism course. J. Taibah Univ. Med. Sci. 2020, 15, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Zepke, N.; Leach, L. Improving student engagement: Ten proposals for action. Act. Learn. High. Educ. 2010, 11, 167–189. [Google Scholar] [CrossRef]
- Mazor, K.M.; Zanetti, M.L.; Alper, E.J.; Hatem, D.; Barrett, S.V.; Meterko, V.; Gammon, W.; Pugnaire, M.P. Assessing professionalism in the context of an objective structured clinical examination: An in-depth study of the rating process. Med. Educ. 2007, 41, 331–340. [Google Scholar] [CrossRef]
- Purwono, U.; Carline, M.; Barrett, S.; Alper, J.; Gammon, W.; Pugnaire, M. Assessing Professionalism Using the Objective Structured Clinical Exam. Division of Research & Evaluation 2003; Paper 13. Available online: http://escholarship.umassed.edu/res_eval/13 (accessed on 22 June 2022).
- Rasul, S.; Zahid Bashir, M.; Saleem, S.; Tahir, S.; Rasheed, A.; Ali Sabir, M. Assessment of Medical Professionalism among Students and Faculty Members of Shalamar Medical and Dental College, Lahore. J. Adv. Med. Educ. Prof. 2021, 9, 204–210. [Google Scholar]
- Cruess, S.R.; Cruess, R.L. Understanding medical professionalism: A plea for an inclusive and integrated approach. Med. Educ. 2008, 42, 755–757. [Google Scholar] [CrossRef]
- Yu, Z. The effects of gender, educational level, and personality on online learning outcomes during the COVID-19 pandemic. Int. J. Educ. Technol. High Educ. 2021, 18, 14. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control (n = 27) | Experimental (n = 24) | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | ||
| Professionalism and Patient Safety | Pre-Test | 17.30 | 3.036 | <0.001 | 17.83 | 3.130 | <0.001 |
| Post-Test | 19.81 | 3.465 | 23.17 | 2.444 | |||
| Communication Skills | Pre-Test | 15.00 | 3.113 | <0.001 | 16.54 | 2.553 | <0.001 |
| Post-Test | 20.48 | 2.779 | 23.08 | 2.185 | |||
| Diagnostic Skills | Pre-Test | 14.89 | 3.309 | <0.001 | 15.83 | 3.002 | <0.001 |
| Post-Test | 20.63 | 2.290 | 21.96 | 2.053 | |||
| Clinical Management (Decision making) | Pre-Test | 14.33 | 3.174 | <0.001 | 15.08 | 2.339 | <0.001 |
| Post-Test | 19.85 | 2.797 | 21.50 | 1.911 | |||
| Total | Pre-Test | 61.52 | 10.885 | <0.001 | 65.29 | 8.508 | <0.001 |
| Post-Test | 80.78 | 9.521 | 89.71 | 6.517 | |||
| Pre-Test (51) | Post-Test (51) | ||||||
|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | ||
| Professionalism and Patient Safety | Control | 17.30 | 3.036 | 0.456 | 19.81 | 3.465 | <0.001 |
| Experimental | 17.83 | 3.130 | 23.17 | 2.444 | |||
| Communication Skills | Control | 15.00 | 3.113 | 0.019 | 20.48 | 2.779 | 0.001 |
| Experimental | 16.54 | 2.553 | 23.08 | 2.185 | |||
| Diagnostic Skills | Control | 14.89 | 3.309 | 0.216 | 20.63 | 2.290 | 0.027 |
| Experimental | 15.83 | 3.002 | 21.96 | 2.053 | |||
| Clinical Management (Decision making) | Control | 14.33 | 3.174 | 0.209 | 19.85 | 2.797 | 0.045 |
| Experimental | 15.08 | 2.339 | 21.50 | 1.911 | |||
| Total | Control | 61.52 | 10.885 | 0.091 | 80.78 | 9.521 | <0.001 |
| Experimental | 65.29 | 8.508 | 89.71 | 6.517 | |||
| Question: I Think to Role-Play Activity No of Respondents (27) | Mean (SD) | Strongly Agree (%) | Agree (%) | Disagree (%) | Strongly Disagree (%) | Overall Agreement (%) |
|---|---|---|---|---|---|---|
| Diagnostic Skills | ||||||
1. improves my diagnostic skills in Oral Medicine | 3.8(0.4) | 76.5 | 23.5 | 0 | 0 | 100 |
2. helps me to interpret variations in clinical presentation of oromucosal lesions/conditions | 3.7(0.5) | 70.6 | 29.4 | 0 | 0 | 100 |
3. helps me to diagnose oromucosal lesions/conditions | 3.7(0.5) | 70.6 | 29.4 | 0 | 0 | 100 |
4. helps me to formulate appropriate management plan for patients having oromucosal lesions/conditions | 3.5(0.6) | 52.9 | 41.2 | 5.9 | 0 | 94.1 |
5. makes me more confident in diagnosing oromucosal lesions/conditions without additional help | 3.5(0.6) | 58.8 | 35.3 | 5.9 | 0 | 94.1 |
| Communication Skills | ||||||
6. improves my communication skills with patients having oromucosal lesions/conditions | 3.6(0.5) | 58.8 | 41.2 | 0 | 0 | 100 |
7. makes dentist-patient interaction more interesting | 3.4(0.5) | 41.2 | 58.8 | 0 | 0 | 100 |
8. makes dentist-patient interaction more realistic | 3.5(0.5) | 52.9 | 47.1 | 0 | 0 | 100 |
9. reduces my anxiety when communicating with patients having oromucosal lesions/conditions | 3.5(0.5) | 47.1 | 52.9 | 0 | 0 | 100 |
10. makes me more confident in communicating with patients having oromucosal lesions/conditions without additional help | 3.4(0.6) | 47.1 | 47.1 | 5.9 | 0 | 94.1 |
| Impact on Learning | ||||||
11. positively enhanced learning of diagnostic and communication skills in Oral Medicine | 3.5(0.5) | 52.9 | 47.1 | 0 | 0 | 100 |
12. increases my willingness in learning diagnostic and communication skills in Oral Medicine | 3.5(0.6) | 58.8 | 35.3 | 5.9 | 0 | 94.1 |
13. makes me more concentrated in learning diagnostic and communication skills in Oral Medicine | 3.8(0.4) | 76.5 | 23.5 | 0 | 0 | 100 |
| Question: I think Virtual Oral Medicine Clinic No of Respondents (24) | Mean (SD) | Strongly Agree (%) | Agree (%) | Disagree (%) | Strongly Disagree (%) | Overall Agreement (%) |
|---|---|---|---|---|---|---|
| Diagnostic Skills | ||||||
1. improves my diagnostic skills in Oral Medicine | 3.1(0.6) | 20.0 | 65.0 | 15.0 | 0 | 85.0 |
2. helps me to interpret variations in clinical presentation of oromucosal lesions/conditions | 3.0(0.7) | 35.0 | 50.0 | 25.0 | 0 | 75.0 |
3. helps me to diagnose oromucosal lesions/conditions | 3.2(0.7) | 30.0 | 55.0 | 15.0 | 0 | 85.0 |
4. helps me to formulate appropriate management plan for patients having oromucosal lesions/conditions | 3.1(0.6) | 25.0 | 65.0 | 10.0 | 0 | 90.0 |
5. makes me more confident in diagnosing oromucosal lesions/conditions without additional help | 2.7(0.7) | 5.0 | 60.0 | 30.0 | 5.0 | 65.0 |
| Communication Skills | ||||||
6. improves my communication skills with patients having oromucosal lesions/conditions | 2.9(0.6) | 5.0 | 80.0 | 10.0 | 5.0 | 85.0 |
7. makes dentist-patient interaction more interesting | 2.5(0.6) | 0 | 55.0 | 40.0 | 5.0 | 55.0 |
8. makes dentist-patient interaction more realistic | 2.5(0.8) | 5.0 | 50.0 | 35.0 | 10.0 | 55.0 |
9. reduces my anxiety when communicating with patients having oromucosal lesions/conditions | 2.9(0.7) | 10.0 | 70.0 | 15.0 | 5.0 | 80.0 |
10. makes me more confident in communicating with patients having oromucosal lesions/conditions without additional help | 2.8(0.6) | 5.0 | 70.0 | 20.0 | 5.0 | 75.0 |
| Impact on Learning | ||||||
11. positively enhanced learning of diagnostic and communication skills in Oral Medicine | 3.1(0.5) | 15.0 | 75.0 | 10.0 | 0 | 90.0 |
12. increases my willingness in learning diagnostic and communication skills in Oral Medicine | 3.0(0.6) | 20.0 | 60.0 | 20.0 | 0 | 80.0 |
13. makes me more concentrated in learning diagnostic and communication skills in Oral Medicine | 2.8(0.9) | 20.0 | 40.0 | 35.0 | 5.0 | 60.0 |
| Question: I Think Role-Play Activity/Virtual Oral Medicine Clinic | Group | Mean | SD | p-Value |
|---|---|---|---|---|
| Diagnostic Skills | ||||
1. improves my diagnostic skills in Oral Medicine | Control | 3.76 | 0.437 | <0.001 |
| Experimental | 3.05 | 0.605 | ||
2. helps me to interpret variations in clinical presentation of oromucosal lesions/conditions | Control | 3.71 | 0.470 | 0.003 |
| Experimental | 3.00 | 0.725 | ||
3. helps me to diagnose oromucosal lesions/conditions | Control | 3.71 | 0.470 | 0.009 |
| Experimental | 3.15 | 0.671 | ||
4. helps me to formulate appropriate management plan for patients having oromucosal lesions/conditions | Control | 3.47 | 0.624 | 0.099 |
| Experimental | 3.15 | 0.587 | ||
5. makes me more confident in diagnosing oromucosal lesions/conditions without additional help | Control | 3.53 | 0.624 | <0.001 |
| Experimental | 2.65 | 0.671 | ||
| Total | Control | 18.18 | 2.351 | 0.001 |
| Experimental | 15.00 | 2.555 | ||
| Communication Skills | ||||
6. improves my communication skills with patients having oromucosal lesions/conditions | Control | 3.59 | 0.507 | <0.001 |
| Experimental | 2.85 | 0.587 | ||
7. makes dentist-patient interaction more interesting | Control | 3.41 | 0.507 | <0.001 |
| Experimental | 2.50 | 0.607 | ||
8. makes dentist-patient interaction more realistic | Control | 3.53 | 0.514 | <0.001 |
| Experimental | 2.50 | 0761 | ||
9. reduces my anxiety when communicating with patients having oromucosal lesions/conditions | Control | 3.47 | 0.514 | 0.004 |
| Experimental | 2.85 | 0.671 | ||
10. makes me more confident in communicating with patients having oromucosal lesions/conditions without additional help | Control | 3.41 | 0.618 | 0.003 |
| Experimental | 2.75 | 0.639 | ||
| Total | Control | 17.41 | 2.373 | 0.000 |
| Experimental | 15.00 | 2.625 | ||
| Impact on Learning | ||||
11. positively enhanced learning of diagnostic and communication skills in Oral Medicine | Control | 3.53 | 0.514 | 0.010 |
| Experimental | 3.05 | 0.510 | ||
12. increases my willingness in learning diagnostic and communication skills in Oral Medicine | Control | 3.53 | 0.624 | 0.016 |
| Experimental | 3.00 | 0.649 | ||
13. makes me more concentrated in learning diagnostic and communication skills in Oral Medicine | Control | 3.76 | 0.437 | <0.001 |
| Experimental | 2.75 | 0.851 | ||
| Total | Control | 10.82 | 1.286 | 0.001 |
| Experimental | 8.80 | 1.824 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tee, W.X.; Tan, S.H.; Marican, F.; Sidhu, P.; Yerebairapura Math, S.; Gopinath, D. Comparison of Digital Interactive Case-Based Educational Resource with Virtual Role Play in Dental Undergraduates in Clinical Oral Medicine/Oral Pathology Education. Healthcare 2022, 10, 1767. https://doi.org/10.3390/healthcare10091767
Tee WX, Tan SH, Marican F, Sidhu P, Yerebairapura Math S, Gopinath D. Comparison of Digital Interactive Case-Based Educational Resource with Virtual Role Play in Dental Undergraduates in Clinical Oral Medicine/Oral Pathology Education. Healthcare. 2022; 10(9):1767. https://doi.org/10.3390/healthcare10091767
Chicago/Turabian StyleTee, Wen Xi, Siew Huey Tan, Fareeza Marican, Preena Sidhu, Swarna Yerebairapura Math, and Divya Gopinath. 2022. "Comparison of Digital Interactive Case-Based Educational Resource with Virtual Role Play in Dental Undergraduates in Clinical Oral Medicine/Oral Pathology Education" Healthcare 10, no. 9: 1767. https://doi.org/10.3390/healthcare10091767