
Effects of Abdominal Microcurrent in the Consumption and Proportion of Energy Substrates during Aerobic Exercise: A Pilot Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
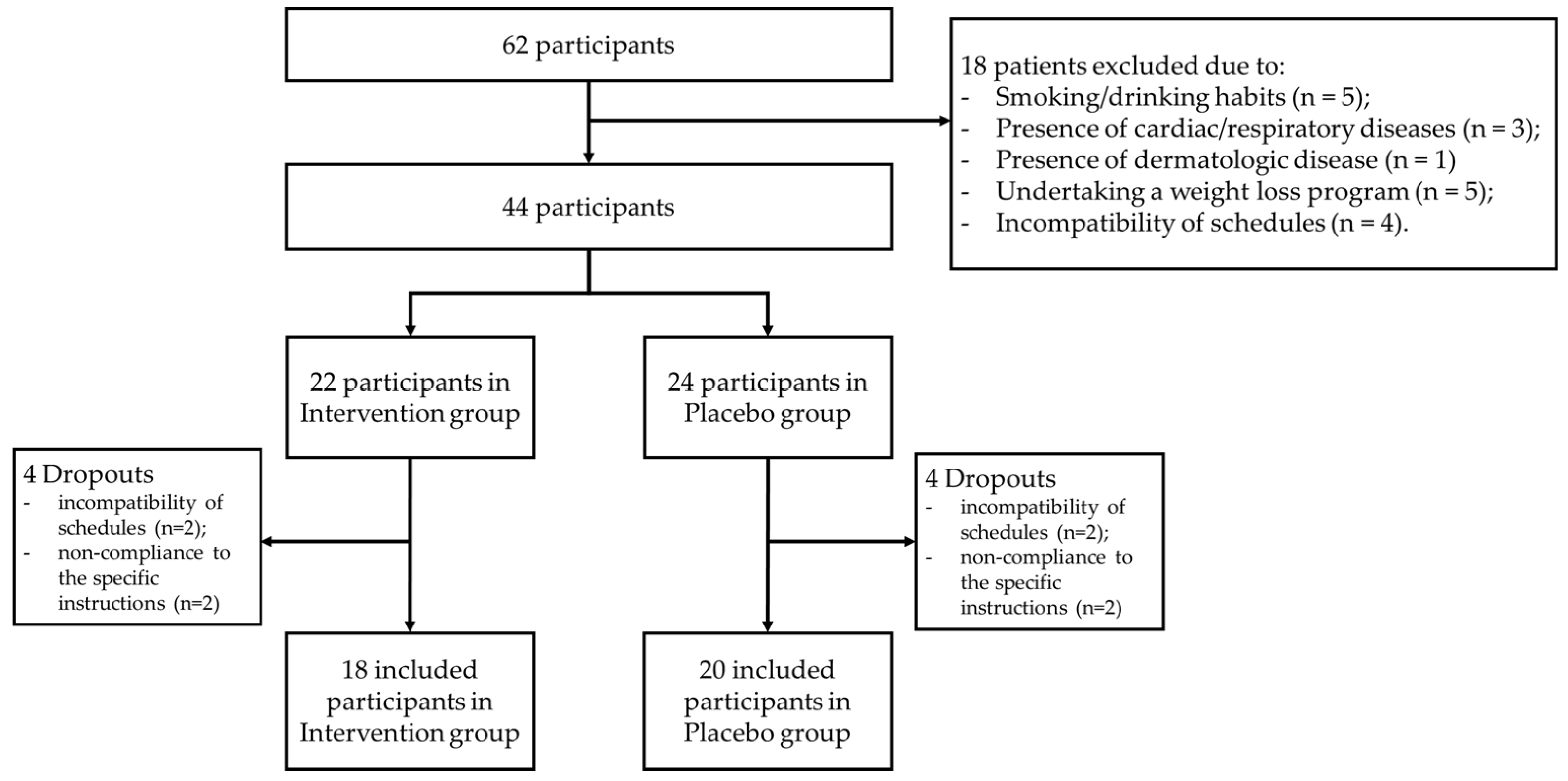
2.1. Study Design, Participants
2.2. Sample Size
2.3. Intervention
2.4. Measurements
Substrate Oxidation and RER Values
2.5. Statistical Analysis
3. Results
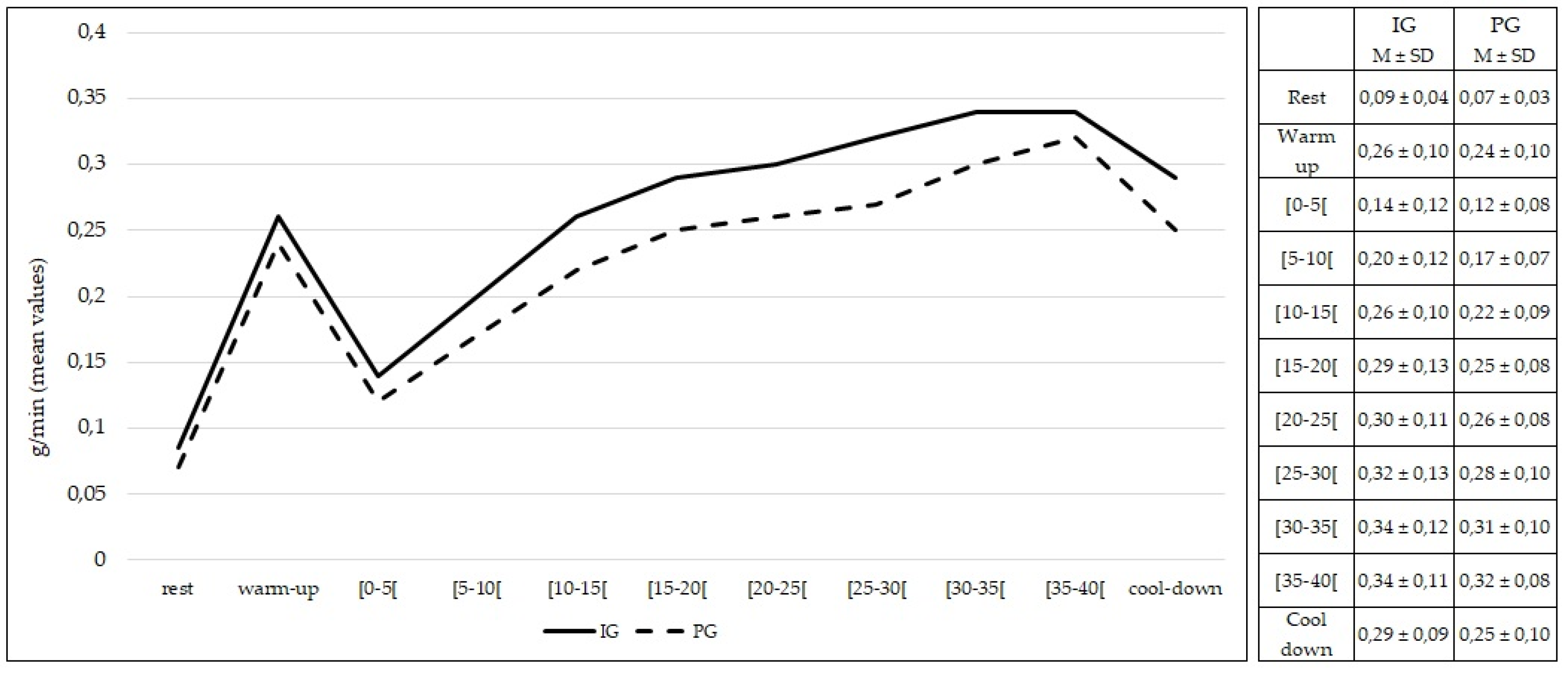
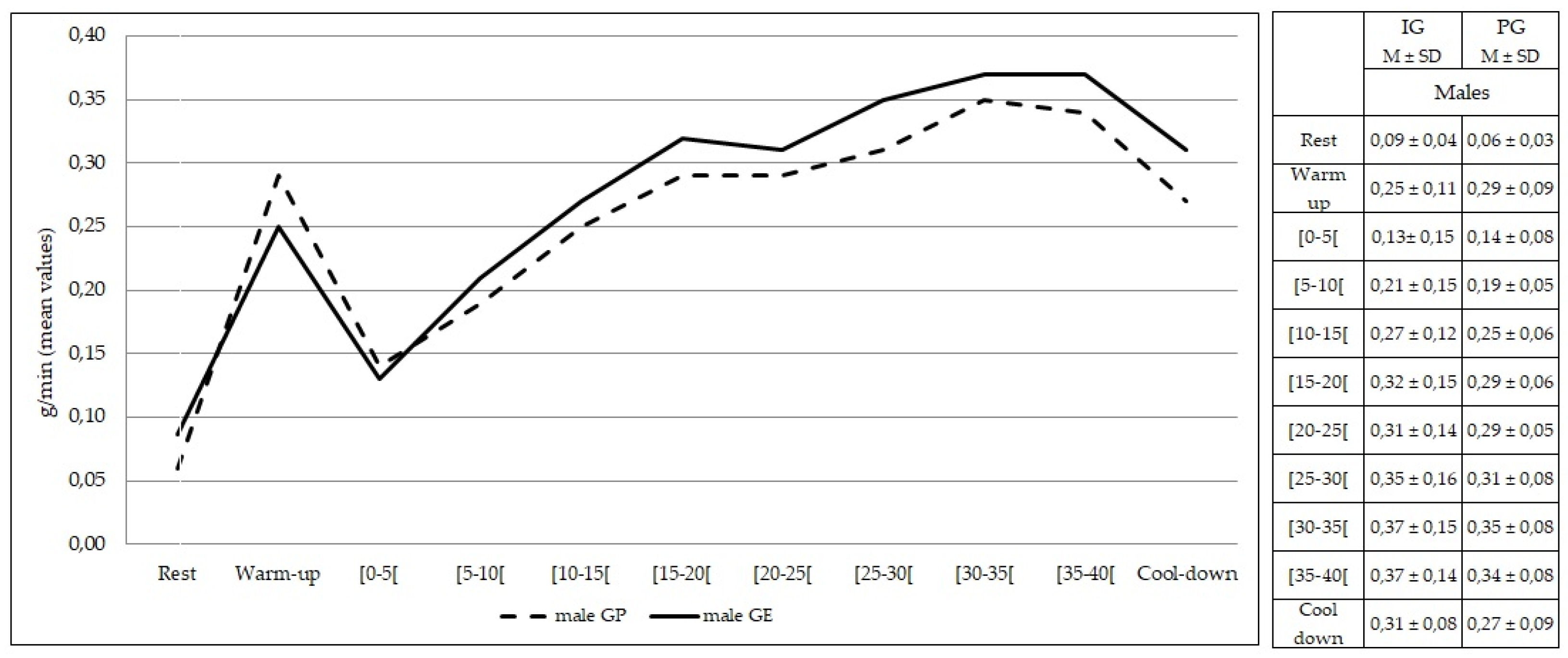
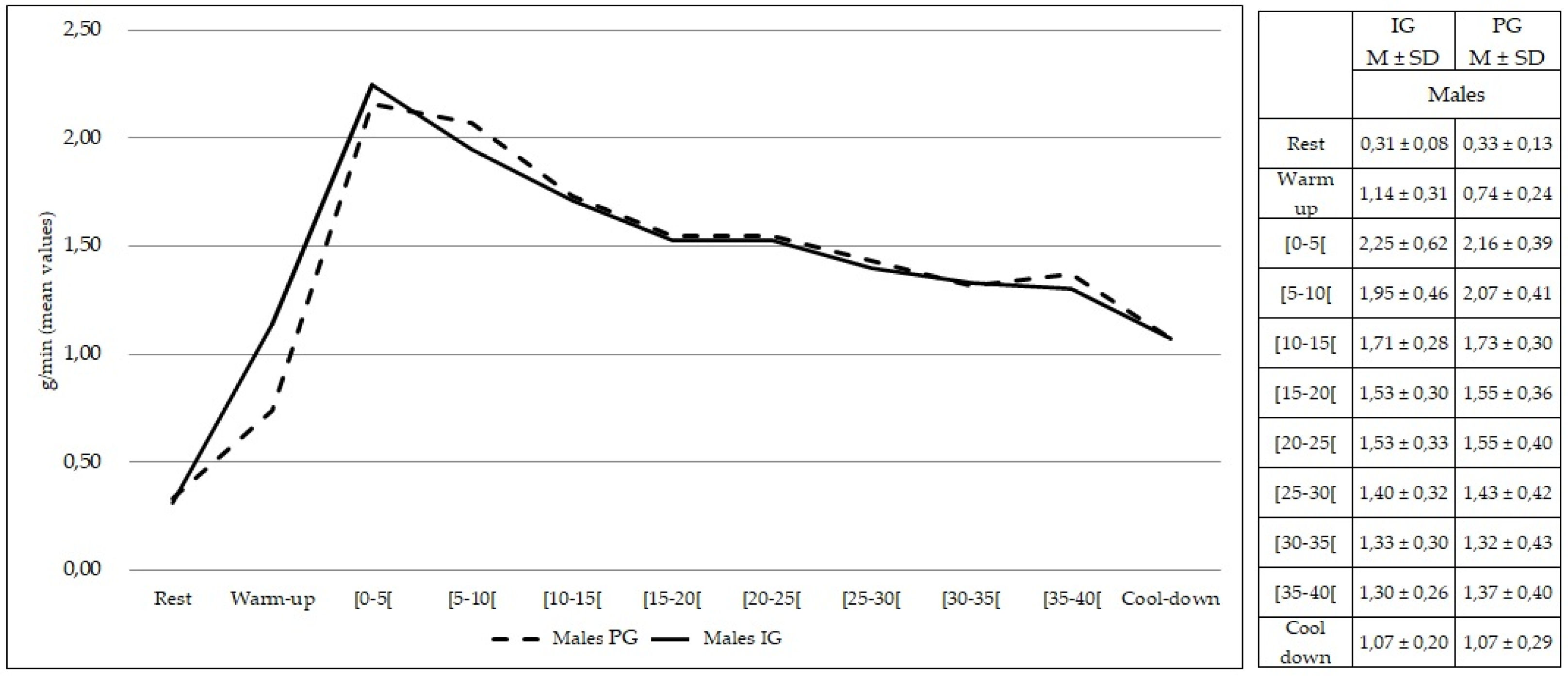
3.1. Lipid and Carbohydrate Consumption
3.2. Substrate Energy Proportion—Respiratory Exchange Ratio
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kolnes, K.J.; Petersen, M.H.; Lien-Iversen, T.; Højlund, K.; Jensen, J. Effect of Exercise Training on Fat Loss—Energetic Perspectives and the Role of Improved Adipose Tissue Function and Body Fat Distribution. Front. Physiol. 2021, 12, 737709. [Google Scholar] [CrossRef] [PubMed]
- Arner, P.; Bernard, S.; Salehpour, M.; Possnert, G.; Liebl, J.; Steier, P.; Buchholz, B.A.; Eriksson, M.; Arner, E.; Hauner, H.; et al. Dynamics of human adipose lipid turnover in health and metabolic disease. Nature 2011, 478, 110–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lafontan, M. Adipose tissue and adipocyte dysregulation. Diabetes Metab. 2014, 40, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Virtue, S.; Vidal-Puig, A. Adipose tissue expandability, lipotoxicity and the Metabolic Syndrome—An allostatic perspective. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2010, 1801, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Unger, R.H.; Clark, G.O.; Scherer, P.E.; Orci, L. Lipid homeostasis, lipotoxicity and the metabolic syndrome. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2010, 1801, 209–214. [Google Scholar] [CrossRef]
- Wang, S.; Soni, K.G.; Semache, M.; Casavant, S.; Fortier, M.; Pan, L.; Mitchell, G.A. Lipolysis and the integrated physiology of lipid energy metabolism. Mol. Genet. Metab. 2008, 95, 117–126. [Google Scholar] [CrossRef]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Wadden, T.A.; Webb, V.L.; Moran, C.H.; Bailer, B.A. Lifestyle Modification for Obesity. Circulation 2012, 125, 1157–1170. [Google Scholar] [CrossRef] [Green Version]
- Romijn, J.A.; Coyle, E.F.; Sidossis, L.S.; Gastaldelli, A.; Horowitz, J.F.; Endert, E.; Wolfe, R.R. Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am. J. Physiol. -Endocrinol. Metab. 1993, 265, E380–E391. [Google Scholar] [CrossRef] [Green Version]
- Steele, J.; Plotkin, D.; Van Every, D.; Rosa, A.; Zambrano, H.; Mendelovits, B.; Carrasquillo-Mercado, M.; Grgic, J.; Schoenfeld, B.J. Slow and Steady, or Hard and Fast? A Systematic Review and Meta-Analysis of Studies Comparing Body Composition Changes between Interval Training and Moderate Intensity Continuous Training. Sports 2021, 9, 155. [Google Scholar] [CrossRef]
- Mercola, J.M.; Kirsch, D.L. The Basis for Microcurrent Electrical Therapy in Conventional Medical Practice. J. Adv. Med. 1995, 8, 107–120. [Google Scholar]
- Iijima, H.; Takahashi, M. Microcurrent Therapy as a Therapeutic Modality for Musculoskeletal Pain: A Systematic Review Accelerating the Translation From Clinical Trials to Patient Care. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100145. [Google Scholar] [CrossRef] [PubMed]
- Hamida, Z.H.; Comtois, A.S.; Portmann, M.; Boucher, J.P.; Savard, R. Effect of electrical stimulation on lipolysis of human white adipocytes. Appl. Physiol. Nutr. Metab. 2011, 36, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernández-González, V.; Reverter-Masia, J. Effects of whole-body ELECTROMYOSTIMULATION on health and performance: A systematic review. BMC Complement. Altern. Med. 2019, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Naclerio, F.; Seijo, M.; Karsten, B.; Brooker, G.; Carbone, L.; Thirkell, J.; Larumbe-Zabala, E. Effectiveness of combining microcurrent with resistance training in trained males. Eur. J. Appl. Physiol. 2019, 119, 2641–2653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noites, A.; Pinto, J.; Freitas, C.P.; Melo, C.; Albuquerque, A.; Teixeira, M.; Ribeiro, F.; Bastos, J.M. Effects of microcurrents and physical exercise on the abdominal fat in patients with coronary artery disease. Eur. J. Integr. Med. 2015, 7, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Noites, A.; Nunes, R.; Gouveia, A.I.; Mota, A.; Melo, C.; Viera, Á.; Adubeiro, N.; Bastos, J.M. Effects of aerobic exercise associated with abdominal microcurrent: A preliminary study. J. Altern. Complement. Med. 2015, 21, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Noites, A.; Moreira, A.; Melo, C.; Faria, M.; Vilarinho, R.; Freitas, C.; Monteiro, P.R.R.; Carvalho, P.; Adubeiro, N.; Amorim, M.; et al. Acute effects of physical exercise with microcurrent in the adipose tissue of the abdominal region: A randomized controlled trial. Eur. J. Integr. Med. 2017, 9, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Melo, A.S.C.; Moreira, J.S.; Noites, A.; Couto, M.F.; Argel Melo, C. Clay body wrap with microcurrent: Effects in central adiposity. Appl. Clay Sci. 2013, 80–81, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Duffield, R.; Dawson, B.; Pinnington, H.C.; Wong, P. Accuracy and reliability of a Cosmed K4b2 portable gas analysis system. J. Sci. Med. Sport 2004, 7, 11–22. [Google Scholar] [CrossRef]
- McLaughlin, J.E.; King, G.A.; Howley, E.T.; Bassett, D.R., Jr.; Ainsworth, B.E. Validation of the COSMED K4 b2 Portable Metabolic System. Int. J. Sports. Med. 2001, 22, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Romijn, J.A.; Coyle, E.F.; Hibbert, J.; Wolfe, R.R. Comparison of indirect calorimetry and a new breath 13C/12C ratio method during strenuous exercise. Am. J. Physiol. -Endocrinol. Metab. 1992, 263, E64–E71. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- ACSM. American College of Sports Medicine’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva, 8–11 December 2008; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, C.; Aro, A.; Azevedo, A.; Ramos, E.; Barros, H. Intake and Adipose Tissue Composition of Fatty Acids and Risk of Myocardial Infarction in a Male Portuguese Community Sample. J. Am. Diet. Assoc. 2007, 107, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Péronnet, F.; Massicotte, D. Table of nonprotein respiratory quotient: An update. Can. J. Sport Sci. 1991, 16, 23–29. [Google Scholar]
- Brooks, G.A. Amino acid and protein metabolism during exercise and recovery. Med. Sci. Sports Exerc. 1987, 19, S150–S156. [Google Scholar] [CrossRef]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Jeukendrup, A.E. Modulation of carbohydrate and fat utilization by diet, exercise and environment. Biochem. Soc. Trans. 2003, 31, 1270–1273. [Google Scholar] [CrossRef] [Green Version]
- Ramirez-Ponce, M.; Acosta, J.; Bellido, J.; Mateos, J. Noradrenaline modulates the electrical activity of white adipocytes by a cAMP-dependent mechanism. J. Endocrinol. 1998, 159, 397–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramírez-Ponce, M.P.; Mateos, J.C.; Bellido, J.A. Human Adipose Cells Have Voltage-dependent Potassium Currents. J. Membr. Biol. 2003, 196, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Achten, J.; Gleeson, M.; Jeukendrup, A.E. Determination of the exercise intensity that elicits maximal fat oxidation. Med. Sci. Sports Exerc. 2002, 34, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Blaak, E.E.; Saris, W.H.M. Substrate oxidation, obesity and exercise training. Best Pract. Res. Clin. Endocrinol. Metab. 2002, 16, 667–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frayn, K.N. Fat as a fuel: Emerging understanding of the adipose tissue–skeletal muscle axis. Acta Physiol. 2010, 199, 509–518. [Google Scholar] [CrossRef]
- Melzer, K. Carbohydrate and fat utilization during rest and physical activity. E-SPEN Eur. e-J. Clin. Nutr. Metab. 2011, 6, e45–e52. [Google Scholar] [CrossRef] [Green Version]
- Blaak, E. Gender differences in fat metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Bülow, J.; Gjeraa, K.; Enevoldsen, L.H.; Simonsen, L. Lipid mobilization from human abdominal, subcutaneous adipose tissue is independent of sex during steady-state exercise. Clin. Physiol. Funct. Imaging 2006, 26, 205–211. [Google Scholar] [CrossRef]
- Carter, S.L.; Rennie, C.; Tarnopolsky, M.A. Substrate utilization during endurance exercise in men and women after endurance training. Am. J. Physiol. -Endocrinol. Metab. 2001, 280, E898–E907. [Google Scholar] [CrossRef] [Green Version]
- Henderson, G.C.; Krauss, R.M.; Fattor, J.A.; Faghihnia, N.; Luke-Zeitoun, M.; Brooks, G.A. Plasma triglyceride concentrations are rapidly reduced following individual bouts of endurance exercise in women. Eur. J. Appl. Physiol. 2010, 109, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Power, M.L.; Schulkin, J. Sex differences in fat storage, fat metabolism, and the health risks from obesity: Possible evolutionary origins. Br. J. Nutr. 2008, 99, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.E.; Febbraio, M.A. Effects of ovarian hormones on exercise metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Casazza, G.A.; Jacobs, K.A.; Suh, S.-H.; Miller, B.F.; Horning, M.A.; Brooks, G.A. Menstrual cycle phase and oral contraceptive effects on triglyceride mobilization during exercise. J. Appl. Physiol. 2004, 97, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedlander, A.L.; Casazza, G.A.; Horning, M.A.; Huie, M.J.; Piacentini, M.F.; Trimmer, J.K.; Brooks, G.A. Training-induced alterations of carbohydrate metabolism in women: Women respond differently from men. J. Appl. Physiol. 1998, 85, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Tarnopolsky, M.A. Sex Differences in Exercise Metabolism and the Role of 17-Beta Estradiol. Med. Sci. Sports Exerc. 2008, 40, 648–654. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Participants (n = 38) | Intervention Group (n = 18) | Placebo Group (n = 20) | p Value between Groups |
|---|---|---|---|---|
| Age (years) | 20.6, ± 1.8 | 20.7 ± 1.8 | 20.6 ± 1.9 | 0.845 |
| Height (m) | 1.7 ± 0.1 | 1.7 ± 0.1 | 1.7 ± 0.1 | 0.830 |
| Body mass (kg) | 66.8 ± 10.9 | 66.9 ± 6.3 | 66.8 ± 11.7 | 0.430 |
| BMI (kg/m2) | 23.1 ± 2.8 | 24.0 ± 2.8 | 22.3 ± 2.6 | 0.060 |
| %TBF | 19.9 ± 8.8 | 22.4 ± 7.6 | 16.6 ± 4.3 | 0.108 |
| WC (cm) | 79.6 ± 8.1 | 80.0 ± 4.9 | 77.5 ± 5.8 | 0.156 |
| WHtR | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.4 ± 0.1 | 0.060 |
| IPAQ-SF (MET/min/week) | 3447.0 [1989; 3958] | 3425.0 [1612; 4196] | 3453.0 [2272; 3447] | 0.613 |
| Calories 1 | 2348.1 ± 669.4 | 2242.4 ± 745.4 | 2443.3 ± 596.2 | 0.363 |
| % Protein 1 | 22.4 ± 3.4 | 22.0 ± 2.4 | 22.5 ± 2.8 | 0.826 |
| % CHO 1 | 60.0 ± 5.7 | 61.0 ± 4.3 | 60.9 ± 4.4 | 0.693 |
| % Total fat 1 | 17.6 ± 3.6 | 17.0 ± 2.5 | 16.6 ± 1.7 | 0.589 |
| Characteristics | Intervention Group (n = 18) | Placebo Group (n = 20) | p Value between Groups | |||
|---|---|---|---|---|---|---|
| Females (n = 9) | Males (n = 9) | Females (n = 11) | Males (n = 9) | Females | Males | |
| Age (years) | 20.3 ± 2.3 | 21.0 ± 1.0 | 20.2 ± 1.6 | 21.0 ± 2.2 | 0.846 | 1.000 |
| Height (m) | 1.63 ± 0.1 | 1.75 ± 0.1 | 1.62 ± 0.1 | 1.80 ± 0.0 | 0.598 | 0.480 |
| Body mass (kg) | 62.2 ± 3.3 | 68.7 ± 8.5 | 53.7 ±8.3 | 72.8 ± 6.5 | 0.149 | 0.965 |
| BMI (kg/m2) | 24.1 ± 1.9 | 22.9 ± 1.6 | 20.9 ± 2.6 | 22.0 ± 1.5 | 0.090 | 0.310 |
| %TBF | 29.3 ± 4.0 | 14.3 ± 3.1 | 19.7 ± 5.8 | 11.8 ± 3.8 | 0.053 | 0.038 * |
| WC (cm) | 80.0 ± 5.2 | 83.4 ± 9.7 | 75.2 ± 9.4 | 80.8 ± 5.0 | 0.176 | 0.480 |
| WHtR | 0.49 ± 0.0 | 0.48 ± 0.1 | 0.46 ± 0.0 | 0.45 ± 0.0 | 0.140 | 0.233 |
| IPAQ -SF (MET/min/week) | 3447.0 [647.0; 4173.0] | 3420.0 [2536.0; 5424.0] | 2772.0 [1035.0; 3324.0] | 3447.0 [3447.0; 3963.0] | 0.766 | 0.863 |
| Calories 1 | 2261.7 ± 298.1 | 1851.7 ± 773.4 | 2348.1 ± 752.5 | 2330.1 ± 320.5 | 0.569 | 0.270 |
| % Protein 1 | 20.8 ± 2.5 | 21.3 ± 2.3 | 22.4 ± 1.9 | 20.6 ± 2.7 | 0.849 | 0.507 |
| % CHO 1 | 61.0 ± 4.1 | 61.0 ± 6.3 | 60.4 ± 4.7 | 62.8 ± 4.8 | 0.909 | 0.627 |
| % Total fat 1 | 18.2 ± 2.8 | 17.7 ± 2.7 | 17.2 ± 2.1 | 16.6 ± 1.4 | 0.470 | 0.627 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vilarinho, R.; Faria, S.M.; Monteiro, P.R.R.; Melo, C.; Santos, R.; Noites, A. Effects of Abdominal Microcurrent in the Consumption and Proportion of Energy Substrates during Aerobic Exercise: A Pilot Study. Healthcare 2022, 10, 917. https://doi.org/10.3390/healthcare10050917
Vilarinho R, Faria SM, Monteiro PRR, Melo C, Santos R, Noites A. Effects of Abdominal Microcurrent in the Consumption and Proportion of Energy Substrates during Aerobic Exercise: A Pilot Study. Healthcare. 2022; 10(5):917. https://doi.org/10.3390/healthcare10050917
Chicago/Turabian StyleVilarinho, Rui, Susana Miriam Faria, Pedro Ribeiro Rocha Monteiro, Cristina Melo, Rubim Santos, and Andreia Noites. 2022. "Effects of Abdominal Microcurrent in the Consumption and Proportion of Energy Substrates during Aerobic Exercise: A Pilot Study" Healthcare 10, no. 5: 917. https://doi.org/10.3390/healthcare10050917