
The Psychological Impact of Coronavirus Disease 2019 on Patients Attending a Tertiary Healthcare Facility in Pakistan: A Cross-Sectional Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
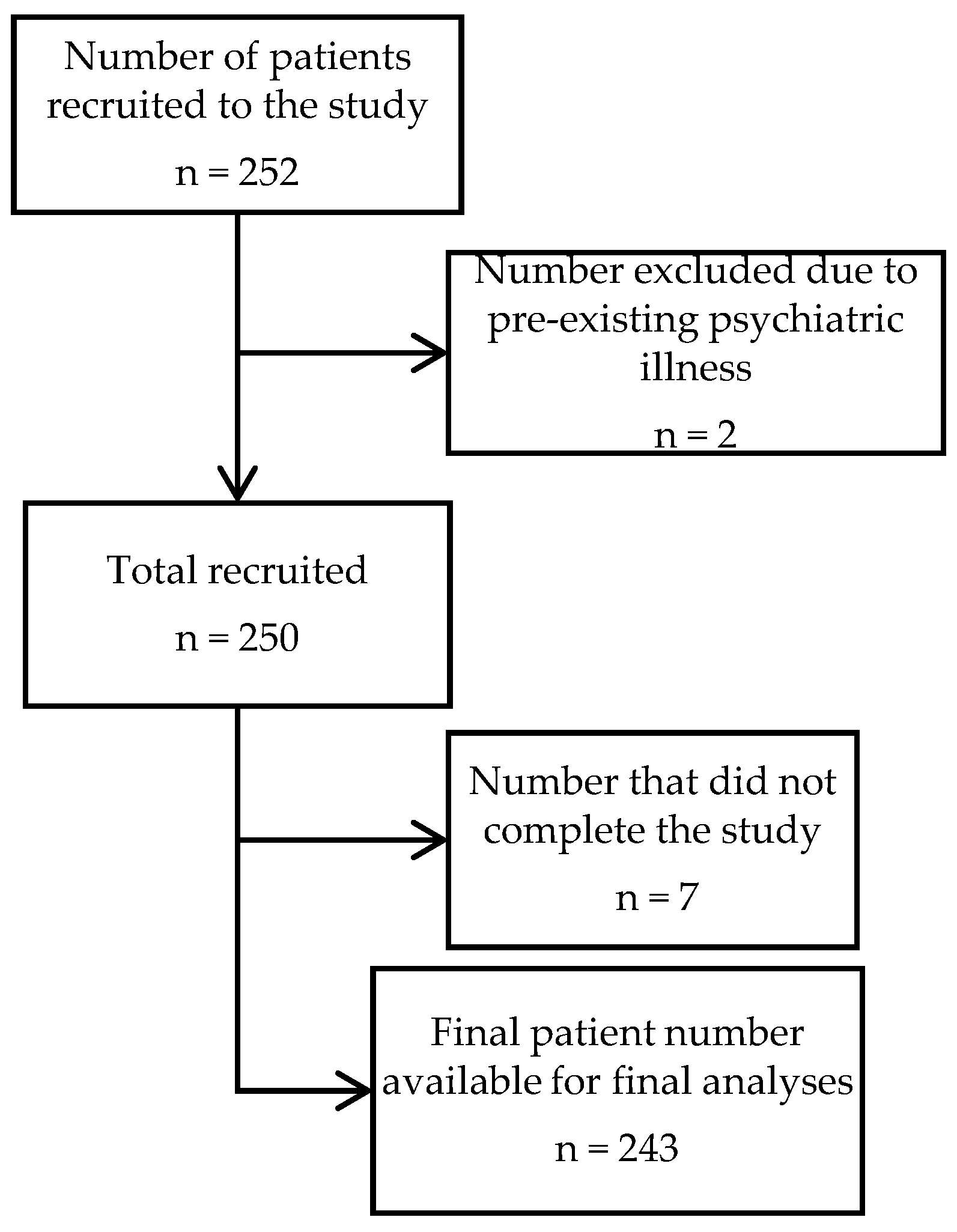
2.2. Participants and Sample Size
2.3. Questionnaire Development
2.3.1. Demographic Data
2.3.2. Severity of COVID-19
2.3.3. Depression, Anxiety and Stress Scale-21 (DASS-21)
2.3.4. Assessment of Post-Traumatic Stress Disorder using PTSD Checklist for DSM-5 (PCL-5)
2.4. Statistical Analysis
3. Results
3.1. Demographics of the Study Participants
3.2. Depression, Anxiety, Stress and PTSD Measurements
4. Discussion
5. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ji, Y.; Ma, Z.; Peppelenbosch, M.P.; Pan, Q. Potential association between COVID-19 mortality and health-care resource availability. Lancet Glob. Health 2020, 8, e480. [Google Scholar] [CrossRef] [Green Version]
- Abid, K.; Bari, Y.A.; Younas, M.; Tahir Javaid, S.; Imran, A. Progress of COVID-19 Epidemic in Pakistan. Asia Pac. J. Public Health 2020, 32, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S. Another decade, another coronavirus. N. Engl. J. Med. 2020, 382, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatrics 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahedian-Azimi, A.; Moayed, M.S.; Rahimibashar, F.; Shojaei, S.; Ashtari, S.; Pourhoseingholi, M.A. Comparison of the severity of psychological distress among four groups of an Iranian population regarding COVID-19 pandemic. BMC Psychiatry 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef]
- Norton, P.J. Depression Anxiety and Stress Scales (DASS-21): Psychometric analysis across four racial groups. Anxiety Stress Coping 2007, 20, 253–265. [Google Scholar] [CrossRef]
- Osorio, F.L.; Silva, T.D.A.D.; Santos, R.G.D.; Chagas, M.H.N.; Chagas, N.M.S.; Sanches, R.F.; Crippa, J.A.D.S. Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Transcultural adaptation of the Brazilian version. Arch. Clin. Psychiatry 2017, 44, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Hayat, K.; Haq, M.; Wang, W.; Khan, F.U.; Rehman, A.U.; Rasool, M.; Kadirhaz, M.; Omer, S.; Rasheed, U.; Fang, Y. Impact of the COVID-19 outbreak on mental health status and associated factors among general population: A cross-sectional study from Pakistan. Psychol. Health Med. 2021, 27, 54–68. [Google Scholar] [CrossRef]
- Ng, Q.X.; De Deyn, M.L.Z.Q.; Lim, D.Y.; Chan, H.W.; Yeo, W.S. The wounded healer: A narrative review of the mental health effects of the COVID-19 pandemic on healthcare workers. Asian J. Psychiatr. 2020, 54, 102258. [Google Scholar] [CrossRef]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.M.T.; Furlan, R.; Ciceri, F.; Rovere-Querini, P. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Tansey, C.M.; Louie, M.; Loeb, M.; Gold, W.L.; Muller, M.P.; de Jager, J.; Cameron, J.I.; Tomlinson, G.; Mazzulli, T.; Walmsley, S.L. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch. Intern. Med. 2007, 167, 1312–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moldofsky, H.; Patcai, J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Baumeister, R.F.; Veilleux, J.C.; Chen, C.; Liu, W.; Yue, Y.; Zhang, S. Risk factors associated with mental illness in hospital discharged patients infected with COVID-19 in Wuhan, China. Psychiatry Res. 2020, 292, 113297. [Google Scholar] [CrossRef] [PubMed]
- WHO. 2020. Available online: https://www.who.int/health-topics/mental-health#tab=tab_1 (accessed on 14 May 2022).
- Oei, T.P.; Sawang, S.; Goh, Y.W.; Mukhtar, F. Using the depression anxiety stress scale 21 (DASS-21) across cultures. Int. J. Psychol. 2013, 48, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, M.S.; Sujan, M.S.H.; Tasnim, R.; Sikder, M.T.; Potenza, M.N.; Van Os, J. Psychological responses during the COVID-19 outbreak among university students in Bangladesh. PLoS ONE 2020, 15, e0245083. [Google Scholar] [CrossRef]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Asún, R.A.; Rdz-Navarro, K.; Alvarado, J.M. Developing multidimensional Likert scales using item factor analysis: The case of four-point items. Sociol. Methods Res. 2016, 45, 109–133. [Google Scholar] [CrossRef]
- Wortmann, J.H.; Jordan, A.H.; Weathers, F.W.; Resick, P.A.; Dondanville, K.A.; Hall-Clark, B.; Foa, E.B.; Young-McCaughan, S.; Yarvis, J.S.; Hembree, E.A. Psychometric analysis of the PTSD Checklist-5 (PCL-5) among treatment-seeking military service members. Psychol. Assess. 2016, 28, 1392. [Google Scholar] [CrossRef]
- Islam, M.S.; Ferdous, M.Z.; Sujan, M.S.H.; Tasnim, R.; Masud, J.H.B.; Kundu, S.; Mosaddek, A.S.M.; Choudhuri, M.S.K.; Kira, I.A.; Gozal, D. The psychometric properties of the Bangla Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Preliminary reports from a large-scale validation study. BMC Psychiatry 2022, 22, 280. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.; Zhang, Y.; Li, Y.; Zhao, Q.; Bi, Y.; Lu, X.; Kong, Y.; Wang, L.; Lu, Z.; Hu, L. Post-traumatic stress symptoms in COVID-19 survivors: A self-report and brain imaging follow-up study. Mol. Psychiatry 2021, 26, 7475–7480. [Google Scholar] [CrossRef] [PubMed]
- Cullen, W.; Gulati, G.; Kelly, B. Mental health in the COVID-19 pandemic. Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients' clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Morgul, E.; Bener, A.; Atak, M.; Akyel, S.; Aktaş, S.; Bhugra, D.; Ventriglio, A.; Jordan, T.R. COVID-19 pandemic and psychological fatigue in Turkey. Int. J. Soc. Psychiatry 2021, 67, 128. [Google Scholar] [CrossRef] [PubMed]
- Orgilés, M.; Morales, A.; Delvecchio, E.; Mazzeschi, C.; Espada, J.P. Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Front. Psychol. 2020, 11, 2986. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Contextual Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Cai, X.; Hu, X.; Ekumi, I.O.; Wang, J.; An, Y.; Li, Z.; Yuan, B. Psychological distress and its correlates among COVID-19 survivors during early convalescence across age groups. Am. J. Geriatr. Psychiatry 2020, 28, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Krokstad, S.; Mykletun, A.; Dahl, A.A.; Tell, G.S.; Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 2008, 66, 1334–1345. [Google Scholar] [CrossRef]
- Tan, B.Y.; Chew, N.W.; Lee, G.K.; Jing, M.; Goh, Y.; Yeo, L.L.; Zhang, K.; Chin, H.-K.; Ahmad, A.; Khan, F.A. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020, 173, 317–320. [Google Scholar] [CrossRef] [Green Version]
- De Coninck, D.; Frissen, T.; Matthijs, K.; d’Haenens, L.; Lits, G.; Champagne-Poirier, O.; Carignan, M.E.; David, M.D.; Pignard-Cheynel, N.; Salerno, S.; et al. Beliefs in Conspiracy Theories and Misinformation about COVID-19: Comparative Perspectives on the Role of Anxiety, Depression and Exposure to and Trust in Information Sources. Front Psychol. 2021, 12, 646394. [Google Scholar] [CrossRef]
- Su, Z.; McDonnell, D.; Wen, J.; Kozak, M.; Abbas, J.; Šegalo, S.; Li, X.; Ahmad, J.; Cheshmehzangi, A.; Cai, Y.; et al. Mental health consequences of COVID-19 media coverage: The need for effective crisis communication practices. Glob. Health 2021, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Alamri, H.S.; Algarni, A.; Shehata, S.F.; Al Bshabshe, A.; Alshehri, N.N.; ALAsiri, A.M.; Hussain, A.H.; Alalmay, A.Y.; Alshehri, E.A.; Alqarni, Y. Prevalence of depression, anxiety, and stress among the general population in Saudi Arabia during COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 9183. [Google Scholar] [CrossRef] [PubMed]
- Mohta, M.; Sethi, A.; Tyagi, A.; Mohta, A. Psychological care in trauma patients. Injury 2003, 34, 17–25. [Google Scholar] [CrossRef]
- Ng, Q.X.; Chee, K.T.; De Deyn, M.L.Z.Q.; Chua, Z. Staying connected during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2020, 66, 519–520. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Cruz, A.R.; Kammar-García, A.; Mancilla-Galindo, J.; Quezada-Figueroa, G.; Tlalpa-Prisco, M.; Vera-López, O.; Aguilar-Alonso, P.; Lazcano-Hernández, M.; Segura-Badilla, O. Association of Differences in Dietary Behaviours and Lifestyle with Self-Reported Weight Gain during the COVID-19 Lockdown in a University Community from Chile: A Cross-Sectional Study. Nutrients 2021, 13, 3213. [Google Scholar] [CrossRef]


{kind=link}
| Anxiety Levels | ||||||||
|---|---|---|---|---|---|---|---|---|
| Normal | Mild | Moderate | Severe | Extremely Severe | p Value | |||
| Total | n | 117 | 24 | 44 | 30 | 28 | ||
| % | (48.10%) | (9.90%) | (18.10%) | (12.30%) | (11.50%) | |||
| Gender | Male | n | 94 | 16 | 39 | 22 | 19 | 0.31 |
| % | (38.70%) | (6.60%) | (16.00%) | (9.10%) | (7.80%) | |||
| Female | n | 23 | 8 | 5 | 8 | 9 | ||
| % | (9.50%) | (3.30%) | (2.10%) | (3.30%) | (3.70%) | |||
| Age | <20 | n | 1 | 0 | 1 | 1 | 0 | 0.75 |
| % | (0.40%) | (0.00%) | (0.40%) | (0.40%) | (0.00%) | |||
| 20–39 | n | 56 | 14 | 26 | 14 | 11 | ||
| % | (23.00%) | (5.80%) | (10.70%) | (5.80%) | (4.50%) | |||
| 40–59 | n | 42 | 7 | 12 | 12 | 14 | ||
| % | (17.30%) | (2.90%) | (4.90%) | (4.90%) | (5.80%) | |||
| >60 | n | 18 | 3 | 5 | 3 | 3 | ||
| % | (7.40%) | (1.20%) | (2.10%) | (1.20%) | (1.20%) | |||
| Education | Below Graduate Level | n | 41 | 10 | 15 | 7 | 9 | 0.471 |
| % | (16.90%) | (4.10%) | (6.20%) | (2.90%) | (3.70%) | |||
| Graduate | n | 37 | 8 | 17 | 13 | 8 | ||
| % | (15.20%) | (3.30%) | (7.00%) | (5.30%) | (3.30%) | |||
| Physicians | n | 15 | 2 | 4 | 2 | 4 | ||
| % | (6.20%) | (0.80%) | (1.60%) | (0.80%) | (1.60%) | |||
| Post-Graduate Level | n | 24 | 4 | 8 | 8 | 7 | ||
| % | (9.90%) | (1.60%) | (3.30%) | (3.30%) | (2.90%) | |||
| Healthcare Workers | Yes | n | 34 | 5 | 6 | 4 | 7 | 0.10 |
| % | (14.00%) | (2.10%) | (2.50%) | (1.60%) | (2.90%) | |||
| No | n | 83 | 19 | 38 | 26 | 21 | ||
| % | (34.20%) | (7.80%) | (15.60%) | (10.70%) | (8.60%) | |||
| History of Interaction with COVID-19 Patients | Yes | n | 27 | 4 | 3 | 4 | 7 | 0.35 |
| % | (11.10%) | (1.60%) | (1.20%) | (1.60%) | (2.90%) | |||
| No | n | 90 | 20 | 41 | 26 | 21 | ||
| % | (37.00%) | (8.20%) | (16.90%) | (10.70%) | (8.60%) | |||
| Severity of COVID-19 Disease | Mild | n | 59 | 11 | 15 | 15 | 9 | 0.13 |
| % | (24.30%) | (4.50%) | (6.20%) | (6.20%) | (3.70%) | |||
| Moderate | n | 44 | 9 | 25 | 9 | 15 | ||
| % | (18.10%) | (3.70%) | (10.30%) | (3.70%) | (6.20%) | |||
| Severe | n | 14 | 4 | 4 | 6 | 4 | ||
| % | (5.80%) | (1.60%) | (1.60%) | (2.50%) | (1.60%) | |||
| Current Condition | Recovering | n | 91 | 17 | 34 | 25 | 17 | 0.03 |
| % | (37.40%) | (7.00%) | (14.00%) | (10.30%) | (7.00%) | |||
| Same as Before Illness | n | 20 | 6 | 7 | 2 | 3 | ||
| % | (8.20%) | (2.50%) | (2.90%) | (0.80%) | (1.20%) | |||
| Getting Worse | n | 6 | 1 | 3 | 3 | 8 | ||
| % | (2.50%) | (0.40%) | (1.20%) | (1.20%) | (3.30%) | |||
| Depression Levels | ||||||||
|---|---|---|---|---|---|---|---|---|
| Normal | Mild | Moderate | Severe | Extremely Severe | p Value | |||
| Total | n | 139 | 42 | 40 | 14 | 8 | ||
| % | (57.20%) | (17.30%) | (16.50%) | (5.80%) | (3.30%) | |||
| Gender | Male | n | 109 | 31 | 29 | 13 | 8 | 0.34 |
| % | (44.90%) | (12.80%) | (11.90%) | (5.30%) | (3.30%) | |||
| Female | n | 30 | 11 | 11 | 1 | 0 | ||
| % | (12.30%) | (4.50%) | (4.50%) | (0.40%) | (0.00%) | |||
| Age | <20 | n | 2 | 0 | 0 | 1 | 0 | 0.83 |
| % | (0.80%) | (0.00%) | (0.00%) | (0.40%) | (0.00%) | |||
| 20–39 | n | 71 | 21 | 19 | 6 | 4 | ||
| % | (29.20%) | (8.60%) | (7.80%) | (2.50%) | (1.60%) | |||
| 40–59 | n | 48 | 13 | 18 | 6 | 2 | ||
| % | (19.80%) | (5.30%) | (7.40%) | (2.50%) | (0.80%) | |||
| >60 | n | 18 | 8 | 3 | 1 | 2 | ||
| % | (7.40%) | (3.30%) | (1.20%) | (0.40%) | (0.80%) | |||
| Education | Below Graduate Level | n | 57 | 8 | 12 | 5 | 0 | 0.04 |
| % | (23.50%) | (3.30%) | (4.90%) | (2.10%) | (0.00%) | |||
| Graduate | n | 40 | 22 | 14 | 4 | 3 | ||
| % | (16.50%) | (9.10%) | (5.80%) | (1.60%) | (1.20%) | |||
| Physicians | n | 15 | 4 | 4 | 1 | 3 | ||
| % | (6.20%) | (1.60%) | (1.60%) | (0.40%) | (1.20%) | |||
| Post-Graduate Level | n | 27 | 8 | 10 | 4 | 2 | ||
| % | (11.10%) | (3.30%) | (4.10%) | (1.60%) | (0.80%) | |||
| Healthcare Workers | Yes | n | 34 | 9 | 9 | 1 | 3 | 0.66 |
| % | (14.00%) | (3.70%) | (3.70%) | (0.40%) | (1.20%) | |||
| No | n | 105 | 33 | 31 | 13 | 5 | ||
| % | (43.20%) | (13.60%) | (12.80%) | (5.30%) | (2.10%) | |||
| History of Interaction with COVID-19 Patients | Yes | n | 27 | 7 | 7 | 1 | 3 | 0.96 |
| % | (11.10%) | (2.90%) | (2.90%) | (0.40%) | (1.20%) | |||
| No | n | 112 | 35 | 33 | 13 | 5 | ||
| % | (46.10%) | (14.40%) | (13.60%) | (5.30%) | (2.10%) | |||
| Severity of COVID-19 Disease | Mild | n | 71 | 19 | 12 | 4 | 3 | 0.03 |
| % | (29.20%) | (7.80%) | (4.90%) | (1.60%) | (1.20%) | |||
| Moderate | n | 49 | 19 | 26 | 5 | 3 | ||
| % | (20.20%) | (7.80%) | (10.70%) | (2.10%) | (1.20%) | |||
| Severe | n | 19 | 4 | 2 | 5 | 2 | ||
| % | (7.80%) | (1.60%) | (0.80%) | (2.10%) | (0.80%) | |||
| Current Condition | Recovering | n | 109 | 35 | 23 | 10 | 7 | 0.04 |
| % | (44.90%) | (14.40%) | (9.50%) | (4.10%) | (2.90%) | |||
| Same as Before Illness | n | 21 | 7 | 9 | 1 | 0 | ||
| % | (8.60%) | (2.90%) | (3.70%) | (0.40%) | (0.00%) | |||
| Getting Worse | n | 9 | 0 | 8 | 3 | 1 | ||
| % | (3.70%) | (0.00%) | (3.30%) | (1.20%) | (0.40%) | |||
| Stress Levels | ||||||||
|---|---|---|---|---|---|---|---|---|
| Normal | Mild | Moderate | Severe | Extremely Severe | p Value | |||
| Total | n | 141 | 57 | 32 | 7 | 6 | ||
| % | (58.00%) | (23.50%) | (13.20%) | (2.90%) | (2.50%) | |||
| Gender | Male | n | 110 | 43 | 25 | 7 | 5 | 0.50 |
| % | (45.30%) | (17.70%) | (10.30%) | (2.90%) | (2.10%) | |||
| Female | n | 31 | 14 | 7 | 0 | 1 | ||
| % | (12.80%) | (5.80%) | (2.90%) | (0.00%) | (0.40%) | |||
| Age | <20 | n | 1 | 1 | 1 | 0 | 0 | 0.79 |
| % | (0.40%) | (0.40%) | (0.40%) | (0.00%) | (0.00%) | |||
| 20–39 | n | 73 | 27 | 17 | 2 | 2 | ||
| % | (30.00%) | (11.10%) | (7.00%) | (0.80%) | (0.80%) | |||
| 40–59 | n | 46 | 22 | 12 | 5 | 2 | ||
| % | (18.90%) | (9.10%) | (4.90%) | (2.10%) | (0.80%) | |||
| >60 | n | 21 | 7 | 2 | 0 | 2 | ||
| % | (8.60%) | (2.90%) | (0.80%) | (0.00%) | (0.80%) | |||
| Education | Below Graduate Level | n | 50 | 18 | 12 | 1 | 1 | 0.35 |
| % | (20.60%) | (7.40%) | (4.90%) | (0.40%) | (0.40%) | |||
| Graduate | n | 48 | 19 | 11 | 2 | 3 | ||
| % | (19.80%) | (7.80%) | (4.50%) | (0.80%) | (1.20%) | |||
| Physicians | n | 16 | 6 | 3 | 1 | 1 | ||
| % | (6.60%) | (2.50%) | (1.20%) | (0.40%) | (0.40%) | |||
| Post-Graduate Level | n | 27 | 14 | 6 | 3 | 1 | ||
| % | (11.10%) | (5.80%) | (2.50%) | (1.20%) | (0.40%) | |||
| Healthcare Workers | Yes | n | 36 | 13 | 5 | 1 | 1 | 0.19 |
| % | (14.80%) | (5.30%) | (2.10%) | (0.40%) | (0.40%) | |||
| No | n | 105 | 44 | 27 | 6 | 5 | ||
| % | (43.20%) | (18.10%) | (11.10%) | (2.50%) | (2.10%) | |||
| History of Interaction with COVID-19 Patients | Yes | n | 28 | 11 | 4 | 1 | 1 | 0.42 |
| % | (11.50%) | (4.50%) | (1.60%) | (0.40%) | (0.40%) | |||
| No | n | 113 | 46 | 28 | 6 | 5 | ||
| % | (46.50%) | (18.90%) | (11.50%) | (2.50%) | (2.10%) | |||
| Severity of COVID-19 Disease | Mild | n | 70 | 25 | 11 | 2 | 1 | 0.04 |
| % | (28.80%) | (10.30%) | (4.50%) | (0.80%) | (0.40%) | |||
| Moderate | n | 54 | 24 | 17 | 3 | 4 | ||
| % | (22.20%) | (9.90%) | (7.00%) | (1.20%) | (1.60%) | |||
| Severe | n | 17 | 8 | 4 | 2 | 1 | ||
| % | (7.00%) | (3.30%) | (1.60%) | (0.80%) | (0.40%) | |||
| Current Condition | Recovering | n | 110 | 47 | 19 | 3 | 5 | 0.01 |
| % | (45.30%) | (19.30%) | (7.80%) | (1.20%) | (2.10%) | |||
| Same as Before Illness | n | 24 | 6 | 7 | 0 | 1 | ||
| % | (9.90%) | (2.50%) | (2.90%) | (0.00%) | (0.40%) | |||
| Getting Worse | n | 7 | 4 | 6 | 4 | 0 | ||
| % | (2.90%) | (1.60%) | (2.50%) | (1.60%) | (0.00%) | |||
| PTSD | |||||
|---|---|---|---|---|---|
| No | Yes | p Value | |||
| Total | n | 224 | 19 | ||
| % | (92.2%) | (7.8%) | |||
| Gender | Male | n | 177 | 13 | 0.28 |
| % | (72.8%) | (5.3%) | |||
| Female | n | 47 | 6 | ||
| % | (19.3%) | (2.5%) | |||
| Age | <20 | n | 3 | 0 | 0.61 |
| % | (1.2%) | (0.0%) | |||
| 20–39 | n | 114 | 7 | ||
| % | (46.9%) | (2.9%) | |||
| 40–59 | n | 78 | 9 | ||
| % | (32.1%) | (3.7%) | |||
| >60 | n | 29 | 3 | ||
| % | (11.9%) | (1.2%) | |||
| Education | Below Graduate Level | n | 78 | 4 | 0.54 |
| % | (32.1%) | (1.6%) | |||
| Graduate | n | 76 | 7 | ||
| % | (31.3%) | (2.9%) | |||
| Physicians | n | 25 | 2 | ||
| % | (10.3%) | (0.8%) | |||
| Post-Graduate Level | n | 45 | 6 | ||
| % | (18.5%) | (2.5%) | |||
| Healthcare Workers | Yes | n | 53 | 3 | 0.43 |
| % | (21.8%) | (1.2%) | |||
| No | n | 171 | 16 | ||
| % | (70.4%) | (6.6%) | |||
| History of Interaction with COVID-19 Patients | Yes | n | 42 | 3 | 0.75 |
| % | (17.3%) | (1.2%) | |||
| No | n | 182 | 16 | ||
| % | (74.9%) | (6.6%) | |||
| Severity of COVID-19 Disease | Mild | n | 106 | 3 | 0.02 |
| % | (43.6%) | (1.2%) | |||
| Moderate | n | 89 | 13 | ||
| % | (36.6%) | (5.3%) | |||
| Severe | n | 29 | 3 | ||
| % | (11.9%) | (1.2%) | |||
| Current Condition | Recovering | n | 172 | 12 | 0.01 |
| % | (70.8%) | (4.9%) | |||
| Same as Before Illness | n | 36 | 2 | ||
| % | (14.8%) | (0.8%) | |||
| Getting Worse | n | 16 | 5 | ||
| % | (6.6%) | (2.1%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, U.A.; Iftikhar, N.; Amat-ur-Rasool, H.; Ahmed, M.; Hafeez, J.; Carter, W.G. The Psychological Impact of Coronavirus Disease 2019 on Patients Attending a Tertiary Healthcare Facility in Pakistan: A Cross-Sectional Study. Healthcare 2022, 10, 1049. https://doi.org/10.3390/healthcare10061049
Ali UA, Iftikhar N, Amat-ur-Rasool H, Ahmed M, Hafeez J, Carter WG. The Psychological Impact of Coronavirus Disease 2019 on Patients Attending a Tertiary Healthcare Facility in Pakistan: A Cross-Sectional Study. Healthcare. 2022; 10(6):1049. https://doi.org/10.3390/healthcare10061049
Chicago/Turabian StyleAli, Umar Abdul, Nadia Iftikhar, Hafsa Amat-ur-Rasool, Mehboob Ahmed, Javeria Hafeez, and Wayne G. Carter. 2022. "The Psychological Impact of Coronavirus Disease 2019 on Patients Attending a Tertiary Healthcare Facility in Pakistan: A Cross-Sectional Study" Healthcare 10, no. 6: 1049. https://doi.org/10.3390/healthcare10061049