
Effect of the Sway Bed on Autonomic Response, Emotional Responses, and Muscle Hardness in Children with Severe Motor and Intellectual Disabilities: A Pilot Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Location
2.3. Sway Bed
2.4. Study Outcomes
2.4.1. Autonomic Response
2.4.2. Emotional Responses
2.4.3. Muscle Hardness
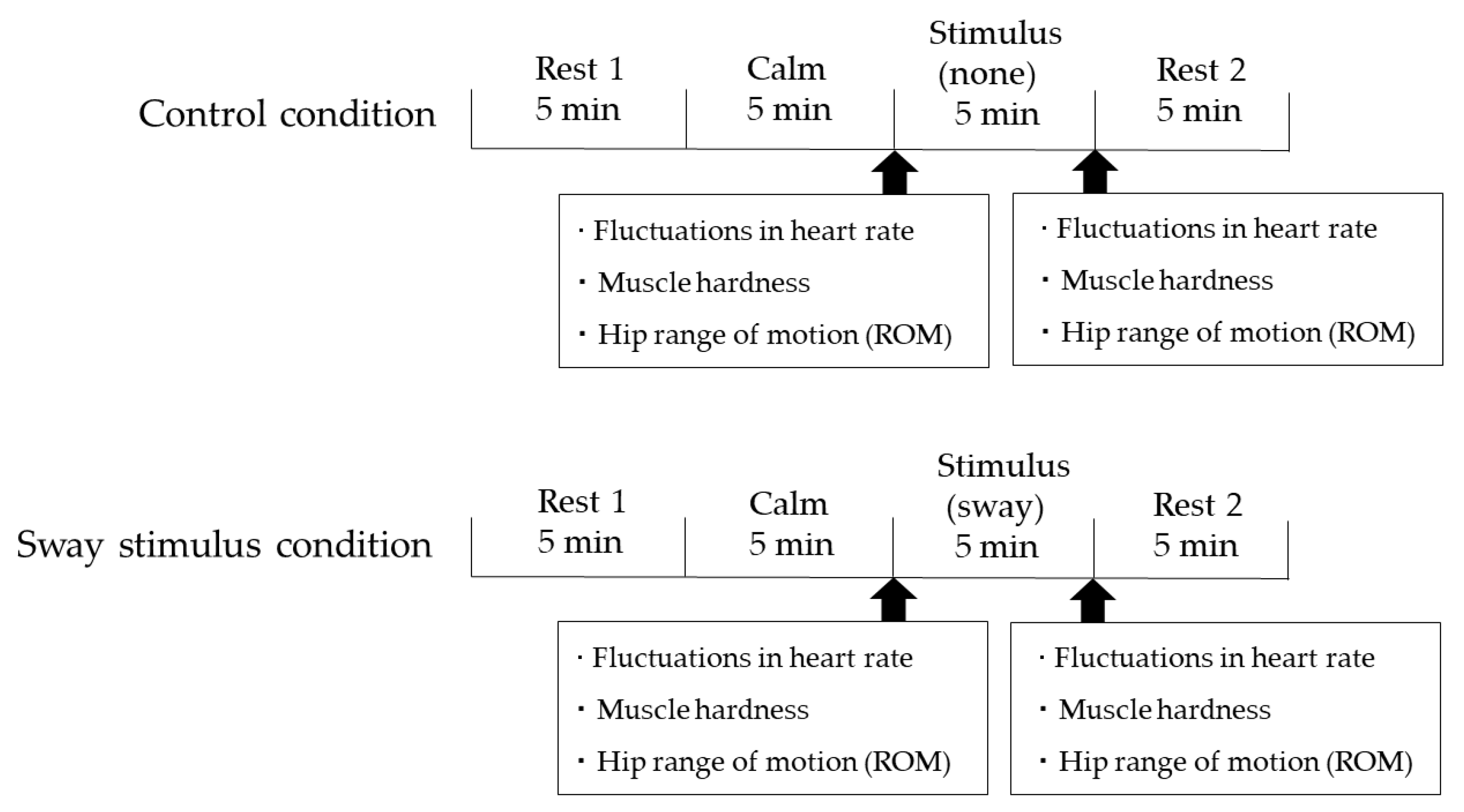
2.5. Experimental Protocol
2.6. Data Analysis
2.7. Ethical Considerations
3. Results

{kind=link}
{kind=link}
{kind=link}
| Item | Control Conditions | Sway Stimulus Conditions | Amount of Change | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Control Conditions | Sway Stimulus Conditions | Comparison between the Two Conditions | |||||||
| Pre | Post | p | Pre | Post | p | Pre | Post | p | |
| Median (IQR) | Median (IQR) | Median (IQR) | |||||||
| LF/HF | 1.09 (0.5–1.3) | 1.04 (0.6–1.8) | 0.38 | 0.96 (0.8–2.6) | 0.79 (0.4–1.8) | <0.005 | 0.25 (−0.3–−0.7) | −0.34 (−0.3–−0.7) | <0.007 |
| HF | 48.03 (42.8–63.2) | 48.97 (35.4–61.1) | 0.44 | 51.04 (27.2–55.5) | 55.78 (34.6–69.9) | <0.005 | −5.7 (−15.7–−13.7) | 7.50 (4.4–15.8) | <0.01 |
| Muscle hardness [right] (N) | 33.5 (28.7–39.0) | 33.00 (29.7–37.2) | 0.79 | 37.00 (31.5–39.5) | 36.50 (28.5–39.5) | 0.73 | −5.72 (−15.7–13.7) | 7.50 (4.4–15.8) | 0.62 |
| Muscle hardness [left] (N) | 35.0 (32.0–39.2) | 36.00 (31.0–37.5) | 0.36 | 37.50 (34.7–40.2) | 36.00 (35.7–39.2) | 0.70 | −1 (−2.5–1.2) | 0.5 (−1–2.2) | 0.21 |
| Hip range of motion (cm) | 51.00 (28.0–62.7) | 48.50 (26.1–56.7) | 0.87 | 47.50 (33.3–65.2) | 45.50 (35.2–58.2) | 0.53 | 1.00 (−6.5–4.0) | 0.75 (−5.2–3.5) | 0.87 |
| Item | Control Conditions | Sway Stimulus Conditions | p |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Awakening/arousal | 10 (10–10) | 10 (10–10) | 0.32 |
| Enjoyment | 5.5 (5–7) | 7 (5–7) | 0.29 |
| Body movement | 5 (2–6) | 5 (3–5) | 0.46 |
| Relaxation | 7 (4–8) | 8 (7–10) | <0.04 |
| Satisfaction | 6.5 (5–8) | 6.5 (5–7.5) | 0.31 |
| Anger | 1 (1–1) | 1 (1–1) | 0.32 |
| Depression/sorrow | 1 (1–1) | 1 (1–1) | 0.31 |
| Anxiety/fear | 1 (1–1.3) | 1 (1–1) | 0.18 |
4. Discussion
4.1. The Impact of Sway Stimuli on Relaxation in Children with SMID
4.2. The Impact of Sway Stimuli on Muscle Hardness in Children with SMID
4.3. Limitations
4.4. Introduction of Sway Bed Use in the Clinical Setting for Children with SMID
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Oshima, K. Basic issue on severe motor and intellectual disabilities. Nippon Koshu Eisei 1971, 35, 648–655. (In Japanese) [Google Scholar]
- Suzuki, Y.; Kobayashi, M.; Kuwabara, K.; Kawabe, M.; Kikuchi, C.; Fukuda, M. Skin temperature responses to cold stress in patients with severe motor and intellectual disabilities. Brain Dev. 2013, 35, 265–269. [Google Scholar] [CrossRef]
- van Timmeren, E.A.; van der Putten, A.A.J.; van Schrojenstein Lantman-de Valk, H.M.J.; van der Schans, C.P.; Waninge, A. Prevalence of reported physical health problems in people with severe or profound intellectual and motor disabilities: A cross-sectional study of medical records and care plans. J. Intellect. Disabil. Res. 2016, 60, 1109–1118. [Google Scholar] [CrossRef]
- Mensch, S.M.; Echteld, M.A.; Lemmens, R.; Oppewal, A.; Evenhuis, H.M.; Rameckers, E.A.A. The relationship between motor abilities and quality of life in children with severe multiple disabilities. J. Intellect. Disabil. Res. 2019, 63, 100–112. [Google Scholar] [CrossRef]
- Riquelme, I.; Cifre, I.; Montoya, P. Age-related changes of pain experience in cerebral palsy and healthy individuals. Pain Med. 2011, 12, 535–545. [Google Scholar] [CrossRef]
- Dahan-Oliel, N.; Mazer, B.; Majnemer, A. Preterm birth and leisure participation: A synthesis of the literature. Res. Dev. Disabil. 2012, 33, 1211–1220. [Google Scholar] [CrossRef]
- Russman, B.S. Cerebral palsy. Curr. Treat. Options Neurol. 2000, 2, 97–108. [Google Scholar] [CrossRef]
- Tekin, F.; Kavlak, E.; Cavlak, U.; Altug, F. Effectiveness of neuro developmental treatment (Bobath concept) on postural control and balance in cerebral palsied children. J. Back Musculoskelet. Rehabil. 2018, 31, 397–403. [Google Scholar] [CrossRef]
- Pin, T.; Dyke, P.; Chan, M. The effectiveness of passive stretching in children with cerebral palsy. Dev. Med. Child. Neuro. 2006, 48, 855–862. [Google Scholar] [CrossRef]
- Benson, H.; Klipper, M.X. The Relaxation Response; Harper Collins e-Books: New York, NY, USA, 2009. [Google Scholar]
- Nakao, M. Heart rate variability and perceived stress as measurements of relaxation response. J. Clin. Med. 2019, 8, 1704. [Google Scholar] [CrossRef] [Green Version]
- Hyman, R.B.; Feldman, H.R.; Harris, R.B.; Levin, R.F.; Malloy, G.B. The effects of relaxation training on clinical symptoms: A meta-analysis. Nurs. Res. 1989, 38, 216–220. [Google Scholar] [CrossRef]
- Velluti, R.A. Interactions between sleep and sensory physiology. J. Sleep Res. 1997, 6, 61–77. [Google Scholar] [CrossRef]
- Bayer, L.; Constantinescu, I.; Perrig, S.; Vienne, J.; Vidal, P.P.; Muhlethaler, M.; Schwartz, S. Rocking synchronizes brain waves during a short nap. Curr. Biol. 2011, 21, R461–R462. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, M.; Kaname, T.; Tabata, M.; Hotta, K.; Shimizu, R.; Kamiya, K.; Kamekawa, D.; Kato, M.; Akiyama, A.; Ohta, M.; et al. Hippotherapy to improve hypertonia caused by an autonomic imbalance in children with spastic cerebral palsy. Kitasato Med. J. 2013, 43, 67–73. [Google Scholar]
- Park, I.K.; Lee, J.Y.; Suk, M.H.; Yoo, S.; Seo, Y.G.; Oh, J.K.; Kwon, J.Y. Effect of equine assisted activities on cardiac autonomic function in children with cerebral palsy: A pilot randomized controlled trial. J. Altern. Complement Med. 2021, 27, 96–102. [Google Scholar] [CrossRef]
- Cheng, H.Y.; Yu, Y.C.; Wong, A.M.; Tsai, Y.S.; Ju, Y.Y. Effects of an eight-week whole body vibration on lower extremity muscle tone and function in children with cerebral palsy. Res. Dev. Disabil. 2015, 38, 256–261. [Google Scholar] [CrossRef]
- Ao, A.; Tokunaga, O.; Aita, C.; Samura, T.; Sasaki, Y.; Miyashita, R.; Miyanomae, T. An open label uncontrolled trial of the efficacy and safety of a hug with singing and rocking for promotion of relaxation in pediatric patients with severe motor and intellectual disabilities: Study protocol. Kurume Med. J. 2019, 65, 91–97. [Google Scholar] [CrossRef]
- Iwanaga, R.; Murata, J.; Tokunaga, A.; Tanaka, R.; Higashionna, T.; Tateishi, K. Effectiveness of the sway bed on joint mobility and emotional and behavioral responses in children with severe physical and intellectual disabilities. Jpn. J. Occup. Ther. Pediatr. 2017, 5, 9–12. (In Japanese) [Google Scholar]
- Reaves, C.; Angosta, A.D. The relaxation response: Influence on psychological and physiological responses in patients with COPD. Appl. Nurs. Res. 2021, 57, 1–6. [Google Scholar] [CrossRef]
- Gao, Z.; Zhao, L.; Fekete, G.; Katona, G.; Baker, J.S.; Gu, Y. Continuous time series analysis on the effects of induced running fatigue on leg symmetry using kinematics and kinetic variables: Implications for knee joint injury during a countermovement jump. Front. Physiol. 2022, 17, 1571. [Google Scholar] [CrossRef]
- Sawada, T.; Okawara, H.; Nakashima, D.; Iwabuchi, S.; Matsumoto, M.; Nakamura, M.; Nagura, T. Reliability of trapezius muscle hardness measurement: A comparison between portable muscle hardness meter and ultrasound strain elastography. Sensors 2020, 20, 7200. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [CrossRef] [Green Version]
- Kasaoka, S.; Nakahara, T.; Kawamura, Y.; Tsuruta, R.; Maekawa, T. Real-time monitoring of heart rate variability in critically ill patients. J. Crit. Care 2010, 25, 313–316. [Google Scholar] [CrossRef]
- Delaney, J.P.; Leong, K.S.; Watkins, A.; Brodie, D. The short-term effects of myofascial trigger point massage therapy on cardiac autonomic tone in healthy subjects. J. Adv. Nurs. 2002, 37, 364–371. [Google Scholar] [CrossRef]
- Chen, J.H.; Chao, Y.H.; Lu, S.F.; Shiung, T.F.; Chao, Y.F. The effectiveness of valerian acupressure on the sleep of ICU patients: A randomized clinical trial. Int. J. Nurs. Stud. 2012, 49, 913–920. [Google Scholar] [CrossRef]
- Peng, S.M.; Koo, M.; Yu, Z.R. Effects of music and essential oil inhalation on cardiac autonomic balance in healthy individuals. J. Altern. Complement. Med. 2009, 15, 53–57. [Google Scholar] [CrossRef]
- Crivelli, F.; Omlin, X.; Rauter, G.; von Zitzewitz, J.; Achermann, P.; Riener, R. Somnomat: A novel actuated bed to investigate the effect of vestibular stimulation. Med. Biol. Eng. Comput. 2016, 54, 877–889. [Google Scholar] [CrossRef]



| Case | Sex | Age | Bodyweight (kg) | Diagnosis | GMFCS 1 Level | Characteristics |
|---|---|---|---|---|---|---|
| A | Male | 17 years and 9 months | 38.0 | Sequelae of an acute encephalopathy, Refractory epilepsy | V | No clear response when spoken to. |
| B | Male | 16 years and 4 months | 18.9 | Cerebral palsy (athetosis type), Osteoarthritis, Periventricular leukomalacia, Kernicterus | V | No clear response when spoken to. Switches gaze to the direction of voice and smiles at times when spoken to. |
| C | Female | 17 years and 1 month | 37.2 | Low birth weight, Cerebral palsy, Congenital cataract, Suspected Leigh syndrome | V | Shifts gaze, and moves left hand a little to make simple yes/no signals when spoken to. Smiles when comfortable and distorts face when uncomfortable. |
| D | Male | 14 years and 2 months | 18.7 | Sequelae of an acute encephalopathy, Pneumonia, Epilepsy, Ulcerative colitis, Scoliosis, Dehydration | V | No clear response when spoken to. Switches gaze to the direction of voice and smiles at times when spoken to. |
| E | Male | 13 years and 10 months | 25.4 | Very low birth weight, Cerebral palsy, Whooping cough, respiratory arrest, Bronchitis, Hip dislocation | V | No clear response when spoken to. Smiles when comfortable and sticks tongue out when uncomfortable. |
| F | Male | 15 years and 5 months | 32.4 | Cerebral palsy, Lennox–Gastaut syndrome | V | No clear response when spoken to. |
| G | Male | 17 years and 10 months | 42.0 | Ultralow birth weight, Epilepsy, Bronchopneumonia | V | Capable of simple expressions of intention, such as yes/no, by vocalizing “ahh.” Smiles when comfortable and distorts face when uncomfortable. |
| H | Male | 18 years and 2 months | 39.5 | Cerebral palsy | V | Capable of simple expressions of intent, such as yes/no, through the slight movement of neck and nodding. Smiles when comfortable and distorts face when uncomfortable. |
| I | Male | 8 years and 7 months | 19.8 | Lennox–Gastaut syndrome, Delayed motor development, Hip dislocation | V | No clear response when spoken to. |
| J | Male | 8 years and 9 months | 14.0 | MCT8 deficiency, Hip dislocation | V | No clear response when spoken to. Smiles when comfortable and cries when uncomfortable. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozaki, M.; Murata, J.; Sato, K.; Tanaka, G.; Imamura, A.; Iwanaga, R. Effect of the Sway Bed on Autonomic Response, Emotional Responses, and Muscle Hardness in Children with Severe Motor and Intellectual Disabilities: A Pilot Study. Healthcare 2022, 10, 2337. https://doi.org/10.3390/healthcare10112337
Ozaki M, Murata J, Sato K, Tanaka G, Imamura A, Iwanaga R. Effect of the Sway Bed on Autonomic Response, Emotional Responses, and Muscle Hardness in Children with Severe Motor and Intellectual Disabilities: A Pilot Study. Healthcare. 2022; 10(11):2337. https://doi.org/10.3390/healthcare10112337
Chicago/Turabian StyleOzaki, Mitsuki, Jun Murata, Katsuya Sato, Goro Tanaka, Akira Imamura, and Ryoichiro Iwanaga. 2022. "Effect of the Sway Bed on Autonomic Response, Emotional Responses, and Muscle Hardness in Children with Severe Motor and Intellectual Disabilities: A Pilot Study" Healthcare 10, no. 11: 2337. https://doi.org/10.3390/healthcare10112337