1. Introduction
Mental health problems are considered to be one of the leading causes of disability. Moreover, this problem is a threat to public health in the world’s population due to the progression of the pathology, the increase in prevalence, and the difficulties in therapeutic control [
1,
2]. In particular, depression and anxiety are considered to be highly relevant indicators of mental health, and can have a harmful effect on people who do not receive adequate treatment for these pathologies [
3].
Depression is a globally prevalent illness, affecting 3.8% of the population, which means that 280 million people worldwide suffer from depression [
4]. Symptoms of depression are related to lack of interest and energy, loss of concentration, and feelings of guilt and worthlessness [
5]. This pathology can negatively influence the affected person’s school, work, and family activities, where a worsening of the condition could lead to recurrent thoughts of death and even suicide [
6]. In Spain, the estimated social costs of depressive disorders in the Spanish population were EUR 6145 million, with an average cost per patient/year of EUR 3402 [
7].
In addition, research with adults shows that depression is a risk factor for cardiovascular disease [
8,
9]. Health indicators related to depressive symptoms in adolescence and early adulthood have begun to be identified. In this regard, it is suggested that depressive symptoms may be precursors of cardiovascular disease health risks [
10].
Depression and anxiety disorders are among the most prevalent and debilitating mental health conditions (3.8–25%) [
11]. There are several subtypes of anxiety disorders whose severity or impact can negatively affect an individual’s well-being and daily life, characterised by an aversive state of worry that becomes severe and persistent [
12]. If left untreated, the personal and social costs of anxiety are significant, associated with frequent primary and acute care visits, reduced work productivity, and impaired social relationships [
13]. Anxiety also influences cardiovascular disease, being associated with a 26% increase in the risk of coronary heart disease and a 48% increase in the risk of cardiac death [
14].
Tobacco is currently considered a global health risk factor. Tobacco use is the most important preventable cause of death in the world, due to its prevalence and its association with numerous causes of death [
15]. Cigarette smoke contains dozens of complex chemical substances that can give rise to relevant pathologies, such as 17 types of cancers (lung cancer being the most prominent), asthma, COPD, mental illness, and pulmonary fibrosis, as well as increasing the risk of coronary artery disease and atherosclerosis [
16,
17]. In Spain, 28.2% of men and 20.8% of women over the age of 16 were smokers in 2017 and, according to data from the National Statistics Institute (INE), diseases of the circulatory system, respiratory pathologies, and tumours were the main causes of death in the country, most of which were associated with tobacco use [
18].
The link between smoking and depression is consistent, as the action of smoking is associated with stress relief in the smoker [
19]. In several epidemiological studies, smoking is often comorbid with major depression [
20]. Furthermore, smoking has been found to increase the risk of depression [
21].
There is cross-sectional evidence that a variety of mental disorders (schizophrenia, depression, anxiety, bipolar disorder…) are related to detrimental health behaviours, such as low levels of physical activity (PA), poorer dietary and sleep patterns, and higher rates of smoking compared to healthy individuals [
22]. Physical inactivity and sedentary lifestyles have been shown to have potential detrimental effects on physical and mental health, and may have a negative impact on cognitive processes, such as memory and attention, and are a potential predictor of disorders, such as depression [
23]. In line with this fact, according to the World Health Organization (WHO) in 2020, regular PA reduces depressive and anxiety symptoms [
24,
25].
More specifically, people with established depression tend to have low levels of moderate to vigorous intensity PA and are less likely than healthy people to meet the recommended PA guidelines [
26,
27]. PA and exercise are recommended as possible treatments for depression and are introduced in guidelines as a complementary approach to other treatments for mild to moderate severity of illness [
28].
In relation to PA and anxiety, several studies in the general population show that people who engage in more PA have a lower risk of anxiety diagnosis and less frequent and less severe anxiety symptoms [
29,
30,
31,
32,
33,
34]. Physical inactivity has also been identified as a risk factor for the development of anxiety itself [
35].
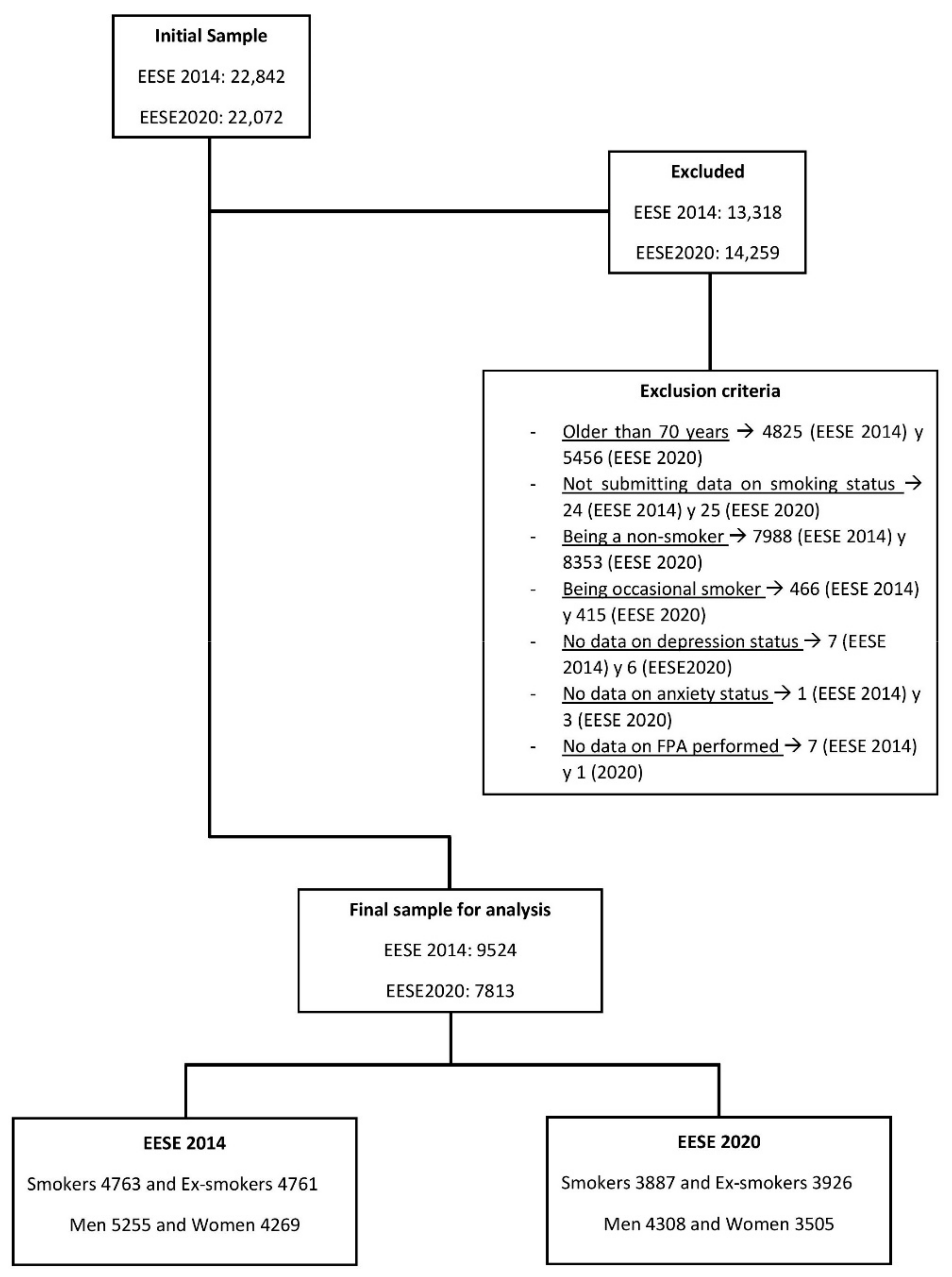
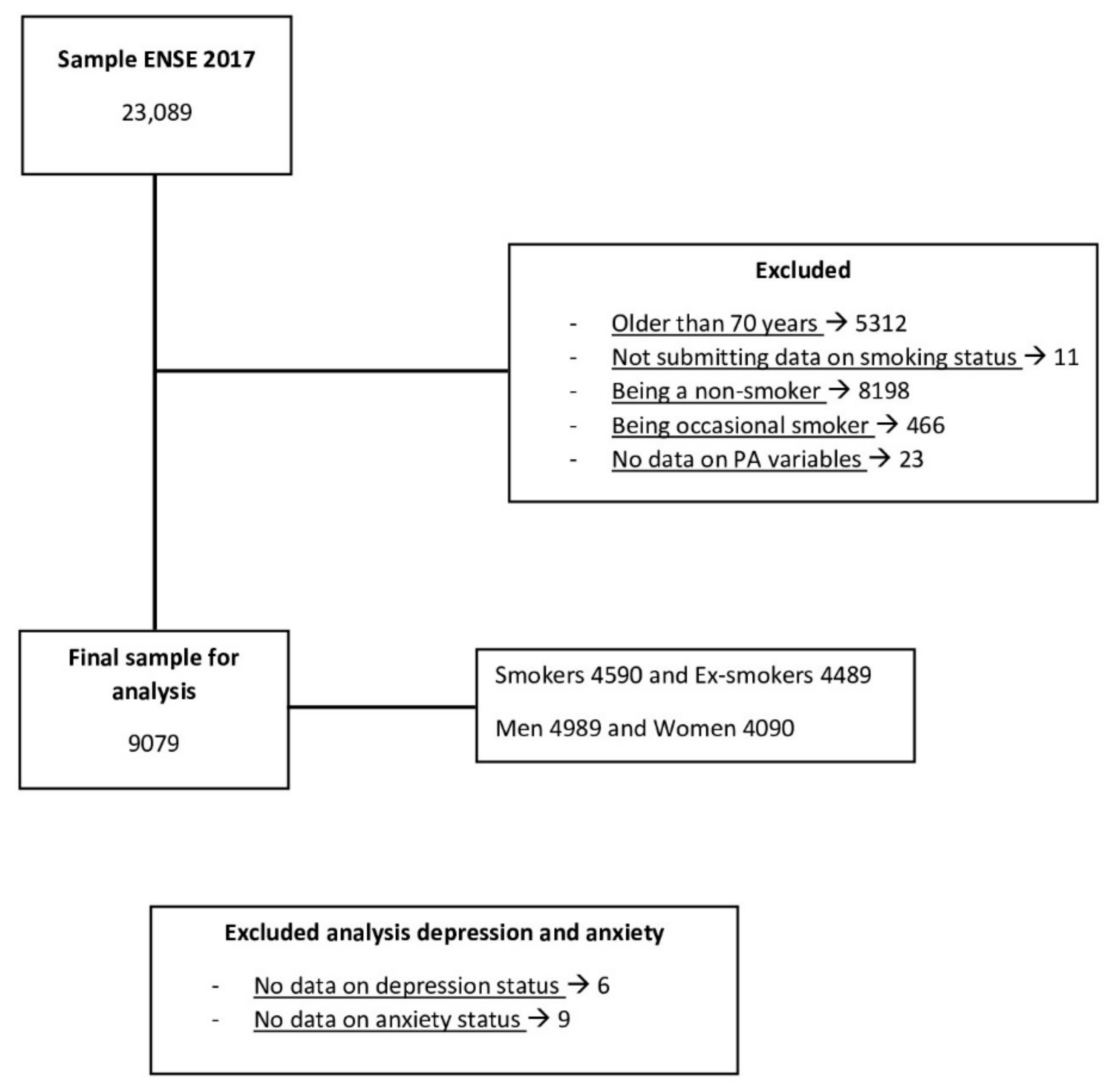
Therefore, the present study aims to (1) explore the prevalence of depression and anxiety in relation to sex and to the condition of smoker and ex-smoker, (2) study the possible differences in the proportions of prevalence of depression and anxiety according to the frequency (sub study 1) and level (sub study 2) of PA performed, as well as (3) calculate the risks of probability of presenting depression or anxiety in the population according to the frequency (sub study 1) and level (sub study 2) of PA performed.
According to these objectives, it is hypothesized that: (1) there will be dependency relationships between the levels of prevalence of depression and anxiety and sex in the Spanish population of smokers and ex-smokers; (2) differences in prevalence proportions will be found according to frequency (sub-study 1) and level (sub-study 2); and (3) there will be a greater risk of probability of presenting depression or anxiety in the population that performs PA less frequently.
4. Discussion
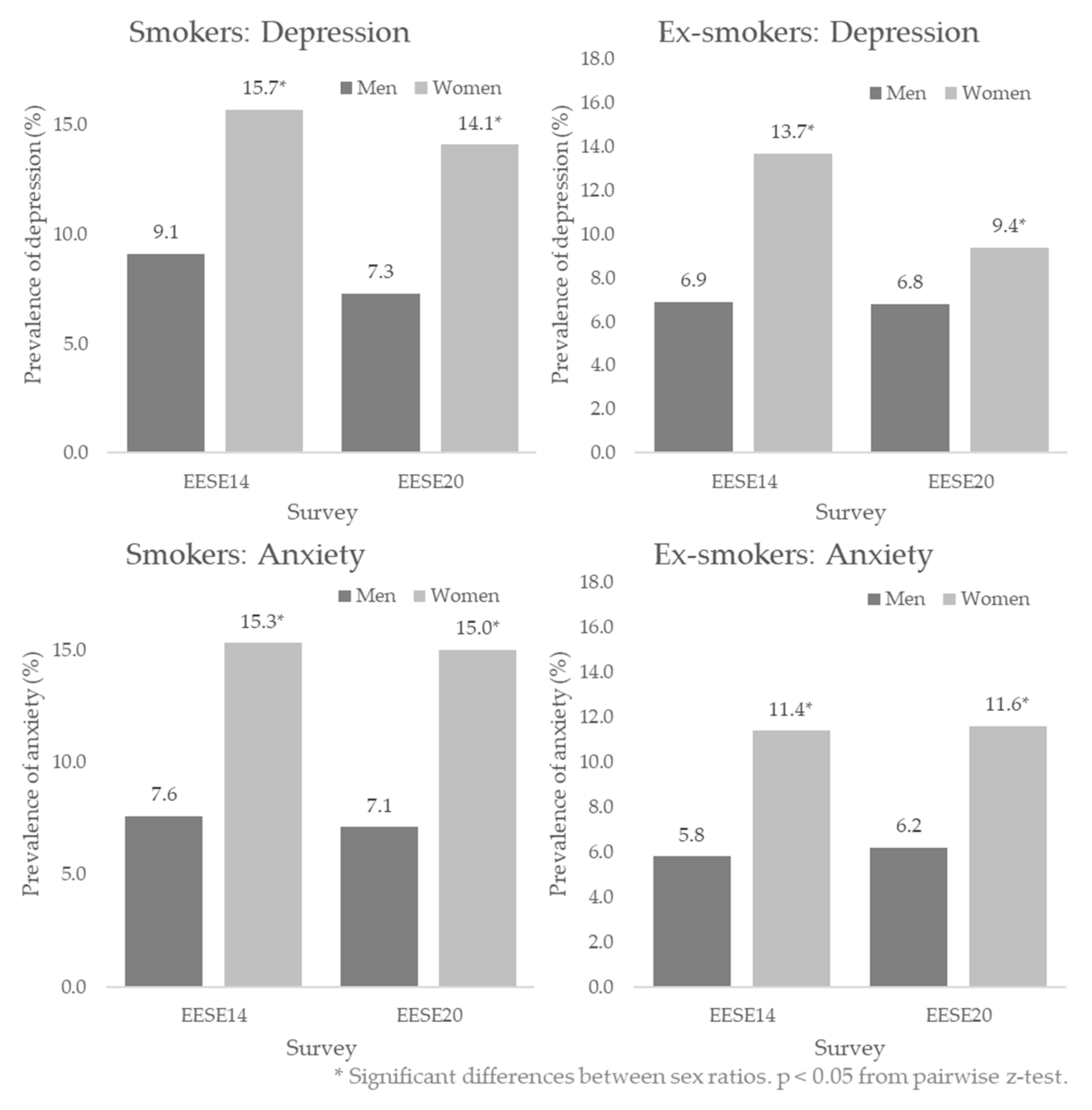
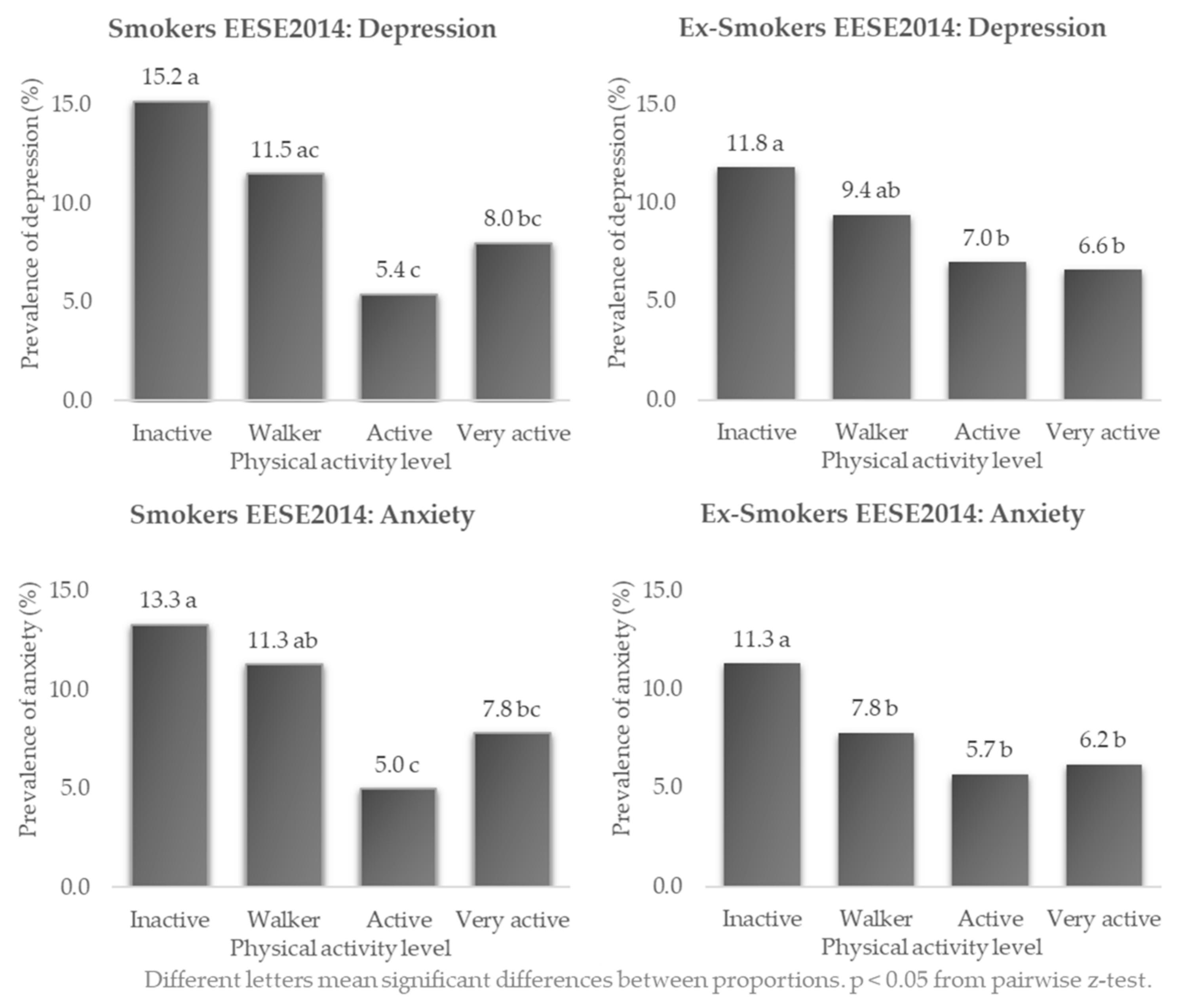
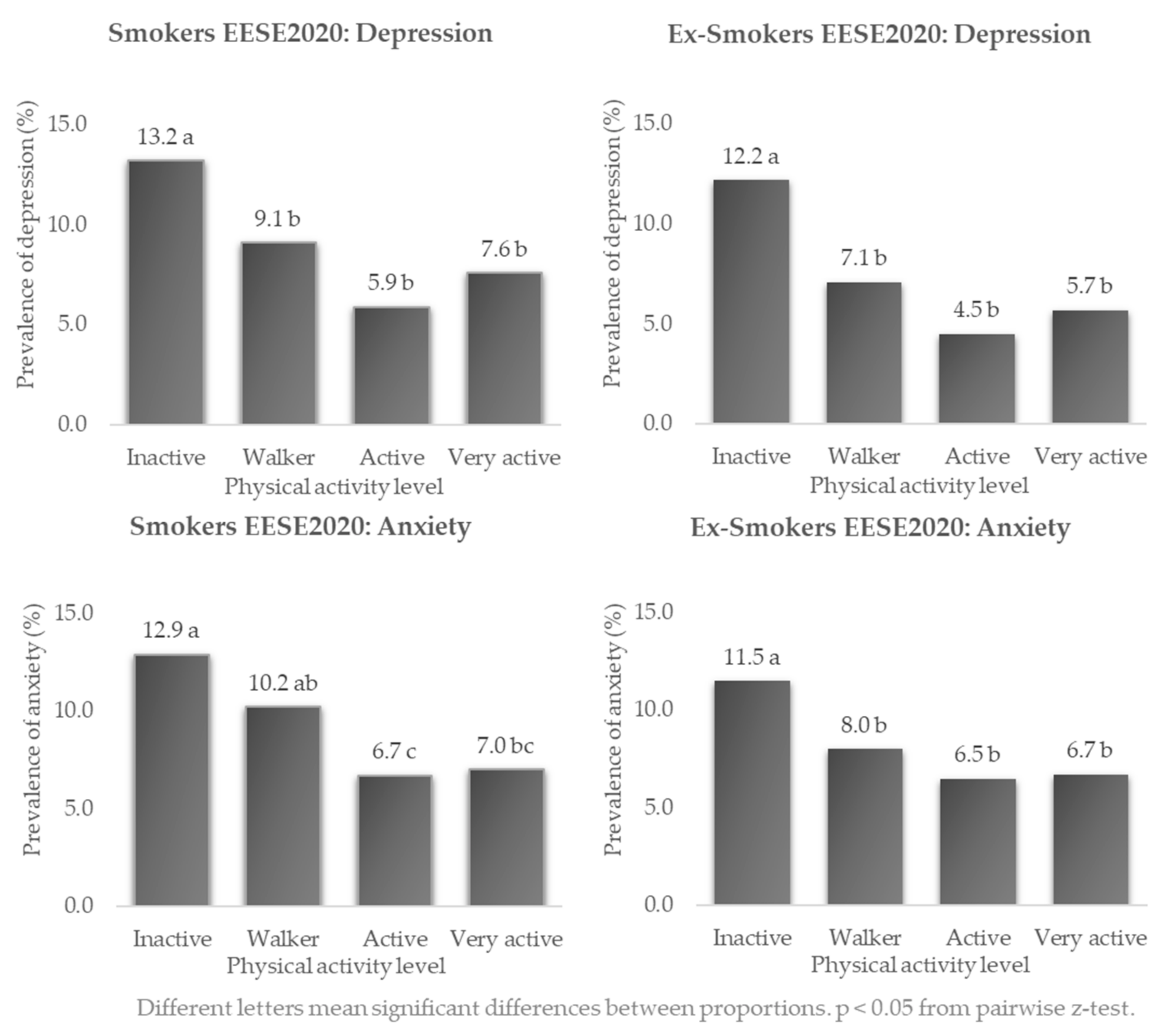
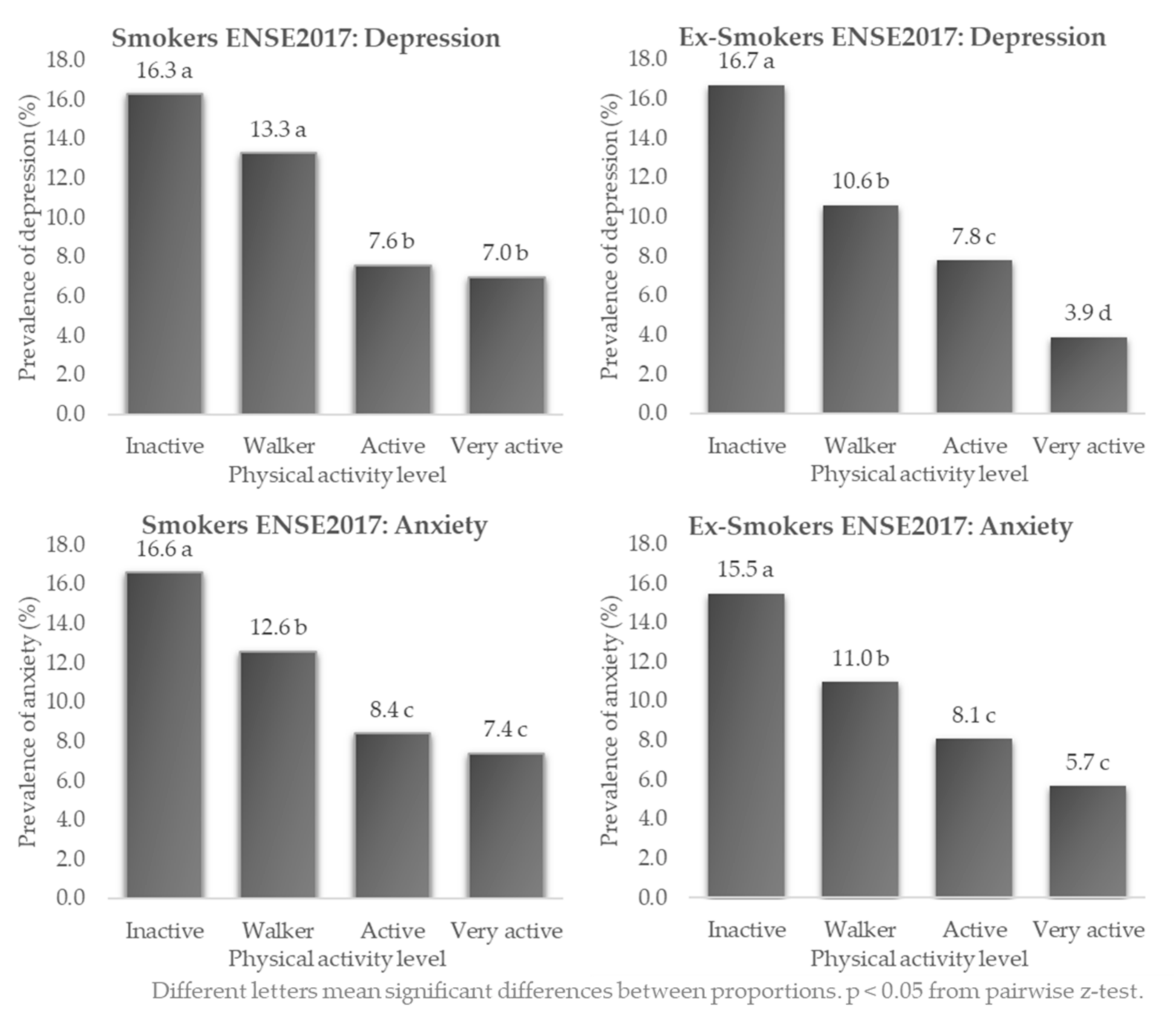
Among the main findings on the levels of prevalence of depression and anxiety in the Spanish smoking and ex-smoking population aged 15–70 years, dependence relationships between levels of prevalence and sex of the participants were shown. Thus, female smokers and ex-smokers had a significantly higher proportion of sufferers of depression and anxiety than men. Dependence relationships were also found between the prevalence of depression and anxiety with the frequency of PA (EESE 2014 and 2020) and the PA level (ENSE 2017) in smokers and ex-smokers. In general, levels of prevalence were higher in inactive versus very active or active people, whose differences in proportions were statistically significant. According to the data collected, being a smoker or ex-smoker and, in addition, being “inactive” from the point of view of PA could imply a higher risk of probability of suffering from depression and anxiety compared to “very active” people. Furthermore, in the EESE 2020 and in the ENSE 2017, the risk of depression was higher in ex-smokers than in smokers, with the highest risk in ex-smokers (OR: 4.91; 95%CI: 3.04–7.94) in the ENSE 2017. As for anxiety in the ENSE 2017, the risk of anxiety was also higher in ex-smokers than in smokers.
In both sub-study 1 and sub-study 2, in smokers and ex-smokers, a higher prevalence of depression (9.4–15.7% vs. 6.8–9.1%) and anxiety (11.4–16.3% vs. 5.8–7.9%) was found in women compared to men. Another study in the general population also found a higher prevalence of depression in women (12.5%) than in men (6.2%), in this case twice as high [
42].
A slightly higher prevalence of depression and anxiety in smokers than in ex-smokers was observed in all three surveys in the present study. Moreover, these results in both groups (depression 12% to 8%; anxiety 11.8% to 8.3%) can be considered slightly higher when compared to general population data in Spain from other studies. For example, in the study by Vieta et al., the mean annual prevalence of depression estimated during 2015–2017 was 4.73% [
7], and with the EESE 2020 where chronic anxiety was 5.8% and depression was 5.3% [
43]. Furthermore, if we compare the levels of prevalence of depression and anxiety in smokers and ex-smokers with other populations, such as older Spanish adults (people over 65 years of age), we observe that the overall prevalence of anxiety (11%) is similar to those in the present research [
44]. This may be due to the fact that older adults may interpret or experience affective terms differently and have a higher health concern than younger adults [
45]. In other pathologies, such as type 2 diabetes mellitus, the prevalence of depression was higher (20.03 %), these higher values are possibly associated with poor adherence to medication for blood glucose, blood pressure, and cholesterol, among other factors [
46,
47]. In inflammatory bowel disease, a non-curable condition, the levels of prevalence were higher (anxiety 32.1% and depression was 25.2%) [
48]. Thus, in smokers and ex-smokers, having an associated pathology may even increase the risk of depression or anxiety.
This is supported by Luger et al., who highlighted in their research that there were longitudinal associations between smoking and subsequent risk of depression across four meta-analyses of 19 studies for a total of 79,729 participants. In these, smoking significantly increased the risk of depression (smokers compared to never smokers), measured as diagnosed depressive disorders or cynically significant depressive symptoms on validated scales (OR = 1.62; 95 % CI: 1.1–2.4). A similar situation was found between smokers and ex-smokers, where smokers were more likely to be depressed than ex-smokers (OR = 1.76, 95 % CI: 1.48–2.09) [
49].
In relation to PA and the prevalence of depression and anxiety in both smokers and ex-smokers, the highest prevalence was found in inactive people, i.e., people who do not exercise and spend their free time doing sedentary activities. The highest prevalence of depression in all three surveys was found in inactive ex-smokers, with 16.7%, which is remarkable since the usual tendency was for smokers to have higher levels of prevalence than ex-smokers. The highest prevalence of anxiety was in inactive smokers, with 16.6%. In relation to other research, Galán-Arroyo et al. highlighted that, in the general population, the prevalence of depression and anxiety were associated with the frequency of PA. The highest levels of prevalence of depression were also found in the population that “never” performs PA (13.4%), however, these data were slightly lower than in the present study, as the main difference lay in the fact that they studied the general population, as opposed to the condition of being a smoker or ex-smoker in the present study [
42]. This study by Galán-Arroyo et al. also shows that there is a lower prevalence of depression in the “active” population, which is noteworthy as they have lower prevalence data than the “very active” population, as in our study. This could be due to the fact that excessive PA could lead to overtraining and trigger psychological symptoms that mimic depression [
50].
In this line, Schuch et al., in their meta-analysis of 36 prospective comparisons, observed that higher levels of PA significantly decreased the subsequent risk of depressive events during a mean follow-up time of 7 years (comparison between higher levels of PA with lower levels) (OR = 0.837, 95 % CI: 0.794 to 0.883) [
51], in their meta-analysis in 11 cohorts with a total of 69,037 participants, found that higher levels of PA significantly reduced incident anxiety (OR = 0.748, 95 % CI 0.629–0.889) over a follow-up period of 3.5 years [
52]. These data are consistent with those of the present study and the frequency of PA or the PA level where, compared to “very active” smokers and ex-smokers, “inactive” smokers had elevated risks of depression and anxiety.
As noted, physical inactivity may increase the likelihood of depression and anxiety, however, the possibility of reverse causality, i.e., that depression and anxiety are precursors of physical inactivity itself, should be considered, which was not taken into account in the present study. Hartanto et al. show an inverse causal relationship between social networks and depressive symptoms. Cross-sectional and correlational trend analyses appear to show increases in rates of depression along with increased participation in social networks. However, depressive symptoms may precede increased use of social networks, using them as an escape or for self-esteem reaffirmation through social validation [
53]. In relation to our research, depression and anxiety could precede physical inactivity, and symptoms of these mental illnesses could influence a possible demotivation towards PA, i.e., suffering from depression and anxiety could reduce the levels or frequency of PA. It would be interesting to study this assumption in future research as there is not much scientific evidence in this respect.
Therefore, increasing frequency of PA or PA level in smokers and ex-smokers could lead to a reduction in the risk of depression and anxiety. To this end, the possible practical implications of this study could be used by public administrations, as well as by national and regional health services, favouring the reduction in the prevalence of depression and anxiety in all age ranges through awareness campaigns focused on health promotion, training and educating people on the importance of PA to reduce the symptomatology of these mental illnesses.
Promoting an increase in frequency of PA or PA level in smokers and inactive ex-smokers would facilitate a decrease in the OR of developing depression or anxiety. Therefore, from the public sphere, it would be advisable to invest in health education throughout the life cycle, introducing sports science professionals in health services, who could prescribe physical exercise adapted to the needs of each patient. In addition, in the private (or public) sector, the inclusion by public organizations and/or companies of PA programmes based on active breaks could increase PA time in the workplace and/or in education. Therefore, these measures could have an impact on reducing the prevalence of these mental disorders for people who do not do PA due to lack of free time. It could even reduce health and social costs in the long term.
This study has a series of limitations, among them we can highlight the lack of differentiation between sexes in the study of the association of PA level with the risk of suffering from depression and anxiety. Therefore, a possible interesting future line of research would be to explore how PA variables affect each sex when differences in the prevalence of depression and anxiety between men and women are detected.
As this was a cross-sectional study, it was not possible to establish cause–effect relationships. It would be advisable to further explore the findings through other research to establish causal relationships. The study is based on self-reported PA data, and PA may be overestimated when measured subjectively. In subsequent studies, it would be innovative to include objective PA data from the participants, using appropriate methods and instruments. Furthermore, the type of training undertaken by each individual was not specified in the surveys, which may have a bearing on the risk of depression and anxiety
The study was based on self-reported depression and anxiety, and not on diagnostic tests, so the results could be affected. As these are national and European surveys, there are many factors and aspects that are collected within them, including for our research the questions and sections that were of most interest to us for the elaboration of this study. In future studies, it would be interesting to use other more complete or objective methods to assess the suffering from these mental illnesses, or even to include participants suffering from depression or anxiety from the outset, whose diagnosis has been made by a specialist.
Only male and female sex was considered, as non-binary sex was not taken into account. Whether participants were taking antidepressants was not taken into account. Other variables that could have an impact on depression, such as socio-demographic, socio-cultural and socio-economic biases of the participants, were also not included [
54]. In future studies, in order to analyse the influence of physical activity on the prevalence rates of depression and anxiety, it would be interesting to divide the sample according to the age ranges and social status of the participants, as other studies have shown that it could have an influence on the reduction or increase in these rates [
55].
Finally, another interesting future line of research would be to study the prevalence of depression and anxiety and their association with the level of PA in different pathologies, especially those that could be associated with smoking, such as COPD or other cardiorespiratory diseases.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





