
Depression and Cognitive Impairment in a Spanish Sample of Psychoactive Substance Users Receiving Mental Health Care


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Analytical Procedure
3. Results
3.1. Relationship between Sociodemographic Variables with Other Study Variables: Type of Substance, Depression Level and Cognitive Impairment
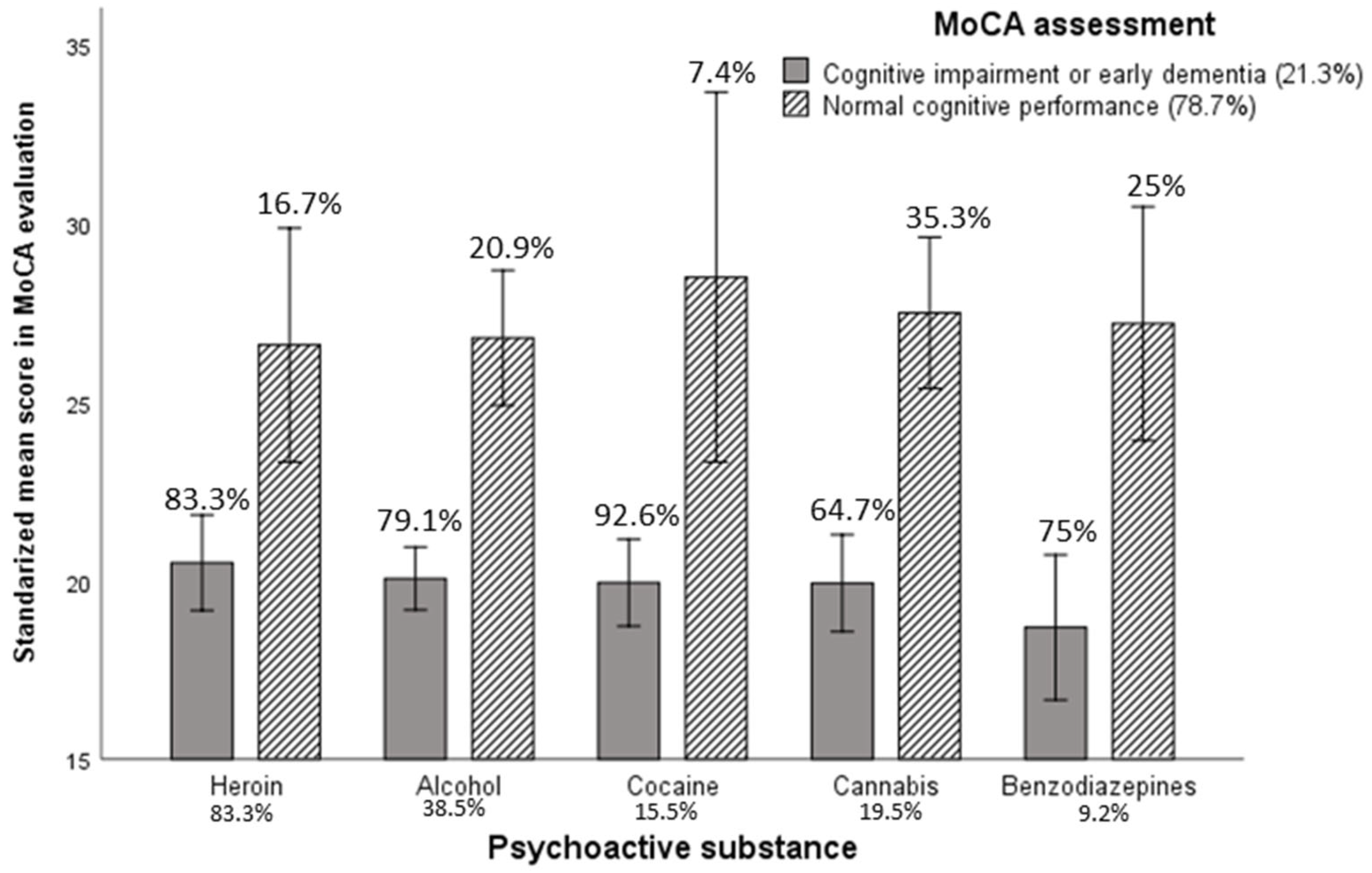
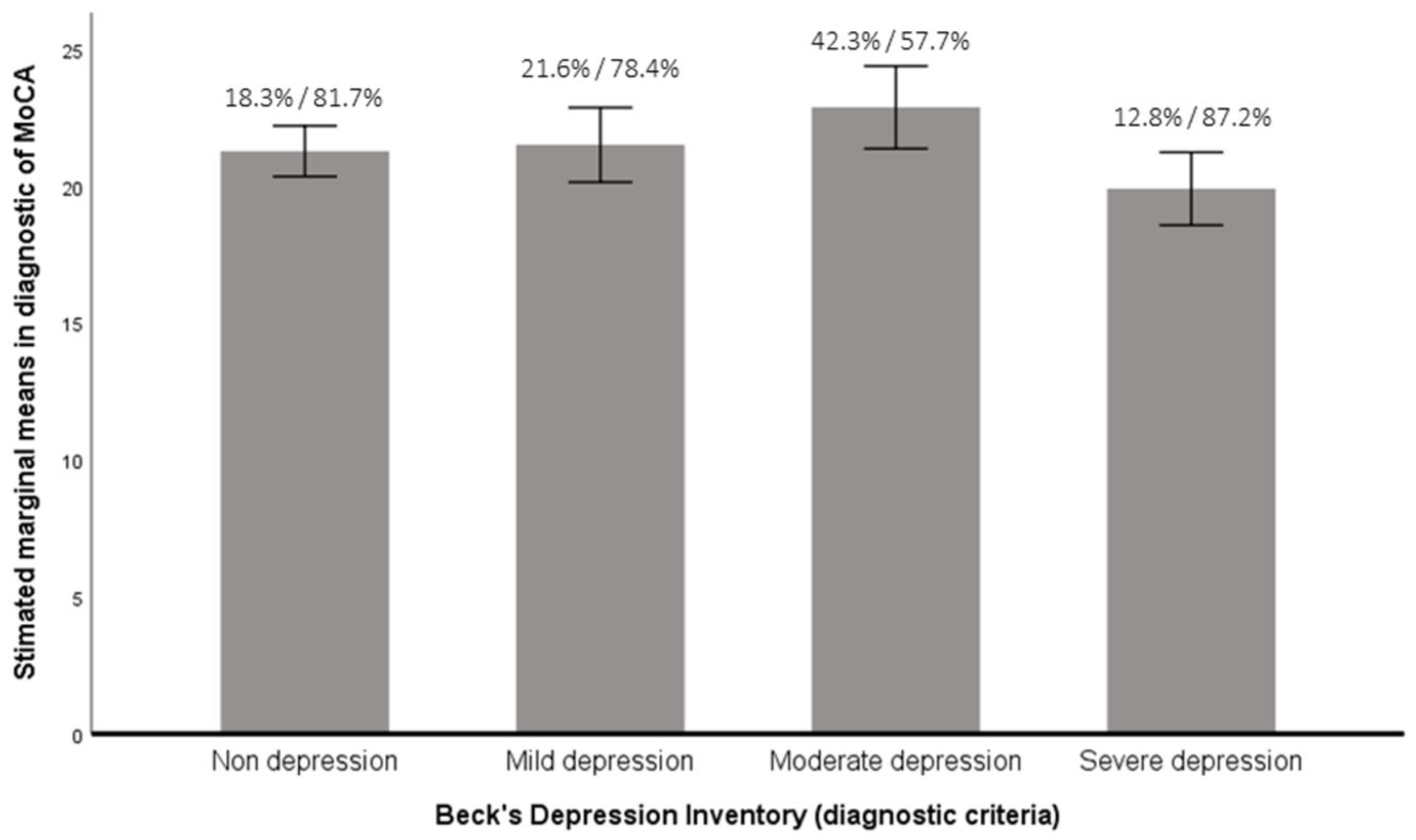
3.2. Differences between Types of Substance and Depression Level or Cognitive Impairment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badiani, A.; Berridge, K.C.; Heilig, M.; Nutt, D.J.; Robinson, T.E. Addiction research and theory: A commentary on the Surgeon General’s Report on alcohol, drugs, and health. Addict. Biol. 2018, 23, 3–5. [Google Scholar] [CrossRef]
- European Monitoring Center for Drugs and Drug Addiction. European Drug Report: Trends and Developments; EMCCDA: Lisbon, Portugal, 2016; Available online: http://www.emcdda.europa.eu/edr2016 (accessed on 15 January 2021).
- Observatorio Español de la Droga y las Toxicomanías. Informe 2016, Alcohol, Tabaco y Drogas Ilegales en España, 2016 [Report 2016, alcohol, tobacco and illegal drugs in Spain, 2016]. Available online: https://pnsd.sanidad.gob.es/gl/profesionales/sistemasInformacion/informesEstadisticas/pdf/2016_INFORME_OEDT.pdf (accessed on 15 January 2022).
- Fernández-Serrano, M.J.; Pérez-García, M.; Verdejo-García, A. What are the specific vs. generalized effects of drugs of abuse on neuropsychological performance? Neurosci. Biobehav. Rev. 2011, 35, 377–406. [Google Scholar] [CrossRef] [PubMed]
- Coullaut-Valera, R.; Arbaiza-Díaz, I.; Arrúe-Ruibloda, R.; Coullaut-Valera, J.; Bajo-Bretón, R. Deterioro cognitivo asociado al consumo de diferentes sustancias psicoactivas. Actas Españolas Psiquiatr. 2011, 39, 168–173. [Google Scholar]
- Torrens, M.; Martínez-Sanvisens, D. Patología Dual: Protocolos de Intervención. Depresión [Dual Pathology: Intervention Protocols. Depression]; Edikamed: Barcelona, Spain, 2009. [Google Scholar]
- Copersino, M.L.; Fals-Stewart, W.; Fitzmaurice, G.; Schretlen, D.J.; Sokoloff, J.; Weiss, R.D. Rapid cognitive screening of patients with substance use disorders. Exp. Clin. Psychopharmacol. 2009, 17, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruijnen, C.J.; Dijkstra, B.A.; Walvoort, S.J.; Markus, W.; VanDerNagel, J.E.; Kessels, R.P.; DE Jong, C.A. Prevalence of cognitive impairment in patients with substance use disorder. Drug Alcohol Rev. 2019, 38, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Damian, A.M.; Jacobson, S.A.; Hentz, J.G.; Belden, C.M.; Shill, H.A.; Sabbagh, M.N.; Caviness, J.N.; Adler, C.H. The Montreal Cognitive Assessment and the Mini-Mental State Examination as screening instruments for cognitive impairment: Item analyses and threshold scores. Dement. Geriatr. Cogn. Disord. 2011, 31, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Rojo-Mota, G.; Pedrero-Pérez, E.J.; Ruiz-Sánchez de León, J.M.; Llanero-Luque, M.; Puerta-García, C. Cribado neurocognitivo en adictos a sustancias: La evaluación cognitiva de Montreal. Rev. Neurol. 2013, 56, 129–136. [Google Scholar] [CrossRef]
- Pelletier, S.; Nalpas, B.; Alarcon, R.; Rigole, H.; Perney, P. Investigation of Cognitive Improvement in Alcohol-Dependent Inpatients Using the Montreal Cognitive Assessment (MoCA) Score. J. Addict. 2016, 2016, 1539096. [Google Scholar] [CrossRef] [Green Version]
- McKetin, R.; Parasu, P.; Cherbuin, N.; Eramudugolla, R.; Anstey, K.J. A longitudinal examination of the relationship between cannabis use and cognitive function in mid-life adults. Drug Alcohol Depend. 2016, 169, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Stasiewicz, P.R.; Bradizza, C.M.; Slosman, K.S. Emotion Regulation Treatment of Alcohol Use Disorders: Helping Clients Manage Negative Thoughts and Feelings; Routledge: London, UK, 2018. [Google Scholar]
- Ávila, J.D.; Escobar, F.; Úrzola, C.; Luz, H. Prevalence of anxiety and depression in bed alcoholics for deintoxication in Bogota. Rev. Fac. Med. 2005, 53, 219–225. [Google Scholar]
- Dos Santos Rigoni, M.; Quarti Irigaray, T.; Duarte de Moraes, J.F.; Ferrão, Y.; da Silva Oliveira, M. Neuropsychological performance and demographic characteristics in alcoholic patients in treatment. Adicciones 2014, 26, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Alves, H.; Kessler, F.; Ratto, L.R.C. Comorbidade: Uso de álcool e outros transtornos psiquiátricos. Rev. Bras. Psiquiatr. 2004, 26, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Brower, K.J. Insomnia, alcoholism and relapse. Sleep Med. Rev. 2003, 7, 523–539. [Google Scholar] [CrossRef]
- Pulcheiro, G.; Bicca, C. Avaliação dos Transtornos Comórbidos. In Alcohol, Outras Drogas, Informações: O que Cada Professional Precisa Saber; Pulcherio, G., Bicca, C., Silva, F.A., Eds.; Casa do Psicólogo: São Paulo, Brazil, 2002; pp. 79–90. [Google Scholar]
- Danielsson, A.K.; Lundin, A.; Agardh, E.; Allebeck, P.; Forsell, Y. Cannabis use, depression and anxiety: A 3-year prospective population-based study. J. Affect. Disord. 2016, 193, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.M.X.; Cleary, M.; Sitharthan, T.; Hunt, G.E. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990–2014: A systematic review and meta-analysis. Drug Alcohol Depend. 2015, 154, 1–13. [Google Scholar] [CrossRef]
- Pacek, L.R.; Martins, S.S.; Crum, R.M. The bidirectional relationships between alcohol, cannabis, co-occurring alcohol and cannabis use disorders with major depressive disorder: Results from a national sample. J. Affect. Disord. 2013, 148, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Vorspan, F.; Mehtelli, W.; Dupuy, G.; Bloch, V.; Lépine, J.P. Anxiety and substance use disorders: Co-occurrence and clinical issues. Current Psychiatry Reports 2015, 17, 4. [Google Scholar] [CrossRef]
- Horwood, L.J.; Fergusson, D.M.; Coffey, C.; Patton, G.C.; Tait, R.; Smart, D.; Letcher, P.; Silins, E.; Hutchinson, D.M. Cannabis and depression: An integrative data analysis of four Australasian cohorts. Drug Alcohol Depend. 2012, 126, 369–378. [Google Scholar] [CrossRef]
- Regier, D.A.; Farmer, M.E.; Rae, D.S.; Locke, B.Z.; Keith, S.J.; Judd, L.L.; Goodwin, F.K. Comorbidity of mental disorders with alcohol and other drug abuse: Results from the Epidemiologic Catchment Area (ECA) study. Jama 1990, 264, 2511–2518. [Google Scholar] [CrossRef]
- Obra Social Fundación “La Caixa” Programa de Prevención del Consumo de Drogas [Drug Abuse Prevention Program]. 2010. Available online: https://educaixa.org/es/-/las-drogas-aqui-y-ahora (accessed on 10 March 2022).
- Instituto de la Mujer. III Macroencuesta Sobre Violencia Contra las Mujeres. 2006. Available online: http://www.inmujer.gob.es/ (accessed on 25 March 2021).
- Ministerio de Sanidad y Consumo. Encuesta Sobre Salud y Consumo de Drogas a Los Internados en Instituciones Penitenciarias (ESDIP). 2006. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/encuestaPenitenciaria2006.pdf (accessed on 23 June 2021).
- Lozano, M.; Hernández-Ferrándiz, M.; Turró-Garriga, O.T.; Pericot, I.; López-Pousa, S.; Vilalta, J. Validación del Montreal Cognitive Assessment (MoCA): Test de Cribado para el Deterioro Cognitivo Leve. Datos Preliminares. Alzheimer Real. Investig. Demenc. 2009, 43, 4–11. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. BDI-II. Beck Depression Inventory: Manual, 2nd ed.; Harcourt Brace: Boston, MA, USA, 1996. [Google Scholar]
- Sanz, J.; Perdigón, A.L.; Vázquez, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general. Clínica Salud 2003, 14, 249–280. [Google Scholar]
- García-Marchena, N.; Araos, P.; Pavón, F.J.; Ponce, G.; Pedraz, M.; Serrano, A.; Arias, F.; Romero-Sanchiz, P.; Suárez, J.; Pastor, A.; et al. Psychiatric comorbidity and plasma levels of 2-acyl-glycerols in outpatient treatment alcohol users. Analysis of gender differences. Adicciones 2017, 29, 86–93. [Google Scholar]
- Rodríguez-Sáez, J.L.; Martín-Antón, L.J.; Salgado-Ruiz, A.; Carbonero, M.Á. Socio-Emotional Variables Linked to the Consumption of Drugs amongst University Students of Social Sciences: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 4502. [Google Scholar] [CrossRef] [PubMed]
- Bourque, J.; Potvin, S. Cannabis and cognitive functioning: From acute to residual effects, from randomized controlled trials to prospective designs. Front. Psychiatry 2021, 12, 919. [Google Scholar] [CrossRef]
- Wendel, L.K.; Daedelow, L.; Kaminski, J.; Banaschewski, T.; Millenet, S.; Bokde, A.L.; Walter, H. Residual effects of cannabis-use on neuropsychological functioning. Cogn. Dev. 2021, 59, 101072. [Google Scholar] [CrossRef]
- Choi, N.G.; DiNitto, D.M.; Marti, C.N.; Choi, B.Y. Cannabis and binge alcohol use among older individuals with major depressive episode. Subst. Abus. 2022, 43, 657–665. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BDI Score | Type of Depression | ||||
|---|---|---|---|---|---|
| Substance | Mean (SD) | No Depression | Mild Depression | Moderate Depression | Severe Depression |
| Heroin | 17.76 (2.25) | 33.3 | 24.2 | 24.2 | 18.2 |
| Alcohol | 18.02 (1.24) | 33.0 | 23.9 | 12.8 | 30.3 |
| Cocaine | 16.80 (2.07) | 38.5 | 25.6 | 7.7 | 28.2 |
| Cannabis | 15.39 (1.81) | 43.1 | 21.6 | 15.7 | 19.6 |
| Benzodiazepines | 20.57 (2.82) | 28.6 | 19.0 | 19.0 | 33.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luque, B.; García, V.; Tabernero, C. Depression and Cognitive Impairment in a Spanish Sample of Psychoactive Substance Users Receiving Mental Health Care. Healthcare 2022, 10, 887. https://doi.org/10.3390/healthcare10050887
Luque B, García V, Tabernero C. Depression and Cognitive Impairment in a Spanish Sample of Psychoactive Substance Users Receiving Mental Health Care. Healthcare. 2022; 10(5):887. https://doi.org/10.3390/healthcare10050887
Chicago/Turabian StyleLuque, Bárbara, Victoriana García, and Carmen Tabernero. 2022. "Depression and Cognitive Impairment in a Spanish Sample of Psychoactive Substance Users Receiving Mental Health Care" Healthcare 10, no. 5: 887. https://doi.org/10.3390/healthcare10050887