
Malocclusions in Pediatric Patients with Asthma: A Case–Control Study


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asenjo, C.; Pinto, R. Function and anatomy of respiratory system during the childhood. Rev. Médica Clínica Las Condes. 2017, 28, 7–19. [Google Scholar] [CrossRef]
- Navarro-Torné, A.; Vidal, M.; Trzaska, D.K.; Passante, L.; Crisafulli, A.; Laang, H.; van de Loo, J.-W.; Berkouk, K.; Draghia-Akli, R. Chronic respiratory diseases and lung cancer research: A perspective from the European Union. Eur. Respir. J. 2015, 46, 1270–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Consultation on the Development of a Comprehensive Approach for the Prevention and Control of Chronic Respiratory Diseases, 11–13 January 2001, Geneva [Report]; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Ramos-Ríos, J.A.; Ramírez-Hernández, E.; Vázquez-Rodríguez, E.M.; Vázquez-Nava, F. Asthma-associated oral and dental health repercussions in children aged 6 to 12 years. Rev. Alerg. Mex. 2017, 64, 270–276. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of asthma in children and adults. Front. Pediatr. 2019, 7, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bacab, B.; Albertos Alpuche, N.E. Prevalence of asthma in schoolchildren in Merida, Yucatan. Rev. Panam. Salud Pública 1997, 2, 299–302. [Google Scholar]
- Del Río-Navarro, B.E.; Hidalgo-Castro, E.M.; Sienra-Monge, J.J.L. Asthma. Bol. Med. Hosp. Infant. Mex. 2009, 66, 3–33. [Google Scholar]
- Ocampo, J.; Gaviria, R.; Sánchez, J. Prevalence of asthma in Latin America. Critical look at ISAAC and other studies. Rev. Alerg. Mex. 2017, 64, 188–197. [Google Scholar] [CrossRef] [Green Version]
- Vargas Becerra, M.H. Epidemiology of asthma. NCT Neumol. y Cirugía Tórax 2009, 68, 91–97. [Google Scholar]
- Cherkasov, S.V.; Yu, L.; Tatyana, P.; Demina, R.R.; Khlopko, Y.A.; Balkin, A.S.; Plotnikov, A.O. Oral microbiomes in children with asthma and dental caries. Oral Dis. 2019, 25, 898–910. [Google Scholar] [CrossRef]
- Dong, J.; Li, W.; Wang, Q.; Chen, J.; Zu, Y.; Zhou, X.; Guo, Q. Relationships Between Oral Microecosystem and Respiratory Diseases. Front. Mol. Biosci. 2022, 8, 1–17. [Google Scholar] [CrossRef]
- Gani, F.; Caminati, M.; Bellavia, F.; Baroso, A.; Faccioni, P.; Pancera, P.; Batani, V.; Senna, G. Oral health in asthmatic patients: A review: Asthma and its therapy may impact on oral health. Clin. Mol. Allergy 2020, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Arafa, A.; Aldahlawi, S.; Fathi, A. Assessment of the oral health status of asthmatic children. Eur. J. Dent. 2017, 11, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Guo, L.; Gu, H.; Huo, Y.; Lin, H. Alterations in Oral–Nasal–Pharyngeal Microbiota and Salivary Proteins in Mouth-Breathing Children. Front. Microbiol. 2020, 11, 575550. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Kim, J.G.; Yang, Y. mi Influence of mouth breathing on atopic dermatitis risk and oral health in children: A population-based cross-sectional study. J. Dent. Sci. 2021, 16, 178–185. [Google Scholar] [CrossRef]
- Favero, L.; Arreghini, A.; Cocilovo, F.; Favero, V. Respiratory disorders in paediatric age: Orthodontic diagnosis and treatment in dysmetabolic obese children and allergic slim children. Eur. J. Paediatr. Dent. 2013, 14, 190–194. [Google Scholar]
- Rezende, G.; Dos Santos, N.M.L.; Stein, C.; Hilgert, J.B.; Faustino-Silva, D.D. Asthma and oral changes in children: Associated factors in a community of southern Brazil. Int. J. Paediatr. Dent. 2019, 29, 456–463. [Google Scholar] [CrossRef]
- Araújo, B.C.L.; de Magalhães Simões, S.; de Gois-Santos, V.T.; Martins-Filho, P.R.S. Association between mouth breathing and asthma: A systematic review and meta-analysis. Curr. Allergy Asthma Rep. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Yadav, P.K.; Saha, S.; Singh, S.; Gupta, N.D.; Agrawal, N.; Bharti, K. Oral health status and treatment needs of asthmatic children aged 6–12 Years in Lucknow. J. Indian Assoc. Public Health Dent. 2017, 15, 122. [Google Scholar] [CrossRef]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- García-Flores, G.; Figueroa, A.; Müller, V.; Agell, A. Relación entre las maloclusiones y la respiración bucal en pacientes que asistieron al servicio de otorrinolaringología del Hospital Pediátrico San Juan de Dios. Acta Odontológica Venez. 2007, 45, 407–409. [Google Scholar]
- Silva Pérez, G.A.; Bulnes López, R.M.; Rodríguez López, L.V. Prevalence of mouth breathing as an etiological factor in malocclusion in schoolchildren in the municipality of Centro, Tabasco. Rev. ADM 2014, 71, 285–289. [Google Scholar]
- Kumar, S.S.; Nandlal, B. Effects of Asthma and Inhalation corticosteroids on the dental arch morphology in children. J. Indian Soc. Pedod. Prev. Dent. 2012, 30, 242. [Google Scholar] [CrossRef] [PubMed]
- Aguilar Roldán, M.; Nieto Sánchez, I.; Pérez De la Cruz, J. Relación entre hábitos nocivos y maloclusiones en una muestra de 525 pacientes de Ortodoncia. Rev. Latinoam. Ortod. y Odontopediatría 2011, 5, 1–9. [Google Scholar]
- dos Santos, N.M.L.; Rezende, G.; da Silva, D.D.F.; Hugo, F.N.; Hilgert, J.B. Relationship between asthma, malocclusion and mouth breathing in primary health care children. Pesqui. Bras. Odontopediatria Clin. Integr. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Stensson, M.; Wendt, L.; Koch, G.; Oldaeus, G.; Birkhed, D. Oral health in preschool children with asthma. Int. J. Paediatr. Dent. 2008, 18, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Giraldo-Vélez, N.; Olarte-Sossa, M.; Ossa-Ramírez, J.E.; Parra-Isaza, M.A.; Tobón-Arango, F.E.; Agudelo-Suárez, A.A. Occlusion in 6-12 Year Old Mouth Breathers of the Child’s Clinic of the Faculty of Dentistry at Universidad de Antioquia. Rev. Nac. Odontol. 2015, 11, 21–29. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Barbieri, S.; Bruni, A.; Sinesi, A.; Ricci, M.; Trombini, J.; et al. Assessment of genetical, pre, peri and post natal risk factors of deciduous molar hypomineralization (Dmh), hypomineralized second primary molar (hspm) and molar incisor hypomineralization (mih): A narrative review. Children 2021, 8, 432. [Google Scholar] [CrossRef]
- Chambi-Rocha, A.; Cabrera-Domínguez, M.E.; Domínguez-Reyes, A. Breathing mode influence on craniofacial development and head posture. J. Pediatr. 2018, 94, 123–130. [Google Scholar] [CrossRef]
- Lopatienė, K.; Babarskas, A. Malocclusion and upper airway obstruction. Medicina 2002, 38, 277–283. [Google Scholar]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef]
- De Gois-Santos, V.T.; Santos, V.S.; Tavares, C.S.S.; Araújo, B.C.L.; Ribeiro, K.M.N.; Simões, S.D.M.; Martins-Filho, P.R. Association between deleterious oral habits and asthma in children: A systematic review and meta-analysis. Braz. Oral Res. 2022, 36, 1–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Frequency n (%) | |||
|---|---|---|---|---|
| Sagittal Plane | Transverse Plane | Vertical Plane | Oral Habits | |
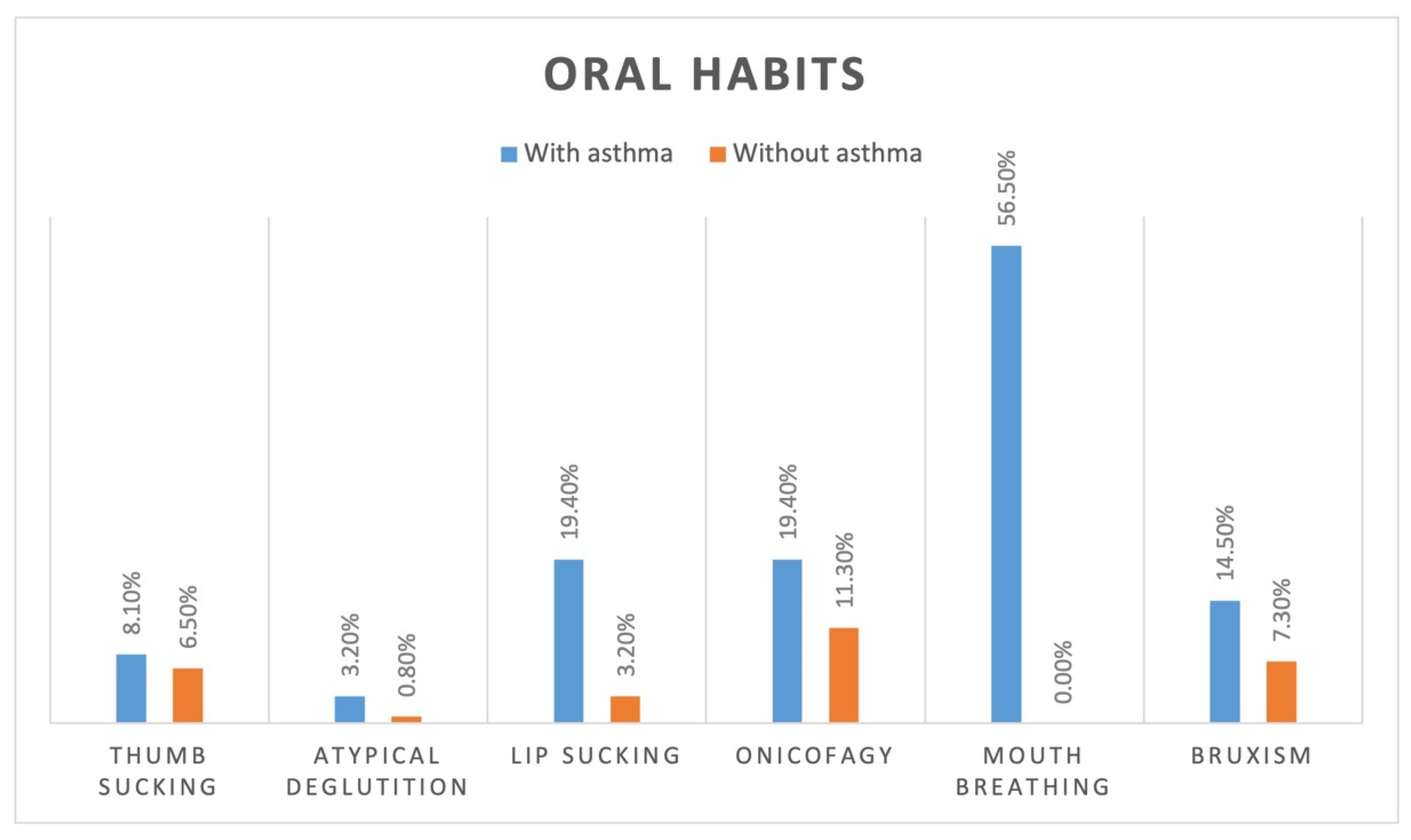
| WITH ASTHMA | 39 (90.7) | 9 (14.5) | 13 (21.0) | 47 (75.8) |
| WITHOUT ASTHMA | 86 (71.7) | 0 (0) | 5 (4.0) | 24 (19.4) |
| Variable | X2 | p | OR | 95% CI |
|---|---|---|---|---|
| Sagittal plane | 7.839 | 0.005 * | 2.424 | 1.241–4.826 |
| Transverse plane | - | <0.001 *,† | - | - |
| Vertical plane | 13.563 | <0.001 * | 6.244 | 1.959–23.605 |
| Oral habits | 55.811 | <0.001 * | 12.817 | 5.936–29.164 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castañeda-Zetina, J.; Chuc-Gamboa, M.G.; Aguilar-Pérez, F.J.; Pinzón-Te, A.L.; Zúñiga-Herrera, I.D.; Esparza-Villalpando, V. Malocclusions in Pediatric Patients with Asthma: A Case–Control Study. Healthcare 2022, 10, 1374. https://doi.org/10.3390/healthcare10081374
Castañeda-Zetina J, Chuc-Gamboa MG, Aguilar-Pérez FJ, Pinzón-Te AL, Zúñiga-Herrera ID, Esparza-Villalpando V. Malocclusions in Pediatric Patients with Asthma: A Case–Control Study. Healthcare. 2022; 10(8):1374. https://doi.org/10.3390/healthcare10081374
Chicago/Turabian StyleCastañeda-Zetina, Jocelyn, Martha Gabriela Chuc-Gamboa, Fernando Javier Aguilar-Pérez, Alicia Leonor Pinzón-Te, Iván Daniel Zúñiga-Herrera, and Vicente Esparza-Villalpando. 2022. "Malocclusions in Pediatric Patients with Asthma: A Case–Control Study" Healthcare 10, no. 8: 1374. https://doi.org/10.3390/healthcare10081374