
Regional Anesthetic and Analgesic Techniques for Clavicle Fractures and Clavicle Surgeries: Part 1—A Scoping Review

 , ,
, ,
Abstract
:1. Background
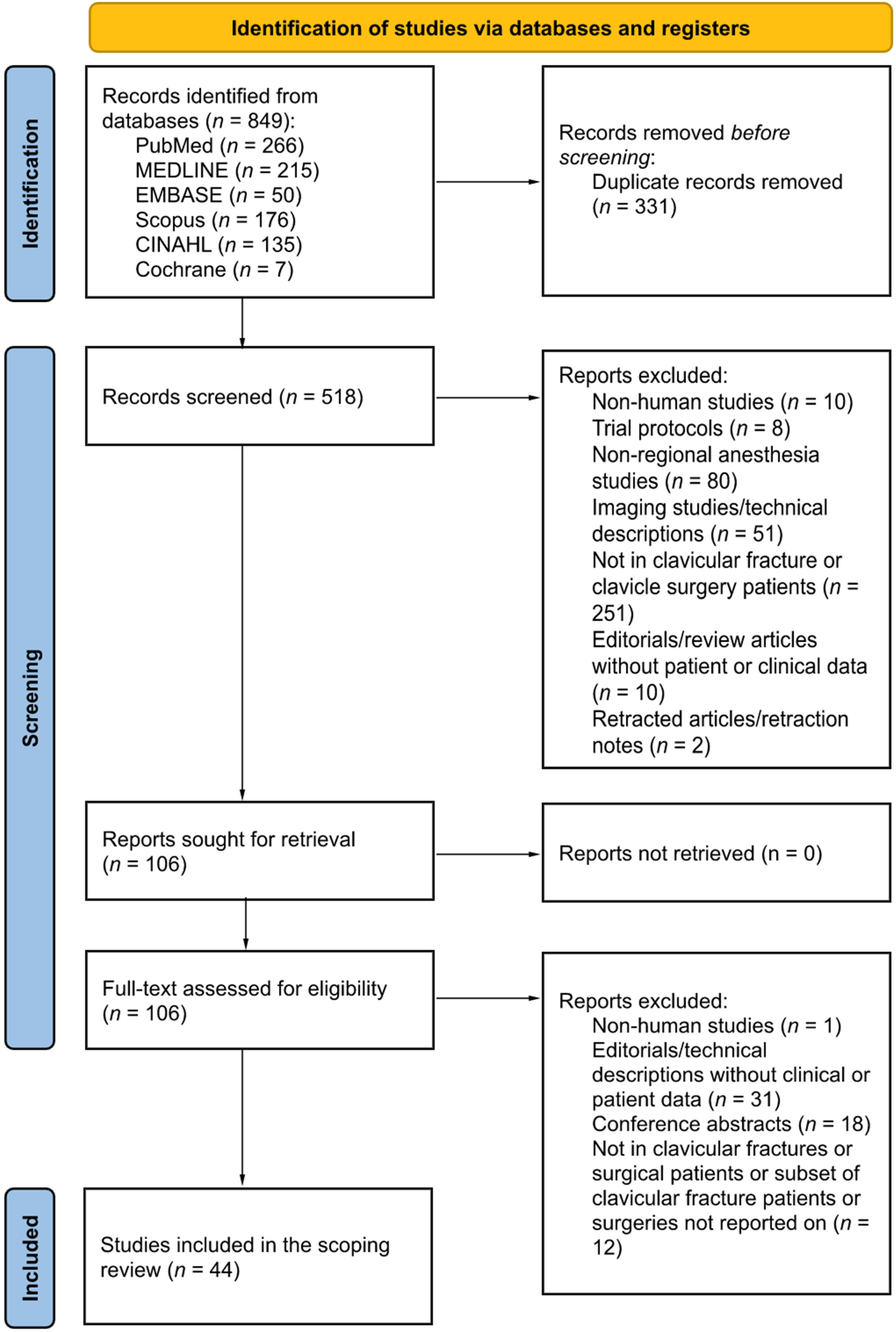
2. Materials and Methods
3. Results

{kind=link}
| Reference (Year), Country | Study Design | Sample Size | Fracture Location | Type of Block | Needle Guidance | LA Type and Volume | Anesthetic Technique | Perioperative Analgesia Regime | Outcome(s) |
|---|---|---|---|---|---|---|---|---|---|
| [6] Yoo and colleagues (2018), South Korea | Retrospective observational | 50 (25 + 25) | Midshaft and distal | GA and surgical site infiltration vs. GA alone | LM | 30 mL of injectate comprising of 300 mg ropivacaine, 5 mg morphine sulphate, 1 mg adrenaline, and 20 mL 0.9% sodium chloride (total volume 61.5 mL) | GA | IV Fentanyl and ketorolac PCA for 24 h, paracetamol, tramadol, pregabalin |
|
| [7] Reverdy (2015), France | Prospective observational | 12 | NR | SCPB and ISB | US | 1% mepivacaine or 0.75% ropivacaine, median volume 20 mL (range 16 to 40 mL) | Sedation or awake | Paracetamol, ketoprofen |
|
| [8] Banerjee and colleagues (2019), India | RCT | 60 (30 + 30) | NR | SCPB and ISB vs. GA alone | US | SCPB: 5 mL 2% lignocaine with adrenaline and 5 mL 0.5% bupivacaine ISB: 8 mL 2% lignocaine with adrenaline and 8 mL 0.5% bupivacaine | Awake vs. GA | Fentanyl, paracetamol, tramadol |
|
| [13] Zhuo and colleagues (2022), China | RCT | 40 | Midshaft | ICPB and ISB vs. CPB and ISB | US | ICPB: 5 mL 0.375% ropivacaine ISB: 20 mL 0.375% ropivacaine CPB: 20 mL 0.375% ropivacaine | Awake | NR |
|
| [21] Abdelghany and colleagues (2021), Egypt | RCT | 70 (35 + 35) | NR | SCPB vs. SCPB and ISB | US | SCPB: 10 mL 0.25% bupivacaine ISB: 15 mL 0.25% bupivacaine | GA | Fentanyl *, paracetamol, morphine |
|
| [23] Arjun and colleagues (2020), India | Randomised, double-blind RCT | 50 (25 + 25) | 26 Midshaft 24 Distal | SCPB and ISB vs. ICPB and ISB | US | SCPB or ICPB: 10 mL 0.5% bupivacaine ISB: 10 mL 0.5% bupivacaine | Sedation | Tramadol |
|
| [24] Olofsson and colleagues (2020), Switzerland | Prospective case-control | 126 (50 + 76) | 95 Midshaft 31 Distal | ISB with GA vs. GA alone | US | ISB: 20 mL 0.5% bupivacaine | GA | Sufentanil *, morphine, paracetamol, oxycodone |
|
| [25] Ryan and colleagues (2020), USA | Retrospective observational | 110 (52 + 58) | 90 Midshaft 20 Distal | SCPB and ISB vs. ISB with GA | LM | SCPB: 10 mL 0.5% bupivacaine ISB: 20 mL 0.5% bupivacaine with adrenaline | Awake vs. GA | No standardized analgesia regimen |
|
| [35] Beletsky and colleagues (2020), USA | Retrospective observational | 2300 (346 + 1954) | NR | NR | NR | NR | NR | NR | Regional anesthesia use is associated with ↑ odds (1.70, p < 0.01) for same-day discharge. |
| [36] Neha Gupta and colleagues (2019), India | RCT | 60 (30 + 30) | NR | ISB alone vs. ISB and SCPB | NR | SCPB: 0.5 mg.kg−1 bupivacaine with 1 mg·kg−1 lignocaine to ≥10 mL ISB: 1 mg·kg−1 bupivacaine with 3 mg·kg−1 lignocaine to ≥20 mL | Sedation | Fentanyl * |
|
| [37] Kaciroglu and colleagues (2019), Turkey | Retrospective | 16 | 1 Medial 3 Midshaft 6 Lateral | SCPB and ISB | US | SCPB: 5 mL 2% lignocaine and 5 mL 0.5% bupivacaine ISB: 7.5 mL 2% lignocaine and 7.5 mL 0.5% bupivacaine | Mixed | NR |
|
| [43] Rajbanshi and colleagues (2018), Nepal | Randomised prospective comparative study | 60 (30 + 30) | NR | SCPB and ISB vs. SCPB and SpC | US | SCPB: 10 mL 0.25% bupivacaine ISB: 20 mL 0.25% bupivacaine SpC: 20 mL 0.25% bupivacaine | Sedation | Fentanyl, paracetamol |
|
| [44] Ho and colleagues (2018), Canada | Prospective observational | 7 | NR | SCPB | US | 8–14 mL 0.25–0.5% bupivacaine with adrenaline | Not applicable | NR |
|
| [45] Balaban and colleagues (2018), Turkey | Retrospective observational | 12 | NR | SCPB and ISB | US | SCPB: 0.25 mL·kg−1 0.5% bupivacaine ISB: 0.25 mL·kg−1 0.5% bupivacaine | Sedation | Tramadol | One patient felt mild pain at the start of surgery, and another patient required deeper sedation during manipulation of the clavicle. |
| [48] Contractor and colleagues (2016), India | Prospective | 30 | NR | SCPB and ISB | Unclear, possibly US | SCPB: 10 mL 0.25% bupivacaine ISB: 10–15 mL 1.5% lignocaine with adrenaline plus 5–10 mL 0.5% bupivacaine | Sedation | NR |
|
| [53] Kuchyn (2013), Russia | Randomised controlled trial | 60 | NR | SCPB and ISB (nerve stimulator vs. ultrasound guided) | LM | SCPB: 0.5% lignocaine ISB: 1% lignocaine, 0.25% bupivacaine Total LA volume 30–40 mL | Sedation | NR | Ultrasound guidance ↓ conversion to GA vs. nerve stimulation (p = 0.024) (failure ↑ with nerve stimulation alone, odds ratio 13.16) |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Postacchini, F.; Gumina, S.; De Santis, P.; Albo, F. Epidemiology of clavicle fractures. J. Should. Elbow Surg. 2002, 11, 452. [Google Scholar] [CrossRef]
- Kim, D.W.; Kim, D.H.; Kim, B.S.; Cho, C.H. Current Concepts for Classification and Treatment of Distal Clavicle Fractures. Clin. Orthop. Surg. 2020, 12, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Frima, H.; van Heijl, M.; Michelitsch, C.; van der Meijden, O.; Beeres, F.J.P.; Houwert, R.M.; Sommer, C. Clavicle fractures in adults; current concepts. Eur. J. Trauma Emerg Surg. 2020, 46, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Guerra, E.; Previtali, D.; Tamborini, S.; Filardo, G.; Zaffagnini, S.; Candrian, C. Midshaft Clavicle Fractures: Surgery Provides Better Results as Compared With Nonoperative Treatment: A Meta-analysis. Am. J. Sports Med. 2019, 47, 3541–3551. [Google Scholar] [CrossRef] [PubMed]
- Moverley, R.; Little, N.; Gulihar, A.; Singh, B. Current concepts in the management of clavicle fractures. J. Clin. Orthop. Trauma 2020, 11 (Suppl. S1), S25–S30. [Google Scholar] [CrossRef]
- Yoo, J.S.; Heo, K.; Kwon, S.M.; Lee, D.H.; Seo, J.B. Effect of Surgical-Site, Multimodal Drug Injection on Pain and Stress Biomarkers in Patients Undergoing Plate Fixation for Clavicular Fractures. Clin. Orthop. Surg. 2018, 10, 455–461. [Google Scholar] [CrossRef]
- Reverdy, F. Combined interscalene-superficial cervical plexus block for clavicle surgery: An easy technique to avoid general anesthesia. Br. J. Anaesth. 2015, 115. [Google Scholar] [CrossRef]
- Banerjee, S.; Acharya, R.; Sriramka, B. Ultrasound-Guided Inter-scalene Brachial Plexus Block with Superficial Cervical Plexus Block Compared with General Anesthesia in Patients Undergoing Clavicular Surgery: A Comparative Analysis. Anesth. Essays Res. 2019, 13, 149–154. [Google Scholar]
- Gurumoorthi, P.; Mistry, T.; Sonawane, K.B.; Balasubramanian, S. Ultrasound guided selective upper trunk block for clavicle surgery. Saudi J. Anaesth. 2019, 13, 394–395. [Google Scholar] [PubMed]
- Pinto, L.D.C.; Silva, C.H.R.D.; Gonçalves, P.M.S.E.; Valadares, R.J. Bloqueio do nervo supraclavicular e do tronco superior para tratamento cirúrgico de fratura de clavícula em paciente portador de doença de Steinert–Relato de caso [Supraclavicular nerve and superior trunk block for surgical treatment of clavicle fracture in a patient with Steinert’s disease-Case report]. Rev. Bras. Anestesiol. 2019, 69, 99–103. [Google Scholar]
- Tran, D.Q.; Tiyaprasertkul, W.; González, A.P. Analgesia for clavicular fracture and surgery: A call for evidence. Reg. Anesth. Pain Med. 2013, 38, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.; Chin, K.J. Advances in regional anaesthesia and acute pain management: A narrative review. Anaesthesia 2020, 75 (Suppl. S1), e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, Q.; Zheng, Y.; Hu, Z.; Xiong, J.; Wu, Y.; Zheng, Y.; Wang, L. Ultrasound-Guided Clavipectoral Fascial Plane Block with Intermediate Cervical Plexus Block for Midshaft Clavicular Surgery: A Prospective Randomized Controlled Trial. Anesth. Analg. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ince, I.; Kilicaslan, A.; Roques, V.; Elsharkawy, H.; Valdes, L. Ultrasound-guided clavipectoral fascial plane block in a patient undergoing clavicular surgery. J. Clin. Anesth. 2019, 58, 125–127. [Google Scholar] [CrossRef]
- Atalay, Y.O.; Mursel, E.; Ciftci, B.; Iptec, G. Clavipectoral Fascia Plane Block for Analgesia after Clavicle Surgery. Rev. Esp. Anestesiol. Reanim. 2019, 66, 562–563. [Google Scholar] [CrossRef]
- Schuitemaker, R.J.B.; Sala-Blanch, X.; Rodriguez-Pérez, C.L.; Mayoral, R.J.T.; López-Pantaleon, L.A.; Sánchez-Cohen, A.P. The PECS II block as a major analgesic component for clavicle operations: A description of 7 case reports. Rev. Esp. Anestesiol. Reanim. 2018, 65, 53–58. [Google Scholar] [CrossRef]
- Neal, J.M.; Gerancher, J.C.; Hebl, J.R.; Ilfeld, B.M.; McCartney, C.J.; Franco, C.D.; Hogan, Q.H. Upper extremity regional anesthesia: Essentials of our current understanding, 2008. Reg. Anesth. Pain Med. 2009, 34, 134–170. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Ueshima, H.; Otake, H. Successful clavicle fracture surgery performed under selective supraclavicular nerve block using the new subclavian approach. JA Clin. Rep. 2016, 2, 34. [Google Scholar] [CrossRef] [Green Version]
- Rosales, A.L.; Aypa, N.S. Clavipectoral plane block as a sole anesthetic technique for clavicle surgery-A case report. Anesth. Pain Med. 2022, 17, 93–97. [Google Scholar] [CrossRef]
- Abdelghany, M.S.; Ahmed, S.A.; Afandy, M.E. Superficial cervical plexus block alone or combined with interscalene brachial plexus block in surgery for clavicle fractures: A randomized clinical trial. Minerva Anestesiol. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Niempoog, S.; Tanariyakul, Y.; Jaroenporn, W. Wide-awake local anesthesia for clavicle fracture fixation: A case report. Int. J. Surg. Case Rep. 2021, 79, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Arjun, B.K.; Vinod, C.N.; Puneeth, J.; Narendrababu, M.C. Ultrasound-guided interscalene block combined with intermediate or superficial cervical plexus block for clavicle surgery: A randomised double blind study. Eur. J. Anaesthesiol. 2020, 37, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Olofsson, M.; Taffé, P.; Kirkham, K.R.; Vauclair, F.; Morin, B.; Albrecht, E. Interscalene brachial plexus block for surgical repair of clavicle fracture: A matched case-controlled study. BMC Anesthesiol. 2020, 20, 91. [Google Scholar] [CrossRef] [Green Version]
- Ryan, D.J.; Iofin, N.; Furgiuele, D.; Johnson, J.; Egol, K. Regional anesthesia for clavicle fracture surgery is safe and effective. J. Should. Elbow Surg. 2021, 30, e356–e360. [Google Scholar] [CrossRef]
- Diwan, S.; Nair, A.; Sermeus, L.A.; Patil, A.A.; Attarde, D.S. Low-Volume Local Anesthetics for C5 and Supraclavicular Nerve Blocks for Mid and Lateral Clavicle Surgery: A Case Series. A A Pract. 2020, 14, e01322. [Google Scholar] [CrossRef]
- Ahmad, A.A.; Ubaidah Mustapa Kamal, M.A.; Ruslan, S.R.; Abdullah, S.; Ahmad, A.R. Plating of clavicle fracture using the wide-awake technique. J. Shoulder Elbow Surg. 2020, 29, 2319–2325. [Google Scholar] [CrossRef]
- Yoshimura, M.; Morimoto, Y. Use of clavipectoral fascial plane block for clavicle fracture: Two case reports. Saudi J. Anaesth. 2020, 14, 284–285. [Google Scholar] [CrossRef]
- Magalhães, J.; Segura-Grau, E. Single puncture clavipectoral fascial block as a potential effective analgesic strategy for clavicle surgery. J. Clin. Anesth. 2020, 67, 110062. [Google Scholar] [CrossRef]
- Kukreja, P.; Davis, C.J.; MacBeth, L.; Feinstein, J.; Kalagara, H. Ultrasound-Guided Clavipectoral Fascial Plane Block for Surgery Involving the Clavicle: A Case Series. Cureus 2020, 12, e9072. [Google Scholar] [CrossRef]
- Atalay, Y.O.; Ciftci, B.; Ekinci, M.; Yesiltas, S. The effectiveness of clavipectoral fascia plane block for analgesia after clavicle surgery: A report of five cases. Minerva Anestesiol. 2020, 86, 992–993. [Google Scholar] [CrossRef] [PubMed]
- Baran, O.; Kır, B.; Ateş, İ.; Şahin, A.; Üztürk, A. Combined supraclavicular and superficial cervical plexus block for clavicle surgery. Korean J. Anesthesiol. 2020, 73, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Sanllorente-Sebastián, R.; Pino-Gómez, S.; González-Romanillo, M.E.; María-Boal, L.; MacKenzie, E.X.; González-Barrera, V. PECS1 with superficial cervical plexus block for clavicle surgery analgesia. Minerva Anestesiol. 2020, 86, 683–684. [Google Scholar] [CrossRef]
- Ho, A.M.H.; Parlow, J.; Allard, R.; McMullen, M.; Mizubuti, G.B. Interscalene block in an anesthetized adult with hypertrophic obstructive cardiomyopathy undergoing clavicle fracture reduction. POCUS J. 2020, 5, 6–9. [Google Scholar]
- Beletsky, A.; Burton, B.N.; Swisher, M.W.; IV Finneran, J.J.; Gabriel, R.A. Utilization of regional anesthesia for open reduction and internal fixation of clavicular fractures is associated with increased same-day discharge and not readmissions. Reg. Anesth. Pain Med. 2020, 45, 716–719. [Google Scholar] [CrossRef]
- Gupta, N.; Gupta, V.; Kumar, G.; Gupta, D. Comparative Evaluation of Efficacy of Interscalene Block vs. Interscalene Block and Superficial Cervical Plexus Block for Fixation of Clavicular Fractures. Int. J. Contemp. Med. Res. 2019, 6, 11–13. [Google Scholar] [CrossRef]
- Kaciroglu, A.; Karakaya, M.A.; Ahiskalioglu, A.; Ciftci, B.; Ekinci, M.; Yayik, A.M. Ultrasound-guided combined interscalene and superficial cervical plexus blocks for anesthesia management during clavicle fracture surgery. Ain-Shams J. Anesthesiol. 2019, 11, 28. [Google Scholar] [CrossRef]
- Fugelli, C.G.; Westlye, E.T.; Ersdal, H.; Strand, K.; Bjørshol, C. Combined Interscalene Brachial Plexus and Superficial Cervical Plexus Nerve Block for Midshaft Clavicle Surgery: A Case Series. AANA J. 2019, 87, 374–378. [Google Scholar]
- Kiran Kumar, K.K.; Hyoju, S.; Raya, P.K.; Budhathoki, C.; Sharma, R.P.; Lamichhane, S.; Yadav, A. Combined Interscalene and Superficial cervical plexus block for clavicle surgery: Case series. Nepal Med. J. 2019, 01, 95–97. [Google Scholar]
- Ozen, V. Ultrasound-guided, combined application of selective supraclavicular nerve and low-dose interscalene brachial plexus block in a high-risk patient. Hippokratia 2019, 23, 25–27. [Google Scholar]
- Kim, H.; Jang, H.Y.; Heo, H.J.; Shin, Y.D.; Park, S.H.; Choi, J.H.; Kim, H.T.; Lee, H.M. Ipsilateral vocal cord paralysis after interscalene brachial plexus block for clavicle surgery: Anatomical considerations and technical recommendations-a case report. Int. J. Clin. Exp. Med. 2019, 12, 10132–10138. [Google Scholar]
- Paul, A.A.; Ranjan, R.V.; George, S.K.; Suranigi, S.M. Ultrasound Guided Superficial Cervical Plexus and Superior Trunk Interscalene Block as Sole Anaesthetic Technique for Acromioclavicular Joint Fixation Surgery. J. Clin. Diag Res. 2019, 13, UD01–UD02. [Google Scholar] [CrossRef]
- Rajbanshi, L.K.; Arjyal, B.; Bajracharya, A.; Khanal, K. Comparison of Ultrasound Guided Interscalene and Supraclavicular Brachial Plexus Block for Clavicle Fracture Surgery. J. Coll Med. Sci. Nepal. 2018, 14, 189–195. [Google Scholar] [CrossRef]
- Ho, B.; De Paoli, M. Use of Ultrasound-Guided Superficial Cervical Plexus Block for Pain Management in the Emergency Department. J. Emerg. Med. 2018, 55, 87–95. [Google Scholar] [CrossRef]
- Balaban, O.; Dülgeroğlu, T.C.; Aydın, T. Ultrasound-Guided Combined Interscalene-Cervical Plexus Block for Surgical Anesthesia in Clavicular Fractures: A Retrospective Observational Study. Anesthesiol. Res. Pract. 2018, 2018, 7842128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, B.R.; Sharma, P. Regional Anaesthesia in Clavicle Surgery. JNMA J. Nepal Med. Assoc. 2017, 56, 265–267. [Google Scholar] [CrossRef] [Green Version]
- Salvadores de Arzuaga, C.I.; Naya Sieiro, J.M.; Salmeron Zafra, O.; González Posada, M.A.; Marquez Martínez, E. Selective Low-Volume Nerve Block for the Open Surgical Fixation of a Midshaft Clavicle Fracture in a Conscious High-Risk Patient: A Case Report. A A Case Rep. 2017, 8, 304–306. [Google Scholar] [CrossRef]
- Contractor, H.U.; Shah, V.A.; Gajjar, V.A. Ultrasound guided superficial cervical plexus and interscalene brachial plexus block for clavicular surgery. Anaesth. Pain Intensive Care 2016, 20, 447–450. [Google Scholar]
- Flores, S.; Riguzzi, C.; Herring, A.A.; Nagdev, A. Horner’s Syndrome after Superficial Cervical Plexus Block. West. J. Emerg. Med. 2015, 16, 428–431. [Google Scholar] [CrossRef]
- Shanthanna, H. Ultrasound guided selective cervical nerve root block and superficial cervical plexus block for surgeries on the clavicle. Indian J. Anaesth. 2014, 58, 327–329. [Google Scholar] [CrossRef]
- Vandepitte, C.; Latmore, M.; O’Murchu, E.; Hadzic, A.; Van de Velde, M.; Nijs, S. Combined interscalene-superficial cervical plexus blocks for surgical repair of a clavicular fracture in a 15-week pregnant woman. Int. J. Obstet Anesth. 2014, 23, 194–195. [Google Scholar] [CrossRef] [PubMed]
- Dillane, D.; Ozelsel, T.; Gadbois, K. Anesthesia for clavicular fracture and surgery. Reg. Anesth. Pain Med. 2014, 39, 256. [Google Scholar] [CrossRef] [PubMed]
- Kuchyn, I.L. Interscalene brachial plexus block in patients with clavicle fractures: Randomized comparison of techniques with ultrasound guidance and neurostimulator. Novosti Khirurgii 2013, 21, 105–108. [Google Scholar] [CrossRef]
- Telford, R.J.; Stoneham, M.D. Correct nomenclature of superficial cervical plexus blocks. Br. J. Anaesth. 2004, 92, 775. [Google Scholar] [CrossRef] [Green Version]
- Nash, L.; Nicholson, H.D.; Zhang, M. Does the investing layer of the deep cervical fascia exist? Anesthesiology 2005, 103, 962–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, S.K.; Picton, P.; Shanks, A.; Dorje, P.; Pandit, J.J. Comparison of intermediate vs subcutaneous cervical plexus block for carotid endarterectomy. Br. J. Anaesth. 2011, 107, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Syal, K.; Chandel, A.; Goyal, A.; Sharma, A. Comparison of ultrasound-guided intermediate vs subcutaneous cervical plexus block for postoperative analgesia in patients undergoing total thyroidectomy: A randomised double-blind trial. Indian J. Anaesth. 2020, 64, 37–42. [Google Scholar]
- Choquet, O.; Dadure, C.; Capdevila, X. Ultrasound-guided deep or intermediate cervical plexus block: The target should be the posterior cervical space. Anesth. Analg. 2010, 111, 1563–1564. [Google Scholar] [CrossRef]
- Kline, J.P. Ultrasound-guided placement of combined superficial cervical plexus and selective C5 nerve root catheters: A novel approach to treating distal clavicle surgical pain. AANA J. 2013, 81, 19–22. [Google Scholar]
- Choi, D.S.; Atchabahian, A.; Brown, A.R. Cervical plexus block provides postoperative analgesia after clavicle surgery. Anesth. Analg. 2005, 100, 1542–1543. [Google Scholar]
- Moriggl, B. ESRA19-0712 Clavicle innervation and implications for regional anaesthesia. Reg. Anesth. Pain Med. 2019, 44, A63–A64. [Google Scholar]
- Fillingim, R.B. Individual differences in pain: Understanding the mosaic that makes pain personal. Pain 2017, 158 (Suppl. S1), S11–S18. [Google Scholar] [CrossRef] [Green Version]
- Leurcharusmee, P.; Maikong, N.; Kantakam, P.; Navic, P.; Mahakkanukrauh, P.; Tran, D. Innervation of the clavicle: A cadaveric investigation. Reg Anesth Pain Med. 2021, 46, 1076–1079. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Peng, P.W.H.; Agur, A.M.R. Anatomical study of the innervation of glenohumeral and acromioclavicular joint capsules: Implications for image-guided intervention. Reg. Anesth. Pain Med. 2019, 11, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Borbas, P.; Eid, K.; Ek, E.T.; Feigl, G. Innervation of the acromioclavicular joint by the suprascapular nerve. Should. Elbow. 2020, 12, 178–183. [Google Scholar] [CrossRef]
- Kihlström, C.; Möller, M.; Lönn, K.; Wolf, O. Clavicle fractures: Epidemiology, classification and treatment of 2 422 fractures in the Swedish Fracture Register; an observational study. BMC Musculoskelet Disord. 2017, 18, 82. [Google Scholar] [CrossRef] [Green Version]
- Curtis, R.J. Operative management of children’s fractures of the shoulder region. Orthop. Clin. N. Am. 1990, 21, 315–324. [Google Scholar] [CrossRef]
- Kubiak, R.; Slongo, T. Operative treatment of clavicle fractures in children: A review of 21 years. J. Pediatr. Orthop. 2002, 22, 736–739. [Google Scholar] [CrossRef]
- Morgan, R.J.; Bankston, L.S.; Hoenig, M.P.; Connor, P.M. Evolving management of middle-third clavicle fractures in the National Football League. Am. J. Sports Med. 2010, 38, 2092–2096. [Google Scholar]
- Pandya, N.K.; Namdari, S.; Hosalkar, H.S. Displaced clavicle fractures in adolescents: Facts, controversies, and current trends. J. Am. Acad. Orthop. Surg. 2012, 20, 498–505. [Google Scholar]
- Fanter, N.J.; Kenny, R.M.; Baker, C.L., 3rd; Baker, C.L., Jr. Surgical treatment of clavicle fractures in the adolescent athlete. Sports Health 2015, 7, 137–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, D.R.; Rubenstein, W.J.; Barnes, L.A.; Klion, M.J.; Gladstone, J.N.; Kim, J.M.; Cleeman, E.; Forsh, D.A.; Parsons, B.O. The Influence of Incision Type on Patient Satisfaction After Plate Fixation of Clavicle Fractures. Orthop. J. Sports Med. 2017, 5, 2325967117712235. [Google Scholar] [CrossRef] [PubMed]
- Chechik, O.; Batash, R.; Goldstein, Y.; Snir, N.; Amar, E.; Drexler, M.; Maman, E.; Dolkart, O. Surgical approach for open reduction and internal fixation of clavicle fractures: A comparison of vertical and horizontal incisions. Int. Orthop. 2019, 43, 1977–1982. [Google Scholar] [CrossRef]
- Hoogervorst, P.; van Dam, T.; Verdonschot, N.; Hannink, G. Functional outcomes and complications of intramedullary fixation devices for Midshaft clavicle fractures: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 395. [Google Scholar] [CrossRef] [PubMed]
- Boonard, M.; Sumanont, S.; Arirachakaran, A.; Sikarinkul, E.; Ratanapongpean, P.; Kanchanatawan, W.; Kongtharvonskul, J. Fixation method for treatment of unstable distal clavicle fracture: Systematic review and network meta-analysis. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 1065–1078. [Google Scholar] [CrossRef]
- Chin, K.J.; Lirk, P.; Hollmann, M.W.; Schwarz, S.K.W. Mechanisms of action of fascial plane blocks: A narrative review. Reg. Anesth. Pain Med. 2021, 46, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Valdés-Vilches, L. Analgesia for clavicular surgery/fractures. Symposia 01: Postoperative Analgesia for Orthopedic Upper and Lower limb Surgery. In Proceedings of the Symposium Conducted at the 36th Annual European Society of Regional Anaesthesia and Pain Therapy (ESRA) Congress, Lugano, Switzerland, 13–16 September 2017. [Google Scholar]
- Roqués, V.; Valdés, L.; Pradere, A. How I do it: PoCUS and fascial plane blocks. Video presented at: IS-09 Ask the Experts Interactive Session. Clavipectoral fascia plain block for clavicle surgery. In Proceedings of the Session Conducted at the 44th Annual Regional Anesthesiology and Acute Pain Medicine Meeting, Las Vegas, NV, USA, 13 April 2019. [Google Scholar]
- Desroches, J.; Belliveau, M.; Bilodeau, C.; Landry, M.; Roy, M.; Beaulieu, P. Pectoral nerves I block is associated with a significant motor blockade with no dermatomal sensory changes: A prospective volunteer randomized-controlled double-blind study. Can. J. Anaesth. 2018, 65, 806–812. [Google Scholar] [CrossRef] [Green Version]
- Kang, R.; Jeong, J.S.; Chin, K.J.; Yoo, J.C.; Lee, J.H.; Choi, S.J.; Gwak, M.S.; Hahm, T.S.; Ko, J.S. Superior Trunk Block Provides Noninferior Analgesia Compared with Interscalene Brachial Plexus Block in Arthroscopic Shoulder Surgery. Anesthesiology 2019, 131, 1316–1326. [Google Scholar] [CrossRef] [Green Version]
- Kurtzman, J.S.; Etcheson, J.I.; Koehler, S.M. Wide-awake Local Anesthesia with No Tourniquet: An Updated Review. Plast. Reconstr. Surg. Glob. Open. 2021, 9, e3507. [Google Scholar] [CrossRef]
- Tahir, M.; Chaudhry, E.A.; Zaffar, Z.; Anwar, K.; Mamoon, M.A.H.; Ahmad, M.; Jamali, A.R.; Mehboob, G. Fixation of distal radius fractures using wide-awake local anaesthesia with no tourniquet (WALANT) technique: A randomized control trial of a cost-effective and resource-friendly procedure. Bone Joint. Res. 2020, 9, 429–439. [Google Scholar] [CrossRef]
- Abd Hamid, M.H.; Abdullah, S.; Ahmad, A.A.; Narin Singh, P.S.G.; Soh, E.Z.F.; Liu, C.Y.; Sapuan, J. A Randomized Controlled Trial Comparing Wide-Awake Local Anesthesia With No Tourniquet (WALANT) to General Anesthesia in Plating of Distal Radius Fractures With Pain and Anxiety Level Perception. Cureus 2021, 13, e12876. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Chen, C.Y.; Lin, K.C.; Yang, S.W.; Tarng, Y.W.; Chang, W.N. Comparison of Wide-Awake Local Anesthesia No Tourniquet with General Anesthesia With Tourniquet for Volar Plating of Distal Radius Fracture. Orthopedics 2019, 42, e93–e98. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.S.; Chen, C.Y.; Lin, K.C.; Tarng, Y.W.; Hsu, C.J.; Chang, W.N. Open reduction and internal fixation of ankle fracture using wide-awake local anaesthesia no tourniquet technique. Injury 2019, 50, 990–994. [Google Scholar] [CrossRef]
- Evangelista, T.M.P.; Pua, J.H.C.; Evangelista-Huber, M.T.P. Wide-Awake Local Anesthesia No Tourniquet (WALANT) versus Local or Intravenous Regional Anesthesia with Tourniquet in Atraumatic Hand Cases in Orthopedics: A Systematic Review and Meta-Analysis. J. Hand Surg. Asian Pac. Vol. 2019, 24, 469–476. [Google Scholar] [CrossRef]
- Sonawane, K.; Dixit, H.; Balavenkatasubramanian, J.; Gurumoorthi, P. Uncovering secrets of the beauty bone: A comprehensive review of anatomy and regional anesthesia techniques of clavicle surgeries. Open J. Orthop. Rheumatol. 2021, 6, 19–29. [Google Scholar]
- Burckett-St Laurent, D.; Chan, V.; Chin, K.J. Refining the ultrasound-guided interscalene brachial plexus block: The superior trunk approach. Can. J. Anaesth. 2014, 61, 1098–1102. [Google Scholar] [CrossRef] [PubMed]

| Criteria |
|---|
| Inclusion |
| Any published primary prospective or retrospective studies, case reports, case series, conference abstracts Regional anesthesia technique(s) administered for clavicular pain in the context of a clavicle fracture or surgical procedure |
| Exclusion |
| Studies on non-human subjects |
| Cadaveric studies |
| Studies not reporting clinical data or patient outcome (e.g., editorials or technical descriptions) |
| Overlapping participant data |
| Retracted articles |
| Reference (Year), Country | Block Description | Needle Guidance | Original Description | Block Site (Needle Tip Position)/Description from Cited Literature |
|---|---|---|---|---|
| Superficial cervical plexus | ||||
| In-text | LM | Superficial | Subcutaneous infiltration along the posterior border of the SCM. |
| In-text | US | Superficial | Just beneath the skin, at the midpoint of the line joining the mastoid and clavicle. |
| In-text | LM | Superficial | Subcutaneous infiltration along the posterior border of the SCM. |
| In-text, image | US | Superficial | Scan plane along the long axis of the SCM. Hydrodissection along the superficial cervical plexus plane. Sonographic image provided, demonstrating LA deposition above the posterior border of the SCM. |
| Intermediate cervical plexus | ||||
| In-text | US | Intermediate | Along the posterior border of SCM, into the interfascial space between the SCM and the prevertebral fascia |
| In-text | US | Superficial | Just superficial to the prevertebral fascia. |
| In-text | US | Superficial vs. Intermediate | Study comparing SCPB vs. ICPB. SCPB consisted of subcutaneous infiltration along the posterior border of the SCM, while ICPB consisted of local anesthetic deposited after piercing the investing layer of cervical fascia. |
| In-text | US | Superficial | Needle inserted lateral to medial through the thyroid cartilage with the needle tip tracked under and positioned in the fascia deep to the SCM. |
| In-text | US | Superficial | Local anesthetic deposited under the posterolateral belly of the SCM; sonographic image provided. |
| In-text | US | Superficial | Infiltration at the posterior border of the SCM but superficial to the prevertebral fascia. |
| In-text | US | Superficial | Injection along the fascial plane separating the posterior border of the SCM and anterior scalene muscle. |
| In-text, image | US | Superficial | The needle is visualized in position just deep to the lateral border of the SCM with injectate seen tracking along the fascial plane. |
| In-text | US | Not specified | Plane block in the prevertebral fascia posterior to the SCM. Needle advanced along the posterior border of the SCM to the nerve point of the neck. |
| In-text, image | US | Superficial and intermediate | Both SCPB and ICPB was performed. Injection performed just beneath the skin at the lateral border of the SCM. Additionally, for the second case, injectate was deposited at the superficial cervical plexus (indicated on the provided image to be superficial to the prevertebral fascia and anterior and middle scalene muscles, and deep to the SCM). |
| In-text | US | Superficial | Beneath the posterior border of the SCM, above the prevertebral fascia, and avoiding excessive medial spread of the injectate. |
| In-text, image | US | Superficial | Injection between the anterior and middle scalene muscles, in the space posterior to the SCM. |
| In-text, image | US | Superficial | Injectate deposited under the SCM, in the fascial space between the SCM and levator scapulae muscles. |
| In-text | US | Superficial | Needle positioned just under the SCM, at the posterior border around the midpoint between C6 and the mastoid process. |
| In-text | US | Superficial | Injectate deposited deep to the prevertebral fascia between the SCM and anterior scalene muscles *. |
| Deep cervical plexus | ||||
| In-text | US | Superficial | Needle position under the SCM below the prevertebral fascia. |
| In-text | US | Superficial | Needle beneath the prevertebral fascia. |
| Technique not described or in insufficient detail | ||||
| NR | NR | Superficial | Not reported or directly referenced. |
| NR | US | Superficial | Not reported or directly referenced. |
| NR | LM | Superficial | Not reported or directly referenced. |
| NR | US | Superficial | Not reported or directly referenced. |
| NR | NR | Superficial | Not reported or directly referenced. |
| NR | US | Superficial | Not reported or directly referenced. |
| NR | Unclear, possibly US | Superficial | Not reported or directly referenced. |
| NR | NR | Deep and Superficial | Not reported. Superficial component described as a classic approach with reference to a single article †. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.C.M.; Beh, Z.Y.; Lua, C.B.; Peng, K.; Fathil, S.M.; Hou, J.-D.; Lin, J.-A. Regional Anesthetic and Analgesic Techniques for Clavicle Fractures and Clavicle Surgeries: Part 1—A Scoping Review. Healthcare 2022, 10, 1487. https://doi.org/10.3390/healthcare10081487
Lee CCM, Beh ZY, Lua CB, Peng K, Fathil SM, Hou J-D, Lin J-A. Regional Anesthetic and Analgesic Techniques for Clavicle Fractures and Clavicle Surgeries: Part 1—A Scoping Review. Healthcare. 2022; 10(8):1487. https://doi.org/10.3390/healthcare10081487
Chicago/Turabian StyleLee, Chang Chuan Melvin, Zhi Yuen Beh, Chong Boon Lua, Kailing Peng, Shahridan Mohd Fathil, Jin-De Hou, and Jui-An Lin. 2022. "Regional Anesthetic and Analgesic Techniques for Clavicle Fractures and Clavicle Surgeries: Part 1—A Scoping Review" Healthcare 10, no. 8: 1487. https://doi.org/10.3390/healthcare10081487