
The Interpersonal Dimension of Pandemic Fear and the Dual-Factor Model of Mental Health: The Role of Coping Strategies


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Preliminary Analysis
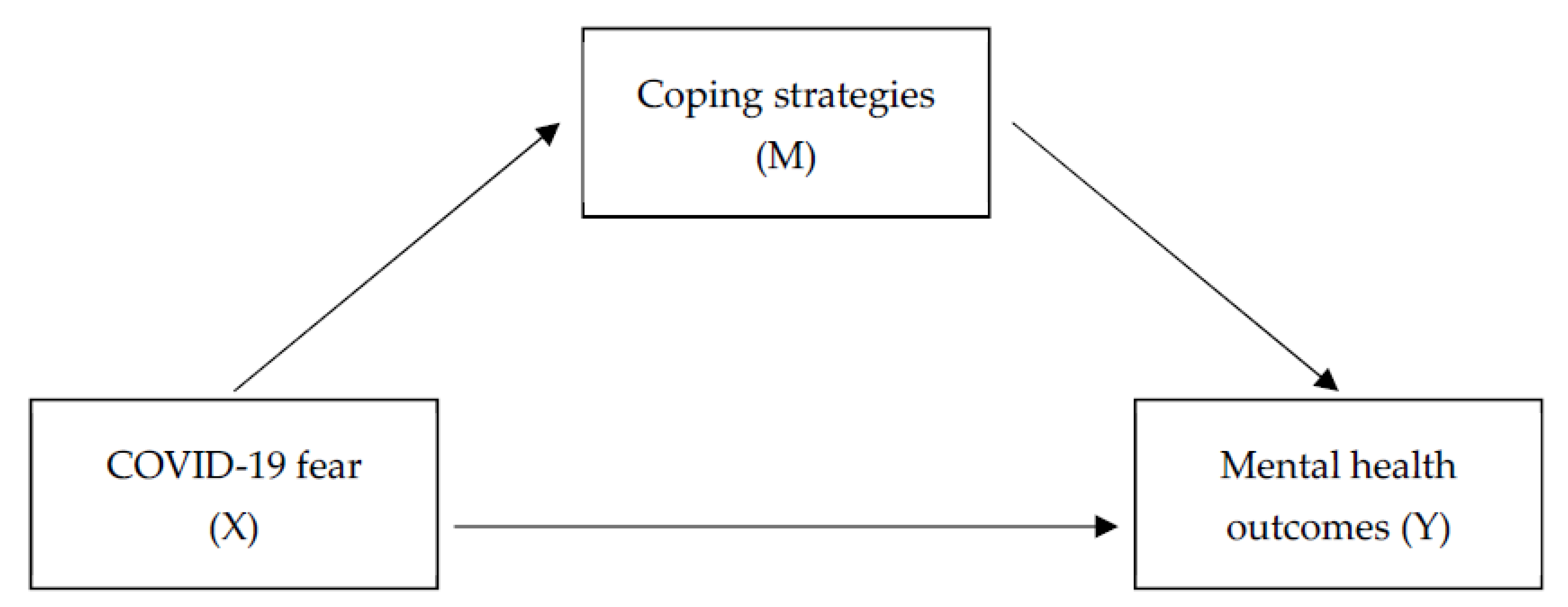
3.2. Pandemic Fear and Negative and Positive Mental Health Outcomes: The Mediating Role of Coping Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pappas, G.; Kiriaze, I.J.; Giannakis, P.; Falagas, M.E. Psychosocial consequences of infectious diseases. Clin. Microbiol. Infect. 2009, 15, 743–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.K.W.; Wong, C.W.; Tsang, J.; Wong, K.C. Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychol. Med. 2004, 34, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Gardner, P.J.; Moallef, P. Psychological impact on SARS survivors: Critical review of the English language literature. Can. Psychol. 2015, 56, 123–135. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.E. Affiliation and stress. In Oxford Handbook of Stress, Health, and Coping; Folkman, S., Ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Fino, E.; Fino, V.; Mazzetti, M.; Russo, P.M. Tending and mending: Affiliative responses to the COVID-19 pandemic by healthcare professionals in Italy. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S171–S173. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Res. 2020, 290, 113117. [Google Scholar] [CrossRef]
- Röhr, S.; Müller, F.; Jung, F.; Apfelbacher, C.; Seidler, A.; Riedel-Heller, S.G. Psychosoziale Folgen von Quarantänemaßnahmen bei schwerwiegenden Coronavirus-Ausbrüchen: Ein Rapid Review. Psychosocial Impact of Quarantine Measures during Serious Coronavirus Outbreaks: A Rapid Review. Psychiatr. Prax. 2020, 47, 179–189. [Google Scholar]
- Wigand, M.E.; Becker, T.H.; Steger, F. Psychosocial Reactions to Plagues in the Cultural History of Medicine A Medical Humanities Approach. J. Nerv. Ment. Dis. 2020, 208, 443–444. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. Posttraumatic Growth: Conceptual Foundations and Empirical Evidence. Psychol. Inq. 2004, 15, 1–18. [Google Scholar] [CrossRef]
- Epstein, J.M.; Parker, J.; Cummings, D.; Hammond, R.A. Coupled Contagion Dynamics of Fear and Disease: Mathematical and Computational Explorations. PLoS ONE 2008, 3, e3955. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Sun, C.; Chen, J.; Jen, H.; Kang, X.L.; Kao, C.; Chou, K. A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2020, 30, 102–116. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Doege, D.; Thong, M.S.; Arndt, V. The relationship between posttraumatic growth and health-related quality of life in adult cancer survivors: A systematic review. J. Affect. Disord. 2020, 276, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, M.; Pfefferbaum, B. Posttraumatic Growth as a Response to Natural Disasters in Children and Adolescents. Curr. Psychiatry Rep. 2018, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Pooley, J.A.; Sims, K. Post-traumatic growth amongst refugee populations: A systematic review. In The Routledge International Handbook of Psychosocial Resilience; Routledge: Abingdon, UK; New York, NY, USA, 2017; Chapter 19. [Google Scholar]
- Bonanno, G.A. Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive After Extremely Aversive Events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Bonanno, G.A.; Ho, S.M.Y.; Chan, J.C.K.; Kwong, R.S.Y.; Cheung, C.K.Y.; Wong, C.P.Y.; Wong, V.C.W. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: A latent class approach. Health Psychol. 2008, 27, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Linley, P.A.; Joseph, S. Positive change following trauma and adversity: A review. J. Trauma. Stress 2004, 17, 11–21. [Google Scholar] [CrossRef]
- Skinner, E.A.; Edge, K.; Altman, J.; Sherwood, H. Searching for the structure of coping: A review and critique of category systems for classifying ways of coping. Psychol. Bull. 2003, 129, 216–269. [Google Scholar] [CrossRef] [Green Version]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef]
- Paredes, M.R.; Apaolaza, V.; Fernandez-Robin, C.; Hartmann, P.; Yañez-Martinez, D. The impact of the COVID-19 pandemic on subjective mental well-being: The interplay of perceived threat, future anxiety and resilience. Pers. Individ. Differ. 2020, 170, 110455. [Google Scholar] [CrossRef]
- Fino, E.; Mema, D.; Russo, P. War trauma exposed refugees and posttraumatic stress disorder: The moderating role of trait resilience. J. Psychosom. Res. 2020, 129, 109905. [Google Scholar] [CrossRef]
- Morris, N.; Moghaddam, M.; Tickle, A.; Biswas, S. The relationship between coping style and psychological distress in people with head and neck cancer: A systematic review. Psycho-Oncology 2018, 27, 734–747. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Strengthening Mental Health Promotion; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Keyes, C.L.; Shmotkin, D.; Ryff, C.D. Optimizing well-being: The empirical encounter of two traditions. J. Personal. Soc. Psychol. 2002, 82, 1007–1022. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Promoting and protecting mental health as flourishing: A complementary strategy for improving national mental health. Am. Psychol. 2007, 62, 95–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen-Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Bontempo, R. Translation fidelity of psychological scales: An item response theory analysis of an individualism-collectivism scale. J. Cross-Cult. Psychol. 1993, 24, 149–166. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. Fear of COVID-19 and the mental health consequences in America. Psychol. Trauma Theory Res. Pract. Policy 2020, 12 (Suppl. S1), S17–S21. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.M.Y.; Kwong-Lo, R.S.Y.; Mak, C.W.Y.; Wong, J.S. Fear of Severe Acute Respiratory Syndrome (SARS) Among Health Care Workers. J. Consult. Clin. Psychol. 2005, 73, 344–349. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Whelan-Goodinson, R.; Ponsford, J.; Schönberger, M. Validity of the Hospital Anxiety and Depression Scale to assess depression and anxiety following traumatic brain injury as compared with the Structured Clinical Interview for DSM-IV. J. Affect. Disord. 2009, 114, 94–102. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. The Posttraumatic Growth Inventory: Measuring the positive legacy of trauma. J. Trauma. Stress 1996, 9, 455–471. [Google Scholar] [CrossRef] [PubMed]
- Tobin, D.L.; Holroyd, K.A.; Reynolds, R.V.; Wigal, J.K. The hierarchical factor structure of the coping strategies inventory. Cogn. Ther. Res. 1989, 13, 343–361. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2013. [Google Scholar]
- Jiang, H.J.; Nan, J.; Lv, Z.Y.; Yang, J. Psychological impacts of the COVID-19 epidemic on Chinese people: Exposure, post-traumatic stress symptom, and emotion regulation. Asian Pac. J. Trop. Med. 2020, 13, 252–259. [Google Scholar]
- Findlay, C.L.; Ruhab, A.; Kohen, D. Understanding the Perceived Mental Health of Canadians during the COVID-19 Pandemic. Health Rep. 2020, 31, 22–27. [Google Scholar]
- Boyraz, G.; Legros, D.N.; Tigershtrom, A. COVID-19 and traumatic stress: The role of perceived vulnerability, COVID-19-related worries, and social isolation. J. Anxiety Disord. 2020, 76, 102307. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. COVID-19 Pandemic in the Italian Population: Validation of a Post-Traumatic Stress Disorder Questionnaire and Prevalence of PTSD Symptomatology. Int. J. Environ. Res. Public Health 2020, 17, 4151. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H.C. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Shansky, R.M. Sex differences in PTSD resilience and susceptibility: Challenges for animal models of fear learning. Neurobiol. Stress 2015, 1, 60–65. [Google Scholar] [CrossRef] [Green Version]
- Fino, E.; Di Campli, S.; Patrignani, G.; Mazzetti, M. The Modulating Role of Gender and Aggression in Emotional Reactions of Nursing Students: A Cross sectional Study. J. Adv. Nurs. 2019, 75, 1462–1472. [Google Scholar] [CrossRef] [PubMed]
- Schubert, C.F.; Schmidt, U.; Rosner, R. Posttraumatic Growth in Populations with Posttraumatic Stress Disorder-A Systematic Review on Growth-Related Psychological Constructs and Biological Variables. Clin. Psychol. Psychother. 2016, 23, 469–486. [Google Scholar] [CrossRef] [PubMed]
- Fino, E.; Bonfrate, I.; Fino, V.; Bocus, P.; Russo, P.M.; Mazzetti, M. Harnessing distress to boost growth in frontline healthcare workers during COVID-19 pandemic: The protective role of resilience, emotion regulation and social support. Psychol. Med. 2021, 1–3. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. (%); Mean (SD) | |||||
|---|---|---|---|---|---|
| Total Sample (n = 231) | Males (n = 62) | Females (n = 169) | F/χ2 | p | |
| Age | 10.035 | 0.040 | |||
| 18–24 years | 51 (21.1) | 8 (12.9) | 43 (25.4) | ||
| 25–34 years | 70 (30.3) | 26 (41.9) | 44 (26.0) | ||
| 35–44 years | 63 (27.3) | 17 (27.4) | 46 (27.2) | ||
| 45–54 years | 35 (15.2) | 6 (9.6) | 29 (17.1) | ||
| 55–65 years | 12 (5.2) | 5 (8.0) | 7 (4.1) | ||
| Civil status | 2.283 | 0.684 | |||
| Single | 105 (45.5) | 26 (41.9) | 79 (46.7) | ||
| In a relationship | 22 (9.5) | 4 (6.4) | 18 (10.6) | ||
| Married | 95 (41.1) | 30 (48.3) | 65 (38.4) | ||
| Divorced/widowed | 9 (3.9) | 2 (3.2) | 7 (4.1) | ||
| Education | 13.393 | 0.004 | |||
| High school | 21 (9.7) | 12 (19.3) | 9 (5.3) | ||
| University | 113 (48.9) | 32 (51.6) | 81 (47.9) | ||
| Post-graduate | 97 (42.0) | 18 (29.0) | 79 (46.7) | ||
| Fear of COVID-19 | 60.1 (13.1) | 55.4 (12.5) | 61.8 (13.0) | 11.022 | 0.001 |
| Anxiety (HADS) | 8.3 (3.4) | 7.5 (2.8) | 8.6 (3.5) | 4.707 | 0.031 |
| Cutoff score ≥ 8 | 58 (25.1) | 7 (11.2) | 51 (30.1) | 8.906 | 0.012 |
| Depression (HADS) | 7.9 (2.7) | 7.3 (2.9) | 8.2 (2.6) | 4.064 | 0.045 |
| Cutoff score ≥ 8 | 39 (16.4) | 8 (12.9) | 31 (18.4) | 1.176 | 0.555 |
| Post-traumatic growth (PTGI) | 55.7 (22.4) | 47.6 (23.5) | 58.8 (21.3) | 11.344 | 0.001 |
| Relationships with others (PTGI) | 18.8 (7.8) | 16.5 (8.3) | 19.6 (7.5) | 7.145 | 0.008 |
| New possibilities (PTGI) | 12.2 (5.8) | 10.3 (5.6) | 12.9 (5.8) | 8.733 | 0.003 |
| Personal strength (PTGI) | 11.6 (4.9) | 10.1 (5.0) | 12.1 (4.7) | 6.968 | 0.009 |
| Spirituality (PTGI) | 5.2 (2.8) | 4.2 (2.5) | 5.5 (2.8) | 10.023 | 0.002 |
| Appreciation for life (PTGI) | 8.1 (3.4) | 6.6 (3.5) | 8.6 (3.2) | 16.892 | <0.001 |
| Engagement coping (CSI-SF) | 18.0 (4.2) | 16.8 (4.0) | 18.5 (4.3) | 7.095 | 0.008 |
| Disengagement coping (CSI-SF) | 7.3 (5.4) | 5.9 (4.2) | 7.8 (5.8) | 5.984 | 0.015 |
| Total Effect | Direct Effect | Indirect Effect (Disengagement Coping) | Indirect Effect (Engagement Coping) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE | LLCI I | ULC | β | SE | LLCI | ULCI | β | bootSE | bootLLCI | bootULCI | β | bootSE | bootLLCI | bootULCI | |
| Anxiety | 0.559 | 0.014 | [0.115 | 0.172] | 0.297 | 0.015 | [0.045 | 0.106] | 0.334 | 0.051 | [0.237 | 0.433] | −0.072 | 0.027 | [−0.127 | −0.020] |
| Depression | 0.382 | 0.013 | [0.054 | 0.107] | 0.218 | 0.015 | [0.017 | 0.075] | 0.318 | 0.055 | [0.211 | 0.428] | −0.155 | 0.031 | [−0.221 | −0.098] |
| PTG | 0.312 | 0.108 | [0.313 | 0.738] | 0.282 | 0.126 | [0.034 | 0.531] | −0.066 | 0.040 | [−0.147 | 0.010] | 0.211 | 0.044 | [0.131 | 0.301] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fino, E.; Mema, D.; Treska, V. The Interpersonal Dimension of Pandemic Fear and the Dual-Factor Model of Mental Health: The Role of Coping Strategies. Healthcare 2022, 10, 247. https://doi.org/10.3390/healthcare10020247
Fino E, Mema D, Treska V. The Interpersonal Dimension of Pandemic Fear and the Dual-Factor Model of Mental Health: The Role of Coping Strategies. Healthcare. 2022; 10(2):247. https://doi.org/10.3390/healthcare10020247
Chicago/Turabian StyleFino, Edita, Denis Mema, and Valbona Treska. 2022. "The Interpersonal Dimension of Pandemic Fear and the Dual-Factor Model of Mental Health: The Role of Coping Strategies" Healthcare 10, no. 2: 247. https://doi.org/10.3390/healthcare10020247