
Vibroacoustic Study in the Neonatal Ward

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
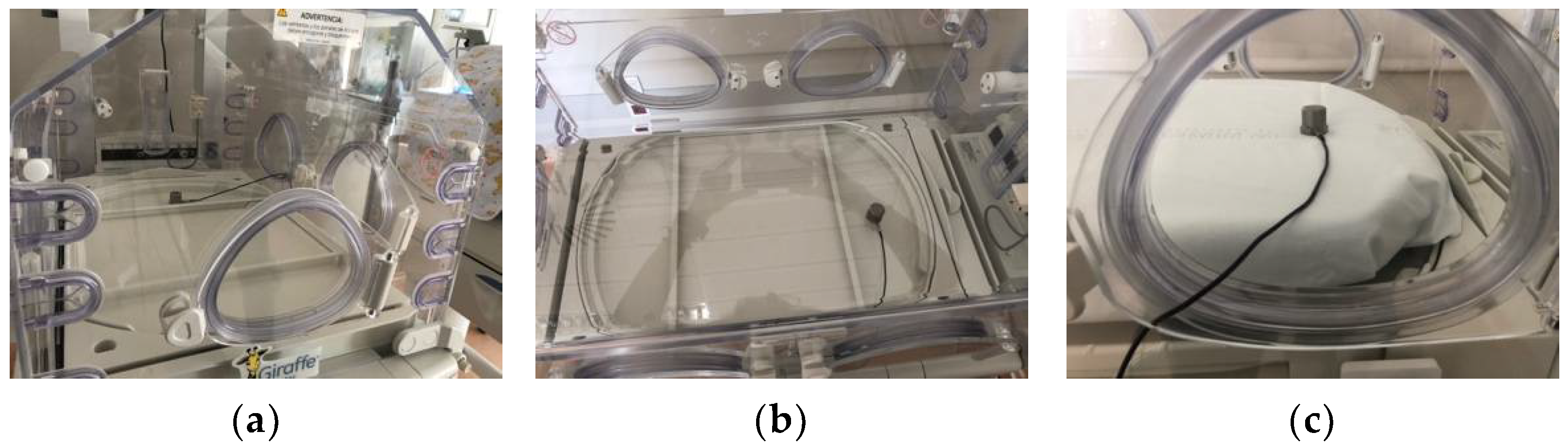
2.1. Measuring Vibrations
2.2. Neonatal Ward, Study Scenarios
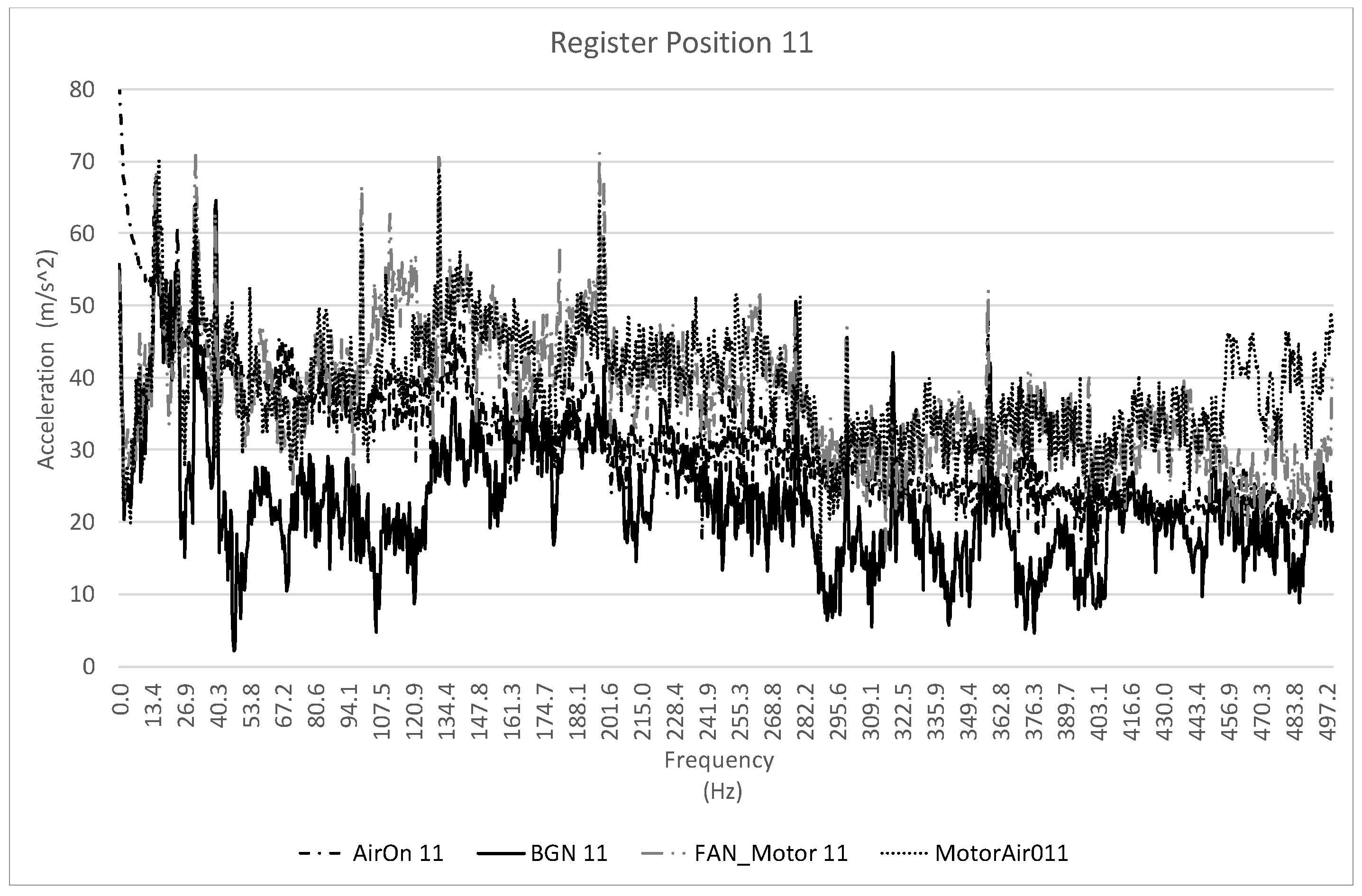
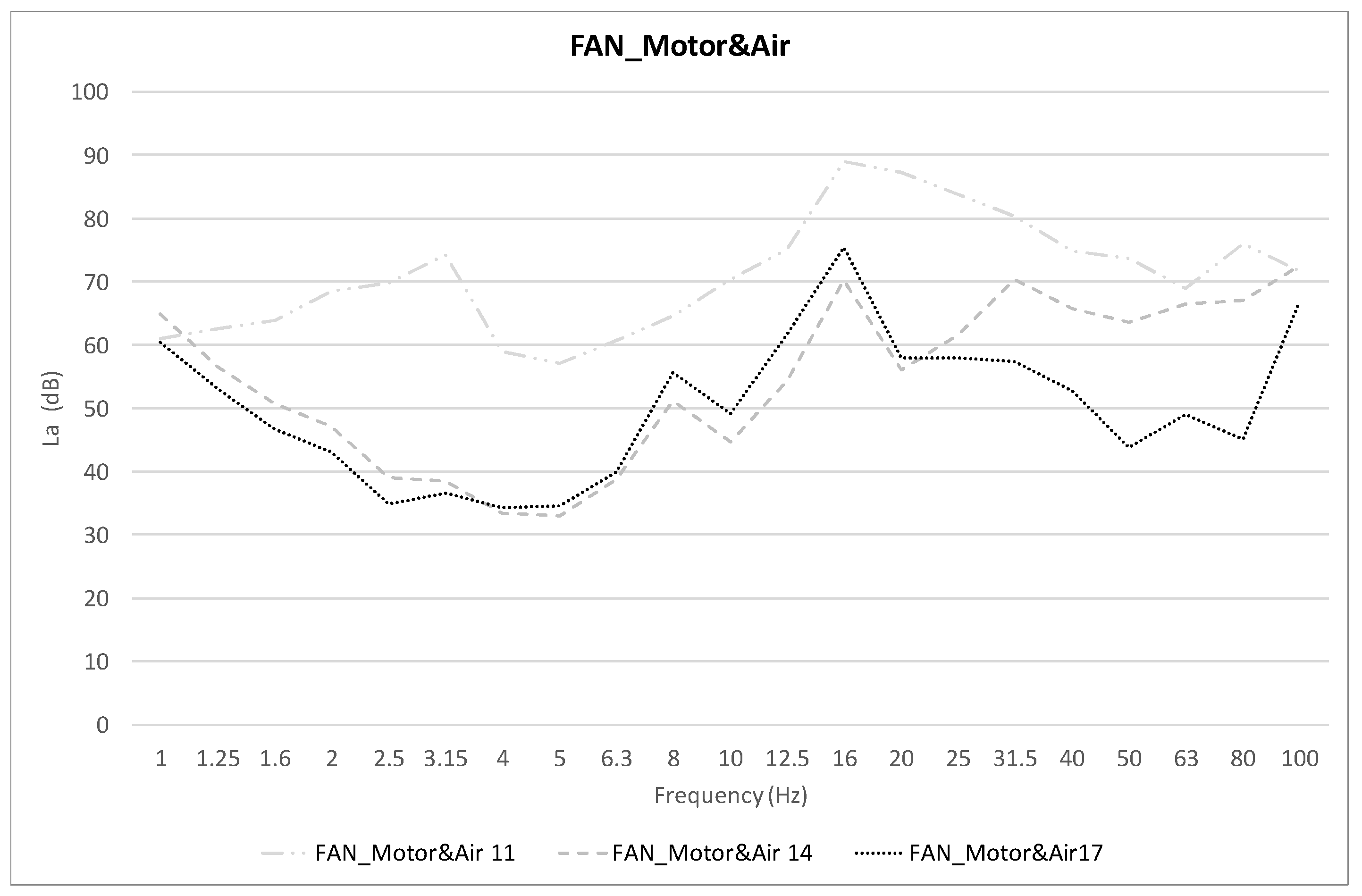
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rite Gracia, J.; Fernández Lorenzo, I.; Echáriz Urcelay, F.; Botet Mussons, G.; Herranz Carrillo, J.; Moreno Hernando, E.; Salguero García, M.; Luna, S. Niveles Asistenciales y Recomendaciones de Mínimos Para La Atención Neinatal. An. Pediatr. 2004, 60, 56–64. [Google Scholar]
- Ahamed, M.F.; Campbell, D.; Horan, S.; Rosen, O. Noise Reduction in the Neonatal Intensive Care Unit: A Quality Improvement Initiative. Am. J. Med. Qual. 2018, 33, 177–184. [Google Scholar] [CrossRef]
- Garinis, A.C.; Liao, S.; Cross, C.P.; Galati, J.; Middaugh, J.L.; Mace, J.C.; Wood, A.-M.; McEvoy, L.; Moneta, L.; Lubianski, T.; et al. Effect of Gentamicin and Levels of Ambient Sound on Hearing Screening Outcomes in the Neonatal Intensive Care Unit: A Pilot Study. Int. J. Pediatr. Otorhinolaryngol. 2017, 97, 42–50. [Google Scholar] [CrossRef]
- Calikusu Incekar, M.; Balci, S. The Effect of Training on Noise Reduction in Neonatal Intensive Care Units. J. Spec. Pediatr. Nurs. 2017, 22, e12181. [Google Scholar] [CrossRef]
- Casavant, S.G.; Bernier, K.; Andrews, S.; Bourgoin, A. Noise in the Neonatal Intensive Care Unit. Adv. Neonatal Care 2017, 17, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Degorre, C.; Ghyselen, L.; Barcat, L.; Dégrugilliers, L.; Kongolo, G.; Leké, A.; Tourneux, P. Noise Level in the NICU: Impact of Monitoring Equipment. Arch. Pediatr. 2017, 24, 100–106. [Google Scholar] [CrossRef]
- Jordão, K.R.; Pinto, L.D.A.P.; Machado, L.R.; Costa, L.B.V.D.L.; Trajano, E.T.L. Possible Stressors in a Neonatal Intensive Care Unit at a University Hospital. Rev. Bras. Ter. Intensiva 2016, 28, 310–314. [Google Scholar] [CrossRef]
- Shoemark, H.; Harcourt, E.; Arnup, S.J.; Hunt, R.W. Characterising the Ambient Sound Environment for Infants in Intensive Care Wards. J. Paediatr. Child Health 2016, 52, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Biabanakigoortani, A.; Namnabati, M.; Abdeyazdan, Z.; Badii, Z. Effect of Peer Education on the Noise Management in Iranian Neonatal Intensive Care Unit. Iran. J. Nurs. Midwifery Res. 2016, 21, 317. [Google Scholar] [CrossRef] [PubMed]
- Garrido Galindo, A.P.; Camargo Caicedo, Y.; Vélez-Pereira, A.M. Nivel de Ruido En Unidades de Cuidado Intensivo de Un Hospital Público Universitario En Santa Marta (Colombia). Med. Intensiva 2016, 40, 403–410. [Google Scholar] [CrossRef]
- Santos, J.; Carvalhais, C.; Xavier, A.; Silva, M.V. Assessment and Characterization of Sound Pressure Levels in Portuguese Neonatal Intensive Care Units. Arch. Environ. Occup. Health 2018, 73, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Gallegos-Martinez, J.; Reyes-Hernéndez, J.; Fernéndez-Hernéndez, V.; González-González, L. Indice de Ruido En La Unidad Neonatal. Su Impacto En Recién Nacidos. Acta Pedriatr. Mex. 2011, 32, 5–14. [Google Scholar]
- Philbin, M.K.; Evans, J.B. Standards for the Acoustic Environment of the Newborn ICU. J. Perinatol. 2006, 26, S27–S30. [Google Scholar] [CrossRef] [Green Version]
- Moreira Pinheiro, E.; Guinsburg, R.; de Aranajo Nabuto, M.A.; Yoshiko Kakehashi, T. Ruido En La Unidad de Terapia Intensiva Neonatal y En El Interior de La Incubadora. Rev. Latino-Am. Enferm. 2011, 19, 1214–1221. [Google Scholar]
- Wang, D.; Aubertin, C.; Barrowman, N.; Moreau, K.; Dunn, S.; Harrold, J. Examining the Effects of a Targeted Noise Reduction Program in a Neonatal Intensive Care Unit. Arch. Dis. Child.-Fetal Neonatal Ed. 2014, 99, F203–F208. [Google Scholar] [CrossRef]
- Parra, J.; de Suremain, A.; Berne Audeoud, F.; Ego, A.; Debillon, T. Sound Levels in a Neonatal Intensive Care Unit Significantly Exceeded Recommendations, Especially inside Incubators. Acta Paediatr. 2017, 106, 1909–1914. [Google Scholar] [CrossRef]
- del Rey, R.; Alba, J.; Sequí, J.; Revert, M. Análisis Acústico Del Entorno de La Sala Neonatal Del Hospital de Gandia. In Proceedings of the XI Congreso Iberoamericano de Acústica. X Congreso Ibérico de Acústica, 49° Congreso Español de Acústica, Cádiz, Spain, 24–26 October 2018. [Google Scholar]
- Valdés-de la Torre, G.E.; Martina Luna, M.; Braverman Bronstein, A.; Iglesias Leboreiro, J.; Bernárdez Zapata, I. Medición Comparativa de La Intensidad de Ruido Dentro y Fuera de Incubadoras Cerradas. Perinatol. Reprod. Hum. 2018, 32, 65–69. [Google Scholar] [CrossRef]
- Ministerio para la Transición Ecológica. Gobierno de España. Miteco. Calid. y Evaluación Ambiental. Atmósfera y Calid. Del Aire. Contam. Acústica. Available online: https://www.miteco.gob.es/es/calidad-y-evaluacion-ambiental/temas/atmosfera-y-calidad-del-aire/contaminacion-acustica/ (accessed on 14 June 2022).
- ISO 2631-2:2003; Mechanical Vibration and Shock-Evaluation of Human Exposure to Whole-Body Vibration-Part 2: Vibration in Buildings (1 Hz to 80 Hz). ISO: Geneva, Switzerland, 2003.
- Kromka-Szydek, M. Preliminary Assessment of Vibration Impacts Generated by the Public Transport Sustems on Pregnant Womwn Based on Subjective Reactions. Acta Bioeng. Biomech. 2018, 20, 79–92. [Google Scholar]
- Joubert, D. Professional Driving and Adverse Reproductive Outcomes: The Evidence to Date and Research Challenges. Open Occup. Health Saf. J. 2009, 1, 1–6. [Google Scholar]
- Mansfied, N. Human Response to Vibration; CRC Press: London, UK, 2005. [Google Scholar]
- Alba, J.; del Rey, R. Evaluación de Las Vibraciones En El Espacio Interior de Las Edificaciones. In Acústica Ambiental: Análisis, Legislación y Soluciones; UPV: Valencia, España, 2009; pp. 353–384. [Google Scholar]
- Real Decreto 286/2006, de 10 de Marzo, Sobre La Protección de La Salud y La Seguridad de Los Trabajadores Contra Riesgos Relacionados Con La Exposición Al Ruido; BOE: Madrid, España, 2006.
- Bailey, V.; Szyld, E.; Cagle, K.; Kurtz, D.; Chaaban, H.; Wu, D.; Williams, P. Modern Neonatal Transport: Sound and Vibration Levels and Their Impact on Physiological Stability. Am. J. Perinatol. 2019, 36, 352–359. [Google Scholar] [CrossRef]
- Blaxter, L.; Yeo, M.; McNally, D.; Crowe, J.; Henry, C.; Hill, S.; Mansfield, N.; Leslie, A.; Sharkey, D. Neonatal Head and Torso Vibration Exposure during Inter-Hospital Transfer. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2017, 231, 99–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carreras-González, E.; Moliner-Calderón, E.; Ginovart-Galiana, G. Fisiopatología Del Transporte En Helicóptero. An. Pediatr. 2014, 81, 269–270. [Google Scholar] [CrossRef]
- Macnab, A.; Chen, Y.; Gagnon, F.; Bora, B.; Laszlo, C. Vibration and Noise in Pediatric Emergency Transport Vehicles. Aviat. Space. Environ. Med. 1995, 66, 212–219. [Google Scholar] [PubMed]
- Browning, J.; Walding, D.; Klasen, J.; David, Y. Vibration Issues of Neonatal Incubators During In-Hospital Transport. J. Clin. Eng. 2008, 33, 74–77. [Google Scholar] [CrossRef]
- Youngblut, J.; Lewandowski, W.; Casper, G.; Youngblut, W. Vibration in Metal and Non-Metall Incubators. Biomed. Instrum. Technol. 1994, 28, 476–480. [Google Scholar]
- Ciesielski, S.; Kopka, J.; Kidawa, B. Incubator Noise and Vibration-Possible Iatrogenic Influence on Neonate. Int. J. Pediatr. Otorhinolaryngol. 1980, 1, 309–316. [Google Scholar] [CrossRef]
- Real Decreo 1299/2006, de 10 de Noviembre, Por El Que Se Aprueba El Cuadro de Enfermedades Profesionales En El Sistema de La Seguridad Social y Se Establecen Criterios Para Su Notificación y Registro; BOE: Madrid, España, 2006.
- Real Decreto 1367/2007, Por El Que Se Desarrolla La Ley 37/2003, Del Ruido, En Lo Referente a Zonificación Acústica, Objetivos de Calidad y Emisiones Acústicas; BOE: Madrid. España, 2007.
- ISO 2631-1:1997/Amd1:2010; Mechanical Vibration and Shock-Evaluation of Human Exposure to Whole-Body Vibration-Part 1: General Requirements-Amendment 1. ISO: Geneva, Switzerland, 1997.
- González Mazarías, G. Neovibra. Estudio de Las Vibraciones En Salas Neonatales: Caso Del Hospital de Gandía; Universitat Politècnica de València: Valencia, Spain, 2020. [Google Scholar]
- McCallig, M.; Pakrashi, V. Whole-Body Vibration Exposure from Incubators in the Neonatal Care Setting: A Review. J. Environ. Occup. Health 2021, 11, 37–46. [Google Scholar]
- Vitale, F.M.; Chirico, G.; Lentini, C. Sensory Stimulation in the NICU Environment: Devices, Systems, and Procedures to Protect and Stimulate Premature Babies. Children 2021, 8, 334. [Google Scholar] [CrossRef]
- Smith, V.; Kelty-stephen, D.; Qureshi Ahmad, M.; Mao, W.; Cakert, K.; Osborne, J.; Paydarfar, D. Stochastic Resonance Effects on Apnea, Bradycardia, and Oxygenation: A Randomized Controlled Trial. Pediatrics 2015, 136, 1561–1568. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1/3 Octave Band Central Frequency (Hz) | Lower Frequency (Hz) | Higher Frequency (Hz) | |
|---|---|---|---|
| 1 | 0.891 | 1.122 | 0.833 |
| 1.25 | 1.114 | 1.403 | 0.907 |
| 1.6 | 1.425 | 1.796 | 0.934 |
| 2 | 1.782 | 2.245 | 0.932 |
| 2.5 | 2.227 | 2.806 | 0.91 |
| 3.15 | 2.806 | 3.536 | 0.872 |
| 4 | 3.564 | 4.490 | 0.818 |
| 5 | 4.454 | 5.612 | 0.75 |
| 6.3 | 5.613 | 7.072 | 0.669 |
| 8 | 7.127 | 8.980 | 0.582 |
| 10 | 8.909 | 11.225 | 0.494 |
| 12.5 | 11.136 | 14.031 | 0.411 |
| 16 | 14.254 | 17.959 | 0.337 |
| 20 | 17.818 | 22.449 | 0.274 |
| 25 | 22.272 | 28.062 | 0.22 |
| 31.5 | 28.063 | 35.358 | 0.176 |
| 40 | 35.636 | 44.898 | 0.14 |
| 50 | 44.545 | 56.123 | 0.109 |
| 63 | 56.127 | 70.715 | 0.0834 |
| 80 | 71.272 | 89.797 | 0.0604 |
| Use of the Building | Vibration Index, Law (dB) |
|---|---|
| Residential | 75 |
| Sanitary | 72 |
| Cultural or Educative | 72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sequí-Canet, J.M.; Rey-Tormos, R.d.; Alba-Fernández, J.; González-Mazarías, G. Vibroacoustic Study in the Neonatal Ward. Healthcare 2022, 10, 1180. https://doi.org/10.3390/healthcare10071180
Sequí-Canet JM, Rey-Tormos Rd, Alba-Fernández J, González-Mazarías G. Vibroacoustic Study in the Neonatal Ward. Healthcare. 2022; 10(7):1180. https://doi.org/10.3390/healthcare10071180
Chicago/Turabian StyleSequí-Canet, Jose Miguel, Romina del Rey-Tormos, Jesús Alba-Fernández, and Gema González-Mazarías. 2022. "Vibroacoustic Study in the Neonatal Ward" Healthcare 10, no. 7: 1180. https://doi.org/10.3390/healthcare10071180