
Bone Turnover Alterations after Completing a Multistage Ultra-Trail: A Case Study




Abstract
:1. Introduction
2. Case Report
3. Discussion
3.1. Bone Formation Biomarkers
3.2. Bone Resorption Biomarkers
3.3. Stress Fractures and BTMs
3.4. Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. GLobal Recommendations on Physical Activity for Health. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/325147/WHO-NMH-PND-2019.4-eng.pdf?sequence=1&isAllowed=y%0Ahttp://www.who.int/iris/handle/10665/311664%0Ahttps://apps.who.int/iris/handle/10665/325147 (accessed on 24 February 2022).
- Benedetti, M.G.; Furlini, G.; Zati, A.; Mauro, G.L. The Effectiveness of Physical Exercise on Bone Density in Osteoporotic Patients. BioMed Res. Int. 2018, 2018, 4840531. [Google Scholar] [CrossRef] [PubMed]
- Kopiczko, A.; Adamczyk, J.G.; Gryko, K.; Popowczak, M. Bone mineral density in elite masters athletes: The effect of body composition and long-term exercise. Eur. Rev. Aging Phys. Act. 2021, 18, 7. [Google Scholar] [CrossRef]
- Gómez-Bruton, A.; Gónzalez-Agüero, A.; Gómez-Cabello, A.; Casajús, J.A.; Vicente-Rodríguez, G. Is Bone Tissue Really Affected by Swimming? A Systematic Review. PLoS ONE 2013, 8, e70119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etherington, J.; Harris, P.A.; Nandra, D.; Hart, D.J.; Wolman, R.L.; Doyle, D.V.; Spector, T.D. The effect of weight-bearing exercise on bone mineral density: A study of female ex-elite athletes and the general population. J. Bone Miner. Res. 1996, 11, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.P.R.; Sale, C.; Greeves, J.P.; Casey, A.; Dutton, J.; Fraser, W.D. The effect of training status on the metabolic response of bone to an acute bout of exhaustive treadmill running. J. Clin. Endocrinol. Metab. 2010, 95, 3918–3925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheer, V.; Basset, P.; Giovanelli, N.; Vernillo, G.; Millet, G.P.; Costa, R.J.S. Defining Off-road Running: A Position Statement from the Ultra Sports Science Foundation. Int. J. Sports Med. 2020, 41, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Eston, R.G.; Finney, S.; Baker, S.; Baltzopoulos, V. Muscle tenderness and peak torque changes after downhill running following a prior bout of isokinetic eccentric exercise. J. Sports Sci. 1996, 14, 291–299. [Google Scholar] [CrossRef]
- Scheer, V.; Krabak, B.J. Musculoskeletal Injuries in Ultra-Endurance Running: A Scoping Review. Front. Physiol. 2021, 12, 664071. [Google Scholar] [CrossRef]
- Dawadi, S.; Basyal, B.; Subedi, Y. Morbidity Among Athletes Presenting for Medical Care During 3 Iterations of an Ultratrail Race in the Himalayas. Wilderness Environ. Med. 2020, 31, 437–440. [Google Scholar] [CrossRef]
- Vernillo, G.; Savoldelli, A.; La Torre, A.; Skafidas, S.; Bortolan, L.; Schena, F. Injury and Illness Rates during Ultratrail Running. Int. J. Sports Med. 2016, 37, 565–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, M.D.; Krishnan, E. Health and exercise-related medical issues among 1212 ultramarathon runners: Baseline findings from the Ultrarunners Longitudinal TRAcking (ULTRA) Study. PLoS ONE 2014, 9, e83867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheer, B.V.; Murray, A. Al Andalus Ultra Trail: An observation of medical interventions during a 219-km, 5-day ultramarathon stage race. Clin. J. Sport Med. 2011, 21, 444–446. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.T.; Knechtle, B. Performance in 100-km Ultramarathoners-At Which Age, It Reaches Its Peak? J. Strength Cond. Res. 2020, 34, 1409–1415. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Malcolm, S.A.; Brukner, P.D.; Green, R.M.; Hopper, J.L.; Wark, J.D.; Ebeling, P.R. A 12-month prospective study of the relationship between stress fractures and bone turnover in athletes. Calcif. Tissue Int. 2020, 4, 80–85. [Google Scholar] [CrossRef]
- Nose-Ogura, S.; Yoshino, O.; Dohi, M.; Torii, S.; Kigawa, M.; Harada, M.; Hiraike, O.; Kawahara, T.; Osuga, Y.; Fujii, T.; et al. Relationship between tartrate-resistant acid phosphatase 5b and stress fractures in female athletes. J. Obstet. Gynaecol. Res. 2020, 46, 1436–1442. [Google Scholar] [CrossRef]
- Adami, S.; Gatti, D.; Viapiana, O.; Fiore, C.E.; Nuti, R.; Luisetto, G.; Ponte, M.; Rossini, M. Physical activity and bone turnover markers: A cross-sectional and a longitudinal study. Calcif. Tissue Int. 2008, 83, 388–392. [Google Scholar] [CrossRef]
- Marini, S.; Barone, G.; Masini, A.; Dallolio, L.; Bragonzoni, L.; Longobucco, Y.; Maffei, F. Current Lack of Evidence for an Effect of Physical Activity Intervention Combined with Pharmacological Treatment on Bone Turnover Biomarkers in People with Osteopenia and Osteoporosis: A Systematic Review. J. Clin. Med. 2021, 10, 3442. [Google Scholar] [CrossRef] [PubMed]
- Vasikaran, S.; Eastell, R.; Bruyère, O.; Foldes, A.J.; Garnero, P.; Griesmacher, A.; McClung, M.; Morris, H.A.; Silverman, S.; Trenti, T.; et al. Markers of bone turnover for the prediction of fracture risk and monitoring of osteoporosis treatment: A need for international reference standards. Osteoporos. Int. 2011, 22, 391–420. [Google Scholar] [CrossRef] [PubMed]
- Kerschan-Schindl, K.; Thalmann, M.; Sodeck, G.H.; Skenderi, K.; Matalas, A.L.; Grampp, S.; Ebner, C.; Pietschmann, P. A 246-km continuous running race signinficant changes in bone metabolism. Bone 2009, 45, 1079–1083. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.M.; Law, R.J.; Thom, J.M. The time course and mechanisms of change in biomarkers of joint metabolism in response to acute exercise and chronic training in physiologic and pathological conditions. Eur. J. Appl. Physiol. 2019, 119, 2401–2420. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Geoffroy, V.; Ridall, A.L.; Karsenty, G.; Tracy, T.; Bonner, A.S.; Duffy, J.B.; Gergen, J.P.; Gergen, J.P.; Karlovich, C.A.; et al. Bone Resorption by Osteoclasts. Science 2000, 289, 1504–1509. [Google Scholar]
- Shin, K.-A.; Kim, A.-C.; Kim, Y.-J.; Lee, Y.-H.; Shin, Y.-O.; Kim, S.-H.; Park, Y.-S.; Nam, H.S.; Kim, T.; Kim, H.S.; et al. Effect of Ultra-marathon (308 km) Race on Bone Metabolism and Cartilage Damage Biomarkers. Ann. Rehabil. Med. 2012, 36, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mouzopoulos, G.; Stamatakos, M.; Tzurbakis, M.; Tsembeli, A.; Manti, C.; Safioleas, M.; Skandalakis, P. Changes of bone turnover markers after marathon running over 245 km. Int. J. Sports Med. 2007, 28, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Tian, A.; Ma, J.; Feng, K.; Liu, Z.; Chen, L.; Jia, H.; Ma, X. Reference markers of bone turnover for prediction of fracture: A meta-analysis. J. Orthop. Surg. Res. 2019, 14, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.; Mezquita, P.; De La Higuera, M.; Fernández, D.; Muñoz, M. Actualización sobre la determinación de marcadores de remodelado óseo. Endocrinol. Nutr. 2003, 50, 237–243. [Google Scholar] [CrossRef]
- Bennell, K.L. Models for the pathogenesis of stress fractures in athletes. Br. J. Sports Med. 1996, 30, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Escrivá, D.; Caplliure-Llopis, J.; Benet, I.; Mariscal, G.; Mampel, J.V.; Barrios, C. Differences in adiposity profile and body fat distribution between forwards and backs in sub-elite spanish female rugby union players. J. Clin. Med. 2021, 10, 5713. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.C.; Wang, Z.; Heo, M.; Ross, R.; Janssen, I.; Heymsfield, S.B. Total-body skeletal muscle mass: Development and cross-validation of anthropometric prediction models. Am. J. Clin. Nutr. 2000, 72, 796–803. [Google Scholar] [CrossRef]
- Lecina, M.; Castellar, C.; Pradas, F.; López-Laval, I. 768-km Multi-Stage Ultra-Trail Case Study-Muscle Damage, Biochemical Alterations and Strength Loss on Lower Limbs. Int. J. Environ. Res. Public Health 2022, 19, 876. [Google Scholar] [CrossRef] [PubMed]
- Fowler, J.; Cohen, L.; Jarvis, P. Practical Statistics for Field Biology; John Wiley & Sons: Hoboken, NJ, USA, 2013; ISBN 1118685644. [Google Scholar]
- Sansoni, V.; Vernillo, G.; Perego, S.; Barbuti, A.; Merati, G.; Schena, F.; La Torre, A.; Banfi, G.; Lombardi, G. Bone turnover response is linked to both acute and established metabolic changes in ultra-marathon runners. Endocrine 2017, 56, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Dolan, E.; Varley, I.; Ackerman, K.E.; Pereira, R.M.R.; Elliott-Sale, K.J.; Sale, C. The Bone Metabolic Response to Exercise and Nutrition. Exerc. Sport Sci. Rev. 2020, 48, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Rubert, M.; De la Piedra, C. Osteocalcin: From marker of bone formation to hormone; and bone, an endocrine organ. Osteoporos. Metab Miner. 2021, 12, 146–151. [Google Scholar] [CrossRef]
- Malm, C.; Sjödin, B.; Sjöberg, B.; Lenkei, R.; Renström, P.; Lundberg, I.E.; Ekblom, B. Leukocytes, cytokines, growth factors and hormones in human skeletal muscle and blood after uphill or downhill running. J. Physiol. 2004, 556, 983–1000. [Google Scholar] [CrossRef]
- Knechtle, B.; Nikolaidis, P.T. Physiology and pathophysiology in ultra-marathon running. Front. Physiol. 2018, 9, 634. [Google Scholar] [CrossRef] [Green Version]
- Nizet, A.; Cavalier, E.; Stenvinkel, P.; Haarhaus, M.; Magnusson, P. Bone alkaline phosphatase: An important biomarker in chronic kidney disease—Mineral and bone disorder. Clin. Chim. Acta 2020, 501, 198–206. [Google Scholar] [CrossRef]
- Civitelli, R.; Armamento-Villareal, R.; Napoli, N. Bone turnover markers: Understanding their value in clinical trials and clinical practice. Osteoporos. Int. 2009, 20, 843–851. [Google Scholar] [CrossRef]
- Malm, H.T.; Ronni-Sivula, H.M.; Viinikka, L.U.; Ylikorkala, O.R. Marathon running accompanied by transient decreases in urinary calcium and serum osteocalcin levels. Calcif. Tissue Int. 1993, 52, 209–211. [Google Scholar] [CrossRef]
- Larsen, E.L.; Poulsen, H.E.; Michaelsen, C.; Kjær, L.K.; Lyngbæk, M.; Andersen, E.S.; Petersen-Bønding, C.; Lemoine, C.; Gillum, M.; Jørgensen, N.R.; et al. Differential time responses in inflammatory and oxidative stress markers after a marathon: An observational study. J. Sports Sci. 2020, 38, 2080–2091. [Google Scholar] [CrossRef]
- Lee, J.H. The effect of long-distance running on bone strength and bone biochemical markers. J. Exerc. Rehabil. 2019, 15, 26–30. [Google Scholar] [CrossRef]
- Vora, N.M.; Kukreja, S.C.; York, P.A.J.; Bowser, E.N.; Hargis, G.K.; Williams, G.A. Effect of exercise on serum calcium and parathyroid hormone. J. Clin. Endocrinol. Metab. 1983, 57, 1067–1069. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Subject 1 | Subject 2 | Subject 3 | Subject 4 |
|---|---|---|---|---|
| Age (years) | 33 | 37 | 41 | 42 |
| VO2max (mL/kg/min−1) | 58.28 | 70.6 | 67.1 | 50.71 |
| HRmax (beats·min−1) | 194 | 186 | 194 | 176 |
| Maximal aerobic speed (km·h−1) | 18 | 17 | 16.7 | 16 |
| Height (cm) | 180.7 | 176.1 | 172.3 | 173.9 |
| Weight (kg) | 79.1 | 64.9 | 60.8 | 77.3 |
| BMI | 24.2 | 20.9 | 20.5 | 25.6 |
| Fat mass (%) | 8.82 | 6.88 | 8.70 | 8.14 |
| Muscle mass (%) | 43.4 | 47.38 | 57.63 | 38.55 |
| Experience (years) | 6 | 6 | 4 | 7 |
| Distance covered (h·week−1) | 11 | 11 | 15 | 11 |
| Annual slope accumulated (m) | 140,655 | 120,404 | 156,000 | 70,000 |
| Stages | Distance (km) | Elevation (m+) | Elevation (m−) |
|---|---|---|---|
| 1 | 78.5 | 3136 | 3024 |
| 2 | 72.3 | 3886 | 3458 |
| 3 | 72 | 4655 | 4044 |
| 4 | 68.1 | 5660 | 4581 |
| 5 | 72.6 | 5411 | 6336 |
| 6 | 76.1 | 5344 | 4788 |
| 7 | 63.7 | 5492 | 5163 |
| 8 | 66 | 3641 | 4576 |
| 9 | 66.1 | 3361 | 3841 |
| 10 | 66.5 | 2958 | 2934 |
| 11 | 83 | 3321 | 4100 |
| Total | 784.9 | 46,865 | 46,845 |
| Md | 71.35 | 4260.45 | 4258.63 |
| Sd | ±6.00 | ±1063.26 | ±989.13 |
| Parameter Blood (Reference Values) | Before-Race | Post-Race | ||
|---|---|---|---|---|
| Pre (Baseline) Value | Post (Post-Exercise) Value (% Difference) | Day 2 (rec2) Value (% Difference) | Day 9 (rec9) Value (% Difference) | |
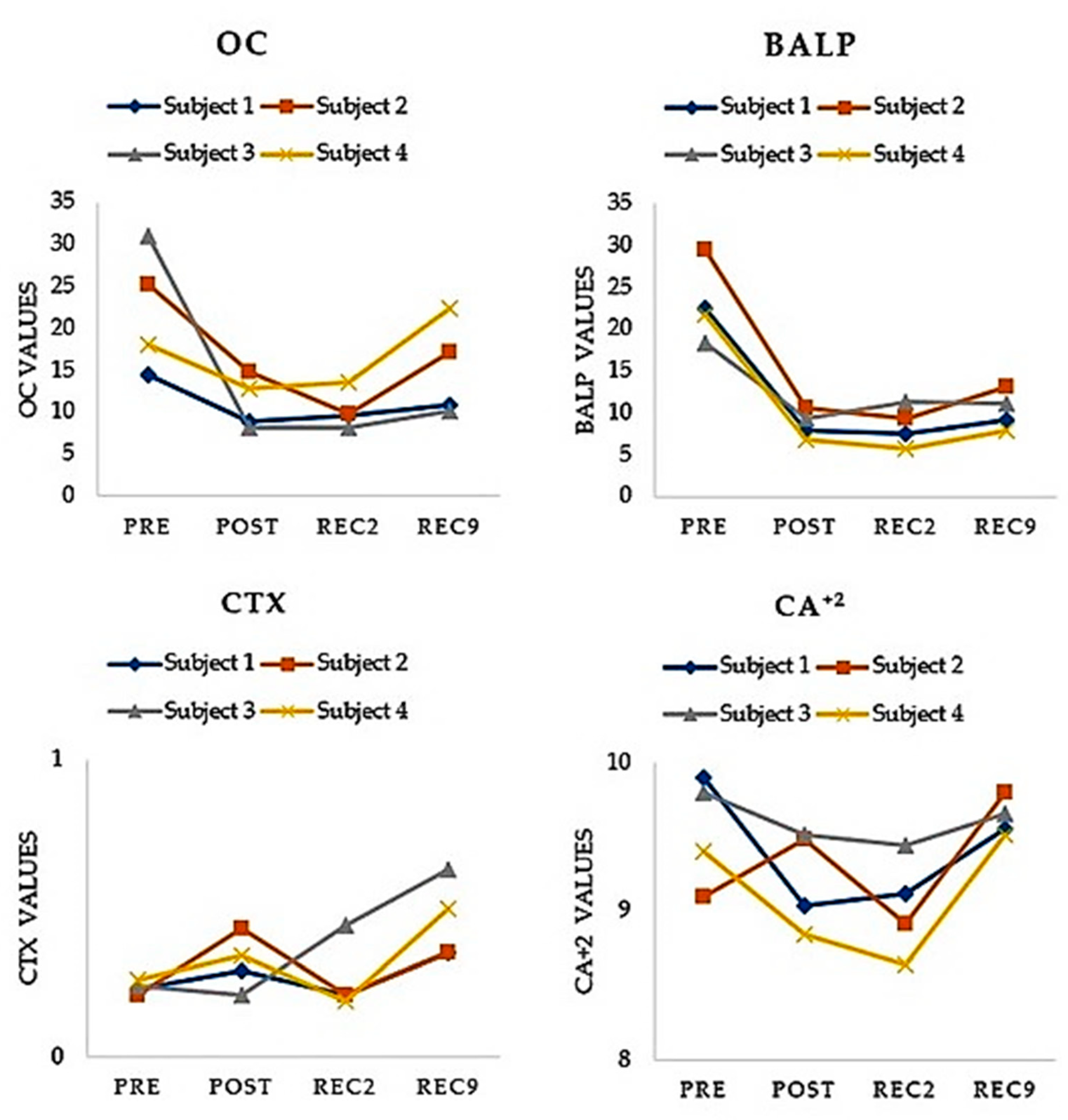
| OC (ng/mL) (13.98–41.99) | 22.20 ± 7.41 | 11.15 ± 3.14 ↓ (−45.78) | 10.30 ± 2.29 ↓ (−48.31) | 15.14 ± 5.73 ↓ (−25.12) |
| BALP (ug/L) (6–30) | 23.03 ± 4.68 | 8.64 ± 1.63 ↓ (−61.74) | 8.50 ± 2.37 ↓ (−61.66) | 10.29 ± 2.30 ↓ (−54.65) |
| CTX (μg/L) (0.23–0.94) | 0.24 ± 0.02 | 0.32 ± 0.09 ↑ (+37.28) | 0.26 ± 0.12 ↑ (+11.93) | 0.46 ± 0.14 ↑ (+93.41) |
| Ca2+ (mg/L) (8.70–10.40) | 9.35 ± 0.33 | 9.22 ± 0.32 ↓ (−3.60) | 9.03 ± 0.34 ↓ (−3.38) | 9.64 ± 0.12 ↑ (+3.15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellar-Otín, C.; Lecina, M.; Pradas, F. Bone Turnover Alterations after Completing a Multistage Ultra-Trail: A Case Study. Healthcare 2022, 10, 798. https://doi.org/10.3390/healthcare10050798
Castellar-Otín C, Lecina M, Pradas F. Bone Turnover Alterations after Completing a Multistage Ultra-Trail: A Case Study. Healthcare. 2022; 10(5):798. https://doi.org/10.3390/healthcare10050798
Chicago/Turabian StyleCastellar-Otín, Carlos, Miguel Lecina, and Francisco Pradas. 2022. "Bone Turnover Alterations after Completing a Multistage Ultra-Trail: A Case Study" Healthcare 10, no. 5: 798. https://doi.org/10.3390/healthcare10050798