
Pericapsular Nerve Group Block and Iliopsoas Plane Block: A Scoping Review of Quadriceps Weakness after Two Proclaimed Motor-Sparing Hip Blocks

 , , ,
, , ,
Abstract
:1. Introduction
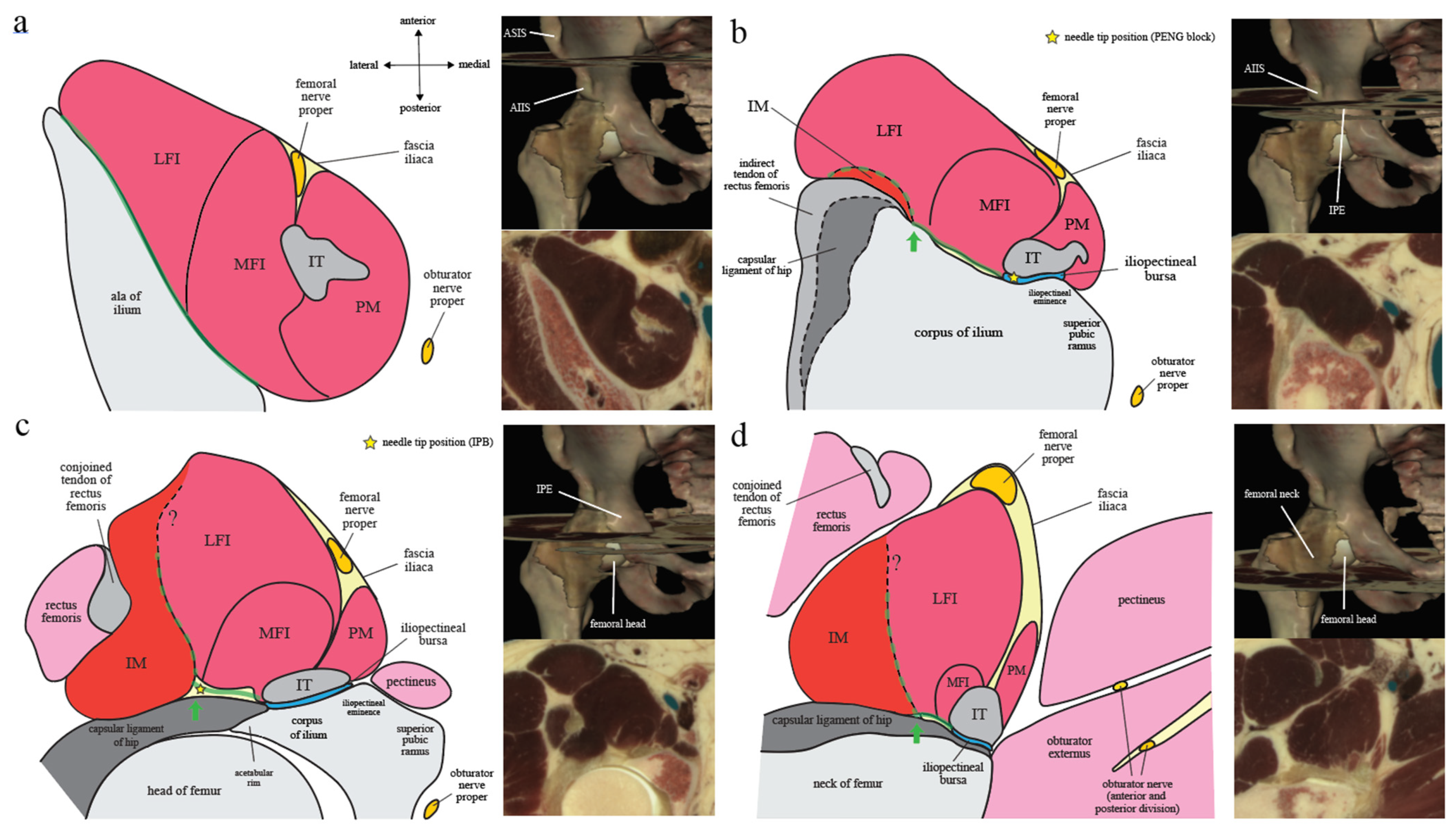
2. Applied Anatomy
2.1. Iliopsoas Complex
2.2. Iliopectineal Bursa
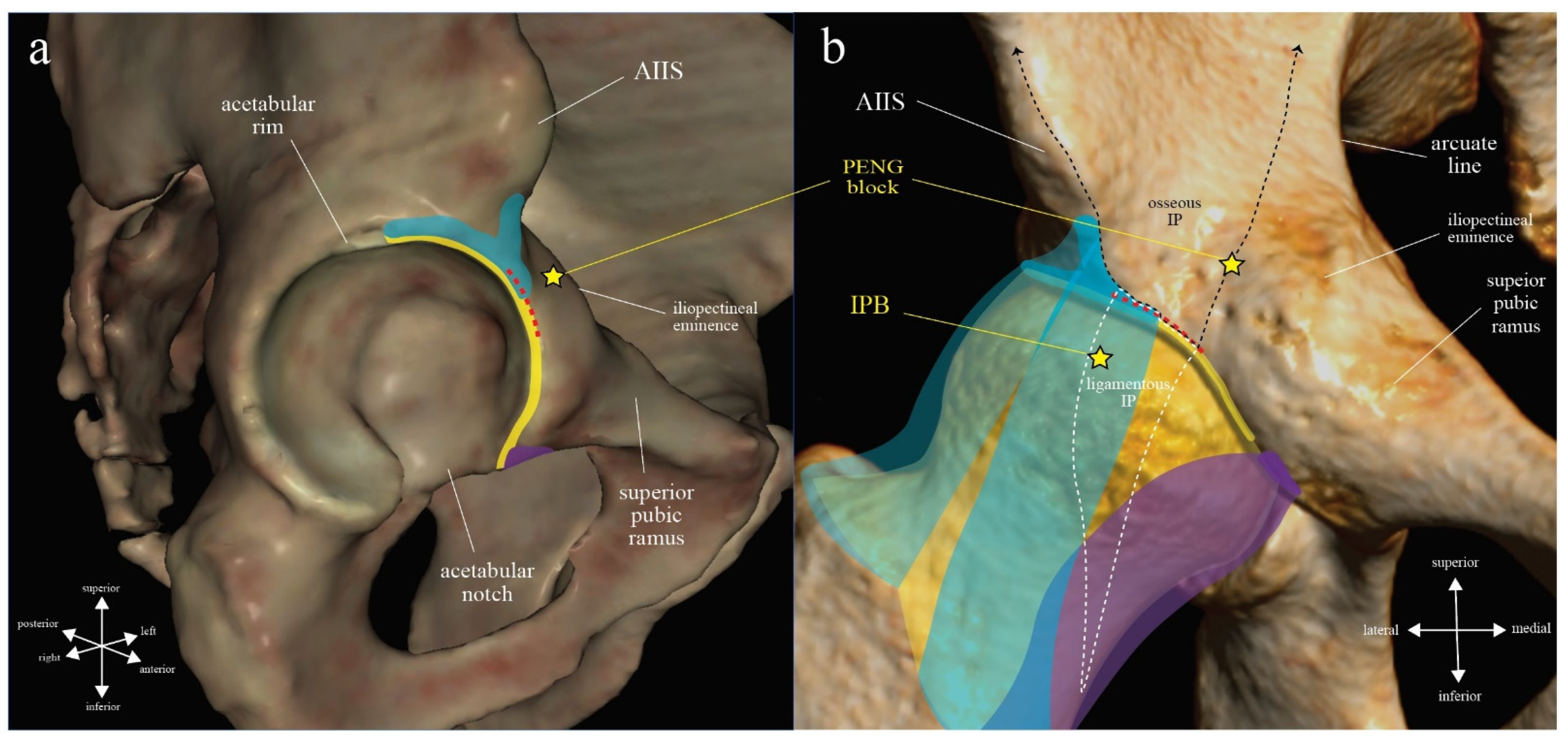
2.3. Iliopsoas Plane
2.3.1. Iliopectineal Eminence
2.3.2. Capsular Ligaments of Hip: Iliofemoral Ligament
2.3.3. Iliopsoas Plane (IP): Osseous, Ligamentous, and Muscular
2.4. Fascia Iliaca Compartment (FIC) and Subpectineal Plane (SP)
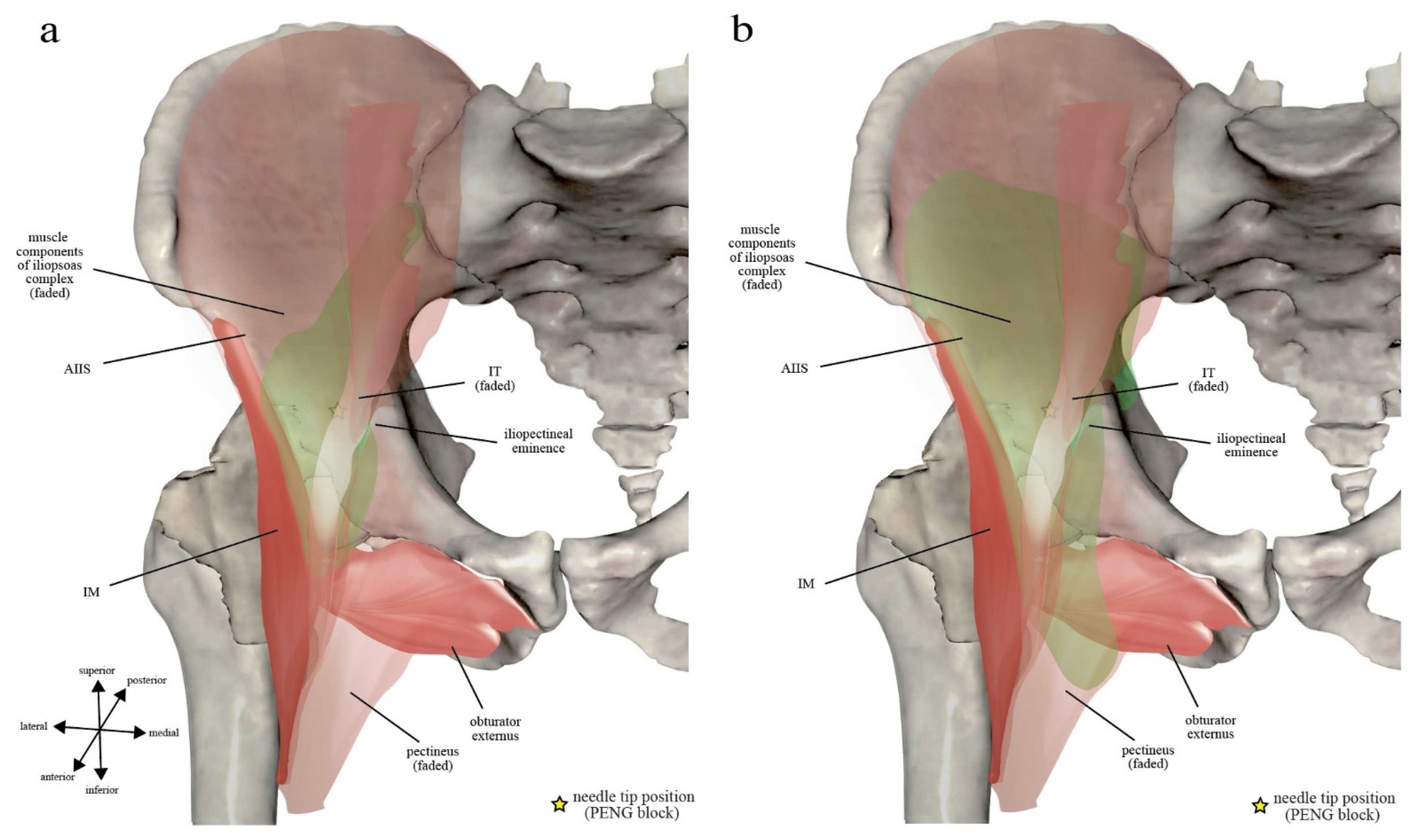
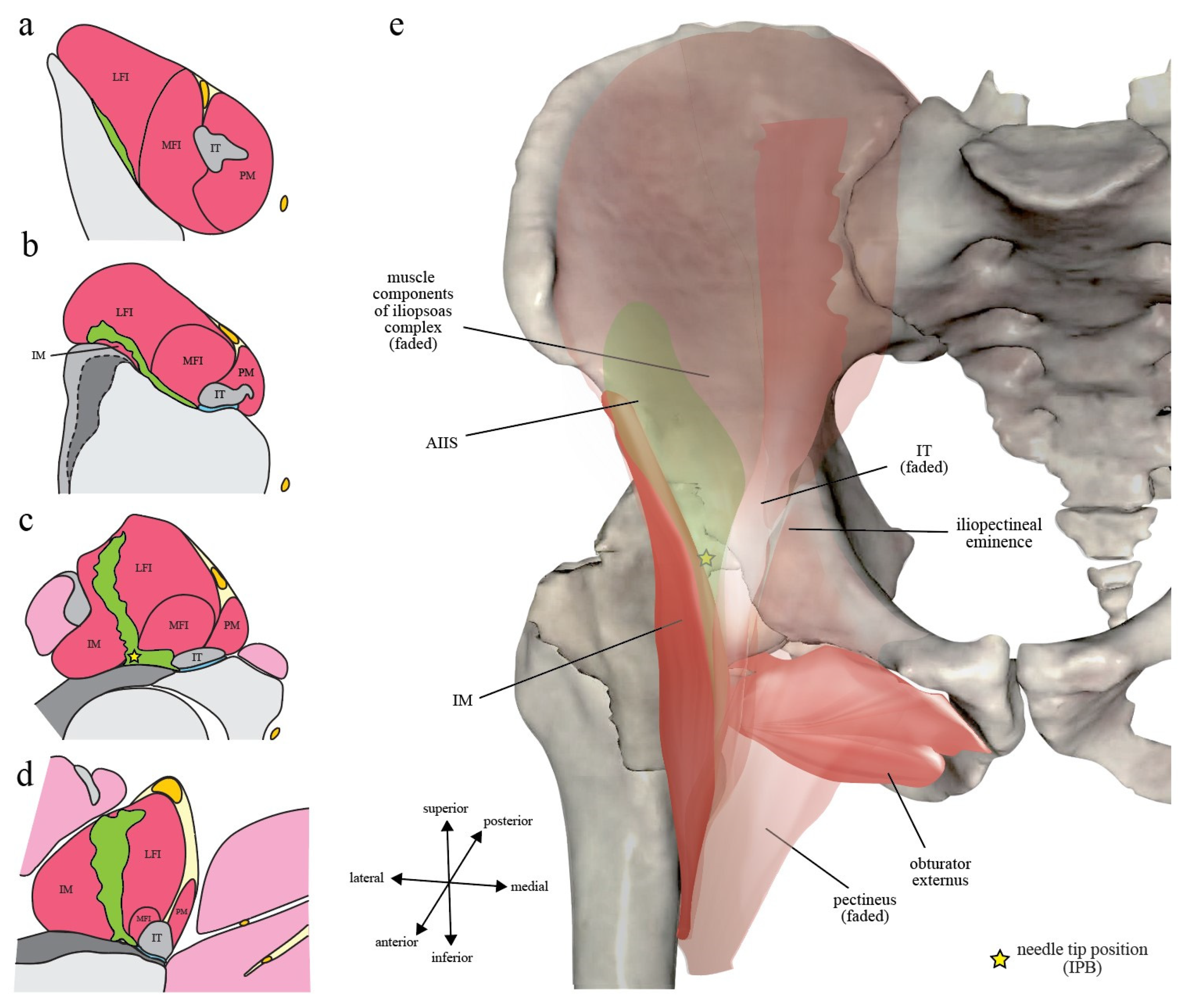
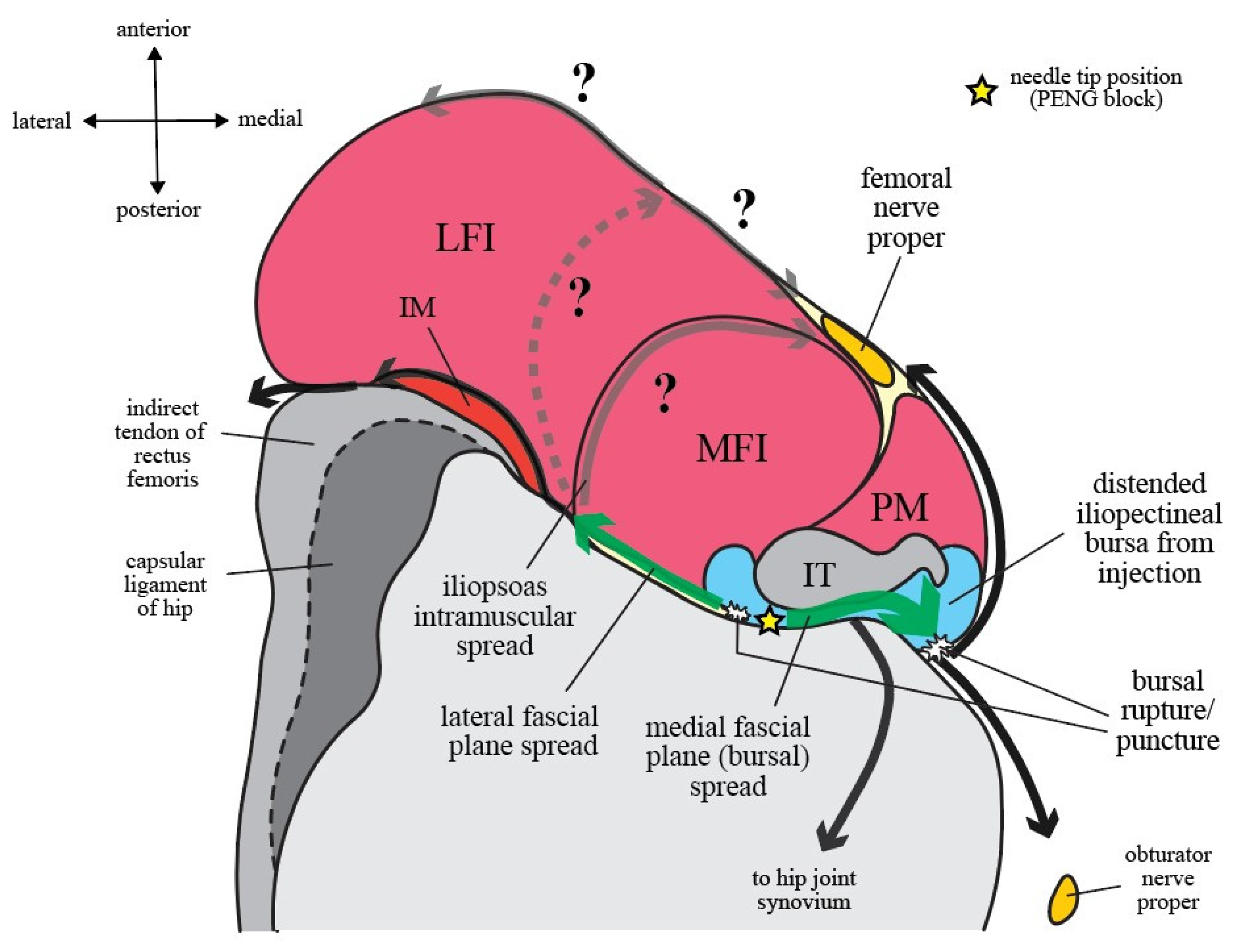
2.5. Pericapsular Nerve Group (PENG) Block and Iliopsoas Plane Block (IPB): Same, Same but Different?
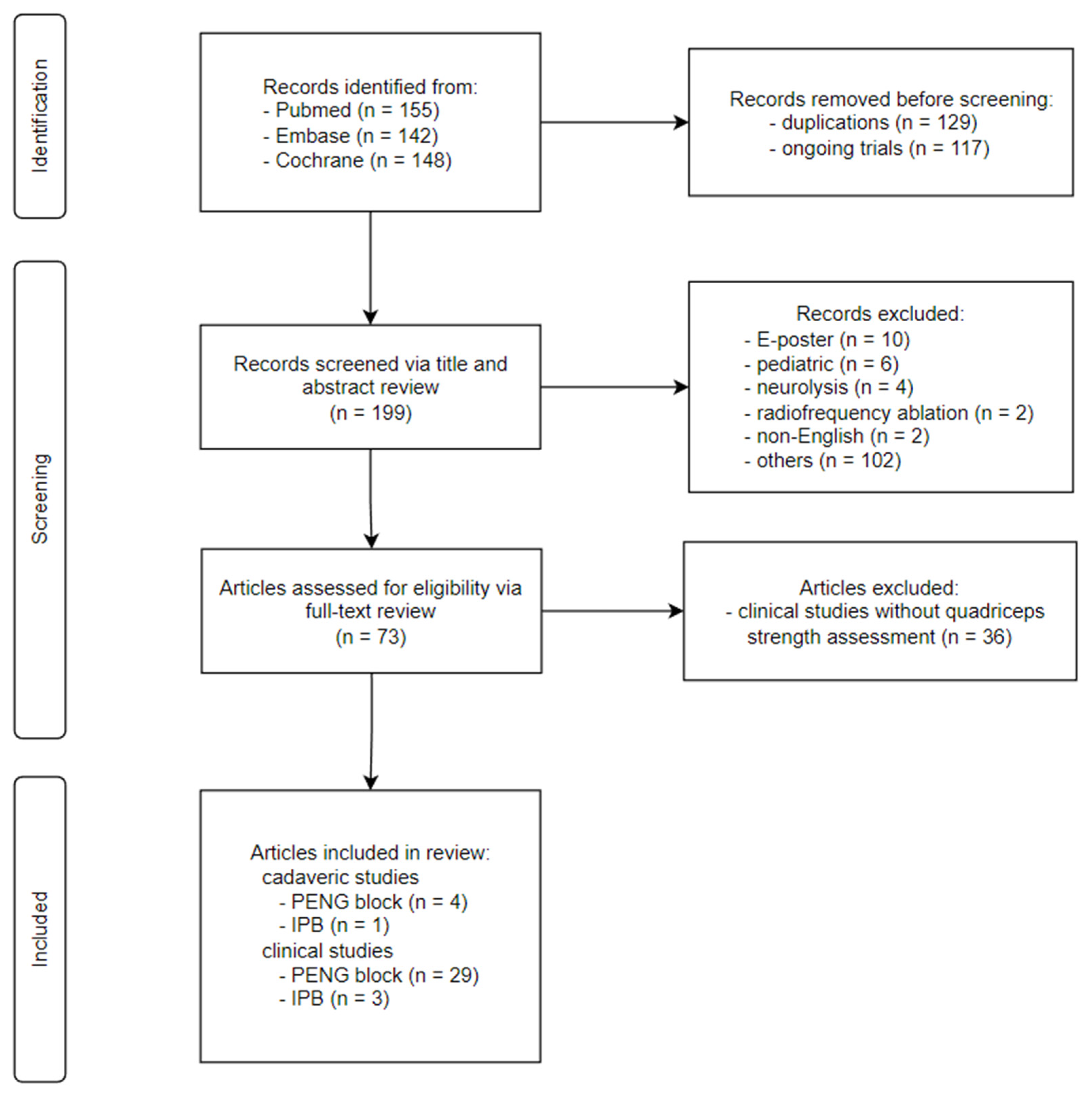
3. Methods
4. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Published Date, Country) | Study Type (Case Number) | Final Needle Tip Position | Bolus Volume | Quadriceps Weakness Frequency | Extra-IP Injectate Spread † | Routes of Injectate Spread | |
|---|---|---|---|---|---|---|---|
| Position in IP | Relative to IT | ||||||
| A. Studies reporting quadriceps weakness (PENG block, n = 4) | |||||||
| Yu [2] (May 2019, Canada) a | Case report (2) | Medial border of osseous IP (PENG block) | Deep to IT but more cephalad and superficial (case 1), more medial (case 2) | 20 mL | <2% (purported, no supporting data) | FIC (+) | Medial fascial plane (bursal) spread, superficial intramuscular spread |
| Ahiskalioglu [3] (May 2020, Turkey) b | Case report (2) | Medial border of osseous IP (PENG block) | Not specified | 30 mL | Not assessable | FIC (+), SP (+) | Not deducible |
| Lin [5] (February 2021, Australia) c | RCT (30) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | 26% | FIC (+) | Medial fascial plane (bursal) spread |
| Aliste [4] (July 2021, Chile) d | RCT (20) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | 25–45% ¶ | FIC (?), SP (?) ¶ | Not deducible |
| B. Studies with signs of potential quadriceps weakness (PENG block, n = 11; IPB, n = 1) | |||||||
| Santos [42] (June 2019, Portugal) e | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | FIC (+) ‡, SP (−) ‡ | Medial fascial plane (bursal) spread, lateral fascial plane spread |
| Aydin [43] (August 2019, Turkey) f | Case report (2) | Medial border of osseous IP (PENG block) | Deep to IT | 30 mL | - | FIC (+), SP (+) | Not deducible |
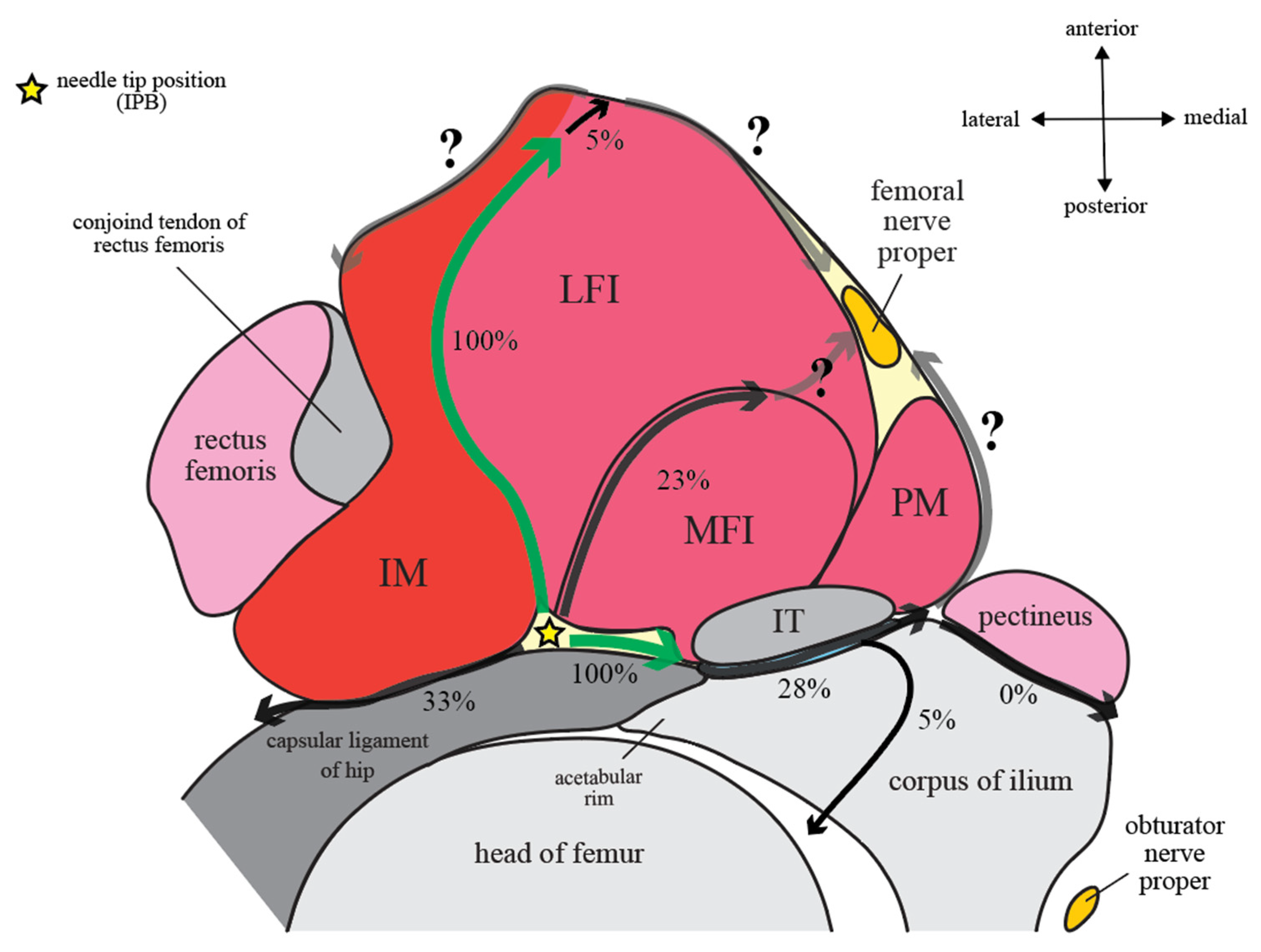
| Nielsen [7] (October 2019, Denmark) g | RCT (20), volunteer study | Junction between ligamentous and muscular IP (IPB) | Lateral to IT | 5 mL | - | FIC (+), SP (−) | See Figure 4 |
| Ahiskalioglu [45] (February 2020, Turkey) h | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 30 mL | - | FIC (+), SP (+) | Not deducible |
| Ahiskalioglu [44] (March 2020, Turkey) i | Case report (2) | Medial border of osseous IP (PENG block) | Deep to IT | 30 mL | - | FIC (+), SP (+) | Not deducible |
| Sandri [46] (June 2020, Italy) j | Case series (10) | Medial border of osseous IP (PENG block) | Not specified | 40 mL | - | FIC (+), SP (+) | Not deducible |
| Talawar [47] (July 2020, India) k | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | FIC (+) | Not deducible |
| Singh [49] (October 2020, India) l | Case report (1) | - l | Superficial to IT (intramuscular) | 15 mL | - | FIC (+), SP (+) | Not deducible |
| Oksuz [50] (March 2021, Turkey) m | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 35 mL | - | FIC (+) | Not deducible |
| Gong [51] (October 2021, China) n | Case series (5) | Medial border of osseous IP (PENG block) | Not specified | 30 mL | - | FIC (+) | Not deducible |
| Choi [60] (March 2022, Korea) o | RCT (27) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | FIC (+) § | Medial fascial plane (bursal) spread |
| Senthil [61] (March 2022, India) p | RCT (20) | Medial border of osseous IP (PENG block) | Deep to IT | 30 mL | - | FIC (+) § | Not deducible |
| C. Studies reporting no quadriceps weakness (PENG block, n = 14, IPB, n = 2) | |||||||
| Giron-Arango [1] (November 2018, Canada) | Case series (5) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Mistry [52] (March 2019, India) | Case series (5) | Medial border of osseous IP (PENG block) | Deep to IT | no information | - | - | Medial fascial plane (bursal) spread, lateral fascial plane spread |
| Pagano [55] (December 2019, Italy) | Case series (6) | Medial border of osseous IP (PENG block) | Not specified | 20 mL | - | - | Lateral fascial plane spread |
| Prado-Kittel [58] (March 2020, Chile) | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Casas Reza [56] (April 2020, Spain) | Case series (8) | Medial border of osseous IP (PENG block) | Not specified | 20 mL | - | - | Not deducible |
| Alrefaey [62] (September 2020, Egypt) | RCT (30) | Medial border of osseous IP (PENG block) | Not specified | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Singh [48] (September 2020, India) | Case series (10) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Fujino [57] (March 2021, Japan) | Case report (2) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread, lateral fascial plane spread |
| Rocha-Romero [54] (April 2021, Costa Rica) | Case series (5) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Not deducible |
| Pascarella [65] (May 2021, Italy) | RCT (30) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Allard [59] (June 2021, France) | Cohort study (21) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Not deducible |
| Hua [63] (February 2022, China) | RCT (27) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Not deducible |
| da Costa [66] (March 2022, Brazil) | Case report (1) | Medial border of osseous IP (PENG block) | Deep to IT | 15 mL | - | - | Not deducible |
| Zheng [64] (March 2022, China) | RCT (36) | Medial border of osseous IP (PENG block) | Deep to IT | 20 mL | - | - | Medial fascial plane (bursal) spread |
| Wang [40] (April 2022, China) | Case series (8) | Junction between ligamentous and muscular IP (IPB) | Lateral to IT | 10 mL | - | - | Not deducible |
| Wang [41] (May 2022, China) | Case series (5) | Junction between ligamentous and muscular IP (IPB) | Lateral to IT | 10 mL | - | - | Not deducible |

5. Discussion
5.1. Cadaveric Studies
5.2. Clinical Studies
5.3. Injectate Spread Behavior
5.3.1. Craniocaudal Spread within Iliopsoas Plane (IP)
5.3.2. Spread Outside of Iliopsoas Plane (IP): Extra-IP Spread
5.4. Factors Leading to Quadriceps Weakness
5.5. Recommendations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Girón-Arango, L.; Peng, P.W.H.; Chin, K.J.; Brull, R.; Perlas, A. Pericapsular Nerve Group (PENG) Block for Hip Fracture. Reg. Anesth. Pain Med. 2018, 43, 859–863. [Google Scholar] [CrossRef]
- Yu, H.C.; Moser, J.J.; Chu, A.Y.; Montgomery, S.H.; Brown, N.; Endersby, R.V.W. Inadvertent quadriceps weakness following the pericapsular nerve group (PENG) block. Reg. Anesth. Pain Med. 2019, 44, 611–613. [Google Scholar] [CrossRef] [PubMed]
- Ahiskalioglu, A.; Aydin, M.E.; Celik, M.; Ahiskalioglu, E.O.; Tulgar, S. Can high volume pericapsular nerve group (PENG) block act as a lumbar plexus block? J. Clin. Anesth. 2020, 61, 109650. [Google Scholar] [CrossRef]
- Aliste, J.; Layera, S.; Bravo, D.; Jara, A.; Munoz, G.; Barrientos, C.; Wulf, R.; Branez, J.; Finlayson, R.J.; Tran, Q. Randomized comparison between pericapsular nerve group (PENG) block and suprainguinal fascia iliaca block for total hip arthroplasty. Reg. Anesth. Pain Med. 2021, 46, 874–878. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.Y.; Morrison, C.; Brown, B.; Saies, A.A.; Pawar, R.; Vermeulen, M.; Anderson, S.R.; Lee, T.S.; Doornberg, J.; Kroon, H.M.; et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery: A single-center double-blinded randomized comparative trial. Reg. Anesth. Pain Med. 2021, 46, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Giron Arango, L.; Peng, P. Reply to Dr Yu et al: Inadvertent quadriceps weakness following the pericapsular nerve group (PENG) block. Reg. Anesth. Pain Med. 2019, 44, 613–614. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.D.; Madsen, M.N.; Østergaard, H.K.; Bjørn, S.; Pedersen, E.M.; Nielsen, T.D.; Søballe, K.; Børglum, J.; Bendtsen, T.F. An iliopsoas plane block does not cause motor blockade-A blinded randomized volunteer trial. Acta Anaesthesiol. Scand. 2019, 64, 368–377. [Google Scholar] [CrossRef]
- Nielsen, N.D.; Greher, M.; Moriggl, B.; Hoermann, R.; Nielsen, T.D.; Borglum, J.; Bendtsen, T.F. Spread of injectate around hip articular sensory branches of the femoral nerve in cadavers. Acta Anaesthesiol. Scand. 2018, 62, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Marhofer, P.; Willschke, H.; Kettner, S. Current concepts and future trends in ultrasound-guided regional anesthesia. Curr. Opin. Anaesthesiol. 2010, 23, 632–636. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.N. Iliopsoas: Pathology, Diagnosis, and Treatment. Clin. Sports Med. 2016, 35, 419–433. [Google Scholar] [CrossRef]
- Guillin, R.; Cardinal, E.; Bureau, N.J. Sonographic anatomy and dynamic study of the normal iliopsoas musculotendinous junction. Eur. Radiol. 2009, 19, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Tatu, L.; Parratte, B.; Vuillier, F.; Diop, M.; Monnier, G. Descriptive anatomy of the femoral portion of the iliopsoas muscle. Anatomical basis of anterior snapping of the hip. Surg. Radiol. Anat. 2001, 23, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Ward, W.T.; Fleisch, I.D.; Ganz, R. Anatomy of the iliocapsularis muscle. Relevance to surgery of the hip. Clin. Orthop. Relat. Res. 2000, 374, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Babst, D.; Steppacher, S.D.; Ganz, R.; Siebenrock, K.A.; Tannast, M. The iliocapsularis muscle: An important stabilizer in the dysplastic hip. Clin. Orthop. Relat. Res. 2011, 469, 1728–1734. [Google Scholar] [CrossRef] [PubMed]
- Souza, P.M.E.; Santos, E.B.G.D. Bursae around the hip: Anatomy, pathology, and mimics. Educ. Exibit. Eur. Soc. Radiol. 2014, ECR 2014, C-0476. [Google Scholar]
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 39th ed.; Churchill Livingstone: London, UK, 2015; p. 2285. [Google Scholar]
- Chandler, S. The iliopsoas bursa in man. Anat. Rec. 1934, 58, 235–240. [Google Scholar] [CrossRef]
- Peters, A.; Tillmann, B. Bursa iliopectineal—Size and morphology. Anat. Anz. 1988, 167, 403–407. [Google Scholar]
- Nestorova, R.; Vlad, V.; Petranova, T.; Porta, F.; Radunovic, G.; Micu, M.C.; Iagnocco, A. Ultrasonography of the hip. Med. Ultrason. 2012, 14, 217–224. [Google Scholar]
- Bianchi, S.; Martinoli, C. Ultrasound of the Musculoskeletal System; Springer: Berlin, Germany, 2007; pp. 554–610. [Google Scholar]
- Jacobson, J.A.; Khoury, V.; Brandon, C.J. Ultrasound of the Groin: Techniques, Pathology, and Pitfalls. AJR Am. J. Roentgenol. 2015, 205, 513–523. [Google Scholar] [CrossRef]
- Tran, J.; Agur, A.; Peng, P. Is pericapsular nerve group (PENG) block a true pericapsular block? Reg. Anesth. Pain Med. 2019, 44, 257. [Google Scholar] [CrossRef]
- Peng, P.W.H.; Perlas, A.; Chin, K.J. Reply to Dr Nielsen: Pericapsular Nerve Group (PENG) block for hip fracture. Reg. Anesth. Pain Med. 2019, 44, 415–416. [Google Scholar] [CrossRef] [PubMed]
- Vandenbussche, E.; Saffarini, M.; Taillieu, F.; Mutschler, C. The asymmetric profile of the acetabulum. Clin. Orthop. Relat. Res. 2008, 466, 417–423. [Google Scholar] [CrossRef]
- Wagner, F.V.; Negrao, J.R.; Campos, J.; Ward, S.R.; Haghighi, P.; Trudell, D.J.; Resnick, D. Capsular ligaments of the hip: Anatomic, histologic, and positional study in cadaveric specimens with MR arthrography. Radiology 2012, 263, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.; Osbahr, D.C.; Choi, D.; Ranawat, A.S.; Kelly, B.T.; Coleman, S.H. Defining the origins of the iliofemoral, ischiofemoral, and pubofemoral ligaments of the hip capsuloligamentous complex utilizing computer navigation. HSS J. 2011, 7, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Kho, J.; Azzopardi, C.; Davies, A.M.; James, S.L.; Botchu, R. MRI assessment of anatomy and pathology of the iliofemoral ligament. Clin. Radiol. 2020, 75, 960.e17–960.e22. [Google Scholar] [CrossRef] [PubMed]
- Dalens, B.; Vanneuville, G.; Tanguy, A. Comparison of the fascia iliaca compartment block with the 3-in-1 block in children. Anesth. Analg. 1989, 69, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.D.; Moriggl, B.; Soballe, K.; Kolsen-Petersen, J.A.; Borglum, J.; Bendtsen, T.F. A Cadaveric Study of Ultrasound-Guided Subpectineal Injectate Spread Around the Obturator Nerve and Its Hip Articular Branches. Reg. Anesth. Pain Med. 2017, 42, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, M.; Johnson, K.; Atkinson, R.; Snow, B.; Shaw, C.; Brown, A.; Vangsness, C.T., Jr. Characterisation and classification of the neural anatomy in the human hip joint. Hip Int. 2012, 22, 75–81. [Google Scholar] [CrossRef]
- Wertheimer, L.G. The sensory nerves of the hip joint. J. Bone Joint Surg. Am. 1952, 34, 477–487. [Google Scholar] [CrossRef]
- Birnbaum, K.; Prescher, A.; Hessler, S.; Heller, K.D. The sensory innervation of the hip joint—An anatomical study. Surg. Radiol. Anat. SRA 1997, 19, 371–375. [Google Scholar] [CrossRef]
- Gardner, E. The innervation of the hip joint. Anat. Rec. 1948, 101, 353–371. [Google Scholar] [CrossRef]
- Short, A.J.; Barnett, J.J.G.; Gofeld, M.; Baig, E.; Lam, K.; Agur, A.M.R.; Peng, P.W.H. Anatomic Study of Innervation of the Anterior Hip Capsule: Implication for Image-Guided Intervention. Reg. Anesth. Pain Med. 2018, 43, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.D.; Bendtsen, T.F. Motor-sparing regional analgesia for hip-derived pain. Reg. Anesth. Pain Med. 2019, 44, 415. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.D.; Bendtsen, T.F. In response: Motor blockade after iliopsoas plane (IPB) and pericapsular nerve group (PENG) blocks: A little may go a long way. Acta Anaesthesiol. Scand. 2021, 65, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Ciftci, B.; Ahiskalioglu, A.; Altintas, H.M.; Tekin, B.; Sakul, B.U.; Alici, H.A. A possible mechanism of motor blockade of high volume pericapsular nerve group (PENG) block: A cadaveric study. J. Clin. Anesth. 2021, 74, 110407. [Google Scholar] [CrossRef] [PubMed]
- Altinpulluk, E.Y.; Galluccio, F.; Salazar, C.; Espinoza, K.; Olea, M.S.; Hochberg, U.; de Santiago, J.; Perez, M.F. Peng block in prosthetic hip replacement: A cadaveric radiological evaluation. J. Clin. Anesth. 2020, 65, 109888. [Google Scholar] [CrossRef]
- Kitcharanant, N.; Leurcharusmee, P.; Wangtapun, P.; Kantakam, P.; Maikong, N.; Mahakkanukrauh, P.; Tran, Q. Surgeon-performed pericapsular nerve group (PENG) block for total hip arthroplasty using the direct anterior approach: A cadaveric study. Reg. Anesth. Pain Med. 2022, 47, 359–363. [Google Scholar] [CrossRef]
- Wang, C.G.; Yang, Y.; Yang, M.Y.; Wang, X.L.; Ding, Y.L. Analgesic effect of iliopsoas plane block for hip fracture. Perioper. Med. 2022, 11, 15. [Google Scholar] [CrossRef]
- Wang, C.G.; Yang, M.Y.; Yang, Y.; Ma, F.; Jiang, B. Iliopsoas plane block for postoperative analgesia after total hip replacement. Minerva Anestesiol. 2022, 88, 635–636. [Google Scholar] [CrossRef] [PubMed]
- Santos, O.; Pereira, R.; Cabral, T.; Lages, N.; Machado, H. Is continuous PENG block the new 3-in-1? J. Anesth. Clin. Res. 2019, 10. [Google Scholar]
- Aydin, M.E.; Borulu, F.; Ates, I.; Kara, S.; Ahiskalioglu, A. A Novel Indication of Pericapsular Nerve Group (PENG) Block: Surgical Anesthesia for Vein Ligation and Stripping. J. Cardiothorac. Vasc. Anesth. 2020, 34, 843–845. [Google Scholar] [CrossRef] [PubMed]
- Ahiskalioglu, A.; Aydin, M.E.; Ozkaya, F.; Ahiskalioglu, E.O.; Adanur, S. A novel indication of Pericapsular Nerve Group (PENG) block: Prevention of adductor muscle spasm. J. Clin. Anesth. 2020, 60, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Ahiskalioglu, A.; Aydin, M.E.; Ahiskalioglu, E.O.; Tuncer, K.; Celik, M. Pericapsular nerve group (PENG) block for surgical anesthesia of medial thigh. J. Clin. Anesth. 2020, 59, 42–43. [Google Scholar] [CrossRef]
- Sandri, M.; Blasi, A.; De Blasi, R.A. PENG block and LIA as a possible anesthesia technique for total hip arthroplasty. J. Anesth. 2020, 34, 472–475. [Google Scholar] [CrossRef]
- Talawar, P.; Tandon, S.; Tripathy, D.K.; Kaushal, A. Combined pericapsular nerve group and lateral femoral cutaneous nerve blocks for surgical anaesthesia in hip arthroscopy. Indian J. Anaesth. 2020, 64, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Ahmed, W. Continuous Pericapsular Nerve Group Block for Hip Surgery: A Case Series. A A Pract. 2020, 14, e01320. [Google Scholar] [CrossRef]
- Singh, S. Total hip arthroplasty under continuous pericapsular nerve group block (cPENG) in a high risk patient. J. Clin. Anesth. 2020, 68, 110096. [Google Scholar] [CrossRef] [PubMed]
- Oksuz, G.; Arslan, M.; Bilal, B.; Gisi, G. A novel indication for pericapsular nerve group (PENG) block: High volume PENG block combination with sciatic block for surgical anesthesia of lower limb. J. Clin. Anesth. 2021, 71, 110218. [Google Scholar] [CrossRef]
- Gong, W.Y.; Li, N.; Chen, Y.Y.; Wang, A.Z.; Fan, K. Combination of Pericapsular Nerve Group (PENG) and Sacral Plexus Blocks for Minimally Invasive Percutaneous Internal Fixation in Outpatient with Femoral Neck Pathologic Fracture. Pain Med. 2022, 23, 427–428. [Google Scholar] [CrossRef]
- Mistry, T.; Sonawane, K.B.; Kuppusamy, E. PENG block: Points to ponder. Reg. Anesth. Pain Med. 2019, 44, 423–424. [Google Scholar] [CrossRef]
- Rocha Romero, A.; Carvajal Valdy, G.; Lemus, A.J. Ultrasound-guided pericapsular nerve group (PENG) hip joint phenol neurolysis for palliative pain. Can. J. Anaesth. 2019, 66, 1270–1271. [Google Scholar] [CrossRef]
- Rocha-Romero, A.; Arias-Mejia, K.; Salas-Ruiz, A.; Peng, P.W.H. Pericapsular nerve group (PENG) block for hip fracture in the emergency department: A case series. Anaesth. Rep. 2021, 9, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Pagano, T.; Scarpato, F.; Chicone, G.; Carbone, D.; Bussemi, C.B.; Albano, F.; Ruotolo, F. Analgesic evaluation of ultrasound-guided pericapsular nerve group (PENG) block for emergency hip surgery in fragile patients: A case series. Arthroplasty 2019, 1, 18. [Google Scholar] [CrossRef] [PubMed]
- Reza, P.C.; García, P.D.; Vazquez, M.G.; Rodriquez, L.S.; Alvarez, S.L. Pericapsular nerve group block for hip surgery. Minerva Anestesiol. 2020, 86, 463–465. [Google Scholar]
- Fujino, T.; Odo, M.; Okada, H.; Takahashi, S.; Kikuchi, T. Continuous pericapsular nerve group block for postoperative pain management in total hip arthroplasty: Report of two cases. JA Clin. Rep. 2021, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Prado-Kittel, C.; Zumelzu-Sanchez, P.; Palma-Licandeo, A.; Faundez-Lillo, G.; Ellenberg-Oyarce, K.; Jorquera-Adarme, B. Continuous pericapsular nerve group blockade as analgesia for fracture of the posterior column and wall of the acetabulum; a case report and description of infusion regimen for extending analgesic effect to the distal femoral area. Rev. Esp. Anestesiol. Reanim. 2020, 67, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Allard, C.; Pardo, E.; de la Jonquiere, C.; Wyniecki, A.; Soulier, A.; Faddoul, A.; Tsai, E.S.; Bonnet, F.; Verdonk, F. Comparison between femoral block and PENG block in femoral neck fractures: A cohort study. PLoS ONE 2021, 16, e0252716. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Park, K.K.; Lee, B.; Nam, W.S.; Kim, D.H. Pericapsular Nerve Group (PENG) Block versus Supra-Inguinal Fascia Iliaca Compartment Block for Total Hip Arthroplasty: A Randomized Clinical Trial. J. Pers. Med. 2022, 12, 408. [Google Scholar] [CrossRef]
- Senthil, K.; Kumar, P.; Ramakrishnan, L. Comparison of Pericapsular Nerve Group Block versus Fascia Iliaca Compartment Block as Postoperative Pain Management in Hip Fracture Surgeries. Anesth. Essays Res. 2022, 15, 352–356. [Google Scholar]
- Alrefaey, A.K.; Abouelela, M.A. Pericapsular nerve group block for analgesia of positioning pain during spinal anesthesia in hip fracture patients, a randomized controlled study. Egypt. J. Anaesth. 2020, 36, 234–239. [Google Scholar] [CrossRef]
- Hua, H.; Xu, Y.; Jiang, M.; Dai, X. Evaluation of Pericapsular Nerve Group (PENG) Block for Analgesic Effect in Elderly Patients with Femoral Neck Fracture Undergoing Hip Arthroplasty. J. Healthc. Eng. 2022, 2022, 7452716. [Google Scholar] [CrossRef]
- Zheng, J.; Pan, D.; Zheng, B.; Ruan, X. Preoperative pericapsular nerve group (PENG) block for total hip arthroplasty: A randomized, placebo-controlled trial. Reg. Anesth. Pain Med. 2022, 47, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Costa, F.; Del Buono, R.; Pulitano, R.; Strumia, A.; Piliego, C.; De Quattro, E.; Cataldo, R.; Agro, F.E.; Carassiti, M.; et al. Impact of the pericapsular nerve group (PENG) block on postoperative analgesia and functional recovery following total hip arthroplasty: A randomised, observer-masked, controlled trial. Anaesthesia 2021, 76, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- da Costa, A.O.; Izolani, G.V.; de Souza, I.F.M.; Santiago, B.V.M. Continuous pericapsular nerve group (PENG) block through an elastomeric infusion system, associated with the lateral cutaneous nerve block of the thigh for total hip arthroplasty. BMJ Case Rep. 2022, 15, e246833. [Google Scholar] [CrossRef] [PubMed]
- Girón-Arango, L.; Tran, J.; Peng, P.W. Reply to Aydin et al.: A Novel Indication of Pericapsular Nerve Group Block: Surgical Anesthesia for Vein Ligation and Stripping. J. Cardiothorac. Vasc. Anesth. 2020, 34, 845–846. [Google Scholar] [CrossRef] [PubMed]
- Barker, J.P.; Yang, Y.; Matz, J.; Marmor, M.T.; Morshed, S. The Iliopectineal Fascia: A Cadaveric Anatomical Study. J. Orthop. Trauma 2020, 35, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Dauffenbach, J.; Pingree, M.J.; Wisniewski, S.J.; Murthy, N.; Smith, J. Distribution pattern of sonographically guided iliopsoas injections: Cadaveric investigation using coned beam computed tomography. J. Ultrasound Med. 2014, 33, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Morrison, C.; Brown, B.; Lin, D.Y.; Jaarsma, R.; Kroon, H. Analgesia and anesthesia using the pericapsular nerve group block in hip surgery and hip fracture: A scoping review. Reg. Anesth. Pain Med. 2021, 46, 169–175. [Google Scholar] [CrossRef]
- Leunig, M.; Faas, M.; von Knoch, F.; Naal, F.D. Skin crease ‘bikini’ incision for anterior approach total hip arthroplasty: Surgical technique and preliminary results. Clin. Orthop. Relat. Res. 2013, 471, 2245–2252. [Google Scholar] [CrossRef]
- Simons, M.J.; Amin, N.H.; Cushner, F.D.; Scuderi, G.R. Characterization of the Neural Anatomy in the Hip Joint to Optimize Periarticular Regional Anesthesia in Total Hip Arthroplasty. J. Surg. Orthop. Adv. 2015, 24, 221–224. [Google Scholar] [PubMed]
- Bhakta, P.; Karim, H.M.R.; O’Donnell, B.D. Comment on: Total hip arthroplasty under continuous pericapsular nerve group block (cPENG) in a high-risk patient. J. Clin. Anesth. 2021, 73, 110301. [Google Scholar] [CrossRef] [PubMed]
- Adler, R.S.; Buly, R.; Ambrose, R.; Sculco, T. Diagnostic and therapeutic use of sonography-guided iliopsoas peritendinous injections. Am. J. Roentgenol. 2005, 185, 940–943. [Google Scholar] [CrossRef] [PubMed]
- Endersby, R.V.W.; Moser, J.J.; Ho, E.C.Y.; Yu, H.C.; Spencer, A.O. Motor blockade after iliopsoas plane (IPB) and pericapsular nerve group (PENG) blocks: A little may go a long way. Acta Anaesthesiol. Scand. 2021, 65, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS (R)) Society recommendations. Acta Orthopaedica. 2020, 91, 363. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeoh, S.-R.; Chou, Y.; Chan, S.-M.; Hou, J.-D.; Lin, J.-A. Pericapsular Nerve Group Block and Iliopsoas Plane Block: A Scoping Review of Quadriceps Weakness after Two Proclaimed Motor-Sparing Hip Blocks. Healthcare 2022, 10, 1565. https://doi.org/10.3390/healthcare10081565
Yeoh S-R, Chou Y, Chan S-M, Hou J-D, Lin J-A. Pericapsular Nerve Group Block and Iliopsoas Plane Block: A Scoping Review of Quadriceps Weakness after Two Proclaimed Motor-Sparing Hip Blocks. Healthcare. 2022; 10(8):1565. https://doi.org/10.3390/healthcare10081565
Chicago/Turabian StyleYeoh, Shang-Ru, Yen Chou, Shun-Ming Chan, Jin-De Hou, and Jui-An Lin. 2022. "Pericapsular Nerve Group Block and Iliopsoas Plane Block: A Scoping Review of Quadriceps Weakness after Two Proclaimed Motor-Sparing Hip Blocks" Healthcare 10, no. 8: 1565. https://doi.org/10.3390/healthcare10081565