

A Hybrid Risk Factor Evaluation Scheme for Metabolic Syndrome and Stage 3 Chronic Kidney Disease Based on Multiple Machine Learning Techniques
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
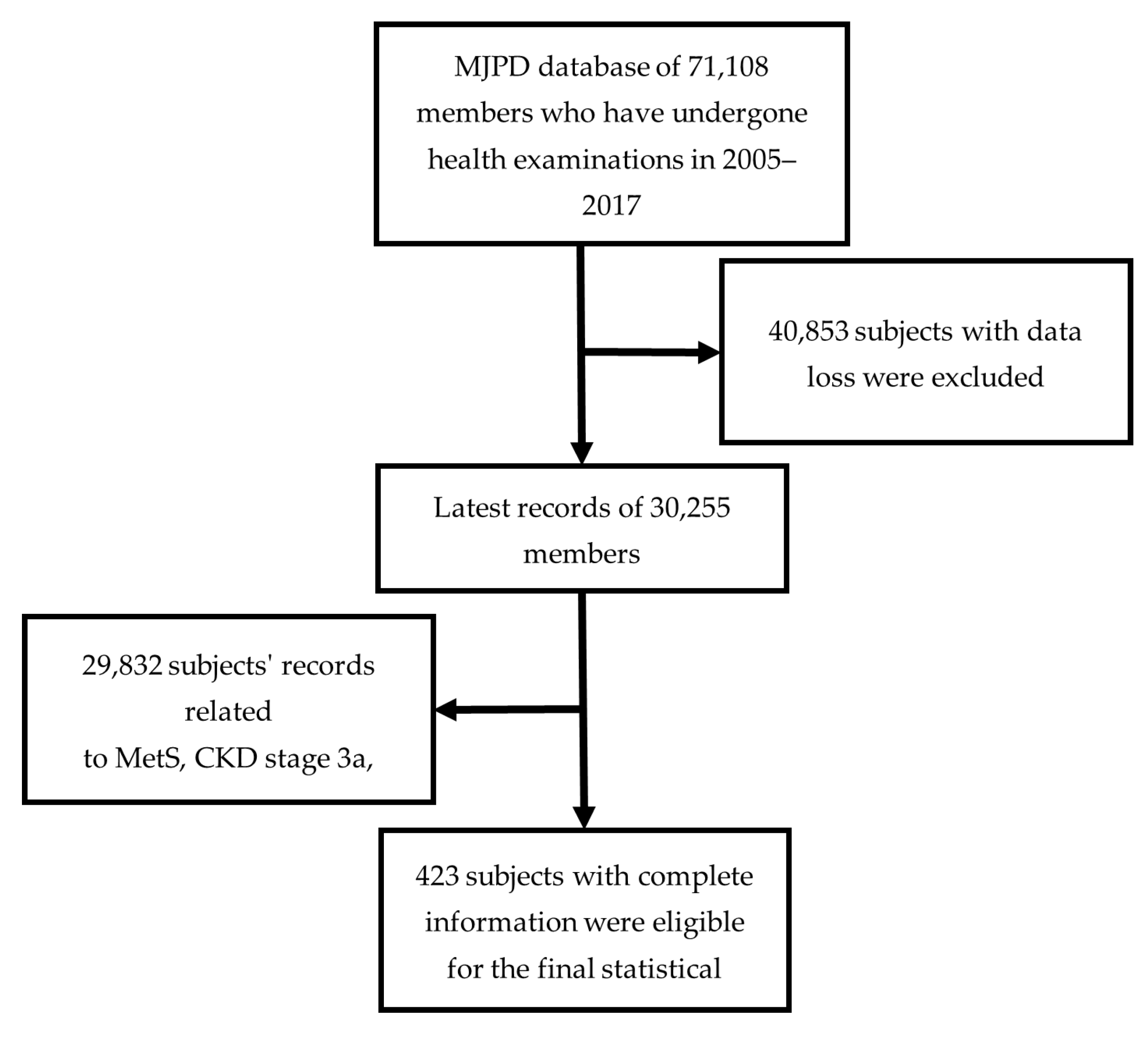
2.1. Data
2.2. Proposed Hybrid Risk Factor Evaluation Scheme
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Health Promotion Administration, Ministry of Health and Welfare. Metabolic Syndrome Criteria. 2007. Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=639&pid=1219 (accessed on 1 September 2022).
- Khosravi, A.; Sadeghi, M.; Barghikar, M. Which Components of Metabolic Syndrome Have a Greater Effect on Mortality, CVA and Myocardial Infarction, Hyperglycemia, High Blood Pressure or Both? Adv. Biomed. Res. 2017, 6, 121. [Google Scholar] [CrossRef] [Green Version]
- DeBoer, M.D.; Filipp, S.L.; Musani, S.K.; Sims, M.; Okusa, M.D.; Gurka, M.J. Metabolic Syndrome Severity and Risk of CKD and Worsened GFR: The Jackson Heart Study. Kidney Blood Press. Res. 2018, 43, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Adair, K.E.; Ylitalo, K.R.; Forsse, J.S.; Funderburk, L.K.; Bowden, R.G. Metabolic Constellations, Clusters, and Renal Function: Findings from the 2013–2018 National Health and Nutrition Examination Surveys. Life 2021, 11, 904. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Eckardt, K.U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; de Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Atkins, R.; Coresh, J.; Cohen, E.P.; Collins, A.J.; Eckardt, K.U.; Nahas, M.E.; Jaber, B.L.; Jadoul, M.; Levin, A.; et al. Chronic kidney disease as a global public health problem: Approaches and initiatives—A position statement from kidney disease improving global outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Baek, S.D.; Baek, C.H.; Kim, J.S.; Kim, S.M.; Kim, J.H.; Kim, S.B. Does stage III chronic kidney disease always progress to endstage renal disease? A ten-year follow-up study. Scand. J. Urol. Nephrol. 2012, 46, 232–238. [Google Scholar] [CrossRef]
- Lee, J.; Oh, K.-H.; Park, S.-K. Dietary Micronutrients and Risk of Chronic Kidney Disease: A Cohort Study with 12 Year Follow-Up. Nutrients 2021, 13, 1517. [Google Scholar] [CrossRef]
- Prasad, G.V. Metabolic syndrome and chronic kidney disease: Current status and future directions. World J. Nephrol. 2014, 3, 210–219. [Google Scholar] [CrossRef]
- Choe, W.S.; Choi, E.K.; Han, K.D.; Lee, E.J.; Lee, S.R.; Cha, M.J.; Oh, S. Association of metabolic syndrome and chronic kidney disease with atrial fibrillation: A nationwide population-based study in Korea. Diabetes Res. Clin. Pract. 2019, 148, 14–22. [Google Scholar] [CrossRef]
- Tozawa, M.; Iseki, C.; Tokashiki, K.; Chinen, S.; Kohagura, K.; Kinjo, K.; Takishita, S.; Iseki, K. Metabolic syndrome and risk of developing chronic kidney disease in Japanese adults. Hypertens. Res. 2007, 30, 937–943. [Google Scholar] [CrossRef]
- Thomas, G.; Sehgal, A.R.; Kashyap, S.R.; Srinivas, T.R.; Kirwan, J.P.; Navaneethan, S.D. Metabolic syndrome and kidney disease: A systematic review and meta-analysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 2364–2373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonhauser, M.; Fernandez, G.; Püschel, K.; Yañez, F.; Montero, J.; Thompson, B.; Coronado, G. Improving physical fitness and emotional well-being in adolescents of low socioeconomic status in Chile: Results of a school-based controlled trial. Health Promot. Int. 2005, 20, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chertow, G.M.; Hsu, C.Y.; Johansen, K.L. The enlarging body of evidence: Obesity and chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 1501–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, R.M.; Brown, T.M.; Muntner, P. Epidemiology of obesity, the metabolic syndrome, and chronic kidney disease. Curr. Hypertens. Rep. 2012, 14, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Chiu, Y.-L.; Jhou, M.-J.; Lee, T.-S.; Lu, C.-J.; Chen, M.-S. Health Data-Driven Machine Learning Algorithms Applied to Risk Indicators Assessment for Chronic Kidney Disease. Risk Manag. Healthc. Policy 2021, 14, 4401–4412. [Google Scholar] [CrossRef]
- Shih, C.-C.; Lu, C.-J.; Chen, G.-D.; Chang, C.-C. Risk Prediction for Early Chronic Kidney Disease: Results from an Adult Health Examination Program of 19,270 Individuals. Int. J. Environ. Res. Public Health 2020, 17, 4973. [Google Scholar] [CrossRef]
- Chowdhury, N.H.; Reaz, M.B.I.; Haque, F.; Ahmad, S.; Ali, S.H.M.; A Bakar, A.A.; Bhuiyan, M.A.S. Performance Analysis of Conventional Machine Learning Algorithms for Identification of Chronic Kidney Disease in Type 1 Diabetes Mellitus Patients. Diagnostics 2021, 11, 2267. [Google Scholar] [CrossRef]
- Wang, W.; Chakraborty, G.; Chakraborty, B. Predicting the Risk of Chronic Kidney Disease (CKD) Using Machine Learning Algorithm. Appl. Sci. 2021, 11, 202. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; KS, K.; Dovgan, E.; Luštrek, M.; Gradišek Piletič, B.; Srinivasan, K.; Li, Y.-C.; Gradišek, A.; Syed-Abdul, S. Machine Learning Prediction Models for Chronic Kidney Disease Using National Health Insurance Claim Data in Taiwan. Healthcare 2021, 9, 546. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, P.-H.C.; Krause, J.; Peng, L. How to Read Articles That Use Machine Learning: Users’ Guides to the Medical Literature. JAMA 2019, 322, 1806–1816. [Google Scholar] [CrossRef]
- Triantafyllidis, A.K.; Tsanas, A. Applications of Machine Learning in Real-Life Digital Health Interventions: Review of the Literature. J. Med. Internet Res. 2019, 21, e12286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peiffer-Smadja, N.; Rawson, T.M.; Ahmad, R.; Buchard, A.; Georgiou, P.; Lescure, F.X.; Birgand, G.; Holmes, A.H. Machine learning for clinical decision support in infectious diseases: A narrative review of current applications. Clin. Microbiol. Infect. 2020, 26, 584–595. [Google Scholar] [CrossRef]
- Huang, L.-Y.; Chen, F.-Y.; Jhou, M.-J.; Kuo, C.-H.; Wu, C.-Z.; Lu, C.-H.; Chen, Y.-L.; Pei, D.; Cheng, Y.-F.; Lu, C.-J. Comparing Multiple Linear Regression and Machine Learning in Predicting Diabetic Urine Albumin–Creatinine Ratio in a 4-Year Follow-Up Study. J. Clin. Med. 2022, 11, 3661. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Yeh, J.-H.; Chiu, H.-C.; Chen, Y.-M.; Jhou, M.-J.; Liu, T.-C.; Lu, C.-J. Utilization of Decision Tree Algorithms for Supporting the Prediction of Intensive Care Unit Admission of Myasthenia Gravis: A Machine Learning-Based Approach. J. Pers. Med. 2022, 12, 32. [Google Scholar] [CrossRef]
- Pes, B. Ensemble feature selection for high-dimensional data: A stability analysis across multiple domains. Neural Comput. Appl. 2020, 32, 5951–5973. [Google Scholar] [CrossRef] [Green Version]
- Galar, M.; Fernandez, A.; Barrenechea, E.; Bustince, H.; Herrera, F. A review on ensembles for the class imbalance problem: Bagging-, boosting-, and hybrid-based approaches. IEEE Trans. Syst. Man Cybern. Part C (Appl. Rev.) 2012, 42, 463–484. [Google Scholar] [CrossRef]
- Amasyali, M.F.; Ersoy, O. A comparative review of regression ensembles on drug design datasets. Turk. J. Electr. Eng. Comput. Sci. 2013, 21, 586–602. [Google Scholar] [CrossRef]
- Alghamdi, M.; Al-Mallah, M.; Keteyian, S.; Brawner, C.; Ehrman, J.; Sakr, S. Predicting diabetes mellitus using SMOTE and ensemble machine learning approach: The Henry Ford ExercIse Testing (FIT) project. PLoS ONE 2017, 12, e0179805. [Google Scholar] [CrossRef] [Green Version]
- Tuli, S.; Basumatary, N.; Gill, S.S.; Kahani, M.; Arya, R.C.; Wander, G.S.; Buyya, R. HealthFog: An ensemble deep learning based Smart Healthcare System for Automatic Diagnosis of Heart Diseases in integrated IoT and fog computing environments. Futur. Gener. Comput. Syst. 2020, 104, 187–200. [Google Scholar] [CrossRef] [Green Version]
- Weber, C.; Röschke, L.; Modersohn, L.; Lohr, C.; Kolditz, T.; Hahn, U.; Ammon, D.; Betz, B.; Kiehntopf, M. Optimized Identification of Advanced Chronic Kidney Disease and Absence of Kidney Disease by Combining Different Electronic Health Data Resources and by Applying Machine Learning Strategies. J. Clin. Med. 2020, 9, 2955. [Google Scholar] [CrossRef]
- Glazyrin, Y.E.; Veprintsev, D.V.; Ler, I.A.; Rossovskaya, M.L.; Varygina, S.A.; Glizer, S.L.; Zamay, T.N.; Petrova, M.M.; Minic, Z.; Berezovski, M.V.; et al. Proteomics-Based Machine Learning Approach as an Alternative to Conventional Biomarkers for Differential Diagnosis of Chronic Kidney Diseases. Int. J. Mol. Sci. 2020, 21, 4802. [Google Scholar] [CrossRef] [PubMed]
- Granal, M.; Slimani, L.; Florens, N.; Sens, F.; Pelletier, C.; Pszczolinski, R.; Casiez, C.; Kalbacher, E.; Jolivot, A.; Dubourg, L.; et al. Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study. Nutrients 2022, 14, 2419. [Google Scholar] [CrossRef]
- Lee, C.-L.; Liu, W.-J.; Tsai, S.-F. Development and Validation of an Insulin Resistance Model for a Population with Chronic Kidney Disease Using a Machine Learning Approach. Nutrients 2022, 14, 2832. [Google Scholar] [CrossRef] [PubMed]
- Abutaleb, N. Why we should sub-divide CKD stage 3 into early (3a) and late (3b) components. Nephrol. Dial. Transplant. 2007, 22, 2728–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahran, A.; Shoker, A. About CKD stage-3 subdivision proposal. Nephrol. Dial. Trans. 2008, 23, 1765. [Google Scholar] [CrossRef] [Green Version]
- Segal, Z.; Kalifa, D.; Radinsky, K.; Ehrenberg, B.; Elad, G.; Maor, G.; Lewis, M.; Tibi, M.; Korn, L.; Koren, G. Machine learning algorithm for early detection of end-stage renal disease. BMC Nephrol. 2020, 21, 518. [Google Scholar] [CrossRef]
- Oh, T.R.; Song, S.H.; Choi, H.S.; Suh, S.H.; Kim, C.S.; Jung, J.Y.; Choi, K.H.; Oh, K.-H.; Ma, S.K.; Bae, E.H.; et al. Predictive Model for High Coronary Artery Calcium Score in Young Patients with Non-Dialysis Chronic Kidney Disease. J. Pers. Med. 2021, 11, 1372. [Google Scholar] [CrossRef] [PubMed]
- Silveira, A.C.M.d.; Sobrinho, Á.; Silva, L.D.d.; Costa, E.d.B.; Pinheiro, M.E.; Perkusich, A. Exploring Early Prediction of Chronic Kidney Disease Using Machine Learning Algorithms for Small and Imbalanced Datasets. Appl. Sci. 2022, 12, 3673. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.-Y.J.; Lee, K.L.; Ingersoll, G.M. An introduction to logistic regression analysis and reporting. J. Educ. Res. 2002, 96, 3–14. [Google Scholar] [CrossRef]
- Friedman, J.H. Multivariate adaptive regression splines. Ann. Stat. 1991, 19, 1–67. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Ke, G.; Meng, Q.; Finley, T.W.; Wang, T.; Chen, W.; Ma, W.; Qiwei, Y.; Liu, T. LightGBM: A highly efficient gradient boosting decision tree. In Proceedings of the Advances in Neural Information Processing Systems, Long Beach, CA, USA, 4–9 December 2017; pp. 3147–3155. [Google Scholar]
- Dorogush, A.V.; Ershov, V.; Gulin, A. CatBoost: Gradient boosting with categorical features support. arXiv 2018, arXiv:1810.11363. [Google Scholar] [CrossRef]
- Meng, J.; Hao, H.; Luan, Y. Classifier ensemble selection based on affinity propagation clustering. J. Biomed. Inform. 2016, 60, 234–242. [Google Scholar] [CrossRef]
- Woloshuk, A.; Khochare, S.; Almulhim, A.F.; McNutt, A.T.; Dean, D.; Barwinska, D.; Ferkowicz, M.J.; Eadon, M.T.; Kelly, K.J.; Dunn, K.W.; et al. In Situ Classification of Cell Types in Human Kidney Tissue Using 3D Nuclear Staining. Cytom. Part A 2021, 99, 707–721. [Google Scholar] [CrossRef]
- Liao, P.-C.; Chen, M.-S.; Jhou, M.-J.; Chen, T.-C.; Yang, C.-T.; Lu, C.-J. Integrating Health Data-Driven Machine Learning Algorithms to Evaluate Risk Factors of Early Stage Hypertension at Different Levels of HDL and LDL Cholesterol. Diagnostics 2022, 12, 1965. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M. Caret: Classification and Regression Training. R Package Version, 6.0-93. 2022. Available online: https://CRAN.R-project.org/package=caret (accessed on 1 September 2022).
- Breiman, L.; Cutler, A.; Liaw, A.; Wiener, M. randomForest: Breiman and Cutler’s Random Forests for Classification and Regression. R Package Version, 4.7-1.1. 2022. Available online: https://CRAN.R-project.org/package=randomForest (accessed on 1 September 2022).
- Milborrow, S. Derived from Mda: MARS by T. Hastie and R. Tibshirani. Earth: Multivariate Adaptive Regression Splines. R Package Version, 5.3.1. 2021. Available online: http://CRAN.R-project.org/package=earth (accessed on 1 September 2022).
- Chen, T.; He, T.; Benesty, M.; Khotilovich, V.; Tang, Y.; Cho, H.; Chen, K.; Mitchell, R.; Cano, I.; Zhou, T.; et al. Xgboost: Extreme Gradient Boosting. R Package Version, 1.6.0.1. 2022. Available online: https://CRAN.R-project.org/package=xgboost (accessed on 1 September 2022).
- Yandex Technologies. CatBoost: Unbiased Boosting with Categorical Features. R Package Version, 1.0.6. 2022. Available online: https://github.com/catboost/catboost/ (accessed on 1 September 2022).
- Microsoft. LightGBM: Light Gradient Boosting Machine. R Package Version, 3.3.2. 2022. Available online: https://github.com/microsoft/LightGBM (accessed on 1 September 2022).
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Boulware, L.E.; Jaar, B.G.; Tarver-Carr, M.E.; Brancati, F.L.; Powe, N.R. Screening for Proteinuria in US Adults: A cost-effectiveness analysis. JAMA 2003, 290, 3101–3114. [Google Scholar] [CrossRef] [Green Version]
- Wen, C.P.; Cheng, T.Y.; Tsai, M.K.; Chang, Y.C.; Chan, H.T.; Tsai, S.P.; Chiang, P.H.; Hsu, C.C.; Sung, P.K.; Hsu, Y.H.; et al. All-cause mortality attributable to chronic kidney disease: A prospective cohort study based on 462,293 adults in Taiwan. Lancet 2008, 371, 2173–2182. [Google Scholar] [CrossRef]
- Kazancioğlu, R. Risk factors for chronic kidney disease: An update. Kidney Int. Suppl. 2013, 3, 368–371. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.J.; Lin, K.R.; Lin, M.T.; Chang, J.L. Association between lifestyle factors and decreased kidney function in older adults: A community-based cross-sectional analysis of the Taipei City elderly health examination database. BMC Nephrol. 2020, 21, 169. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, B.; Sheng, L.-T.; Pan, X.-F.; Zhou, Y.; Zhu, J.; Li, X.; Yang, K.; Guo, K.; Zhang, X.; et al. Association between weight status, metabolic syndrome, and chronic kidney disease among middle-aged and elderly Chinese. Nutr. Metab. Cardiovasc. Dis. NMCD 2020, 30, 2017–2026. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | 1 | 2 | 3a | 3b | 4 | 5 |
|---|---|---|---|---|---|---|
| e-GFR value | ≥90 | 89–60 | 59–45 | 45–30 | 30–15 | <15 or dialysis |
| Description | Kidney damage with normal or e -GFR | Kidney damage with normal or mild e-GFR | Mild-moderately decreased e-GFR | Moderately-severely decreased e-GFR | Severely decreased e-GFR | Severe Renal failure |
| Abbreviation | Variables | Unit/Description |
|---|---|---|
| BMI | Body Mass Index | kg/m2 |
| BF | Body Fat | % (@TANITA, DC-430MA) |
| WC | Waist Circumference | cm |
| SBP | Systolic Blood Pressure | mmHg |
| DBP | Diastolic Blood Pressure | mmHg |
| FPG | Fasting Plasma Glucose | mg/dL |
| L-IOP # | Left Intraocular Pressure | mmHg |
| R-IOP # | Right Intraocular Pressure | mmHg |
| r-GT | Gamma Glutamyl Transpeptidase | U/L |
| BUN | Blood Urea Nitrogen | mg/dL |
| UA | Uric Acid | mg/dL |
| TG | Triglyceride | mg/dL |
| T-Cho | Total Cholesterol | mg/dl |
| HDL-C | High Density Lipoprotein-Cholesterol | mg/dL |
| LDL-C | Low Density Lipoprotein-Cholesterol | mg/dL |
| C/H | T-Cho/HDL-C | the vascular risk predicts index |
| MS | Marital Status | (1) Single, (2) married, remarried, cohabiting, (3) divorced, (4) widowed |
| EL | Educational Level | (1) No formal education, (2) elementary school, (3) secondary school, (4) high school, (5) college, (6) university, (7) graduate school |
| FI | Yearly Family Income | (1) Unwaged, (2) NTD ≤ 200,000, (3) NTD 200,001–400,000, (4) NTD 400,001–800,000, (5) NTD 800,001–1,200,000, (6) NTD 1,200,001–1,600,000, (7) NTD 1,600,001–2,000,000; NTD: New Taiwan Dollar. |
| HC | Hip Circumference | cm |
| WHR | Waist–hip Ratio | % |
| LEE | Lower Extremity Edema | (1) No, (2) Yes |
| SGOT | Serum Glutamic-Oxaloacetic Transaminase | U/L |
| SGPT | Serum Glutamic-Pyruvic Transaminase | U/L |
| BMD | Bone Mass Density | Dual energy X-ray Absorptiometry (DEXA) |
| RBCs | Red Blood Cells | 106/μl |
| Hb | Hemoglobin | g/dl |
| MCV | Mean Cell Volume | fl |
| UP | Urine Protein | Qualitative test, (1) non, (2) +−, (3) + (4) ++, (5) +++, (6) ++++ |
| GU | Glucose Urine | Qualitative test, (1) non, (2) +−, (3) + (4) ++, (5) +++, (6) ++++ |
| CS | Current Smokers | (1) Never, (2) passive smoking, (3) quit, (4) occasional, (5) addicted |
| AD | Alcohol Drinkers | (1) Never, (2) quit, (3) 1–2 times a week, (4) 3–4 times a week, (5) 5–6 times a week, (6) addicted |
| CBN | Chewing “Betel Nut”/“Areca catechu” | (1) Never, (2) quit, (3) 1–3 times a week, (4) 4–5 times a week, (5) addicted |
| CKD | Chronic Kidney Disease | (1) CKD stage 3a, (2) CKD stage 3b |
| Variables | Mean ± SD | Variables | n (%) | ||
|---|---|---|---|---|---|
| BMI | 27.19 ± 3.29 | FI | (1) Unwaged | 78 (18.44%) | |
| BF | 30.32 ± 6.99 | (2) NTD ≤ 200,000 | 60 (14.18%) | ||
| WC | 90.21 ± 8.50 | (3) NTD 200,001–400,000 | 87 (20.57%) | ||
| SBP | 138.18 ± 20.54 | (4) NTD 400,001–800,000 | 82 (19.39%) | ||
| DBP | 84.30 ± 12.50 | (5) NTD 800,001–1,200,000 | 47 (11.11%) | ||
| FPG | 123.20 ± 34.35 | (6) NTD 1,200,001–1,600,000 | 35 (8.27%) | ||
| L-IOP | 14.60 ± 3.40 | (7) NTD 1,600,001–2,000,000 | 34 (8.04%) | ||
| R-IOP | 14.51 ± 3.28 | LEE | (1) No | 418 (98.82%) | |
| r-GT | 38.95 ± 45.14 | (2) Yes | 5 (1.18%) | ||
| BUN | 18.54 ± 4.74 | UP | (1) non | 333 (78.72%) | |
| UA | 7.43 ± 1.64 | (2) +− | 34 (8.04%) | ||
| TG | 194.49 ± 78.31 | (3) + | 29 (6.86%) | ||
| T-Cho | 204.55 ± 37.69 | (4) ++ | 16 (3.78%) | ||
| HDL-C | 47.36 ± 9.98 | (5) +++ | 11 (2.60%) | ||
| LDL-C | 123.30 ± 34.39 | (6) ++++ | NA | ||
| C/H | 4.42 ± 0.85 | GU | (1) non | 405 (95.74%) | |
| HC | 99.28 ± 6.22 | (2) +− | 7 (1.65%) | ||
| WHR | 0.91 ± 0.06 | (3) + | 3 (0.71%) | ||
| SGOT | 28.61 ± 13.88 | (4) ++ | 2 (0.47%) | ||
| SGPT | 34.19 ± 21.16 | (5) +++ | 6 (1.42%) | ||
| BMD | 0.35 ± 1.43 | (6) ++++ | NA | ||
| RBCs | 4.84 ± 0.54 | CS | (1) Never | 292 (69.03%) | |
| Hb | 14.48 ± 1.47 | (2) Passive smoking | 15 (3.55%) | ||
| MCV | 43.19 ± 4.34 | (3) Quit | 57 (13.48%) | ||
| UR | 1.1 ± 0.55 | (4) Occasional | 13 (3.07%) | ||
| (5) Addicted | 46 (10.87%) | ||||
| Variables | n (%) | AD | (1) Never | 327 (77.3%) | |
| MS | (1) Single | 12 (2.84%) | (2) Quit | 22 (5.2%) | |
| (2) Married, remarried, cohabiting | 332 (78.49%) | (3) 1–2 times a week | 44 (10.4%) | ||
| (3) Divorced | 13 (3.07%) | (4) 3–4 times a week | 17 (4.02%) | ||
| (4) Widowed | 66 (15.60%) | (5) 5–6 times a week | NA | ||
| EL | (1) No formal education | 30 (7.09%) | (6) Addicted | 13 (3.07%) | |
| (2) Elementary school | 101 (23.88%) | CBN | (1) Never | 376 (88.89%) | |
| (3) Secondary school | 51 (12.06%) | (2) Quit | 36 (8.51%) | ||
| (4) High school | 64 (15.13%) | (3) 1–3 times a week | 3 (0.71%) | ||
| (5) College | 55 (13.00%) | (4) 4–5 times a week | 3 (0.71%) | ||
| (6) University | 74 (17.49%) | (5) Addicted | 5 (1.18%) | ||
| (7) Graduate school | 48 (11.35%) | CKD | (1) CKD stage 3a | 375 (88.65%) | |
| (2) CKD stage 3b | 48 (11.35%) | ||||
| Methods | Balanced Accuracy Mean (SD) | Sensitivity Mean (SD) | Specificity Mean (SD) | AUC Mean (SD) |
|---|---|---|---|---|
| RF | 0.698 (0.09) | 0.697 (0.21) | 0.700 (0.17) | 0.657 (0.12) |
| LGR | 0.719 (0.06) | 0.678 (0.19) | 0.761 (0.25) | 0.670 (0.09) |
| MARS | 0.690 (0.07) | 0.774 (0.21) | 0.606 (0.26) | 0.658 (0.09) |
| XGBoost | 0.685 (0.09) | 0.615 (0.16) | 0.755 (0.16) | 0.658 (0.14) |
| CatBoost | 0.710 (0.19) | 0.698 (0.17) | 0.722 (0.18) | 0.667 (0.13) |
| LightGBM | 0.660 (0.12) | 0.624 (0.26) | 0.697 (0.27) | 0.662 (0.14) |
| RF | MARS | XGBoost | CatBoost | LightGBM | |
|---|---|---|---|---|---|
| LGR | 1.258 (0.208) | 1.402 (0.160) | 1.615 (0.106) | 0.693 (0.488) | 0.184 (0.853) |
| Variables | Average Ranking of RF | Average Ranking of LGR | Average Ranking of MARS | Average Ranking of XGBoost | Average Ranking of CatBoost | Average Ranking of LightGBM | Average Ranking of the Six Models (SD) |
|---|---|---|---|---|---|---|---|
| BMI | 14 | 12 | 7 | 12 | 29 | 5 | 13.17 (8.47) |
| BF | 12 | 14 | 22 | 15 | 20 | 25 | 18.00 (5.10) |
| WC | 24 | 30 | 26 | 17 | 15 | 26 | 23.00 (5.80) |
| SBP | 4 | 4 | 5 | 5 | 2 | 7 | 4.50 (1.64) |
| DBP | 25 | 27 | 14 | 29 | 33 | 20 | 24.67 (6.77) |
| FPG | 15 | 6 | 11 | 14 | 13 | 14 | 12.17 (3.31) |
| L-IOP | 20 | 19 | 20 | 23 | 16 | 13 | 18.50 (6.35) |
| R-IOP | 9 | 2 | 3 | 4 | 8 | 6 | 5.33 (6.60) |
| r-GT | 18 | 37 | 9 | 20 | 22 | 12 | 19.67 (9.81) |
| BUN | 1 | 1 | 1 | 1 | 1 | 1 | 1 (0) |
| UA | 22 | 23 | 27 | 16 | 25 | 19 | 22.00 (4.00) |
| TG | 10 | 33 | 19 | 9 | 7 | 9 | 14.50 (9.99) |
| T-Cho | 13 | 8 | 23 | 10 | 6 | 15 | 12.50 (6.09) |
| HDL-C | 7 | 17 | 12 | 8 | 18 | 2 | 10.67 (6.19) |
| LDL-C | 17 | 16 | 6 | 13 | 28 | 22 | 17.00 (7.54) |
| … | … | … | … | … | … | … | … |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jhou, M.-J.; Chen, M.-S.; Lee, T.-S.; Yang, C.-T.; Chiu, Y.-L.; Lu, C.-J. A Hybrid Risk Factor Evaluation Scheme for Metabolic Syndrome and Stage 3 Chronic Kidney Disease Based on Multiple Machine Learning Techniques. Healthcare 2022, 10, 2496. https://doi.org/10.3390/healthcare10122496
Jhou M-J, Chen M-S, Lee T-S, Yang C-T, Chiu Y-L, Lu C-J. A Hybrid Risk Factor Evaluation Scheme for Metabolic Syndrome and Stage 3 Chronic Kidney Disease Based on Multiple Machine Learning Techniques. Healthcare. 2022; 10(12):2496. https://doi.org/10.3390/healthcare10122496
Chicago/Turabian StyleJhou, Mao-Jhen, Ming-Shu Chen, Tian-Shyug Lee, Chih-Te Yang, Yen-Ling Chiu, and Chi-Jie Lu. 2022. "A Hybrid Risk Factor Evaluation Scheme for Metabolic Syndrome and Stage 3 Chronic Kidney Disease Based on Multiple Machine Learning Techniques" Healthcare 10, no. 12: 2496. https://doi.org/10.3390/healthcare10122496