
Evaluation of the Relationship between the Weight and Height Percentiles and the Sequence and Chronology of Eruption in Permanent Dentition



Abstract
:1. Introduction
2. Materials and Methods
2.1. Permits and Approvals
2.2. Study Design and Regional Area
2.3. Calibration of Examiners
2.4. Sample Size and Selection Criteria
2.5. Clinical-Physical Records
2.6. Primary and Secondary Covariates
2.7. Data Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Characteristics of Chronology and Eruption Sequence
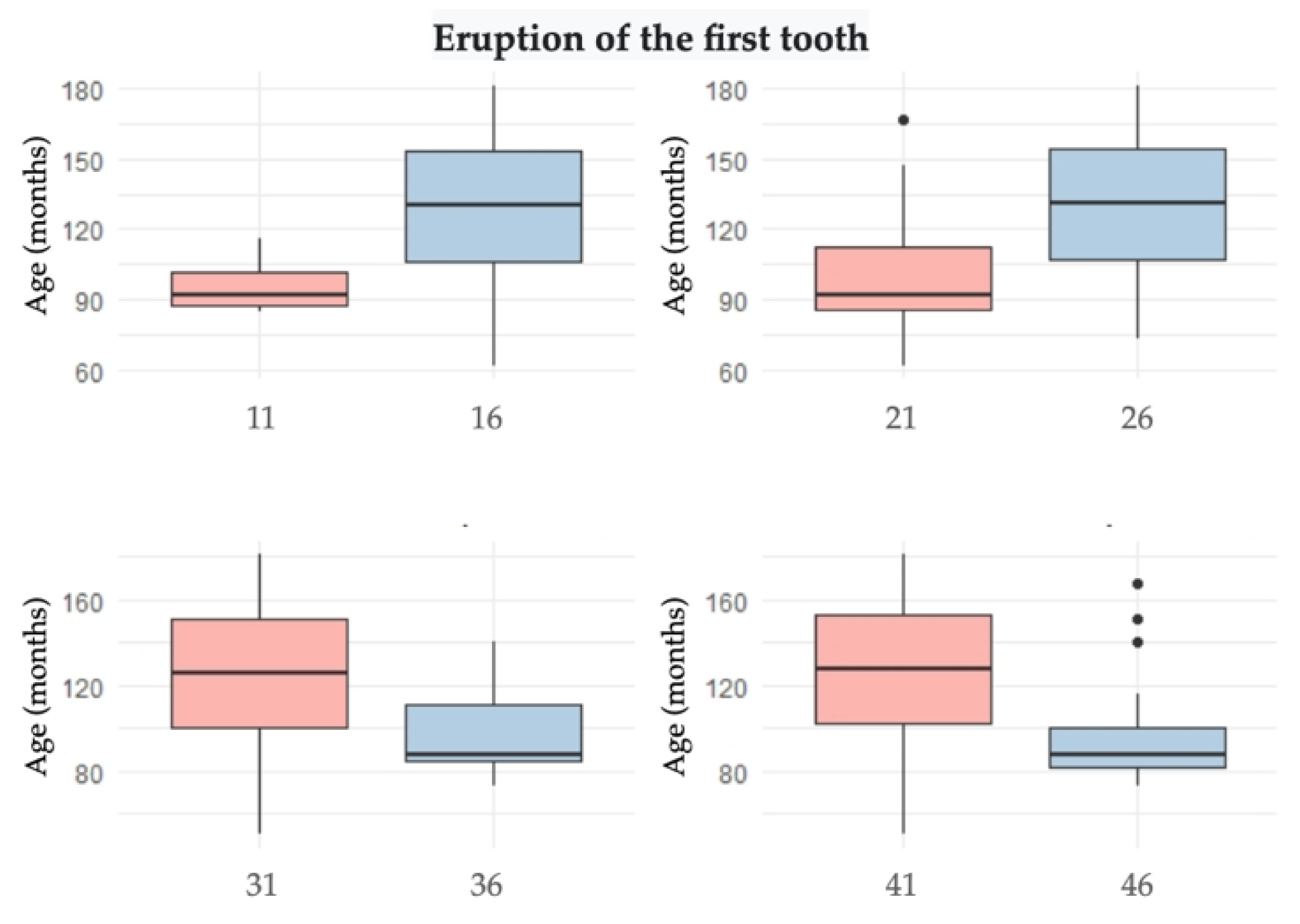
3.3. Characteristics of Eruption Symmetry
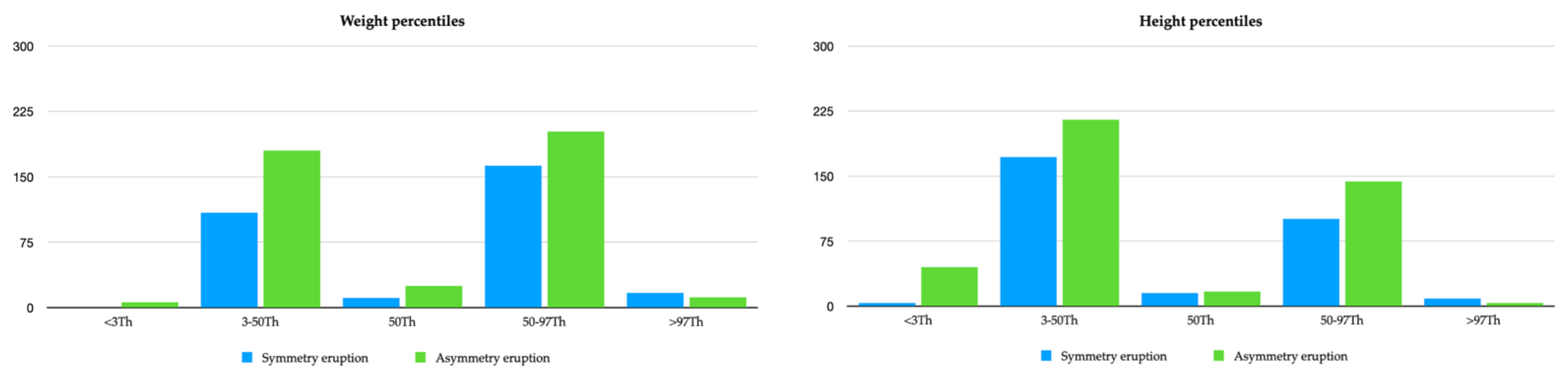
3.4. Characteristics of Weight and Height Percentiles
4. Discussion
4.1. Chronology and Sequence
4.2. Weight/Height
4.3. Association between Eruption and Weight and Height Percentiles
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goyal, A.; Khadgawat, R. Height Velocity Percentile Curves in Indian Children: Time to Move Beyond Standard Growth Charts. Indian Pediatr. 2019, 56, 19–20. [Google Scholar] [CrossRef]
- Hernández, M.; Espasa, E.; Boj, J.R. Eruption Chronology of the Permanent Dentition in Spanish children. J. Clin. Pediatr. Dent. 2008, 32, 347–350. [Google Scholar] [CrossRef]
- Agarwal, K.N.; Gupta, R.; Faridi, M.M.A.; Kaira, N. Permanent Dentition in Dheli Boys of Age 5–14 Years. Indian Pediatr. 2004, 41, 1031–1035. [Google Scholar]
- Heinrich-Weltzien, R.; Zorn, C.; Monse, B.; Kromeyer-Hauschild, K. Relationship between malnutrition and the number of permanent teeth in Filipino 10- to 13-year-olds. Biomed. Res. Int. 2013, 2013, 205950. [Google Scholar] [CrossRef]
- Wong, H.M.; Peng, S.M.; McGrath, C.P.J. Association of infant growth with emergence of permanent dentition among 12 year-aged southern Chinese school children. BMC Oral Health 2019, 19, 47. [Google Scholar] [CrossRef]
- De Onis, M.; Blössner, M. The World Health Organization Global Database on Child Growth and Malnutrition: Methodology and applications. Int. J. Epidemiol. 2003, 32, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Ugochukwu, E. Estimation of total muscle mass from simple anthropometric measurements for adults of Igbo ethnic group of South East Nigeria. Ann. Bioanthropol. 2016, 4, 111–117. [Google Scholar] [CrossRef]
- Abarrategui, I.; Gorritxo, B.G.F. Edades medias de erupción para la dentición permanente. Rev. Esp. Ortod. 2000, 30, 23–29. [Google Scholar]
- Plasencia, E.; García-Izquierdo, F.; Puente-Rodríguez, M. Edad de emergencia y secuencias polimórficas de la dentición permanente en una muestra de población de Asturias. Rcoe 2005, 10, 31–42. [Google Scholar] [CrossRef]
- Tunc, E.; Bayrak, S.; Tuloglu, N. Timing of permanent teeth eruption in Turkish children. J. Clin. Pediatr. Dent. 2012, 37, 207–211. [Google Scholar]
- Cecere, S.; Leroy, R.; Groenen, P.J.F.; Lesaffre, E.D.D. Estimating emergence sequences of permanent teeth in Flemish schoolchildren using interval-censored biplots: A graphical display of tooth emergence sequences. Community Dent. Oral Epidemiol. 2012, 40, 50–56. [Google Scholar] [CrossRef]
- Khan, H.; Khan, N.; Baloch, M.; Abbasi, S.A. Effect of Diet on Eruption Times for Permanent Teeth. Pediatr. Dent. 2020, 40, 24–30. [Google Scholar]
- Psoter, W.; Gebrian, B.; Prophete, S.; Reid, B.; Katz, R. Effect of early childhood malnutrition on tooth eruption in Haitian adolescents. Community Dent. Oral Epidemiol. 2007, 36, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Gaur, R.; Boparai, G.; Saini, K. Effect of under-nutrition on permanent tooth emergence among Rajputs of Himachal Pradesh, India. Ann. Hum. Biol. 2011, 38, 84–92. [Google Scholar] [CrossRef]
- Evangelista, S.E.S.; Vasconcelos, K.R.F.; Xavier, T.A.; Oliveira, S.; Dutra, A.L.T.; Nelson-Filho, P.; Silva, L.A.B.D.; Segato, R.A.B.; Queiroz, A.M.; Küchler, E.C. Timing of permanent tooth emergence is associated with overweight/obesity in children from the Amazon region. Braz. Dent. J. 2018, 29, 465–468. [Google Scholar] [CrossRef] [Green Version]
- Linas, N.; Peyron, M.A.; Hennequin, M.; Eschevins, C.; Nicolas, E.; Delfosse, C.C.V. Masticatory behavior for different solid foods in preschool children according to their oral state. J. Texture Stud. 2019, 50, 224–236. [Google Scholar] [CrossRef]
- Bruna del Cojo, M.; Gallardo López, N.E.; Mourelle Martínez, M.R.; De Nova García, M.J. Time and sequence of eruption of permanent teeth in spanish children. Eur. J. Paediatr. Dent. 2013, 14, 101–103. [Google Scholar]
- Wedl, J.S.; Danias, S.; Schmelzle, R.; Friedrich, R.E. Eruption times of permanent teeth in children and young adolescents in Athens (Greece). Clin. Oral Investig 2005, 9, 131–134. [Google Scholar] [CrossRef]
- Wedl, J.S.; Schoder, V.; Blake, F.A.S.; Schmelzle, R.; Friedrich, R.E. Eruption times of permanent teeth in teenage boys and girls in Izmir. J. Clin. Forensic Med. 2004, 11, 299–302. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Center for Healt Statistics. Available online: https://www.cdc.gov/growthcharts/clinical_charts.htm (accessed on 12 January 2022).
- Centro Nacional para la Prevención de Enfermedades Crónicas y Promoción de la Salud, División de Nutrición AF y O. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/healthyweight/spanish/bmi/calculator.html (accessed on 12 January 2022).
- William, H.G.; Logan, R.K.M. Development of the Human Jaws and Surrounding Structures from Birth to the Age of Fifteen Years. J. Am. Dent. Assoc. 1933, 20, 428–438. [Google Scholar]
- Kutesa, A.; Nkamba, E.M.; Muwazi, L.; Buwembo, W.; Rwenyonyi, C.M. Weight, height and eruption times of permanent teeth of children aged 4–15 years in Kampala, Uganda. BMC Oral Health 2013, 13, 15. [Google Scholar] [CrossRef] [Green Version]
- Dashash, M.; Al-Jazar, N. Timing and sequence of emergence of permanent teeth in Syrian schoolchildren. J. Investig. Clin. Dent. 2018, 9, e12311. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, R.E.; Habib, S.S.H. Eruption times of permanent teeth in children and adolescents in Latakia (Syria). Arch. Kriminol. 2009, 223, 84–97. [Google Scholar] [PubMed]
- Lakshmappa, A.; Guledgud, M.V.P.K. Eruption times and patterns of permanent teeth in school children of India. Indian J. Dent. Res. 2011, 22, 755–763. [Google Scholar] [PubMed]
- Nizam, A.; Naing, L.; Mokhtar, N. Age and sequence of eruption of permanent teeth in Kelantan, north-eastern Malaysia. Clin. Oral Investig. 2003, 7, 222–225. [Google Scholar] [CrossRef]
- Mugonzibwa, E.A.; Kuijpers-Jagtman, A.M.; Laine-Alava, M.T.V.H.M. Emergence of permanent teeth in Tanzanian children. Community Dent. Oral Epidemiol. 2002, 30, 455–462. [Google Scholar] [CrossRef]
- Moslemi, M. An epidemiological survey of the time and sequence of eruption of permanent teeth in 4–15-year-olds in Tehran, Iran. Int. J. Paediatr. Dent. 2004, 14, 432–438. [Google Scholar] [CrossRef]
- Oz, E.; Kırzıoglu, Z. Emergence stages of permanent teeth in twins: A comparative study. Int. J. Paediatr. Dent. 2020, 30, 468–477. [Google Scholar] [CrossRef]
- Makino, E.; Tsujino, K.; Ishii, T.; Shintani, S.; Sueishi, K. Difference in Bilateral Timing of Eruption of Permanent Teeth. Bull. Tokyo Dent. Coll 2018, 59, 277–284. [Google Scholar] [CrossRef] [Green Version]
- Leroy, R.; Bogaerts, K.; Lesaffre, E.; Declerck, D. The emergence of permanent teeth in Flemish children. Community Dent. Oral Epidemiol. 2003, 31, 30–39. [Google Scholar] [CrossRef]
- Shaweesh, A.I. Timing and sequence of emergence of permanent teeth in the Jordanian population. Arch. Oral Biol. 2012, 57, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Šindelárová, R.; Žáková, L.; Broukal, Z. Standards for permanent tooth emergence in Czech children. BMC Oral Health 2017, 17, 44–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedl, J.S.; Schmelzle, R.; Friedrich, R.E. The eruption times of permanent teeth in boys and girls in the Stormarn District, Schleswig-Holstein (Germany). Anthropol. Anz. 2005, 63, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Nyström, M.; Kleemola-Kujala, E.; Evälahti, M.; Peck, L.; Kataja, M. Emergence of permanent teeth and dental age in a series of Finns. Acta Odontol. Scand. 2001, 59, 49–56. [Google Scholar] [CrossRef]
- Gupta, R.; Sivapathasundharam, B.; Einstein, A. Eruption age of permanent mandibular first molars and central incisors in the south Indian population. Indian J. Dent. Res. 2007, 18, 186–189. [Google Scholar]
- Triratana, T.; Kiatiparjuk, C. Eruption of permanent teeth in malnutrition children. J. Dent. Assoc. Thai 1990, 40, 100–108. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Tooth * | n | % | Mean Age (Years and Months) | p-Value ** |
|---|---|---|---|---|
| 1.1 | 520 | 71.7 | 11.1 | 4.34 × 10−8 |
| 2.1 | 505 | 69.6 | 11.1 | |
| 3.1 | 607 | 83.7 | 10.4 | |
| 4.1 | 580 | 80.0 | 10.6 | |
| 1.2 | 441 | 60.8 | 11.6 | 0.0085 |
| 2.2 | 438 | 60.4 | 11.6 | |
| 3.2 | 484 | 66.7 | 11.3 | |
| 4.2 | 484 | 66.7 | 11.3 | |
| 1.3 | 202 | 27.8 | 13.2 | 1.9 × 10−11 |
| 2.3 | 194 | 26.7 | 13.2 | |
| 3.3 | 298 | 41.1 | 12.5 | |
| 43 | 294 | 40.5 | 12.5 | |
| 14 | 268 | 36.9 | 12.7 | 0.0906 |
| 24 | 266 | 36.6 | 12.8 | |
| 34 | 236 | 32.5 | 13.0 | |
| 44 | 242 | 33.3 | 13.0 | |
| 15 | 193 | 26.6 | 13.2 | 0.474 |
| 25 | 191 | 26.3 | 13.2 | |
| 35 | 177 | 24.4 | 13.4 | |
| 45 | 186 | 25.6 | 13.3 | |
| 16 | 556 | 76.6 | 10.8 | 0.836 |
| 26 | 542 | 74.7 | 10.9 | |
| 36 | 559 | 77.1 | 10.8 | |
| 46 | 558 | 76.9 | 10.8 | |
| 17 | 122 | 16.8 | 13.6 | 0.223 |
| 27 | 123 | 16.9 | 13.8 | |
| 37 | 148 | 20.4 | 13.8 | |
| 47 | 142 | 19.5 | 13.6 |
| PERCENTILE (Th) (Weight and Height) | <3 Th | 3–50 Th | 50 Th | 50–97 Th | >97 Th | p-Value * | |
|---|---|---|---|---|---|---|---|
| n (%) Age (years) | Girls | 2 (0.5) | 169 (46.0) | 15 (4.0) | 172 (46.8) | 9 (2.4) | 0.0031 |
| 7.2 | 9.4 | 9.7 | 10.1 | 10.5 | |||
| Boys | 4 (1.1) | 120 (33.5) | 21 (5.8) | 193 (53.9) | 20 (5.5) | ||
| 7.6 | 9.8 | 10.0 | 9.8 | 9.5 | |||
| Total | 6 (0.8) | 289 (39.8) | 36 (4.9) | 365 (50.3) | 29 (4.0) | ||
| 7.4 | 9.6 | 9.9 | 10.0 | 9.8 | |||
| Girls | 25 (6.8) | 227 (61.8) | 13 (3.5) | 100 (27.2) | 2 (0.5) | 2.1 × 10−5 | |
| 6.6 | 10.0 | 10.4 | 9.8 | 13.7 | |||
| Boys | 24 (6.7) | 160 (44.6) | 19 (5.3) | 145 (40.5) | 10 (2.7) | ||
| 6.8 | 10.1 | 9.3 | 9.7 | 12.2 | |||
| Total | 49 (6.7) | 387 (53.3) | 32 (4.4) | 245 (33.7) | 12 (1.66) | ||
| 6.7 | 10.1 | 9.8 | 9.8 | 12.5 | |||
| Weight Percentiles | Height Percentiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3, 50, and 97 | <3 and >97 | p-Value | 3, 50, and 97 | <3 and >97 | p-Value | |||||
| No | Yes | No | Yes | No | Yes | No | Yes | |||
| 11 | 192 (27.8) | 498 (72.2) | 13 (37.1) | 22 (62.9) | 0.2498 | 165 (24.8) | 499 (75.2) | 40 (65.6) | 21 (34.4) | 2.35 × 10−10 |
| 21 | 207 (30.0) | 483 (70.0) | 13 (37.1) | 22 (62.9) | 0.3537 | 181 (27.2) | 483 (72.8) | 39 (63.9) | 22 (36.1) | 1.7 × 10−8 |
| 31 | 110 (15.9) | 580 (84.1) | 8 (22.8) | 27 (77.2) | 0.3443 | 91 (13.7) | 573 (86.3) | 27 (44.2) | 34 (55.8) | 4.97 × 10−8 |
| 41 | 137 (19.8) | 553 (80.2) | 8 (22.8) | 27 (77.2) | 0.6658 | 114 (17.7) | 550 (82.3) | 31 (50.9) | 30 (49.1) | 1.5 × 10−8 |
| 12 | 270 (39.1) | 20 (60.8) | 14 (40.0) | 21 (60.0) | 1 | 244 (36.7) | 420 (63.2) | 40 (65.6) | 21 (34.4) | 1.55 × 10−5 |
| 22 | 273 (39.5) | 417 (60.5) | 14 (40.0) | 21 (60.0) | 1 | 247 (37.2) | 417 (62.8) | 40 (65.6) | 21 (34.4) | 2.8 × 10−5 |
| 32 | 227 (32.9) | 463 (67.1) | 14 (40.0) | 21 (60.0) | 0.432 | 201 (30.2) | 463 (69.7) | 40 (65.6) | 21 (34.4) | 1.03 × 10−7 |
| 42 | 227 (32.9) | 463 (67.1) | 14 (40.0) | 21 (60.0) | 0.432 | 200 (30.1) | 464 (69.8) | 41 (67.3) | 20 (32.7) | 1.8 × 10−8 |
| Weight Percentiles | Height Percentiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3, 50, and 97 | <3 and >97 | p-Value | 3, 50, and 97 | <3 and >97 | p-Value | |||||
| No | Yes | No | Yes | No | Yes | No | Yes | |||
| 13 | 501 (72.7) | 189 (27.3) | 22 (62.9) | 13 (37.1) | 0.2454 | 476 (71.7) | 188 (28.3) | 47 (77.1) | 14 (22.9) | 0.4559 |
| 23 | 508 (73.7) | 182 (26.3) | 23 (65.8) | 12 (34.2) | 0.3284 | 484 (72.9) | 180 (27.1) | 47 (77.1) | 14 (22.9) | 0.5476 |
| 33 | 407 (59.0) | 293 (41.0) | 20 (57.2) | 15 (43.8) | 0.8613 | 382 (59.6) | 282 (42.4) | 45 (37.8) | 16 (26.2) | 0.0142 |
| 43 | 411 (59.6) | 279 (40.4) | 20 (57.2) | 15 (43.8) | 0.8603 | 386 (58.2) | 278 (41.8) | 45 (37.8) | 16 (26.2) | 0.0200 |
| Weight Percentiles | Height Percentiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3, 50, and 97 | <3 and >97 | p-Value | 3, 50, and 97 | <3 and >97 | p-Value | |||||
| No | Yes | No | Yes | No | Yes | No | Yes | |||
| 14 | 437 (63.4) | 253 (36.6) | 20 (57.2) | 15 (42.8) | 0.4763 | 412 (62.1) | 252 (37.9) | 45 (73.8) | 16 (26.2) | 0.0728 |
| 24 | 439 (63.8) | 251 (36.3) | 20 (57.2) | 15 (42.8) | 0.4740 | 413 (62.2) | 251 (37.8) | 46 (75.5) | 15 (24.5) | 0.0511 |
| 34 | 468 (67.9) | 222 (37.1) | 21 (60.0) | 14 (40.0) | 0.3574 | 444 (66.9) | 220 (31.1) | 45 (73.8) | 16 (26.2) | 0.3185 |
| 44 | 462 (66.8) | 228 (33.2) | 21 (60.0) | 14 (40.0) | 0.4625 | 437 (65.9) | 227 (34.1) | 46 (75.5) | 15 (24.5) | 0.1558 |
| 15 | 507 (73.5) | 183 (25.5) | 21 (71.5) | 10 (28.5) | 0.8447 | 484 (72.9) | 180 (27.1) | 48 (78.7) | 13 (21.3) | 0.3669 |
| 25 | 510 (74.6) | 180 (25.4) | 24 (68.6) | 11 (31.4) | 0.5549 | 488 (73.5) | 176 (26.5) | 46 (75.6) | 15 (24.4) | 0.8794 |
| 35 | 526 (76.3) | 164 (23.7) | 22 (62.9) | 13 (37.1) | 0.1038 | 502 (75.6) | 162 (24.4) | 46 (75.6) | 15 (24.4) | 1 |
| 45 | 516 (74.8) | 174 (52.2) | 23 (65.8) | 12 (34.2) | 0.2368 | 493 (74.3) | 171 (25.7) | 46 (75.6) | 15 (24.4) | 1 |
| Weight Percentiles | Height Percentiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 3, 50, and 97 | <3 and >97 | p-Value | 3, 50, and 97 | <3 and >97 | p-Value | |||||
| No | Yes | No | Yes | No | Yes | No | Yes | |||
| 16 | 159 (21.0) | 531(77.0) | 10 (28.5) | 25 (71.5) | 0.4197 | 134 (23.1) | 531 (76.9) | 35 (58.4) | 25 (41.6) | 1.84 × 10−9 |
| 26 | 172 (24.9) | 518 (75.1) | 11 (31.4) | 24 (68.6) | 0.4250 | 114 (21.6) | 520 (78.4) | 39 (63.9) | 22 (36.1) | 2.3 × 10−11 |
| 36 | 156 (22.6) | 534 (77.4) | 10 (28.5) | 25 (71.5) | 0.4122 | 130 (19.5) | 534 (80.5) | 36 (59.1) | 25 (40.9) | 1.8 × 10−10 |
| 46 | 157 (22.7) | 553 (77.3) | 10 (28.5) | 25 (71.5) | 0.4145 | 129 (19.4) | 635 (80.6) | 38 (62.3) | 23 (37.7) | 5.5 × 10−12 |
| 17 | 574 (83.2) | 116 (16.8) | 29 (82.9) | 6 (17.1) | 1 | 552 (83.2) | 112 (16.8) | 51(83.7) | 10 (16.3) | 1 |
| 27 | 573 (83.1) | 117 (16.9) | 29 (82.9) | 6 (17.1) | 1 | 554 (83.5) | 110 (16.5) | 48 (78.7) | 13 (21.3) | 0.3719 |
| 37 | 553 (80.2) | 137 (19.8) | 24 (68.6) | 11 (31.4) | 0.129 | 528 (79.6) | 136 (20.4) | 49 (80.4) | 12 (19.6) | 1 |
| 47 | 558 (80.9) | 132 (19.1) | 25 (71.5) | 10 (28.5) | 0.189 | 534 (80.5) | 130 (19.5) | 49 (80.4) | 12 (19.6) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diéguez-Pérez, M.; Paz-Cortés, M.M.; Muñoz-Cano, L. Evaluation of the Relationship between the Weight and Height Percentiles and the Sequence and Chronology of Eruption in Permanent Dentition. Healthcare 2022, 10, 1363. https://doi.org/10.3390/healthcare10081363
Diéguez-Pérez M, Paz-Cortés MM, Muñoz-Cano L. Evaluation of the Relationship between the Weight and Height Percentiles and the Sequence and Chronology of Eruption in Permanent Dentition. Healthcare. 2022; 10(8):1363. https://doi.org/10.3390/healthcare10081363
Chicago/Turabian StyleDiéguez-Pérez, Montserrat, Marta M. Paz-Cortés, and Laura Muñoz-Cano. 2022. "Evaluation of the Relationship between the Weight and Height Percentiles and the Sequence and Chronology of Eruption in Permanent Dentition" Healthcare 10, no. 8: 1363. https://doi.org/10.3390/healthcare10081363