
Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Focused Question
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Research
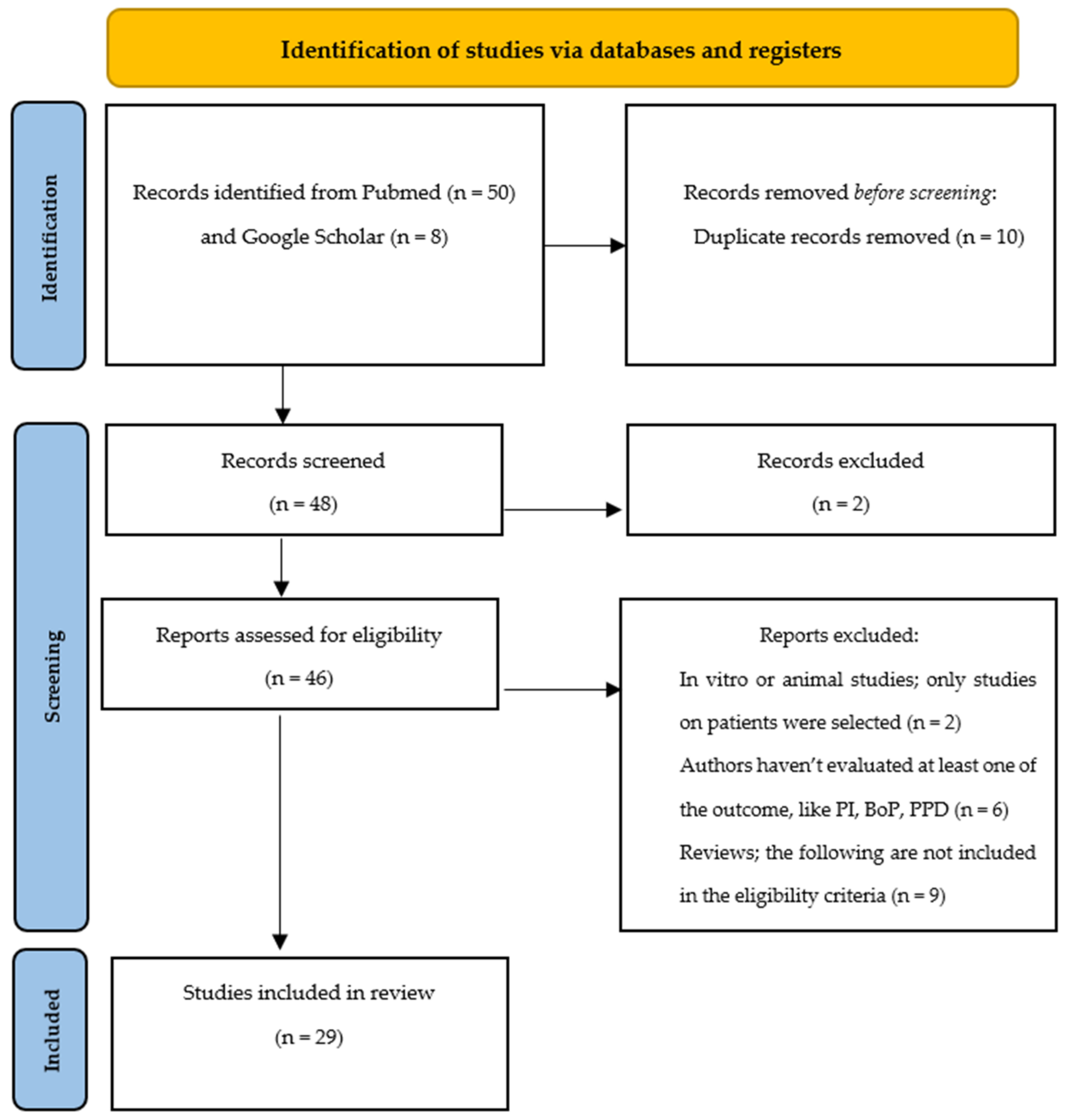
2.5. Search Outcome and Evaluation
3. Results
3.1. Laser
3.2. Ozone
3.3. Glycine/Erythritol
3.4. Probiotics
3.5. Chlorhexidine
3.6. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Meyle, J.; Group D of the European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravidà, A.; Galli, M.; Siqueira, R.; Saleh, M.H.A.; Galindo-Moreno, P.; Wang, H.L. Diagnosis of peri-implant status after peri-implantitis surgical treatment: Proposal of a new classification. J. Periodontol. 2020, 91, 1553–1561. [Google Scholar] [CrossRef]
- Kormas, I.; Pedercini, C.; Pedercini, A.; Raptopoulos, M.; Alassy, H.; Wolff, L.F. Peri-Implant Diseases: Diagnosis, Clinical, Histological, Microbiological Characteristics and Treatment Strategies. A Narrative Review. Antibiotics 2020, 9, 835. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Aghazadeh, A.; Hallström, H.; Persson, G.R. Factors related to peri-implantitis—A retrospective study. Clin. Oral Implant. Res. 2014, 25, 522–529. [Google Scholar] [CrossRef]
- Clementini, M.; Rossetti, P.H.; Penarrocha, D.; Micarelli, C.; Bonachela, W.C.; Canullo, L. Systemic risk factors for peri-implant bone loss: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2014, 43, 323–334. [Google Scholar] [CrossRef]
- Vervaeke, S.; Collaert, B.; Cosyn, J.; Deschepper, E.; de Bruyn, H. A multifactorial analysis to identify predictors of implant failure and peri-implant bone loss. Clin. Implant. Dent. Relat. Res. 2015, 17, e298–e307. [Google Scholar] [CrossRef]
- Schwarz, F.; Ramanauskaite, A. It is all about peri-implant issue health. Periodontology 2022, 88, 9–12. [Google Scholar] [CrossRef]
- Song, X.; Li, L.; Gou, H.; Xu, Y. Impact of implant location on the prevalence of peri-implantitis: A systematic review and meta- analysis. J. Dent. 2020, 103, 103490. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Mariani, G.M.; Ferrarotti, F.; Ercoli, E.; Liu, C.C.; Romano, F. Adjunctive efficacy of diode laser in the treatment of peri-implant mucositis with mechanical therapy: A randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 429–438. [Google Scholar] [CrossRef] [PubMed]
- McKenna, D.F.; Borzabadi-Farahani, A.; Lynch, E. The effect of subgingival ozone and/or hydrogen peroxide on the development of peri-implant mucositis: A double-blind randomized controlled trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 1483–1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hentenaar, D.F.M.; De Waal, Y.C.M.; Stewart, R.E.; Van Winkelhoff, A.J.; Meijer, H.J.A.; Raghoebar, G.M. Erythritol airpolishing in the non-surgical treatment of peri-implantitis: A randomized controlled trial. Clin. Oral Implant. Res. 2021, 32, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Hallström, H.; Lindgren, S.; Widén, C.; Renvert, S.; Twetman, S. Probiotic supplements and debridement of peri-implant mucositis: A randomized controlled trial. Acta Odontol. Scand. 2016, 74, 60–66. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Salvi, G.E.; Botticelli, D.; Mombelli, A.; Faddy, M.; Lang, N.P.; Implant Complication Research Group. Anti-infective treatment of peri-implant mucositis: A randomised controlled clinical trial. Clin. Oral Implant. Res. 2011, 22, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Matys, J.; Romeo, U.; Mroczka, K.; Grzech-Leśniak, K.; Dominiak, M. Temperature Changes and SEM Effects of Three Different Implants-Abutment Connection during Debridement with Er: YAG Laser: An Ex Vivo Study. Materials 2019, 12, 3748. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Dukka, H.; Saleh, M.H.A.; Ravidà, A.; Greenwell, H.; Wang, H.L. Is bleeding on probing a reliable clinical indicator of peri-implant diseases? J. Periodontol. 2021, 92, 1669–1674. [Google Scholar] [CrossRef]
- Gerber, J.A.; Tan, W.C.; Balmer, T.E.; Salvi, G.E.; Lang, N.P. Bleeding on probing and pocket probing depth in relation to probing pressure and mucosal health around oral implants. Clin. Oral Implant. Res. 2009, 20, 75–78. [Google Scholar] [CrossRef]
- Bassetti, M.; Schär, D.; Wicki, B.; Eick, S.; Ramseier, C.A.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sculean, A.; Rothamel, D.; Schwenzer, K.; Georg, T.; Becker, J. Clinical evaluation of an Er: YAG laser for nonsurgical treatment of peri-implantitis: A pilot study. Clin. Oral Implant. Res. 2005, 16, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Schär, D.; Ramseier, C.A.; Eick, S.; Arweiler, N.B.; Sculean, A.; Salvi, G.E. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: Six-month outcomes of a prospective randomized clinical trial. Clin. Oral Implant. Res. 2013, 24, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; John, G.; Hegewald, A.; Becker, J. Non-surgical treatment of peri-implant mucositis and peri-implantitis at zirconia implants: A prospective case series. J. Clin. Periodontol. 2015, 42, 783–788. [Google Scholar] [CrossRef]
- Persson, G.R.; Roos-Jansåker, A.M.; Lindahl, C.; Renvert, S. Microbiologic results after non-surgical erbium-doped:yttrium, aluminum, and garnet laser or air-abrasive treatment of peri-implantitis: A randomized clinical trial. J. Periodontol. 2011, 82, 1267–1278. [Google Scholar] [CrossRef]
- Mariani, G.M.; Ercoli, E.; Guzzi, N.; Bongiovanni, L.; Bianco, L.; Romano, F.; Aimetti, M. One-year clinical outcomes following non-surgical treatment of peri-implant mucositis with adjunctive diode laser application. Minerva Stomatol. 2020, 69, 269–277. [Google Scholar] [CrossRef]
- Arısan, V.; Karabuda, Z.C.; Arıcı, S.V.; Topçuoğlu, N.; Külekçi, G. A randomized clinical trial of an adjunct diode laser application for the nonsurgical treatment of peri-implantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Bieling, K.; Bonsmann, M.; Latz, T.; Becker, J. Nonsurgical treatment of moderate and advanced periimplantitis lesions: A controlled clinical study. Clin. Oral Investig. 2006, 10, 279–288. [Google Scholar] [CrossRef]
- Tenore, G.; Montori, A.; Mohsen, A.; Mattarelli, G.; Palaia, G.; Romeo, U. Evaluation of adjunctive efficacy of diode laser in the treatment of peri-implant mucositis: A randomized clinical trial. Lasers Med. Sci. 2020, 35, 1411–1417. [Google Scholar] [CrossRef]
- Wang, H.; Li, W.; Zhang, D.; Li, W.; Wang, Z. Adjunctive photodynamic therapy improves the outcomes of peri-implantitis: A randomized controlled trial. Aust. Dent. J. 2019, 64, 256–262. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Roos Jansåker, A.M.; Persson, G.R. Treatment of peri-implantitis using an Er: YAG laser or an air-abrasive device: A randomized clinical trial. J. Clin. Periodontol. 2011, 38, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Martos, R.; Samman, A.; Bouazza-Juanes, K.; Díaz-Fernández, J.M.; Arias-Herrera, S. Clinical effect of diode laser on peri-implant tissues during non-surgical peri-implant mucositis therapy: Randomized controlled clinical study. J. Clin. Exp. Dent. 2020, 12, e13–e21. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Riben-Grundstrom, C.; Norderyd, O.; André, U.; Renvert, S. Treatment of peri-implant mucositis using a glycine powder air-polishing or ultrasonic device: A randomized clinical trial. J. Clin. Periodontol. 2015, 42, 462–469. [Google Scholar] [CrossRef]
- Ji, Y.J.; Tang, Z.H.; Wang, R.; Cao, J.; Cao, C.F.; Jin, L.J. Effect of glycine powder air-polishing as an adjunct in the treatment of peri-implant mucositis: A pilot clinical trial. Clin. Oral Implant. Res. 2014, 25, 683–689. [Google Scholar] [CrossRef]
- Sahm, N.; Becker, J.; Santel, T.; Schwarz, F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: A prospective, randomized, controlled clinical study. J. Clin. Periodontol. 2011, 38, 872–878. [Google Scholar] [CrossRef]
- Laleman, I.; Pauwels, M.; Quirynen, M.; Teughels, W. The usage of a lactobacilli probiotic in the non-surgical therapy of peri-implantitis: A randomized pilot study. Clin. Oral Implant. Res. 2020, 31, 84–92. [Google Scholar] [CrossRef]
- Tada, H.; Masaki, C.; Tsuka, S.; Mukaibo, T.; Kondo, Y.; Hosokawa, R. The effects of Lactobacillus reuteri probiotics combined with azithromycin on peri-implantitis: A randomized placebo-controlled study. J. Prosthodont. Res. 2018, 62, 89–96. [Google Scholar] [CrossRef]
- Mongardini, C.; Pilloni, A.; Farina, R.; Di Tanna, G.; Zeza, B. Adjunctive efficacy of probiotics in the treatment of experimental peri-implant mucositis with mechanical and photodynamic therapy: A randomized, cross-over clinical trial. J. Clin. Periodontol. 2017, 44, 410–417. [Google Scholar] [CrossRef]
- Galofré, M.; Palao, D.; Vicario, M.; Nart, J.; Violant, D. Clinical and microbiological evaluation of the effect of Lactobacillus reuteri in the treatment of mucositis and peri-implantitis: A triple-blind randomized clinical trial. J. Periodontal. Res. 2018, 53, 378–390. [Google Scholar] [CrossRef]
- Peña, M.; Barallat, L.; Vilarrasa, J.; Vicario, M.; Violant, D.; Nart, J. Evaluation of the effect of probiotics in the treatment of peri-implant mucositis: A triple-blind randomized clinical trial. Clin. Oral Investig. 2019, 23, 1673–1683. [Google Scholar] [CrossRef]
- Menezes, K.M.; Fernandes-Costa, A.N.; Silva-Neto, R.D.; Calderon, P.S.; Gurgel, B.C. Efficacy of 0.12% Chlorhexidine Gluconate for Non-Surgical Treatment of Peri-Implant Mucositis. J. Periodontol. 2016, 87, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Pulcini, A.; Bollaín, J.; Sanz-Sánchez, I.; Figuero, E.; Alonso, B.; Sanz, M.; Herrera, D. Clinical effects of the adjunctive use of a 0.03% chlorhexidine and 0.05% cetylpyridinium chloride mouth rinse in the management of peri-implant diseases: A randomized clinical trial. J. Clin. Periodontol. 2019, 46, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Hallström, H.; Lindgren, S.; Twetman, S. Effect of a chlorhexidine-containing brush-on gel on peri-implant mucositis. Int. J. Dent. Hyg. 2017, 15, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Hirooka, H.; Polyzois, I.; Kelekis-Cholakis, A.; Wang, H.L.; Working Group 3. Diagnosis and non-surgical treatment of peri-implant diseases and maintenance care of patients with dental implants—Consensus report of working group 3. Int. Dent. J. 2019, 69, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teughels, W.; Feres, M.; Oud, V.; Martín, C.; Matesanz, P.; Herrera, D. Adjunctive effect of systemic antimicrobials in periodontitis therapy: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 257–281. [Google Scholar] [CrossRef]
- Kensy, J.; Dobrzyński, M.; Wiench, R.; Grzech-Leśniak, K.; Matys, J. Fibroblasts Adhesion to Laser-Modified Titanium Surfaces—A Systematic Review. Materials 2021, 14, 7305. [Google Scholar] [CrossRef]
- Nart, J.; Pons, R.; Valles, C.; Esmatges, A.; Sanz-Martín, I.; Monje, A. Non-surgical therapeutic outcomes of peri-implantitis: 12-month results. Clin. Oral Investig. 2020, 24, 675–682. [Google Scholar] [CrossRef]
- Mettraux, G.R.; Sculean, A.; Burgin, W.B.; Salvi, G.E. Two-year clinical outcomes following non-surgical mechanical therapy of peri-implantitis with adjunctive diode laser application. Clin. Oral Implant. Res. 2016, 27, 845–849. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Natoli, V.; Bruni, A.; Coscione, C.; Magliano, G.; Giacobbo, G.; Morelli, A.; Moressa, S.; Scribante, A. Bio-Inspired Systems in Nonsurgical Periodontal Therapy to Reduce Contaminated Aerosol during COVID-19: A Comprehensive and Bibliometric Review. J. Clin. Med. 2020, 9, 3914. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non-Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Appl. Sci. 2021, 11, 8586. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Cuggia, G.; Scribante, A. Domiciliary Use of Chlorhexidine vs. Postbiotic Gels in Patients with Peri-Implant Mucositis: A Split-Mouth Randomized Clinical Trial. Appl. Sci. 2022, 12, 2800. [Google Scholar] [CrossRef]
- Pałka, Ł.; Nowakowska-Toporowska, A.; Dalewski, B. Is Chlorhexidine in Dentistry an Ally or a Foe? A Narrative Review. Healthcare 2022, 10, 764. [Google Scholar] [CrossRef]


{kind=link}
| Article | Follow-Up | Problem | Intervention | Control | Outcomes |
|---|---|---|---|---|---|
| Aimetti et al., 2019 [12] | 3 months | Mucositis | Debridement using curettes and ultrasonic devices + diode laser (980 nm, 2.5 W, 10 kHz, 30 s) | Debridement using curettes and ultrasonic devices | Laser was more effective in reducing clinical signs of inflammation |
| Bassetti et al., 2013 [21] | 12 months | Peri-implantitis | Debridement using titanium curettes and glycine air-polishing + PDT (660 nm, 100 mW) | Debridement using titanium curettes and glycine air-polishing + minocycline microspheres | PDT was effective in the reduction of mucosal inflammation from baseline to 6 months and a decrease in PPD from baseline to 9 months |
| Schwarz et al., 2005 [22] | 6 months | Peri-implantitis | Debridement using Er:YAG laser (2.94 mm, 100 mJ/pulse (12.7 J/cm2)) | Debridement using plastic curettes + chlorhexidine | BOP decreased in the ERL group from 83% at baseline to 31% after 6 months (p < 0.001): the difference between the two groups was statistically significant (p < 0.001) |
| Schär et al., 2012 [23] | 6 months | Peri-implantitis | Debridement using titanium curettes and glycine air-polishing + PDT (660 nm, 100 mW) | Debridement using titanium curettes and glycine air-polishing + minocycline microspheres | Between-group comparisons revealed no statistically significant differences (p > 0.05) |
| Schwarz et al., 2015 [24] | 6 months | Mucositis and peri-implantitis | Debridement using carbon curettes + Er:YAG laser (2.94 μm, 100 mJ/pulse (12.7 J/cm2), 10 Hz) (peri-implantitis) | Debridement using carbon curettes + pockets irrigation using 0.1% chlorhexidine solution (mucositis) | Non-surgical treatment of either peri-implant mucositis using MD + CHX or peri-implantitis using ERL at zirconia implants was associated with significant short-term clinical improvements |
| Persson et al., 2011 [25] | 6 months | Peri-implantitis | Debridement using Er:YAG laser (2.94 μm, 100 mJ/pulse (12.7 J/cm2)) | Debridement using air-abrasive device | The air-abrasive method appeared to have some advantages 1 month after therapy because the countsof pathogens |
| Mariani et al., 2020 [26] | 12 months | Mucositis | Debridement using titanium curettes and power-driven devices + diode laser (980 nm, 2.5 W,10 kHz) | Debridement using titanium curettes and power-driven devices | Diode laser showed little but not statistically significant additional benefits in the treatment of peri-implant mucositis |
| Arisan et al., 2015 [27] | 6 months | Peri-implantitis | Debridement using plastic curettes + diode laser (810 nm (energy density, 3 J/cm2; power density, 400 mW/cm2; energy, 1.5 J; and spot diameter, 1 mm)) | Debridement using plastic curettes | After 6 months, the laser group revealed higher marginal bone loss than the control group. However, in both groups, the microbiota of the implants was found unchanged after 1 month |
| Schwarz et al., 2006 [28] | 12 months | Peri-implantitis | Debridement using Er:YAG laser (2.94 μm, 100 mJ/pulse (12.7 J/cm2), 10 Hz) | Debridement using plastic curettes and 0.2% chlorhexidine | Treatment of periimplantitis lesions with laser resulted in a significantly higher BOP reduction than control group |
| Tenore et al., 2020 [29] | 3 months | Mucositis and peri-implantitis | Debridement using titanium curettes and power-driven devices + diode laser (910 nm, 1 W, 50 s) | Debridement using titanium curettes and power-driven devices | The average PPD value for laser group was significantly decreased at 3 months, like BOP |
| Wang et al., 2019 [30] | 6 months | Peri-implantitis | Full-mouth cleansing and glycine powder + PDT (635 nm, 750 mW) | Full-mouth cleansing and glycine powder + 0.9% normal saline | At 1 month, compared with controls, the PD in the PDT group was larger, while at 3 and 6 months, the PDs were smaller (all p < 0.001) |
| Renvert et al., 2010 [31] | 6 months | Peri-implantitis | Er:YAG laser (2.94 μm, 100 mJ/pulse [12.7 J/cm2], 10 Hz) | Perioflow | A positive treatment outcome, PPD reduction >/−0.5 mm, and gain or no loss of bone was found in 47% and 44% of the perioflow and laser groups, respectively |
| Sánchez-Martos et al., 2020 [32] | 3 months | Mucositis | Debridement with plastic curettes and plastic ultrasound tip + diode laser (810 nm, 1 W, 30 s) | Debridement with plastic curettes and plastic ultrasound tip + sulcus irrigation with 0.12% chlorhexidine and 0.05% cetylpyridinium chloride | The use of diode laser as adjunctive therapy to the conventional treatment of peri-implant mucositis showed promising results, being more effective in reducing the inflammation of the peri-implant tissue |
| Article | Follow-Up | Problem | Intervention | Control | Outcomes |
|---|---|---|---|---|---|
| McKenna et al., 2013 [13] | 21 days | Mucositis | Ozone and saline (1) Ozone and hydrogen peroxide (3) | Hydrogen peroxide and air (2) Air and saline (4) | Significant differences were seen among the treatments (p < 0.01) in plaque (F = 16.68), modified gingival (F = 7.86), and bleeding (F = 18.42) indices. O3 + saline and O3 + H2O2 produced optimum gingival health scores |
| Butera et al., 2021 [33] | 2 months | Mucositis | Professional oral hygiene + ozonized water | Professional oral hygiene + pure water | As regards intragroup differences, in Group 1 ozonized water significantly and progressively reduced all the clinical indexes tested, except for PI in the period T1–T2, whereas no significant differences occurred within the control group |
| Article | Follow-Up | Problem | Intervention | Control | Outcomes |
|---|---|---|---|---|---|
| Hantenaar et al., 2021 [14] | 12 months | Peri-implantitis | Debridement with erytrhritol | Debridement with ultrasonic device | Three months after therapy, no significant difference in mean BoP (%) between air-polishing and ultrasonic therapy was found |
| Riben-Grundstrom et al., 2015 [34] | 12 months | Mucositis | Debridement with glycine | Debridement with ultrasonic device | At 12 months, there was a statistically significant reduction in mean plaque score, bleeding on probing, and number of periodontal pockets ≥4 mm within the treatment groups compared to baseline |
| Ji et al., 2014 [35] | 3 months | Mucositis | Debridement with ultrasonic scaler (carbon fiber tips) + glycine | Debridement with ultrasonic scaler (carbon fiber tips) | At the 3-month visit, the mean reductions in PD at site level were 0.93 ± 0.93 mm and 0.91 ± 0.98 mm in the test and control groups, respectively (p < 0.05), and no significant difference existed between two groups |
| Sahm et al., 2011 [36] | 6 months | Peri-implantitis | Professional oral hygiene + glycine | Debridement using carbon curettes + chlorhexidine | At 6 months, test group revealed significantly higher (p < 0.05) changes in mean BOP scores when compared with control treated sites; both groups exhibited comparable PD reductions |
| Article | Follow-Up | Problem | Intervention | Control | Outcomes |
|---|---|---|---|---|---|
| Hallström et al., 2015 [15] | 6 months | Mucositis | Debridement using titanium curettes + topical application of a droplet of an experimental oil containing Lactobacillus reuteri strains DSM 17938 and ATCC PTA 5289 + lozenges containing the same bacteria (one tablet twice a daily) | Debridement using titanium curettes + topical application of a droplet of a placebo oil + placebo lozenges | After 4 and 12 weeks, all clinical parameters were improved in both the test and the placebo group. PPD and BOP were significantly reduced compared with baseline (p < 0.05), but no significant differences were displayed between the groups. The clinical improvements persisted 3 months after the intervention. |
| Laleman et al., 2020 [37] | 6 months | Peri-implantitis | Debridement using ultrasound specific tips and titanium curettes + drops containing Lactobacillus reuteri DSM 17938 and ATCC PTA 5289 | Debridement using ultrasound specific tips and titanium curettes + placebo drops | All clinical parameters were significantly decreased after 12 and 24 weeks. At the implant level, the only statistically significant difference was a greater decrease in plaque levels in the probiotic versus the control group (p = 0.002 at 24 wks) |
| Tada et al., 2017 [38] | 6 months | Peri-implantitis | Debridement + azithromycin 500 mg once a day for 3 days + probiotic tablets containing Lactobacillus reuteri DSM 17938 and ATCC PTA for 6 months | Debridement + azithromycin 500 mg once a day for 3 days + pacebo tablets for 6 months | PPD in the probiotics group was significantly lower at 4 and 24 weeks than at 0 weeks (p < 0.05); a significant decrease did not occur in the placebo group |
| Mongardini et al., 2016 [39] | 6 weeks | Mucositis | Debridement + PDT + probiotic tablets containing Lactobacillus plantarum and Lactobacillus brevis for 14 days | Debridement + PDT + placebo tablets for 14 days | The combination of plaque removal and PDT, either alone or associated with probiotics, determined a significant reduction of the number of BoP+ sites at 2 and 6 weeks around implants with mucositis |
| Galofré et al., 2017 [40] | 3 months | Mucositis and peri-implantitis | Debridement + probiotic lozenge containing Lactobacillus reuteri DSM 17938 and ATCC PTA 5289 | Debridement + placebo lozenge | The probiotic L. reuteri, together with mechanical therapy, produced an additional improvement over treatment with mechanical therapy alone, both in the general clinical parameters of patients with mucositis and at the level of implants with mucositis or peri-implantitis |
| Peña et al., 2017 [41] | 3 months | Mucositis | Debridement using titanium ultrasound tip + 0.12% chlorhexidine mouthwash + probiotic tablets containing Lactobacillus reuteri DSM 17938 and ATCC PTA 5289 | Debridement + 0.12% chlorhexidine mouthwash + placebo tablets | Following the administration of probiotics or placebo, the clinical variables, except for probing pocket depth, slightly and progressively increased up to 3 months of follow-up, but without reaching baseline levels |
| Article | Follow-Up | Problem | Intervention | Control | Outcomes |
|---|---|---|---|---|---|
| Heitz-Mayfield et al., 2011 [16] | 3 months | Mucositis | Debridement using titanium curettes and carbon fiber curettes + 0.5% chlorhexidine gel twice a day for 4 weeks | Debridement using titanium curettes and carbon fiber curettes + 0.5% placebo gel twice daily for 4 weeks | Adjunctive chlorhexidine gel application did not enhance the results compared with mechanical cleansing alone. There was a reduction in PPD and BoP |
| Menezes et al., 2016 [42] | 6 months | Mucositis | Debridement with plastic curettes + 0.12% chlorhexidine solution was used for brushing the dorsum of the tongue for 1 min, rinsing (the last 10 s, the patient should gargle); and subgingival irrigation 3× within 10 min was performed | Debridement with plastic curettes + placebo solution was used for brushing the dorsum of the tongue for 1 min, rinsing (the last 10 s, the patient should gargle); and subgingival irrigation 3× within 10 min was performed | No statistically significant differences were found between the test and control groups at any time |
| Pulcini et al., 2019 [43] | 12 months | Mucositis | Professional prophylaxis + chlorhexidine mouth rinses twice a day | Professional prophylaxis + placebo mouth rinses twice a day | In the test group, there was a 24.49% greater reduction in BOP at the buccal sites than in controls; 58.3% of test implants and 50% of controls showed healthy peri-implant tissues at final visit (p > 0.05) |
| Hallström et al., 2015 [44] | 3 months | Mucositis | Debridement using titanium curettes and rubber cup + 0.2% chlorhexidine gel (patients were instructed to brush their teeth once daily with gel) | Debridement using titanium curettes and rubber cup + gel without chlorhexidine (patients were instructed to brush their teeth once daily with gel) | The PPD was significantly reduced (p < 0.05) after 12 weeks compared to baseline in the test group but not in the control group |
| Article | Adequate Sequence Generated | Allocation Concealment | Blinding | Incomplete Outcome Data | Registration Outcome |
|---|---|---|---|---|---|
| Aimetti et al., 2019 [12] |  | |  | | |
| Bassetti et al., 2013 [21] | | | | | |
| Schwarz et al., 2005 [22] |  | | | | |
| Schär et al., 2012 [23] | | | | | |
| Schwarz et al., 2015 [24] | | | | | |
| Persson et al., 2011 [25] | | | | | |
| Mariani et al., 2020 [26] | | | | | |
| Arisan et al., 2015 [27] | | | | | |
| Schwarz et al., 2006 [28] | | | | | |
| Tenore et al., 2020 [29] | | | | | |
| Wang et al., 2019 [30] | | | | | |
| Renvert et al., 2010 [31] | | | | | |
| Sánchez-Martos et al., 2020 [32] | | | | | |
| Article | Adequate Sequence Generated | Allocation Concealment | Blinding | Incomplete Outcome Data | Registration Outcome |
|---|---|---|---|---|---|
| McKenna et al., 2013 [13] | | | | | |
| Butera et al., 2021 [33] | | | | | |
| Article | Adequate Sequence Generated | Allocation Concealment | Blinding | Incomplete Outcome Data | Registration Outcome |
|---|---|---|---|---|---|
| Hantenaar et al., 2021 [14] | | | | | |
| Riben-Grundstrom et al., 2015 [34] | | | | | |
| Ji et al., 2014 [35] | | | | | |
| Sahm et al., 2011 [36] | | | | | |
| Article | Adequate Sequence Generated | Allocation Concealment | Blinding | Incomplete Outcome Data | Registration Outcome |
|---|---|---|---|---|---|
| Hallström et al., 2015 [15] | | | | | |
| Laleman et al., 2020 [37] | | | | | |
| Tada et al., 2017 [38] | | | | | |
| Mongardini et al., 2016 [39] | | | | | |
| Galofré et al., 2017 [40] | | | | | |
| Peña et al., 2017 [41] | | | | | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. https://doi.org/10.3390/healthcare10050886
Butera A, Maiorani C, Gallo S, Pascadopoli M, Venugopal A, Marya A, Scribante A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare. 2022; 10(5):886. https://doi.org/10.3390/healthcare10050886
Chicago/Turabian StyleButera, Andrea, Carolina Maiorani, Simone Gallo, Maurizio Pascadopoli, Adith Venugopal, Anand Marya, and Andrea Scribante. 2022. "Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review" Healthcare 10, no. 5: 886. https://doi.org/10.3390/healthcare10050886