
Aggression, Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients


 ,
,  ,
, 
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Research Design
2.2. Study Participants
2.3. Minimal Sample Size Calculation
2.4. Measurement Tools
2.5. Brief Aggression Questionnaire
2.6. Sense of Coherence Questionnaire
2.7. Toronto Alexithymia Scale
2.8. Statistical Analysis
3. Results
3.1. General Characteristics of Participants and Scores on Outcome Variables
3.2. Correlations among Continuous Variables
3.3. Hierarchical Linear Regression Analyses
3.4. Simple Mediation Analyses
3.5. Path Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monahan, J.; Steadman, H.J.; Silver, E.; Appelbaum, P.S.; Robbins, P.C.; Mulvey, E.P.; Roth, L.H.; Grisso, T.; Banks, S.M. Rethinking Risk Assessment: The MacArthur Study of Mental Disorder and Violence; Oxford University Press: Oxford, UK, 2001. [Google Scholar]
- Hodgins, S. Aggressive Behavior Among Persons with Schizophrenia and Those Who Are Developing Schizophrenia: Attempting to Understand the Limited Evidence on Causality. Schizophr. Bull. 2017, 43, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.; Shin, W.S.; An, I.; Bang, M.; Cho, D.Y.; Lee, S.H. Biological Aspects of Aggression and Violence in Schizophrenia. Clin. Psychopharmacol. Neurosci. 2019, 17, 475–486. [Google Scholar] [CrossRef]
- Hodgins, S.; Klein, S. New Clinically Relevant Findings about Violence by People with Schizophrenia. Can. J. Psychiatry 2017, 62, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Volavka, J.; Citrome, L. Pathways to aggression in schizophrenia affect results of treatment. Schizophr. Bull. 2011, 37, 921–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazel, S.; Langstrom, N.; Hjern, A.; Grann, M.; Lichtenstein, P. Schizophrenia, substance abuse, and violent crime. JAMA 2009, 301, 2016–2023. [Google Scholar] [CrossRef] [PubMed]
- Lamsma, J.; Cahn, W.; Fazel, S.; GROUP and NEDEN Investigators. Use of illicit substances and violent behaviour in psychotic disorders: Two nationwide case-control studies and meta-analyses. Psychol. Med. 2020, 50, 2028–2033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, M.T.; Harvey, P.D. Neurocognition and social cognition training as treatments for violence and aggression in people with severe mental illness. CNS Spectr. 2019, 25, 145–153. [Google Scholar] [CrossRef] [Green Version]
- Ndoro, S. Understanding aggressive behaviour in patients with schizophrenia through social cognitive theory: A narrative literature review. Br. J. Ment. Health Nurs. 2020, 9, 1–10. [Google Scholar] [CrossRef]
- Wu, Y.; Kang, R.; Yan, Y.; Gao, K.; Li, Z.; Jiang, J.; Chi, X.; Xia, L. Epidemiology of schizophrenia and risk factors of schizophrenia-associated aggression from 2011 to 2015. J. Int. Med. Res. 2018, 46, 4039–4049. [Google Scholar] [CrossRef]
- Widmayer, S.; Sowislo, J.F.; Jungfer, H.A.; Borgwardt, S.; Lang, U.E.; Stieglitz, R.D.; Huber, C.G. Structural Magnetic Resonance Imaging Correlates of Aggression in Psychosis: A Systematic Review and Effect Size Analysis. Front. Psychiatry 2018, 9, 217. [Google Scholar] [CrossRef]
- Fjellvang, M.; Grøning, L.; Haukvik, U.K. Imaging Violence in Schizophrenia: A Systematic Review and Critical Discussion of the MRI Literature. Front. Psychiatry 2018, 9, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Raine, A.; Han, C.B.; Schug, R.A.; Toga, A.W.; Narr, K.L. Reduced hippocampal and parahippocampal volumes in murderers with schizophrenia. Psychiatry Res. Neuroimaging 2010, 182, 9–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tikàsz, A.; Potvin, S.; Dugré, J.R.; Fahim, C.; Zaharieva, V.; Lipp, O.; Mendrek, A.; Dumais, A. Violent Behavior Is Associated with Emotion Salience Network Dysconnectivity in Schizophrenia. Front. Psychiatry 2020, 11, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakowski, M.I.; De Sanctis, P.; Foxe, J.J.; Hoptman, M.J.; Nolan, K.; Kamiel, S.; Czobor, P. Disturbances in Response Inhibition and Emotional Processing as Potential Pathways to Violence in Schizophrenia: A High-Density Event-Related Potential Study. Schizophr. Bull. 2016, 42, 963–974. [Google Scholar] [CrossRef] [Green Version]
- Botvinick, M.M.; Cohen, J.D.; Carter, C.S. Conflict monitoring and anterior cingulate cortex: An update. Trends Cogn. Sci. 2004, 8, 539–546. [Google Scholar] [CrossRef] [Green Version]
- McRae, K.; Reiman, E.M.; Fort, C.L.; Chen, K.; Lane, R.D. Association between trait emotional awareness and dorsal anterior cingulate activity during emotion is arousal-dependent. Neuroimage 2008, 41, 648–655. [Google Scholar] [CrossRef] [Green Version]
- Swanson, J.W.; Swartz, M.S.; Van Dorn, R.A.; Elbogen, E.B.; Wagner, H.R.; Rosenheck, R.A.; Stroup, T.S.; McEvoy, J.P.; Lieberman, J.A. A national study of violent behavior in persons with schizophrenia. Arch. Gen. Psychiatry 2006, 63, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Barzilay, R.; Lobel, T.; Krivoy, A.; Shlosberg, D.; Weizman, A.; Katz, N. Elevated C-reactive protein levels in schizophrenia inpatients is associated with aggressive behavior. Eur. Psychiatry 2016, 31, 8–12. [Google Scholar] [CrossRef]
- Tong, Z.; Zhu, J.; Wang, J.J.; Yang, Y.J.; Hu, W. The Neutrophil-Lymphocyte Ratio Is Positively Correlated with Aggression in Schizophrenia. Biomed. Res. Int. 2022, 2022, 4040974. [Google Scholar] [CrossRef]
- Velotti, P.; Garofalo, C.; Petrocchi, C.; Cavallo, F.; Popolo, R.; Dimaggio, G. Alexithymia, emotion dysregulation, impulsivity and aggression: A multiple mediation model. Psychiatry Res. 2016, 237, 296–303. [Google Scholar] [CrossRef]
- De Schutter, M.A.; Kramer, H.J.; Franken, E.J.; Lodewijkx, H.F.; Kleinepier, T. The influence of dysfunctional impulsivity and alexithymia on aggressive behavior of psychiatric patients. Psychiatry Res. 2016, 243, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messina, A.; Beadle, J.N.; Paradiso, S. Towards a classification of alexithymia: Primary secondary and organic. J. Psychopathol. 2014, 20, 38–49. [Google Scholar]
- Luminet, O.; Nielson, K.A.; Ridout, N. Having no words for feelings: Alexithymia as a fundamental personality dimension at the interface of cognition and emotion. Cogn. Emot. 2021, 35, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Hemming, L.; Haddock, G.; Shaw, J.; Pratt, D. Alexithymia and Its Associations with Depression, Suicidality, and Aggression: An Overview of the Literature. Front. Psychiatry 2019, 10, 203. [Google Scholar] [CrossRef]
- Kano, M.; Fukudo, S. The alexithymic brain: The neural pathways linking alexithymia to physical disorders. Biopsychosoc. Med. 2013, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Han, D.; Li, M.; Mei, M.; Sun, X. The functional and structural characteristics of the emotion network in alexithymia. Neuropsychiatr. Dis. Treat. 2018, 14, 991–998. [Google Scholar] [CrossRef] [Green Version]
- Goerlich, K.; Aleman, A. Neuroimaging Studies of Alexithymia. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Luminet, O., Bagby, R., Taylor, G., Eds.; Cambridge University Press: Cambridge, UK, 2018; pp. 207–249. [Google Scholar]
- Ihme, K.; Dannlowski, U.; Lichev, V.; Stuhrmann, A.; Grotegerd, D.; Rosenberg, N.; Kugel, H.; Heindel, W.; Arolt, V.; Kersting, A.; et al. Alexithymia is related to differences in gray matter volume: A voxel-based morphometry study. Brain Res. 2013, 1491, 60–67. [Google Scholar] [CrossRef]
- Goerlich-Dobre, K.S.; Bruce, L.; Martens, S.; Aleman, A.; Hooker, C.I. Distinct associations of insula and cingulate volume with the cognitive and affective dimensions of alexithymia. Neuropsychologia 2014, 53, 284–292. [Google Scholar] [CrossRef]
- Farah, T.; Ling, S.; Raine, A.; Yang, Y.; Schug, R. Alexithymia and reactive aggression: The role of the amygdala. Psychiatry Res. Neuroimaging 2018, 281, 85–91. [Google Scholar] [CrossRef]
- Neumann, D.; Malec, J.F.; Hammond, F.M. The Relations of Self-Reported Aggression to Alexithymia, Depression, and Anxiety After Traumatic Brain Injury. J. Head Trauma Rehabil. 2017, 32, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Baslet, G.; Termini, L.; Herbener, E. Deficits in emotional awareness in schizophrenia and their relationship with other measures of functioning. J. Nerv. Ment. Dis. 2009, 197, 655–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremeau, F. A Review of Emotion Deficits in Schizophrenia. Dialogues Clin. Neurosci. 2006, 8, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Zaki, J.; Harvey, P.O.; Ochsner, K.; Green, M.F. Schizophrenia patients are impaired in empathic accuracy. Psychol. Med. 2011, 41, 2297–2304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varachhia, S.; Ferguson, E.; Doody, G.A. A Meta-Analysis Taxonomizing Empathy in Schizophrenia. J. Psychiatry Depress. Anxiety 2018, 4, 016. [Google Scholar] [CrossRef]
- Stanghellini, G.; Ricca, V. Alexithymia and Schizophrenias. Psychopathology 1995, 28, 263–272. [Google Scholar] [CrossRef]
- Todarello, O.; Porcelli, P.; Grilletti, F.; Bellomo, A. Is alexithymia related to negative symptoms of schizophrenia? Psychopathology 2015, 38, 310–314. [Google Scholar] [CrossRef]
- Van’t Wout, M.; Aleman, A.; Bermond, B.; Kahn, R.S. No words for feelings: Alexithymia in schizophrenia patients and first-degree relatives. Compr. Psychiatry 2007, 48, 27–33. [Google Scholar] [CrossRef]
- Van der Meer, L.; van’t Wout, M.; Aleman, A. Emotion regulation strategies in patients with schizophrenia. Psychiatry Res. 2009, 170, 108–113. [Google Scholar] [CrossRef]
- Fogley, R.; Warman, D.; Lysaker, P.H. Alexithymia in schizophrenia: Associations with neurocognition and emotional distress. Psychiatry Res. 2014, 218, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Phillips, M.L.; Drevets, W.C.; Rauch, S.L.; Lane, R. Neurobiology of emotion perception: II. Implications for major psychiatric disorders. Biol. Psychiatry 2003, 54, 515–528. [Google Scholar] [CrossRef]
- Bailey, P.E.; Henry, J.D. Separating component processes of theory of mind in schizophrenia. Br. J. Clin. Psychol. 2010, 49, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Brüne, M. “Theory of mind” in schizohrenia: A review of the literature. Schizophr. Bull. 2005, 31, 21–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, M.; Miyata, J.; Sasamoto, A.; Kawada, R.; Fujimoto, S.; Tanaka, Y.; Sawamoto, N.; Fukuyama, H.; Takahashi, H.; Murai, T. Alexithymia and reduced white matter integrity in schizophrenia: A diffusion tensor imaging study on impaired emotional self-awareness. Schizophr. Res. 2012, 141, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, M.; Miyata, J.; Hirao, K.; Fujiwara, H.; Kawada, R.; Fujimoto, S.; Tanaka, Y.; Sasamoto, A.; Sawamoto, N.; Fukuyama, H.; et al. Alexithymia and regional gray matter alterations in schizophrenia. Neurosci. Res. 2011, 70, 206–213. [Google Scholar] [CrossRef]
- De Rick, A.; Vanheule, S. The relationship between perceived parenting, adult attachment style and alexithymia in alcoholic inpatients. Addict. Behav. 2006, 31, 1265–1270. [Google Scholar] [CrossRef]
- Parnas, J. Self and schizophrenia: A phenomenological perspective. In The Self in Neuroscience and Psychiatry; Kircher, T., David, A., Eds.; Cambridge University Press: Cambridge, UK, 2013; pp. 127–141. [Google Scholar]
- Nelson, B.; Whitford, T.J.; Lavoie, S.; Sass, L.A. What are the neurocognitive correlates of basic self-disturbance in schizophrenia? Integrating phenomenology and neurocognition. Part 1 (Source monitoring deficits). Schizophr. Res. 2014, 152, 12–19. [Google Scholar] [CrossRef]
- Svendsen, I.H.; Øie, M.G.; Møller, P.; Nelson, B.; Haug, E.; Melle, I. Basic self-disturbances independently predict recovery in psychotic disorders: A seven year follow-up study. Schizophr. Res. 2019, 212, 72–78. [Google Scholar] [CrossRef]
- Svendsen, I.H.; Øie, M.G.; Møller, P.; Nelson, B.; Melle, I.; Haug, E. Basic self-disturbances are associated with Sense of Coherence in patients with psychotic disorders. PLoS ONE 2020, 15, e0230956. [Google Scholar] [CrossRef] [Green Version]
- Antonovsky, A. The Structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Eriksson, M.; Mittelmark, M. The sense of coherence and its measurement. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 97–106. [Google Scholar]
- Feldt, T.; Leskinen, E.; Kinnunen, U.; Ruoppila, I. The stability of sense of coherence: Comparing two age groups over a 5-year follow-up study. Pers. Individ. Differ. 2003, 35, 1151–1165. [Google Scholar] [CrossRef]
- Gierowski, J.K.; Cyboran, M.; Poranska, A. Relationship between Coherence and Aggression, Taking Into Account Psychological Gender, in Juvenile Girls and Boys. Probl. Forensic Sci. 2008, 74, 121–149. [Google Scholar]
- Allah-Gholilo, K.; Abolghasemi, A.; Dehghan, H.; Imani, H. The Association of Alexithymia and Sense of Coherence with Life Satisfaction in Attention Deficit Hyperactivity Disorder. Zahedan J. Res. Med. Sci. 2015, 17, e977. [Google Scholar] [CrossRef] [Green Version]
- O’Carroll, R.E.; Ayling, R.; O’Reilly, S.M.; North, N.T. Alexithymia and sense of coherence in patients with total spinal cord transection. Psychosom. Med. 2003, 65, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Sancassiani, F.; Preti, A.; Cacace, E.; Ruggiero, V.; Testa, G.; Romano, F.; Carta, M.G. Alexithymia and sense of coherence: Does their impact on fibromyalgia suggest new targets for therapy? Gen. Hosp. Psychiatry 2019, 59, 78–79. [Google Scholar] [CrossRef] [PubMed]
- Banni, S. Alexithymia, Sense of Coherence and Dysregulation of Biorhythms in Fibromyalgia: Implications for Pain Management and Quality of Life. Ph.D. Thesis, Università degli Studi di Cagliari, Cagliari, Italy, 2015. [Google Scholar]
- Richardson, C.G.; Ratner, P.A. Sense of coherence as a moderator of the effects of stressful life events on health. J. Epidemiol. Community Health 2005, 59, 979–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattila, A.K.; Saarni, S.I.; Salminen, J.K.; Huhtala, H.; Sintonen, H.; Joukamaa, M. Alexithymia and health-related quality of life in a general population. Psychosomatics 2009, 50, 59–68. [Google Scholar] [CrossRef]
- Antonovsky, A. Unravelling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Langeland, E.; Wahl, A.K.; Kristoffersen, K.; Hanestad, B.R. Promoting coping: Salutogenesis among people with mental health problems. Issues Ment. Health Nurs. 2007, 28, 275–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederblad, M.; Hansson, K. Sense of coherence—A concept influencing health and quality of life in a Swedish psychiatric at-risk group. Isr. J. Med. Sci. 1996, 32, 194–199. [Google Scholar] [PubMed]
- Langeland, E.; Wahl, A.K.; Kristoffersen, K.; Nortvedt, M.; Hanestad, B.R. Sense of coherence predicts change in life satisfaction among home-living residents in the community with mental health problems: A 1-year follow-up study. Qual. Life Res. 2007, 16, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Torgalsbøen, A.K.; Rund, B.R. Lessons learned from three studies of recovery from schizophrenia. Int. Rev. Psychiatry 2002, 14, 312–317. [Google Scholar] [CrossRef]
- Harrow, M.; Grossman, L.; Jobe, T.H.; Herbener, E.S. Do patients with schizophrenia ever show periods of recovery? A 15-years multi-follow-up study. Schizophr. Bull. 2005, 31, 723–734. [Google Scholar] [CrossRef] [Green Version]
- Witkowska-Łuć, B. Schizophrenia and sense of coherence. Psychiatr. Pol. 2018, 52, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Izydorczyk, B.; Sitnik-Warchulska, K.; Kühn-Dymecka, A.; Lizińczyk, S. Resilience, Sense of Coherence, and Coping with Stress as Predictors of Psychological Well-Being in the Course of Schizophrenia. The Study Design. Int. J. Environ. Res. Public Health 2019, 16, 1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, C.G.; Hochstrasser, L.; Meister, K.; Schimmelmann, B.G.; Lambert, M. Evidence for an agitated-aggressive syndrome in early-onset psychosis correlated with antisocial personality disorder, forensic history, and substance use disorder. Schizophr. Res. 2016, 175, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Bobes, J.; Fillat, O.; Arango, C. Violence among schizophrenia out-patients compliant with medication: Prevalence and associated factors. Acta Psychiatr. Scand. 2009, 119, 218–225. [Google Scholar] [CrossRef]
- Caqueo-Urízar, A.; Fond, G.; Urzúa, A.; Boyer, L.; Williams, D.R. Violent behavior and aggression in schizophrenia: Prevalence and risk factors. A multicentric study from three Latin-America countries. Schizophr. Res. 2016, 178, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Stündağ, M.; Gulec, H.; Inanç, L.; Sevinç, E.; Semiz, M. Is alexithymia a separate dimension in schizophrenia? Anatol. J. Psychiatry 2020, 21, 85663. [Google Scholar] [CrossRef]
- Maggini, C.; Raballo, A. Alexithymia and schizophrenic psychopathology. Acta Biomed. 2004, 75, 40–49. [Google Scholar] [PubMed]
- Hsu, M.C.; Ouyang, W.C. Effects of Integrated Violence Intervention on Alexithymia, Cognitive, and Neurocognitive Features of Violence in Schizophrenia: A Randomized Controlled Trial. Brain Sci. 2021, 11, 837. [Google Scholar] [CrossRef] [PubMed]
- Kupferberg, S.L. The relation between alexithymia and aggression in a nonclinical sample. Diss. Abstr. Int. Sect. B Sci. Eng. 2002, 63, 3011. [Google Scholar]
- Sfeir, E.; Geara, C.; Hallit, S.; Obeid, S. Alexithymia, aggressive behavior and depression among Lebanese adolescents: A cross-sectional study. Child Adolesc. Psychiatry Ment. Health 2020, 14, 32. [Google Scholar] [CrossRef]
- Garofalo, C.; Velotti, P.; Zavattini, G.C. Emotion regulation and aggression: The incremental contribution of alexithymia, impulsivity, and emotion dysregulation facets. Psychol. Violence 2018, 8, 470–483. [Google Scholar] [CrossRef] [Green Version]
- Mancinelli, E.; Li, J.-B.; Lis, A.; Salcuni, S. Adolescents’ Attachment to Parents and Reactive–Proactive Aggression: The Mediating Role of Alexithymia. Int. J. Environ. Res. Public Health 2021, 18, 13363. [Google Scholar] [CrossRef]
- Manninen, M.; Therman, S.; Suvisaari, J.; Ebeling, H.; Moilanen, I.; Huttunen, M.; Joukamaa, M. Alexithymia is common among adolescents with severe disruptive behavior. J. Nerv. Ment. Dis. 2011, 199, 506–509. [Google Scholar] [CrossRef]
- Konrath, S.; Novin, S.; Li, T. Is the relationship between alexithymia and aggression context-dependent? Impact of group membership and belief similarity. Pers. Individ. Differ. 2012, 53, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Dehghani, F.; Falahi, P. Does impulsivity mediate the relationship between alexithymia and aggression? J. Fundam. Ment. Health 2021, 23, 57–62. [Google Scholar]
- Hemming, L.; Shaw, J.; Haddock, G.; Carter, L.A.; Pratt, D. A Cross-Sectional Study Investigating the Relationship between Alexithymia and Suicide, Violence, and Dual Harm in Male Prisoners. Front. Psychiatry 2021, 12, 670863. [Google Scholar] [CrossRef]
- Parry, C.L. The Nature of the Association between Male Violent Offending and Alexithymia. Ph.D. Thesis, Edith Cowan University, Joondalup, WA, Australia, 2012. Available online: https://ro.ecu.edu.au/theses/483 (accessed on 7 February 2022).
- Evren, C.; Cinar, O.; Evren, B.; Umut, G.; Can, Y.; Bozkurt, M. Relationship between Alexithymia and Aggression in a Sample of Men with Substance Dependence. Klin. Psikofarmakol. Bülteni Bull. Clin. Psychopharmacol. 2015, 25, 233–242. [Google Scholar] [CrossRef]
- Kivimäki, M.; Elovainio, M.; Vahtera, J.; Nurmi, J.E.; Feldt, T.; Keltikangas-Järvinen, L.; Pentti, J. Sense of coherence as a mediator between hostility and health: Seven-year prospective study on female employees. J. Psychosom. Res. 2002, 52, 239–247. [Google Scholar] [CrossRef]
- Silarova, B.; Nagyova, I.; Rosenberger, J.; van Dijk, J.P.; Reijneveld, S.A. Sense of coherence as a mediator between hostility and health-related quality of life among coronary heart disease patients. Heart Lung. 2016, 45, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Julkunen, J.; Ahlström, R. Hostility, anger, and sense of coherence as predictors of health-related quality of life. Results of an ASCOT substudy. J. Psychosom. Res. 2006, 61, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson-Tops, A.; Brunt, D.; Rask, M. The structure of Antonovsky’s sense of coherence in patients with schizophrenia and its relationship to psychopathology. Scand. J. Caring Sci. 2005, 19, 280–287. [Google Scholar] [CrossRef]
- Gassmann, W.; Christ, O.; Lampert, J.; Berger, H. The influence of Antonovsky’s sense of coherence (SOC) and psychoeducational family intervention (PEFI) on schizophrenic outpatients’ perceived quality of life: A longitudinal field study. BMC Psychiatry 2013, 13, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bengtsson-Tops, A.; Hansson, L. The validity of Antonovsky’s Sense of Coherence measure in a sample of schizophrenic patients living in the community. J. Adv. Nurs. 2001, 33, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Bergstein, M.; Weizman, A.; Solomon, Z. Sense of coherence among delusional patients: Prediction of remission and risk of relapse. Compr. Psychiatry. 2008, 49, 288–296. [Google Scholar] [CrossRef]
- Yıldız, B. Investigation the mediator role of sense of coherence in the relationship between self differentiation and alexitymia in university students. Turk. Psychol. Couns. Guid. J. 2020, 10, 603–616. [Google Scholar]
- Cameron, K.; Ogrodniczuk, J.; Hadjipavlou, G. Changes in alexithymia following psychological intervention: A review. Harv. Rev. Psychiatry 2014, 22, 162–178. [Google Scholar] [CrossRef]
- Aci, O.S.; Kutlu, F.Y. The effect of salutogenic approach-based interviews on sense of coherence and resilience in people with schizophrenia: A randomized controlled trial. Perspect. Psychiatr. Care 2021, 1–9. [Google Scholar] [CrossRef]
- Veltro, F.; Latte, G.; Pontarelli, I.; Pontarelli, C.; Nicchiniello, I.; Zappone, L. Long term outcome study of a salutogenic psychoeducational recovery oriented intervention (Inte.G.R.O.) in severe mental illness patients. BMC Psychiatry 2022, 22, 240. [Google Scholar] [CrossRef]
- Langeland, E.; Vaandrager, L.; Nilsen, A.B.V.; Schraner, M.; Meier Magistretti, C. Effectiveness of Interventions to Enhance the Sense of Coherence in the Life Course. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Pearson Education, Inc.: Boston, MA, USA, 2007. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149. [Google Scholar] [CrossRef] [Green Version]
- Schoemann, A.M.; Boulton, A.J.; Short, S.D. Determining Power and Sample Size for Simple and Complex Mediation Models. Soc. Psychol. Pers. Sci. 2017, 8, 379–386. [Google Scholar] [CrossRef]
- Kline, R.B. Methodology in the Social Sciences. Principles and Practice of Structural Equationmodeling; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Pachi, A.; Giotakis, K.; Fanouraki, E.; Vouraki, G.; Bratis, D.; Tselebis, A. Adaptation of the Brief Aggression Questionnaire (BAQ) in Greek population. Encephalos 2021, 58, 6–23. [Google Scholar]
- Webster, G.D.; DeWall, C.N.; Pond, R.S., Jr.; Deckman, T.; Jonason, P.K.; Le, B.M.; Nichols, L.A.; Orozco Schember, T.; Crysel, L.C.; Crosier, B.S.; et al. The Brief Aggression Questionnaire: Psychometric and Behavioral Evidence for an Efficient Measure of Trait Aggression. Aggress. Behav. 2014, 40, 120–139. [Google Scholar] [CrossRef] [PubMed]
- Anagnostopoulou, T.; Kioseoglou, G. Sense of Coherence Scale. In Psychometric Tools in Greece; Stalikas, A., Triliva, S., Roussi, P., Eds.; Ellinika Grammata: Athens, Grece, 2002; pp. 291–292, (In Modern Greek). [Google Scholar]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The Twenty-Item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Anagnostopoulou, T.; Kioseoglou, G. Toronto Alexithymia Scale. In Psychometric Tools in Greece; Stalikas, A., Triliva, S., Roussi, P., Eds.; Ellinika Grammata: Athens, Grece, 2002; pp. 100–101, (In Modern Greek). [Google Scholar]
- Tselebis, A.; Bratis, D.; Roubi, A.; Anagnostopoulou, M.; Giotakis, K.; Pachi, A. Anger management during the COVID-19 lockdown: The role of resilience and family support. Encephalos 2022, 59, 1–10. [Google Scholar]
- Tselebis, A.; Kosmas, E.; Bratis, D.; Moussas, G.; Karkanias, A.; Ilias, I.; Siafakas, N.; Vgontzas, A.; Tzanakis, N. Prevalence of alexithymia and its association with anxiety and depression in a sample of Greek chronic obstructive pulmonary disease (COPD) outpatients. Ann. Gen. Psychiatry 2010, 9, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, M.; Azzoni, A. Hostility and violence of acute psychiatric inpatients. Clin. Pract. Epidemiol. Ment. Health 2005, 1, 11. [Google Scholar] [CrossRef] [Green Version]
- Ochoa, S.; Suarez, D.; Novick, D.; Arranz, B.; Roca, M.; Baño, V.; Haro, J.M. Factors predicting hostility in outpatients with schizophrenia: 36-month results from the SOHO study. J. Nerv. Ment. Dis. 2013, 201, 464–470. [Google Scholar] [CrossRef]
- Smith, T.W. Concepts and methods in the study of anger, hostility, and health. In Anger, Hostility and the Heart; Siegman, A.W., Smith, T.W., Eds.; Lawrence Erlbaum: Hillsdale, NJ, USA, 1994; pp. 23–42. [Google Scholar]
- Perlini, C.; Bellani, M.; Besteher, B.; Nenadić, I.; Brambilla, P. The neural basis of hostility-related dimensions in schizophrenia. Epidemiol. Psychiatr. Sci. 2018, 27, 546–551. [Google Scholar] [CrossRef]
- Pandey, R.; Saxena, P.; Dubey, A. Emotion regulation difficulties in alexithymia and mental health. Eur. J. Psychol. 2011, 7, 604–623. [Google Scholar] [CrossRef]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Henry, J.D.; Green, M.J.; De Lucia, A.; Restuccia, C.; McDonald, S.; O’Donnell, M. Emotion dysregulation in schizophrenia: Reduced amplification of emotional expression is associated with emotional blunting. Schizophr. Res. 2007, 95, 197–204. [Google Scholar] [CrossRef]
- Henry, J.D.; Rendell, P.G.; Green, M.J.; McDonald, S.; O’Donnell, M. Emotion regulation in schizophrenia: Affective, social and clinical correlates of suppression and reappraisal. J. Abnorm. Psychol. 2008, 117, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, A.L.; McCloskey, M.S.; Kulper, D.; Berman, M.E.; Coccaro, E.F. Selfharm behavior among individuals with intermittent explosive disorder and personality disorders. J. Psychiatr. Res. 2014, 60, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Hornsveld, R.H.J.; Kraaimaat, W. Alexithymia in Dutch violent forensic psychiatric outpatients. Psychol. Crime Law 2012, 18, 833–846. [Google Scholar] [CrossRef]
- Ates, M.A.; Algul, A.; Gulsun, M.; Gecici, O.; Ozdemir, B.; Basoglu, C. The relationship between alexithymia, aggression and psychopathy in young adult males with antisocial personality disorder. Noropsikiyatri Ars. Neuropsychiatry 2009, 46, 135–139. [Google Scholar]
- Teten, A.L.; Miller, L.A.; Bailey, S.D.; Dunn, N.J.; Kent, T.A. Empathic deficits and alexithymia in trauma-related impulsive aggression. Behav. Sci. Law 2008, 26, 823–832. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Reheiser, E.C.; Sydeman, S.J. Measuring the experience, expression, and control of anger. Issues Compr. Pediatr. Nurs. 1995, 18, 207–232. [Google Scholar] [CrossRef]
- Damasio, A.R. Descartes Error: Emotion, Reason and the Human Brain; G P Putnam’s Sons: New York, NY, USA, 1994. [Google Scholar]
- Frith, C.D. The Cognitive Neuropsychology of Schizophrenia; Lawrence Erlbaum: Hove, UK, 1992. [Google Scholar]
- Abu-Akel, A.; Abushua’leh, K. “Theory of mind” in violent and nonviolent patients with paranoid schizophrenia. Schizophr. Res. 2004, 69, 45–53. [Google Scholar] [CrossRef]
- Landsverk, S.S.; Kane, C.F. Antonovsky’s sense of coherence: Theoretical basis of psychoeducation in schizophrenia. Issues Ment. Health Nurs. 1998, 19, 419–431. [Google Scholar]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Torgalsbøen, A.K.; Fu, S.; Czajkowski, N. Resilience trajectories to full recovery in first-episode schizophrenia. Eur. Psychiatry 2018, 52, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Hovland, J.F.; Skogvang, B.O.; Ness, O.; Langeland, E. Development of salutogenic coping skills: Experiences with daily challenges among young adults suffering from serious mental illness. Int. J. Qual. Stud. Health Well-Being 2021, 16, 1879369. [Google Scholar] [CrossRef] [PubMed]
- Pelikan, J.M. The Application of Salutogenesis in Healthcare Settings. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; Chapter 25. [Google Scholar]
- Price, O.; Baker, J.; Bee, P.; Lovell, K. The support-control continuum: An investigation of staff perspectives on factors influencing the success or failure of de-escalation techniques for the management of violence and aggression in mental health settings. Int. J. Nurs. Stud. 2018, 77, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Bhat, S.; Rentala, S.; Nanjegowda, R.B.; Chellappan, X.B. Effectiveness of Milieu Therapy in reducing conflicts and containment rates among schizophrenia patients. Invest. Educ. Enferm. 2020, 38, e06. [Google Scholar] [CrossRef]
- Hasson-Ohayon, I. Integrating cognitive behavioral-based therapy with an intersubjective approach: Addressing metacognitive deficits among people with schizophrenia. J. Psychother. Integr. 2012, 22, 356–374. [Google Scholar] [CrossRef]
- Bell, M.D.; Zito, W.Q.; Greig, T.; Wexler, B.E. Neurocognitive enhancement therapy with vocational services: Work outcomes at two-year follow-up. Schizophr. Res. 2008, 105, 18–29. [Google Scholar] [CrossRef]
- Ahmed, A.O.; Hunter, K.M.; van Houten, E.G.; Monroe, J.M.; Bhat, I.A. Cognition and Other Targets for the Treatment of Aggression in People with Schizophrenia. Ann. Psychiatry Ment. Health 2014, 2, 1004. [Google Scholar]
- Pinna, F.; Manchia, M.; Paribello, P.; Carpiniello, B. The Impact of Alexithymia on Treatment Response in Psychiatric Disorders: A Systematic Review. Front. Psychiatry 2020, 11, 311. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, M.; Franklin, J. Skills-based Treatment for Alexithymia: An Exploratory Case Series. Behav. Chang. 2002, 19, 158–171. [Google Scholar] [CrossRef] [Green Version]
- Rathod, S.; Phiri, P.; Kingdon, D. Cognitive behavioral therapy for schizophrenia. Psychiatr. Clin. North Am. 2010, 33, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.B.; Lehman, A.F. Evidence-based psychotherapy for schizophrenia. J. Nerv. Ment. Dis. 2006, 194, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Darmedru, C.; Demily, C.; Franck, N. Cognitive remediation and social cognitive training for violence in schizophrenia: A systematic review. Psychiatry Res. 2017, 251, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Quinn, J.; Kolla, N.J. From Clozapine to Cognitive Remediation. Can. J. Psychiatry 2017, 62, 94–101. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Min | Max | Mean | SD | |
|---|---|---|---|---|---|
| age | 100 | 21 | 65 | 41.71 | 10.718 |
| education | 98 | 6 | 18 | 13.10 | 3.003 |
| BAQ | 100 | 14 | 54 | 30.93 | 8.247 |
| TAS | 100 | 20 | 82 | 49.10 | 13.369 |
| SOC | 99 | 19 | 89 | 56.57 | 15.697 |
| PA | 100 | 3 | 15 | 6.61 | 3.284 |
| VA | 100 | 4 | 15 | 10.06 | 2.473 |
| H | 100 | 3 | 15 | 8.24 | 3.194 |
| A | 100 | 3 | 13 | 6.02 | 2.655 |
| DIF | 100 | 7 | 31 | 16.91 | 6.741 |
| DDF | 100 | 5 | 25 | 13.07 | 4.965 |
| EOT | 100 | 8 | 36 | 19.12 | 5.524 |
| SOC A | 99 | 4 | 28 | 18.82 | 5.530 |
| SOC B | 99 | 5 | 35 | 21.39 | 7.184 |
| SOC C | 99 | 4 | 28 | 16.35 | 5.877 |
| Pearson Correlation N = 100 | AGE | Education (in Years) | Sense of Coherence (SOC) | Toronto Alexithymia Scale (TAS) | |
|---|---|---|---|---|---|
| Education (in years) | r | 0.073 | |||
| p | 0.478 | ||||
| Sense of coherence (SOC) | r | −0.021 | 0.003 | ||
| p | 0.838 | 0.976 | |||
| Toronto Alexithymia Scale (TAS) | r | 0.044 | −0.062 | −0.624 ** | |
| p | 0.664 | 0.545 | 0.000 | ||
| Brief aggression questionnaire (BAQ) | r | 0.058 | 0.057 | −0.653 ** | 0.525 ** |
| p | 0.569 | 0.575 | 0.000 | 0.000 | |
| N = 100 | DIF | DDF | EOT | TAS | SOC A | SOC B | SOC C | SOC | |
|---|---|---|---|---|---|---|---|---|---|
| BAQ | r | 0.579 ** | 0.463 ** | 0.147 | 0.525 ** | −0.366 ** | −0.648 ** | −0.608 ** | −0.525 ** |
| p | 0.000 | 0.000 | 0.144 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| PA | r | 0.435 ** | 0.384 ** | 0.163 | 0.429 ** | −0.298 ** | −0.487 ** | −0.419 ** | −0.485 |
| p | 0.000 | 0.000 | 0.105 | 0.000 | 0.003 | 0.000 | 0.000 | 0.000 | |
| VA | r | 0.140 | −0.127 | −0.004 | 0.116 | 0.068 | −0.261 ** | −0.310 ** | −0.212 * |
| p | 0.166 | 0.207 | 0.967 | 0.251 | 0.506 | 0.009 | 0.002 | 0.035 | |
| H | r | 0.444 ** | 0.292 ** | 0.151 | 0.394 ** | −0.328 ** | −0.534 ** | −0.456 ** | −0.531 ** |
| p | 0.000 | 0.003 | 0.135 | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | |
| A | r | 0.595 ** | 0.495 ** | 0.078 | 0.516 ** | −0.433 ** | −0.517 ** | −0.526 ** | −0.586 ** |
| p | 0.000 | 0.000 | 0.442 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Unstandardized Coefficients | Standardized Coefficients | |||||||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | t | Sig. | R Square | ∆R 2 | ||
| Step 1 | (constant) | 26.906 | 4.740 | 5.676 | 0.000 | 0.009 | 0.009 | |
| age | 0.053 | 0.080 | 0.072 | 0.660 | 0.511 | |||
| gender | −0.533 | 1.771 | −0.034 | −0.301 | 0.764 | |||
| education | 0.170 | 0.278 | 0.065 | 0.613 | 0.542 | |||
| Step 2 | (constant) | 11.954 | 4.850 | 2.465 | 0.016 | 0.270 | 0.261 | |
| age | 0.046 | 0.069 | 0.063 | 0.666 | 0.507 | |||
| gender | −1.183 | 1.532 | −0.075 | −0.772 | 0.442 | |||
| education | 0.273 | 0.241 | 0.104 | 1.135 | 0.259 | |||
| TAS | 0.306 | 0.053 | 0.514 | 5.737 | 0.000 * | |||
| Step 3 | (constant) | 37.840 | 6.391 | 5.921 | 0.000 | 0.448 | 0.178 | |
| age | 0.048 | 0.060 | 0.066 | 0.800 | 0.426 | |||
| gender | −1.410 | 1.340 | −0.089 | −1.052 | 0.296 | |||
| education | 0.235 | 0.211 | 0.089 | 1.117 | 0.267 | |||
| TAS | 0.108 | 0.059 | 0.180 | 1.811 | 0.073 | |||
| SOC | −0.272 | 0.050 | −0.538 | −5.414 | 0.000 * | |||
| Dependent Variables | Unstandardized Coefficients | Standardized Coefficients | ||||||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | t | p | R Square | ∆R 2 | ||
| BAQ | DIF | 0.287 | 0.146 | 0.232 | 1.967 | 0.05 * | 33.4 | 33.4 |
| SOC B | −0.415 | 0.136 | −0.363 | −3.045 | 0.003 ** | 49.9 | 16.5 | |
| SOC C | −0.349 | 0.149 | −0.250 | −2.340 | 0.021 * | |||
| PA | SOC B | −0.134 | 0.066 | −0.291 | −2.041 | 0.044 * | 27.9 | 7.4 |
| VA | SOC A | 0.142 | 0.044 | 0.319 | 2.609 | 0.011 * | 17.1 | 15.3 |
| SOC C | −0.118 | 0.058 | −0.281 | −2.051 | 0.043 * | |||
| H | SOC B | −0.174 | 0.062 | −0.392 | −2.833 | 0.006 ** | 32.5 | 13.2 |
| A | DIF | 0.117 | 0.050 | 0.294 | 2.335 | 0.022 * | 42.7 | 5.9 |
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
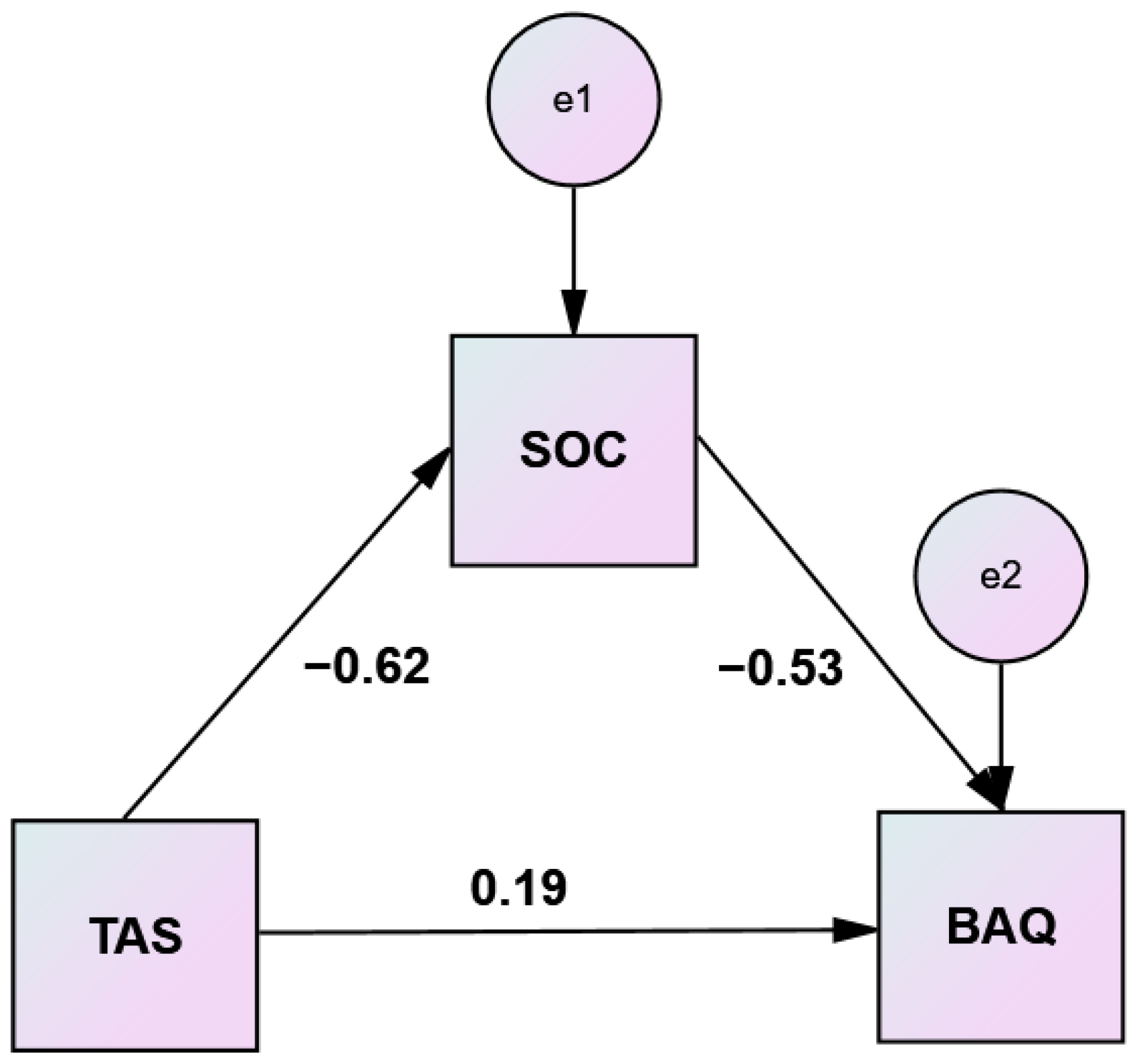
| TAS → SOC | −0.7367 | 0.0936 | −7.8672 | 0.000 | −0.9225 | −0.5508 |
| TAS → BAQ | 0.3193 | 0.0538 | 5.9358 | 0.000 | 0.2125 | 0.4260 |
| TAS → SOC → BAQ | −0.2841 | 0.0510 | −5.5764 | 0.000 | −0.3853 | −0.1830 |
| Effects | ||||||
| Direct | 0.1100 | 0.0601 | 1.8285 | 0.0706 | −0.0094 | 0.2293 |
| Indirect * | 0.2093 | 0.0445 | 0.1234 | 0.2966 | ||
| Total | 0.3193 | 0.0538 | 5.9358 | 0.000 | 0.2125 | 0.4260 |
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
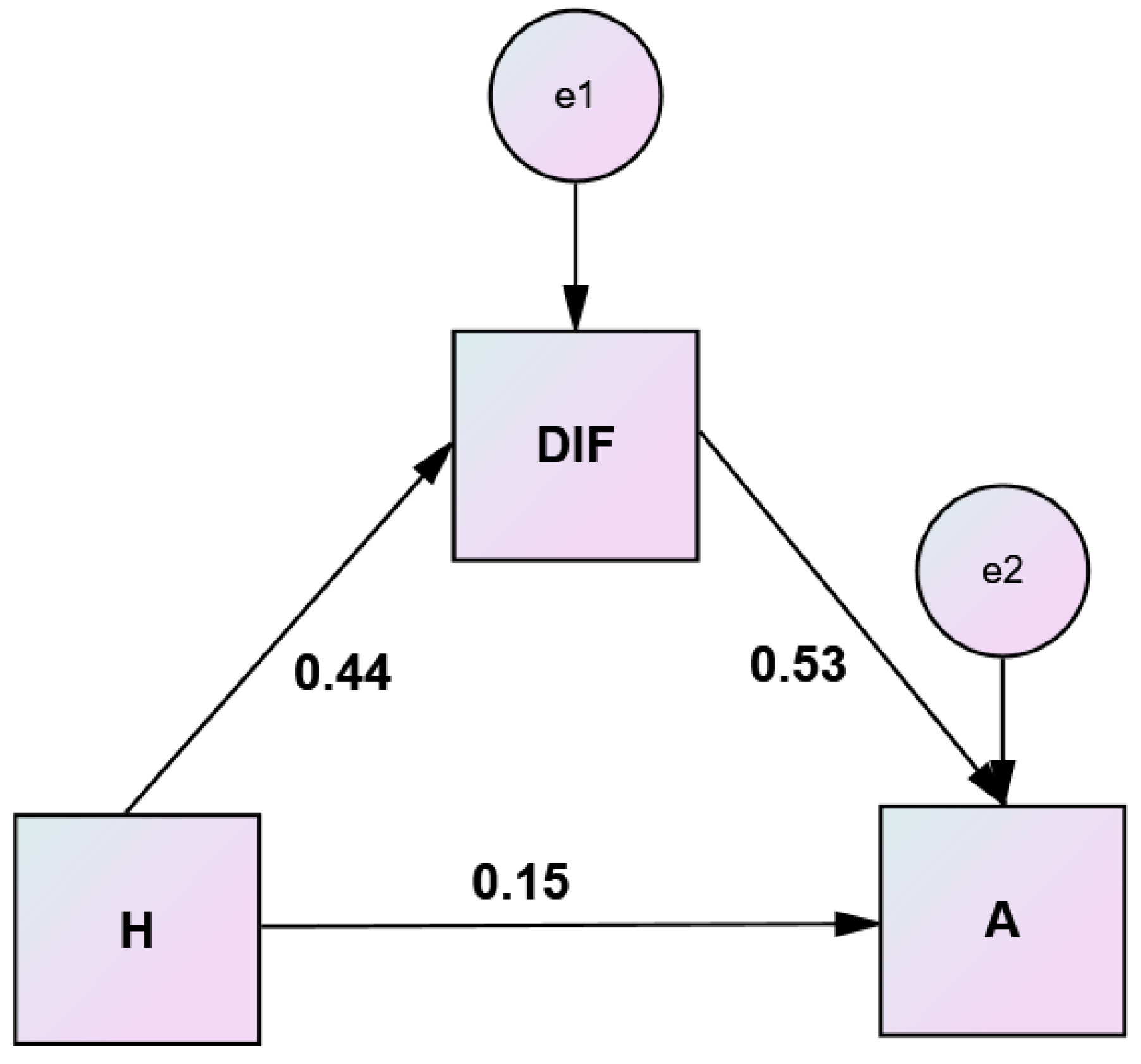
| H → DIF | 0.9366 | 0.1910 | 4.9033 | 0.0000 | 0.5575 | 1.3156 |
| H → A | 0.3202 | 0.0775 | 4.1331 | 0.0001 | 0.1665 | 0.4740 |
| H → DIF → A | 0.2080 | 0.0354 | 5.8810 | 0.0000 | 0.1378 | 0.2782 |
| Effects | ||||||
| Direct | 0.1255 | 0.0746 | 1.6814 | 0.0959 | −0.0226 | 0.2736 |
| Indirect * | 0.1948 | 0.0493 | 0.1041 | 0.2975 | ||
| Total | 0.3202 | 0.0775 | 4.1331 | 0.0001 | 0.1665 | 0.4740 |
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
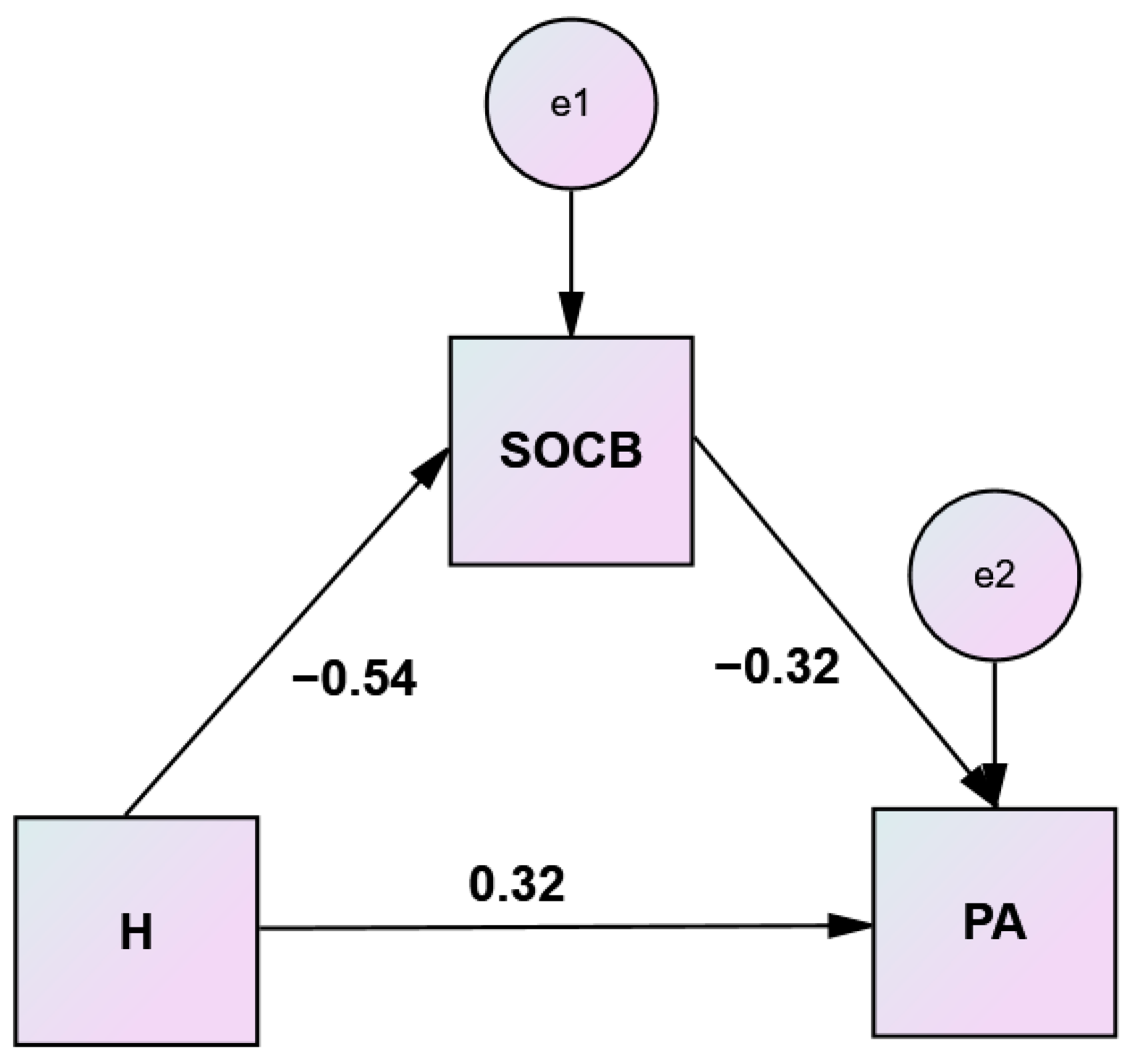
| H → SOC B | −1.2002 | 0.1928 | −6.2264 | 0.0000 | −1.5828 | −0.8176 |
| H → PA | 0.5052 | 0.0913 | 5.5346 | 0.0000 | 0.3241 | 0.6863 |
| H → SOC B → PA | −0.1446 | 0.0460 | −3.1416 | 0.0022 | −0.2359 | −0.0532 |
| Effects | ||||||
| Direct | 0.3317 | 0.1033 | 3.2095 | 0.0018 | 0.1266 | 0.5368 |
| Indirect * | 0.1735 | 0.0657 | 0.0539 | 0.3085 | ||
| Total | 0.5052 | 0.0913 | 5.5346 | 0.0000 | 0.3241 | 0.6863 |
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
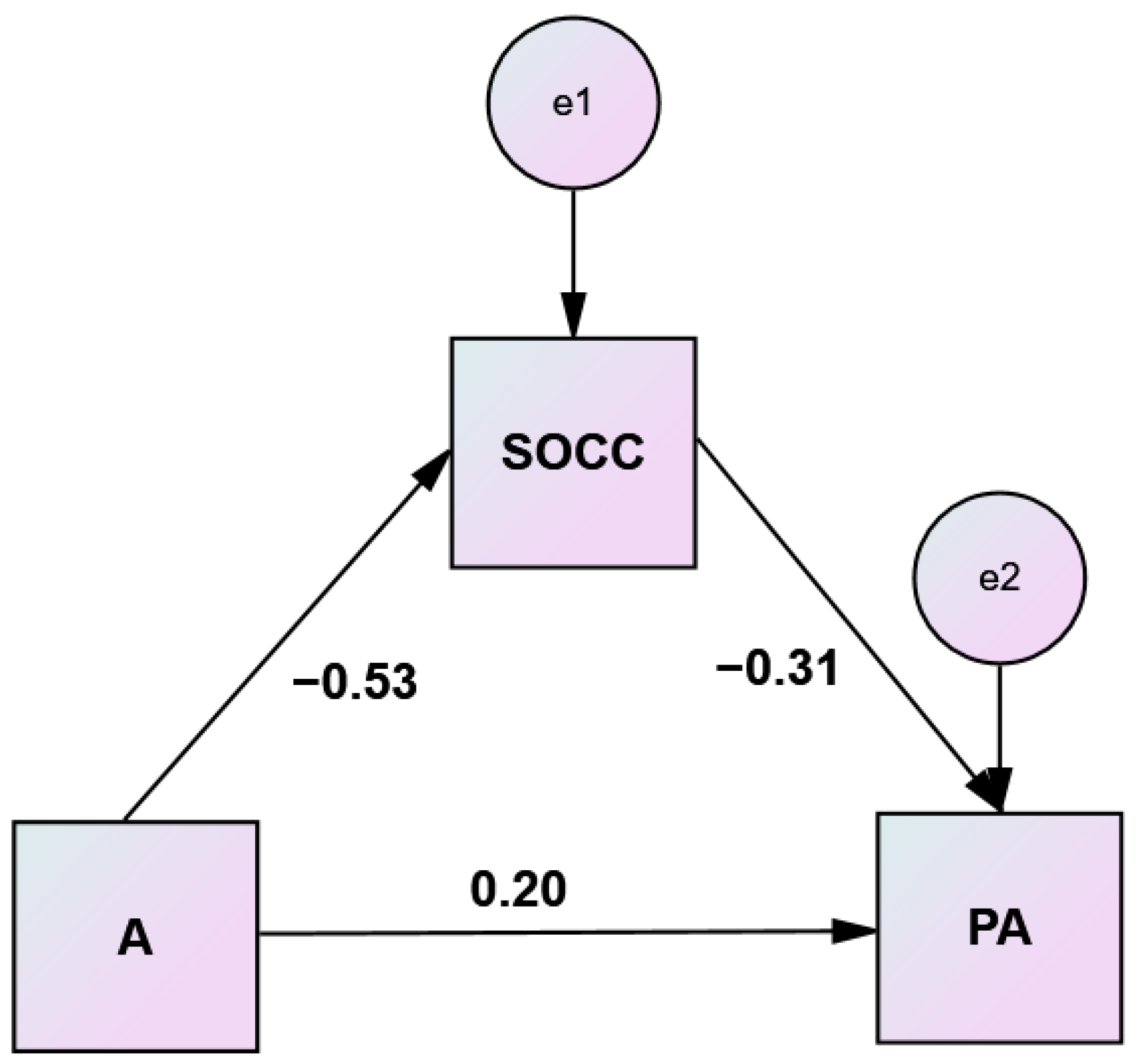
| A → SOC C | −1.1650 | 0.1914 | −6.0850 | 0.0000 | −1.5449 | −0.7850 |
| A → PA | 0.4552 | 0.1175 | 3.8728 | 0.0002 | 0.2219 | 0.6884 |
| A → SOC C → PA | −0.1758 | 0.0600 | −2.9278 | 0.0043 | −0.2949 | −0.0566 |
| Effects | ||||||
| Direct | 0.2504 | 0.1331 | 1.8820 | 0.0626 | −0.0137 | 0.5145 |
| Indirect * | 0.2048 | 0.0771 | 0.0594 | 0.3617 | ||
| Total | 0.4552 | 0.1175 | 3.8728 | 0.0002 | 0.2219 | 0.6884 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pachi, A.; Tselebis, A.; Ilias, I.; Tsomaka, E.; Papageorgiou, S.M.; Baras, S.; Kavouria, E.; Giotakis, K. Aggression, Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients. Healthcare 2022, 10, 1078. https://doi.org/10.3390/healthcare10061078
Pachi A, Tselebis A, Ilias I, Tsomaka E, Papageorgiou SM, Baras S, Kavouria E, Giotakis K. Aggression, Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients. Healthcare. 2022; 10(6):1078. https://doi.org/10.3390/healthcare10061078
Chicago/Turabian StylePachi, Argyro, Athanasios Tselebis, Ioannis Ilias, Effrosyni Tsomaka, Styliani Maria Papageorgiou, Spyros Baras, Evgenia Kavouria, and Konstantinos Giotakis. 2022. "Aggression, Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients" Healthcare 10, no. 6: 1078. https://doi.org/10.3390/healthcare10061078