
Antibiotic Resistance of Helicobacter pylori in Children with Gastritis and Peptic Ulcers in Mekong Delta, Vietnam

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Design
2.2. Helicobacter pylori Culture and Antimicrobial Susceptibility Testing
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
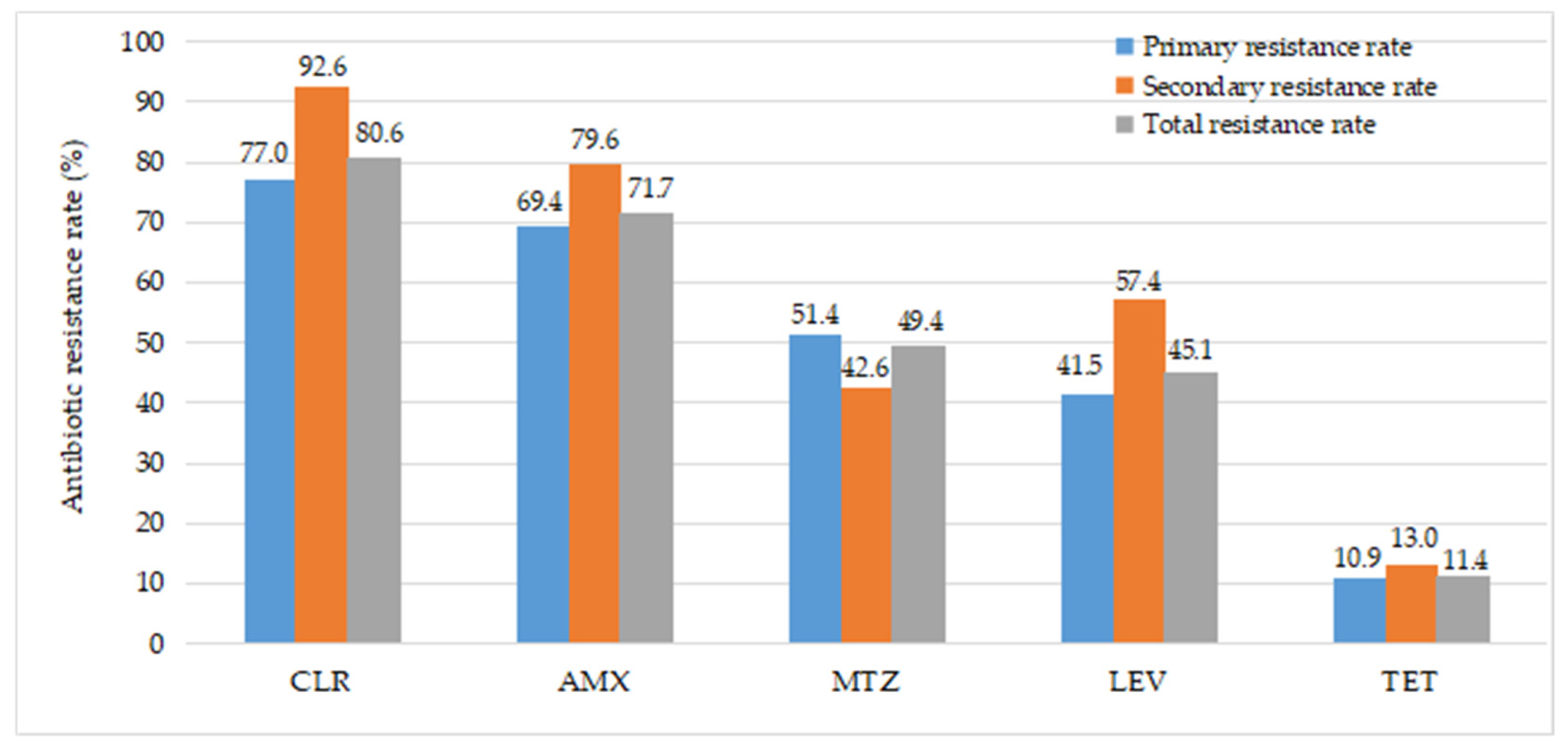
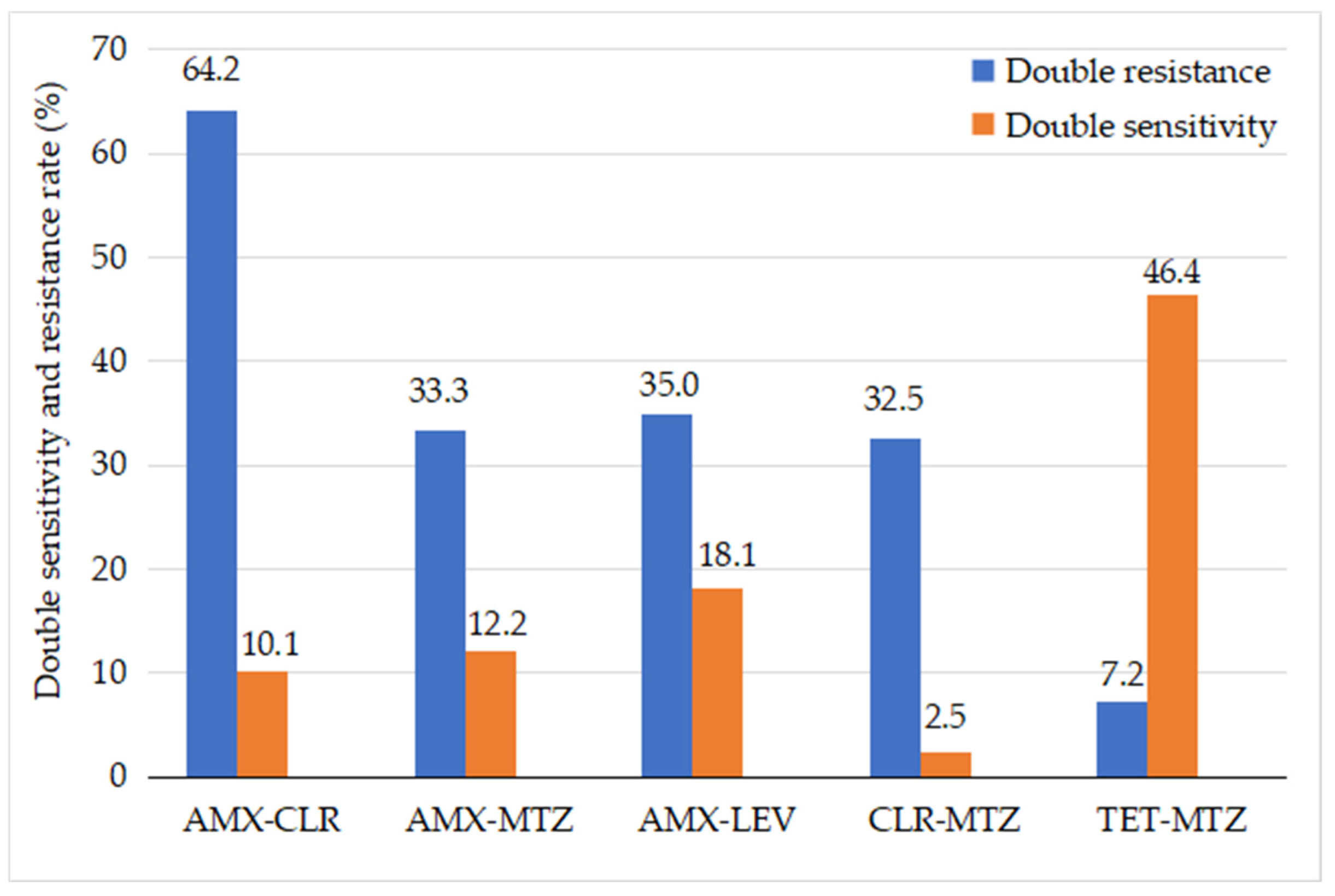
3.2. Antibiotic Resistance
3.3. Factors Associated with Antibiotic Resistance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okuda, M.; Lin, L.; Kikuchi, S. Helicobacter pylori Infection in Children and Adolescents. Adv. Exp. Med. Biol. 2019, 1149, 107–120. [Google Scholar] [PubMed]
- Jones, N.L. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). J. Pediatr. Gastroenterol. Nutr. 2017, 64, 991–1003. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M. How and when investigating and treating Helicobacter pylori infection in children. Acta Biomed. 2018, 89, 65–71. [Google Scholar] [PubMed]
- Quek, C. Antimicrobial susceptibility and clarithromycin resistance patterns of Helicobacter pylori clinical isolates in Vietnam. F1000Res 2016, 5, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Committee on Antimicrobial Susceptibility. Breakpoint Tables for Interpretation of MICs and Zone Diameters European Committee on Antimicrobial Susceptibility Testing; European Committee on Antimicrobial Susceptibility: Vaxjo, Sweden, 2019. [Google Scholar]
- Ogata, S.K. High Helicobacter pylori resistance to metronidazole and clarithromycin in Brazilian children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 645–648. [Google Scholar] [CrossRef]
- Krzyżek, P. High Primary Antibiotic Resistance of Helicobacter pylori Strains Isolated from Pediatric and Adult Patients in Poland during 2016–2018. Antibiotics 2020, 9, 228. [Google Scholar] [CrossRef]
- Silva, G.M. Helicobacter pylori antimicrobial resistance in a pediatric population. Helicobacter 2018, 23, e12528. [Google Scholar] [CrossRef]
- Li, J. Antibiotic Resistance of Helicobacter pylori Strains Isolated from Pediatric Patients in Southwest China. Front. Microbiol. 2020, 11, 621791. [Google Scholar] [CrossRef]
- Nguyen, T.V.H. Eradication of Helicobacter pylori in children in Vietnam in relation to antibiotic resistance. Helicobacter 2012, 17, 319–325. [Google Scholar] [CrossRef]
- Van Thieu, H. Antimicrobial Resistance and the Successful Eradication of Helicobacter pylori-induced Gastroduodenal Ulcers in Vietnamese Children. Med. Arch. 2021, 75, 112–115. [Google Scholar] [CrossRef]
- Awad, Y.M.M.M. Helicobacter pylori Antibiotic resistance patterns among Egyptian children and predictors of resistance. QJM Int. J. Med. 2020, 113, hcaa063-021. [Google Scholar] [CrossRef]
- Butenko, T. Antibacterial resistance and the success of tailored triple therapy in Helicobacter pylori strains isolated from Slovenian children. Helicobacter 2017, 22, e12400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manfredi, M. Primary Antimicrobial Susceptibility Changes in Children with Helicobacter pylori Infection over 13 Years in Northern Italy. Gastroenterol. Res. Pr. 2015, 2015, 717349. [Google Scholar]
- Okuda, M. Nationwide survey of Helicobacter pylori treatment for children and adolescents in Japan. Pediatr. Int. 2017, 59, 57–61. [Google Scholar] [CrossRef]
- Mahmoudi, S. Antibiotic susceptibility of Helicobacter pylori strains isolated from Iranian children: High frequency of A2143G point mutation associated with clarithromycin resistance. J. Glob. Antimicrob. Resist. 2017, 10, 131–135. [Google Scholar] [CrossRef]
- Fischbach, L.; Evans, E.L. Meta-analysis: The effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori. Aliment. Pharmacol. Ther. 2007, 26, 343–357. [Google Scholar] [CrossRef]
- Tankovic, J. Impact of Helicobacter pylori resistance to clarithromycin on the efficacy of the omeprazole-amoxicillin-clarithromycin therapy. Aliment Pharm. 2001, 15, 707–713. [Google Scholar] [CrossRef]
- Shah, S.C.; Iyer, P.G.; Moss, S.F. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastroenterology 2021, 160, 1831–1841. [Google Scholar] [CrossRef]
- Savoldi, A. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Van der Hulst, R.W. Influence of metronidazole resistance on efficacy of quadruple therapy for Helicobacter pylori eradication. Gut 1998, 42, 166–169. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; O’Morain, C.; McNamara, D. Antimicrobial susceptibility testing for Helicobacter pylori in times of increasing antibiotic resistance. World J. Gastroenterol. 2014, 20, 9912. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.Y. Systematic review with meta-analysis: The efficacy of levofloxacin triple therapy as the first- or second-line treatments of Helicobacter pylori infection. Aliment Pharm. 2016, 44, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [Green Version]
- Kato, S.; Shimizu, T.; Toyoda, S. The updated JSPGHAN guidelines for the management of Helicobacter pylori infection in childhood. Pediatrics Int. 2020, 62, 1315–1331. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Characteristics | Frequency (n = 237) | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 116 | 48.9 |
| Female | 121 | 51.1 |
| Age | ||
| Mean age | 10.03 ± 2.53 | |
| 5–8 years | 60 | 25.3 |
| 9–12 years | 122 | 51.5 |
| 13–16 years | 55 | 23.2 |
| Geographic area | ||
| Can Tho city | 150 | 63.3 |
| Nearby regions | 87 | 36.7 |
| Endoscopy findings | ||
| Nodular Gastritis/duodenitis | 168 | 69.2 |
| Gastric ulcer | 5 | 2.1 |
| Duodenal ulcer | 68 | 28.7 |
| History eradication | ||
| Without previous therapy | 183 | 77.2 |
| Prior to H. pylori treatment | 54 | 22.8 |
| Antibiotic Resistance | Frequency (n = 237) | Percentage (%) |
|---|---|---|
| Mono resistance | 24 | 10.1 |
| Dual resistance | 78 | 32.9 |
| Triple resistance | 111 | 46.8 |
| Quadruple resistance | 21 | 8.9 |
| All resistance | 3 | 1.3 |
| Multidrug resistance | 135 | 57.0 |
| Factors | Overall | CLR-R | p | AMX-R | p | MTZ-R | p | LEV-R | p |
|---|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | ||||||
| Age | |||||||||
| 5–10 years | 119 | 92 (77.3%) | 0.20 | 66 (55.5%) | 0.00 | 58 (48.9%) | 0.85 | 56 (47.1%) | 0.55 |
| 11–16 years | 118 | 99 (83.9%) | 104 (88.1%) | 59 (50.0%) | 51 (43.2%) | ||||
| Gender | |||||||||
| Male | 116 | 94 (81.0%) | 0.87 | 92 (79.3%) | 0.01 | 57 (49.1%) | 0.95 | 49 (42.2%) | 0.38 |
| Female | 121 | 97(80.2%) | 78 (64.5%) | 60 (49.6%) | 58 (47.9%) | ||||
| Prior treatment | |||||||||
| No | 183 | 141 (77.0%) | 0.01 | 127 (69.4%) | 0.14 | 94 (51.4%) | 0.26 | 76 (41.5%) | 0.39 |
| Yes | 54 | 50 (92.6%) | 43 (79.6%) | 23 (42.6) | 31 (57.4%) | ||||
| EGD Findings | |||||||||
| Nodular Gastritis | 164 | 127 (77.4%) | 0.66 | 107 (65.2%) | 0.00 | 76 (46.3%) | 0.58 | 80 (48.8%) | 0.79 |
| Peptic ulcer | 73 | 64 (87.7%) | 63 (86.3%) | 31 (42.5%) | 37 (50.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, L.T.T.; Nguyen, T.A.; Nguyen, N.A.; Nguyen, Y.T.H.; Nguyen, H.T.B.; Nguyen, L.T.; Vi, M.T.; Nguyen, T. Antibiotic Resistance of Helicobacter pylori in Children with Gastritis and Peptic Ulcers in Mekong Delta, Vietnam. Healthcare 2022, 10, 1121. https://doi.org/10.3390/healthcare10061121
Le LTT, Nguyen TA, Nguyen NA, Nguyen YTH, Nguyen HTB, Nguyen LT, Vi MT, Nguyen T. Antibiotic Resistance of Helicobacter pylori in Children with Gastritis and Peptic Ulcers in Mekong Delta, Vietnam. Healthcare. 2022; 10(6):1121. https://doi.org/10.3390/healthcare10061121
Chicago/Turabian StyleLe, Loan Thi Thuy, Tuan Anh Nguyen, Nghia An Nguyen, Yen Thi Hai Nguyen, Hai Thi Be Nguyen, Liem Thanh Nguyen, Mai Tuyet Vi, and Thang Nguyen. 2022. "Antibiotic Resistance of Helicobacter pylori in Children with Gastritis and Peptic Ulcers in Mekong Delta, Vietnam" Healthcare 10, no. 6: 1121. https://doi.org/10.3390/healthcare10061121