
Stroke-Related Sarcopenia among Two Different Developing Countries with Diverse Ethnic Backgrounds (Cross-National Study in Egypt and China)
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Respondent
2.3. Method
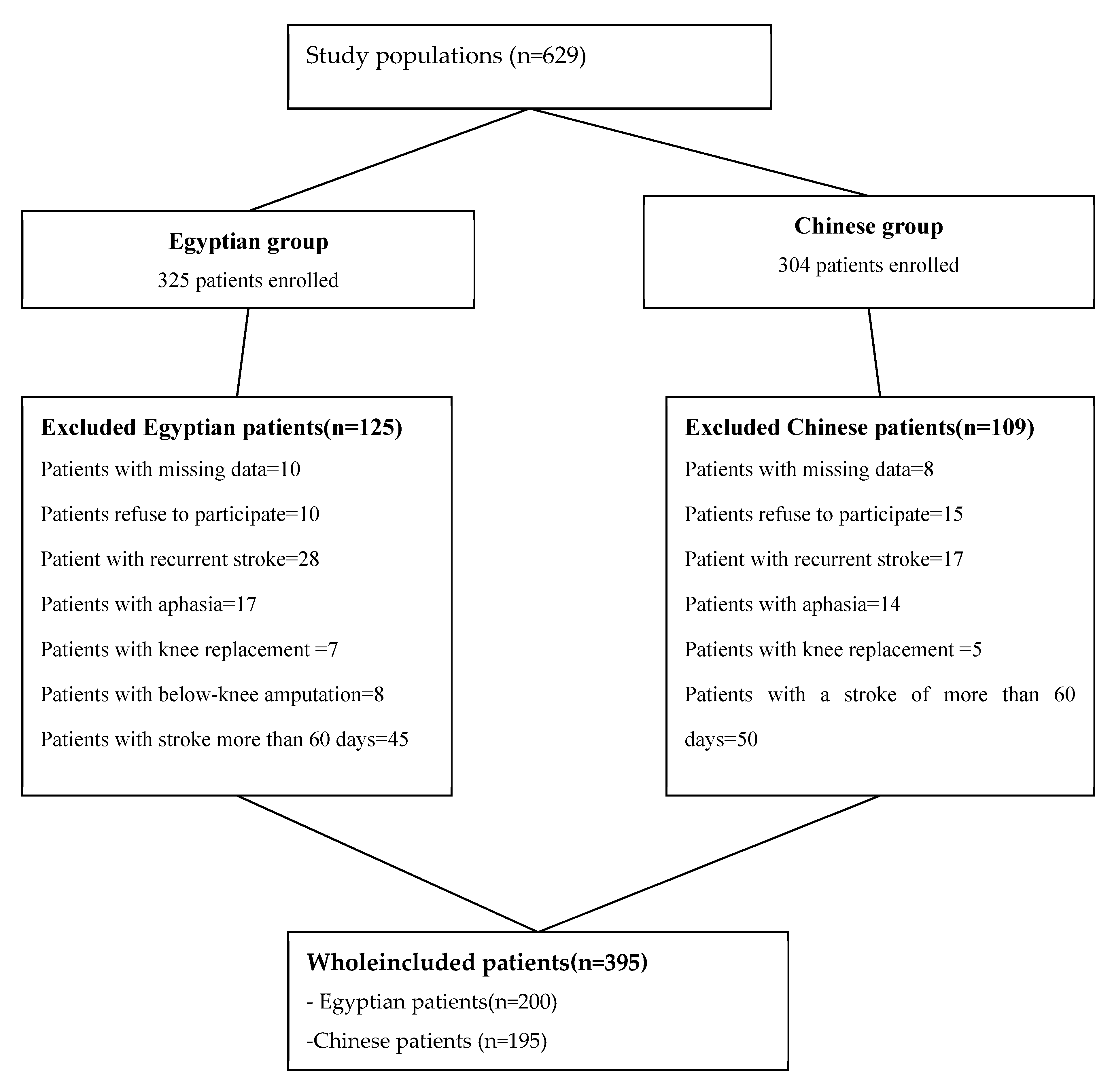
2.4. Inclusion and Exclusion Criteria of the Study Populations
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
2.4.3. Sample Size Calculation
2.5. The Recruiting Criteria
2.5.1. Measurements of the Study Populations
Definition
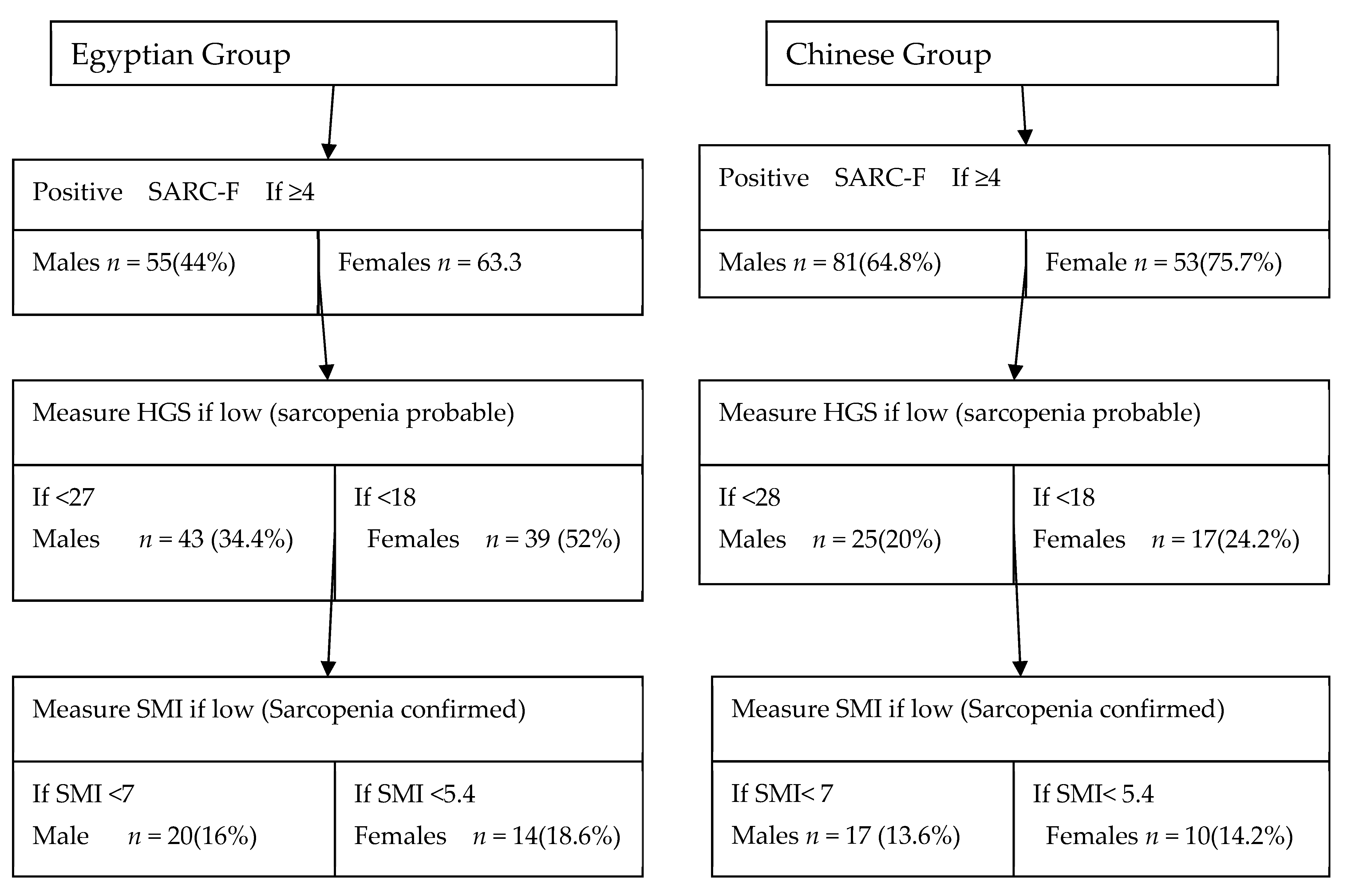
2.5.2. Case Finding (Screening for Sarcopenia)
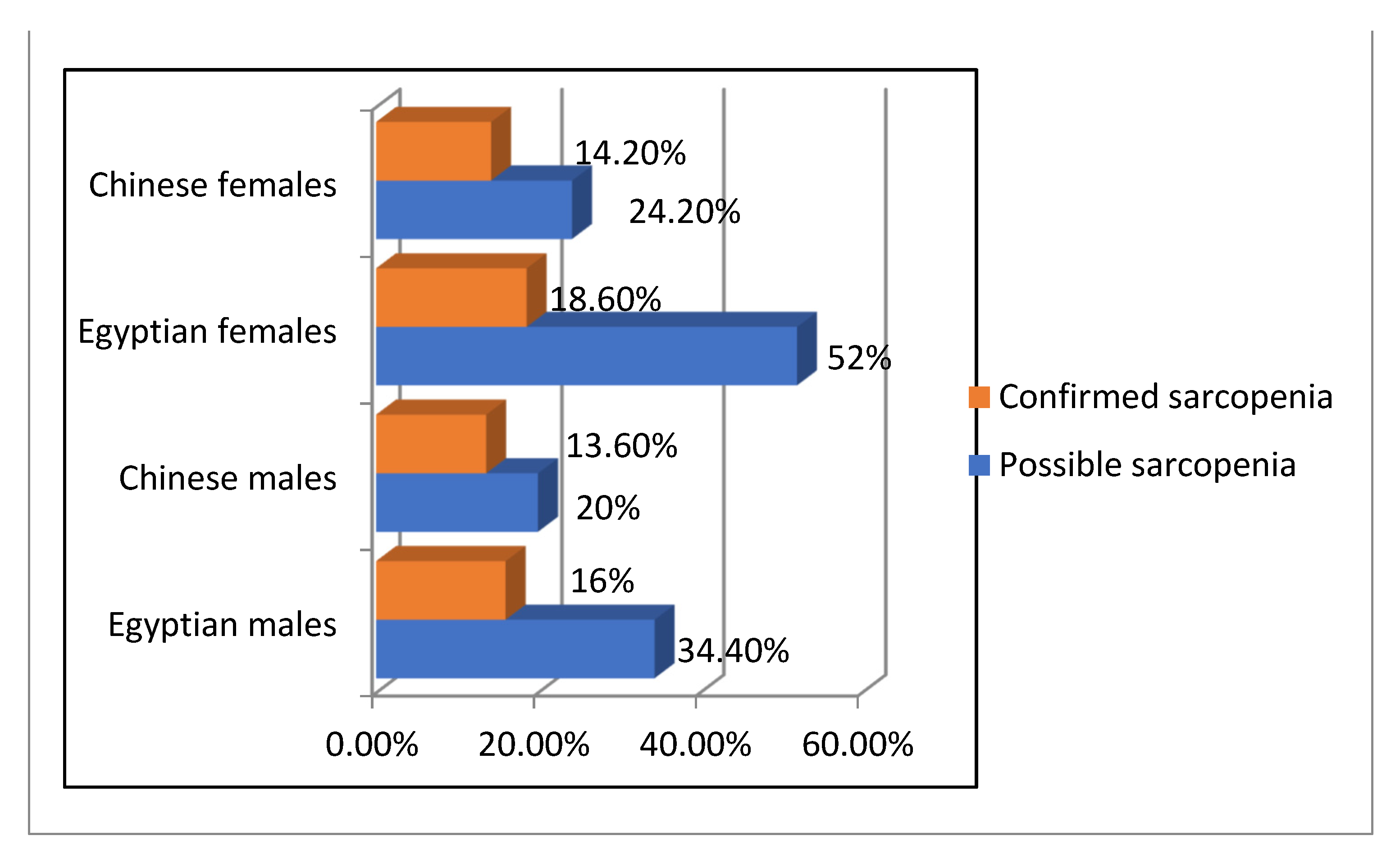
2.5.3. Muscle Strength Assessment (Possible Sarcopenia)
2.5.4. Muscle Mass Assessment for Confirmed Sarcopenia
2.6. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Ryan, A.S.; Buscemi, A.; Forrester, L.; Hafer-Macko, C.E.; Ivey, F.M. Atrophy and Intramuscular Fat in Specific Muscles of the Thigh. Neurorehabilit. Neural Repair 2011, 25, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Lazoura, O.; Papadaki, P.J.; Antoniadou, E.; Groumas, N.; Papadimitriou, A.; Thriskos, P.; Fezoulidis, I.V.; Vlychou, M. Skeletal and Body Composition Changes in Hemiplegic Patients. J. Clin. Densitom. 2010, 13, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, N.; Doehner, W. Sarcopenia in stroke-facts and numbers on muscle loss accounting for disability after stroke. J. Cachex Sarcopenia Muscle 2011, 2, 5–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.G.; Lee, K.W.; Kim, S.B.; Lee, J.H.; Kim, Y.H. Effect of Decreased Skeletal Muscle Index and Hand Grip Strength on Functional Recovery in Subacute Ambulatory Stroke Patients. Ann. Rehabilitation Med. 2019, 43, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Antunes, A.C.; Araújo, D.A.; Veríssimo, M.T.; Amaral, T.F. Sarcopenia and hospitalisation costs in older adults: A cross-sectional study. Nutr. Diet. 2016, 74, 46–50. [Google Scholar] [CrossRef]
- Dent, E.; Morley, J.E.; Cruz-Jentoft, A.J.; Arai, H.; Kritchevsky, S.B.; Guralnik, J.; Bauer, J.M.; Pahor, M.; Clark, B.C.; Cesari, M.; et al. International Clinical Practice Guidelines for Sarcopenia (ICFSR): Screening, Diagnosis and Management. J. Nutr. Health Aging 2018, 22, 1148–1161. [Google Scholar] [CrossRef]
- Ryan, A.S.; Ivey, F.M.; Serra, M.C.; Hartstein, J.; Hafer-Macko, C.E. Sarcopenia and Physical Function in Middle-Aged and Older Stroke Survivors. Arch. Phys. Med. Rehabilitation 2016, 98, 495–499. [Google Scholar] [CrossRef] [Green Version]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients: Implications for oral sarcopenia. Clin. Nutr. 2018, 37, 204–207. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Systemic Inflammation in the Recovery Stage of Stroke: Its Association with Sarcopenia and Poor Functional Rehabilitation Outcomes. Prog. Rehabilitation Med. 2018, 3, 20180011. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, T.; Nishioka, S.; Taguchi, S.; Yamanouchi, A. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 1124–1128. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Krishnamurthi, R.V.; Parmar, P.; Norrving, B.; Mensah, G.A.; Bennett, D.A.; Barker-Collo, S.; Moran, A.E.; Sacco, R.L.; Truelsen, T.; et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990–2013: The GBD 2013 Study. Neuroepidemiology 2015, 45, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Romdhane, N.A.; Ben Hamida, M.; Mrabet, A.; Larnaout, A.; Samoud, S.; Ben Hamda, A.; Oueslati, S.; Ben Hamda, M. Prevalence Study of Neurologic Disorders in Kelibia (Tunisia). Neuroepidemiology 1993, 12, 285–299. [Google Scholar] [CrossRef]
- Al-Rajeh, S.; Larbi, E.; Bademosi, O.; Awada, A.; Ismail, H.; Al-Freihi, H.; Al-Ghassab, G. Stroke in a Tertiary Hospital in Saudi Arabia: A Study of 372 Cases. Eur. Neurol. 1991, 31, 251–256. [Google Scholar] [CrossRef]
- Zhang, Q.; Lu, H.; Pan, S.; Lin, Y.; Zhou, K.; Wang, L. 6MWT Performance and its Correlations with VO2 and Handgrip Strength in Home-Dwelling Mid-Aged and Older Chinese. Int. J. Environ. Res. Public Health 2017, 14, 473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, W.; Jiang, B.; Sun, H.; Ru, X.; Sun, D.; Wang, L.; Wang, L.; Jiang, Y.; Li, Y.; Wang, Y.; et al. Prevalence, Incidence, and Mortality of Stroke in China. Circulation 2017, 135, 759–771. [Google Scholar] [CrossRef]
- Khedr, E.M.; Elfetoh, N.A.; Al Attar, G.; Ahmed, M.A.; Ali, A.M.; Hamdy, A.; Kandil, M.R.; Farweez, H. Epidemiological Study and Risk Factors of Stroke in Assiut Governorate, Egypt: Community-Based Study. Neuroepidemiology 2013, 40, 288–294. [Google Scholar] [CrossRef]
- Scherbakov, N.; Sandek, A.; Doehner, W. Stroke-Related Sarcopenia: Specific Characteristics. J. Am. Med. Dir. Assoc. 2015, 16, 272–276. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Anker, S.D.; Argiles, J.; Aversa, Z.; Bauer, J.M.; Biolo, G.; Boirie, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar] [CrossRef]
- Chen, L.-K.; Liu, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Bahyah, K.S.; Chou, M.-Y.; Chen, L.-Y.; Hsu, P.-S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; van Schoor, N.M.; Lips, P.; Visser, M. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. Ser. A 2018, 73, 1199–1204. [Google Scholar] [CrossRef]
- Ibrahim, K.; May, C.; Patel, H.P.; Baxter, M.; Sayer, A.A.; Roberts, H. A feasibility study of implementing grip strength measurement into routine hospital practice (GRImP): Study protocol. Pilot Feasibility Stud. 2016, 2, 27. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; Koster, A.; Visser, M. Adiposity, Muscle Mass, and Muscle Strength in Relation to Functional Decline in Older Persons. Epidemiologic Rev. 2012, 35, 51–65. [Google Scholar] [CrossRef] [Green Version]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.H.; Rosengren, A.; Kelishadi, R.; et al. Prognostic value of grip strength: Findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Miller, J.; Wells, L.; Nwulu, U.; Currow, D.; Johnson, M.J.; Skipworth, E.R.J. Validated screening tools for the assessment of cachexia, sarcopenia, and malnutrition: A systematic review. Am. J. Clin. Nutr. 2018, 108, 1196–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahat, G.; Yilmaz, O.; Kilic, C.; Oren, M.; Karan, M. Performance of SARC-F Turkish in regard to sarcopenia definitions, muscle mass and functional measures. Clin. Nutr. 2018, 37, S181. [Google Scholar] [CrossRef]
- Beaudart, C.; Locquet, M.; Bornheim, S.; Reginster, J.-Y.; Bruyère, O. French translation and validation of the sarcopenia screening tool SARC-F. Eur. Geriatr. Med. 2017, 9, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Coldham, F.; Lewis, J.; Lee, H. The Reliability of One vs. Three Grip Trials in Symptomatic and Asymptomatic Subjects. J. Hand Ther. 2006, 19, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Thornton, J.C.; Kolesnik, S.; Pierson, R.N. Anthropometry in Body Composition: An Overview. Ann. New York Acad. Sci. 2006, 904, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.P.; Gonzalez, M.C.; Orlandi, S.P.; Bielemann, R.M.; Barbosa-Silva, T.G.; Heymsfield, S.B. COCONUT Study Group New Prediction Equations to Estimate Appendicular Skeletal Muscle Mass Using Calf Circumference: Results From NHANES 1999–2006. J. Parenter. Enter. Nutr. 2019, 43, 998–1007. [Google Scholar] [CrossRef]
- Naderi, M.; Sabour, S. New Prediction Equations to Estimate Appendicular Skeletal Muscle Mass Using Calf Circumference on NHANES Data: Methodological Issues. J. Parenter. Enter. Nutr. 2019, 43, 956–957. [Google Scholar] [CrossRef]
- Aydin, T.; Kesiktaş, F.N.; Oren, M.M.; Erdogan, T.; Ahisha, Y.C.; Kizilkurt, T.; Corum, M.; Karacan, I.; Öztürk, S.; Bahat, G. Sarcopenia in patients following stroke: An overlooked problem. Int. J. Rehabilitation Res. 2021, 44, 269–275. [Google Scholar] [CrossRef]
- Edwards, R.H.T.; Young, A.; Hosking, G.P.; Jones, D.A. Human Skeletal Muscle Function: Description of Tests and Normal Values. Clin. Sci. 1977, 52, 283–290. [Google Scholar] [CrossRef]
- Suetta, C.; Andersen, J.L.; Dalgas, U.; Berget, J.; Koskinen, S.; Aagaard, P.; Magnusson, S.P.; Kjaer, M. Resistance training induces qualitative changes in muscle morphology, muscle architecture, and muscle function in elderly postoperative patients. J. Appl. Physiol. 2008, 105, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Ho, S.C.; Donnan, S.P.B.; Swaminathan, R. Nutritional status of healthy, active, Chinese elderly. Br. J. Nutr. 1988, 60, 21–28. [Google Scholar] [CrossRef]
- Kawakami, R.; Murakami, H.; Sanada, K.; Tanaka, N.; Sawada, S.S.; Tabata, I.; Higuchi, M.; Miyachi, M. Calf circumference as a surrogate marker of muscle mass for diagnosing sarcopenia in Japanese men and women. Geriatr. Gerontol. Int. 2014, 15, 969–976. [Google Scholar] [CrossRef]
- Martin, J.; Ramsay, J.; Hughes, C.; Peters, D.; Edwards, M. Age and Grip Strength Predict Hand Dexterity in Adults. PLoS ONE 2015, 10, e0117598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, P.; Han, Y.; Pang, J.; Wu, S.; Gong, H.; Zhu, J.; Li, J.; Zhang, T. Sarcopenia-related features and factors associated with lower muscle strength and physical performance in older Chinese: A cross sectional study. BMC Geriatr. 2016, 16, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Li, X.; Xu, M.; Zhang, Z.; He, L.; Li, Y. Sarcopenia prevalence and associated factors among older Chinese population: Findings from the China Health and Retirement Longitudinal Study. PLoS ONE 2021, 16, e0247617. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, E.; Sieber, C.C.; Pfeifer, K. Physical activity, exercise, and sarcopenia—Future challenges. Wien. Med. Wochenschr. 2011, 161, 416–425. [Google Scholar] [CrossRef]
- Kim, B.M.; Yi, Y.H.; Kim, Y.J.; Lee, S.Y.; Lee, J.G.; Cho, Y.H.; Tak, Y.J.; Hwang, H.R.; Lee, S.H.; Park, E.J.; et al. Association between Relative Handgrip Strength and Dyslipidemia in Korean Adults: Findings of the 2014–2015 Korea National Health and Nutrition Examination Survey. Korean J. Fam. Med. 2020, 41, 404–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawman, H.G.; Troiano, R.P.; Perna, F.M.; Wang, C.-Y.; Fryar, C.D.; Ogden, C.L. Associations of Relative Handgrip Strength and Cardiovascular Disease Biomarkers in U.S. Adults, 2011–2012. Am. J. Prev. Med. 2015, 50, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Guo, G.; Xia, L.; Yang, X.; Zhang, B.; Liu, F.; Ma, J.; Hu, Z.; Li, Y.; Li, W.; et al. Relative Handgrip Strength Is Inversely Associated with Metabolic Profile and Metabolic Disease in the General Population in China. Front. Physiol. 2018, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [Green Version]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63 Pt B, 2889–2934. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W. Hand-Grip Dynamometry Predicts Future Outcomes in Aging Adults. J. Geriatr. Phys. Ther. 2008, 31, 3–10. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovasculardisease: 2007 update. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blakeley, C.E.; Van Rompay, M.I.; Schultz, N.S.; Sacheck, J.M. Relationship between muscle strength and dyslipidemia, serum 25(OH)D, and weight status among diverse schoolchildren: A cross-sectional analysis. BMC Pediatr. 2018, 18, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Ichinosawa, Y.; Maekawa, E.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; et al. Sarcopenia: Prevalence and Prognostic Implications in Elderly Patients with Cardiovascular Disease. JCSM Clin. Rep. 2017, 2, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Trierweiler, H.; Kisielewicz, G.; Jonasson, T.H.; Petterle, R.R.; Moreira, C.A.; Borba, V.Z.C. Sarcopenia: A chronic complication of type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2018, 10, 25. [Google Scholar] [CrossRef]
- Park, S.W.; Goodpaster, B.H.; Strotmeyer, E.S.; Kuller, L.H.; Broudeau, R.; Kammerer, C.; de Rekeneire, N.; Harris, T.B.; Schwartz, A.V.; Tylavsky, F.A.; et al. Accelerated Loss of Skeletal Muscle Strength in Older Adults with Type 2 Diabetes. Diabetes Care 2007, 30, 1507–1512. [Google Scholar] [CrossRef] [Green Version]
- Scherbakov, N.; von Haehling, S.; Anker, S.D.; Dirnagl, U.; Doehner, W. Stroke induced Sarcopenia: Muscle wasting and disability after stroke. Int. J. Cardiol. 2013, 170, 89–94. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef]
- Jørgensen, L.; Jacobsen, B. Changes in muscle mass, fat mass, and bone mineral content in the legs after stroke: A 1 year prospective study. Bone 2001, 28, 655–659. [Google Scholar] [CrossRef]
- Stenholm, S.; Tiainen, K.; Rantanen, T.; Sainio, P.; Heliövaara, M.; Impivaara, O.; Koskinen, S. Long-Term Determinants of Muscle Strength Decline: Prospective Evidence from the 22-Year Mini-Finland Follow-Up Survey. J. Am. Geriatr. Soc. 2011, 60, 77–85. [Google Scholar] [CrossRef]
- Rinaldi, M.; Maes, K.; De Vleeschauwer, S.; Thomas, D.; Verbeken, E.K.; Decramer, M.; Janssens, W.; Gayan-Ramirez, G.N. Long-term nose-only cigarette smoke exposure induces emphysema and mild skeletal muscle dysfunction in mice. Dis. Model. Mech. 2012, 5, 333–341. [Google Scholar] [CrossRef]
- Szulc, P.; Duboeuf, F.; Marchand, F.; Delmas, P.D. Hormonal and lifestyle determinants of appendicular skeletal muscle mass in men: The MINOS study. Am. J. Clin. Nutr. 2004, 80, 496–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffl, M.; Bohannon, R.W.; Petr, M.; Kohlikova, E.; Holmerova, I. Relation Between Cigarette Smoking and Sarcopenia: Meta-Analysis. Physiol. Res. 2015, 64, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Klesges, R.C.; Eck, L.H.; Isbell, T.R.; Fulliton, W.; Hanson, C.L. Smoking status: Effects on the dietary intake, physical activity, and body fat of adult men. Am. J. Clin. Nutr. 1990, 51, 784–789. [Google Scholar] [CrossRef] [Green Version]
- Castillo, E.M.; Goodman-Gruen, D.; Kritz-Silverstein, D.; Morton, D.J.; Wingard, D.L.; Barrett-Connor, E. Sarcopenia in elderly men and women: The Rancho Bernardo study. Am. J. Prev. Med. 2003, 25, 226–231. [Google Scholar] [CrossRef]
- Nozoe, M.; Kanai, M.; Kubo, H.; Yamamoto, M.; Shimada, S.; Mase, K. Prestroke sarcopenia and functional outcomes in elderly patients who have had an acute stroke: A prospective cohort study. Nutrition 2019, 66, 44–47. [Google Scholar] [CrossRef]
- Kleppinger, A.; Litt, M.D.; Kenny, A.M.; Oncken, C.A. Effects of Smoking Cessation on Body Composition in Postmenopausal Women. J. Women’s Health 2010, 19, 1651–1657. [Google Scholar] [CrossRef] [Green Version]
- Senior, H.E.; Henwood, T.R.; Beller, E.M.; Mitchell, G.K.; Keogh, J.W. Prevalence and risk factors of sarcopenia among adults living in nursing homes. Maturitas 2015, 82, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Mensah, G.A.; Norrving, B.; Murray, C.J.L.; Roth, G.A. GBD 2013 Stroke Panel Experts Group Atlas of the Global Burden of Stroke (1990-2013): The GBD 2013 Study. Neuroepidemiology 2015, 45, 230–236. [Google Scholar] [CrossRef]
- Cadore, E.L.; Izquierdo, M. New Strategies for the Concurrent Strength-, Power-, and Endurance-Training Prescription in Elderly Individuals. J. Am. Med. Dir. Assoc. 2013, 14, 623–624. [Google Scholar] [CrossRef]
- Doehner, W.; Schenkel, J.; Anker, S.D.; Springer, J.; Audebert, H.J. Overweight and obesity are associated with improved survival, functional outcome, and stroke recurrence after acute stroke or transient ischaemic attack: Observations from the TEMPiS trial. Eur. Hear. J. 2012, 34, 268–277. [Google Scholar] [CrossRef]
- Towfighi, A.; Ovbiagele, B. The Impact of Body Mass Index on Mortality After Stroke. Stroke 2009, 40, 2704–2708. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.P.; Wong, A.A.; Schluter, P.J.; Henderson, R.D.; O’Sullivan, J.D.; Read, S.J. Impact of Premorbid Undernutrition on Outcome in Stroke Patients. Stroke 2004, 35, 1930–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakabayashi, H. Seamless community coordination of rehabilitation nutrition care management in patients with Dysphagia. Gan Kagaku Ryoho. 2010, 37 (Suppl. S2), 198–200. (In Japanese) [Google Scholar]
- Yoshimura, Y.; Bise, T.; Shimazu, S.; Tanoue, M.; Tomioka, Y.; Araki, M.; Nishino, T.; Kuzuhara, A.; Takatsuki, F. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: A randomized controlled trial. Nutrition 2018, 58, 1–6. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Stroke Survivors in EgyptianPatients | Stroke Survivors in Chinese Patients | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total, n (%) | Without Sarcopenic | With Sarcopenic | p-Value | Total | Without Sarcopenic | With Sarcopenic | p-Value | ||
| Gender | 200 | 195 | |||||||
| Males | 125(62.50) | 99 | 26 | 125(64.10) | 98 | 27 | |||
| Females | 75(37.50) | 70(35.90) | |||||||
| Age mean ± SD | 55.54 ± 13.1 | 51.6 ± 11.11 | 67.1 ± 7.30 | 0.000 c | 52.8 ± 15.15 | 53.09 ± 15.07 | 53.40 ± 15.25 | 0.925 c | |
| Stroke type, n (%) | |||||||||
| Ischemic | 121(60.50) | 56(56.60) | 18(69.20) | 0.242 a | 84(43.10) | 42(42.9) | 15(55.6) | 0.241 a | |
| Hemorrhagic | 79(39.50) | 43(43.40) | 8(30.80) | 111(56.9) | 56(57.1) | 12(44.4) | |||
| Affected side, n (%) | |||||||||
| Right side Left side | 102(51) 98(49) | 42(42.40) 57(57.60) | 18(69.20) 8(30.80) | 0.015 a | 66(32.80) 129(66.20) | 39(39.80) 59(60.20) | 9(33.30) 18(66.70) | 0.541 a | |
| Smoking n (%) | |||||||||
| No | 110(55) | 27(27.30) | 9(34.60) | 0.462 a | 120(61.50) | 48(49) | 20(70.4) | 0.020 a | |
| Yes | 90(45) | 72(72.70) | 17(65.40) | 75(38.50) | 50(51) | 7(25.9) | |||
| Drinking history, n (%) | |||||||||
| No | 200(100%) | 99(100) | 26(100) | ------ | 99(50.70) | 35(35.70) | 13(48.1) | 0.240 a | |
| Yes | 0(0.0) | 0(0.0) | 0(0.0) | 96(49.20) | 63(64.30) | 14(51.90) | |||
| HTN, n (%) | |||||||||
| No | 29(14.50) | 17(17.20) | 0(0.0) | 0.023 a | 49(24.70) | 20(20.40) | 5(18.50) | 0845 a | |
| Yes | 171(85.5%) | 82(82.8%) | 26(100) | 146(73.7%) | 78(79.20) | 22(81.5) | |||
| DM, n (%) | |||||||||
| No | 118(59) | 67(67.70) | 12(50) | 0.095 a | 24(12.30) | 13(13.30) | 3(11.10) | 0.767 a | |
| Yes | 82(41) | 32(32.30) | 12(50) | 171(87.70) | 85(86.70) | 24(88.90) | |||
| IHD, n (%) | |||||||||
| No | 142(71) | 81(81.80) | 12(46.20) | 0.000 a | 165(84.60) | 79(80.60) | 22(81.50) | 0.919 a | |
| Yes | 58(29) | 18(18.20) | 14(53.80) | 30(15.40) | 19(19.40) | 5(18.50) | |||
| Performed conventional rehabilitation in the early phase, n (%) | |||||||||
| No | 116(58) | 53(53.50) | 15(57.70) | 0.705 a | 65(33.30) | 35(35.70) | 14(51.90) | 0.128 a | |
| Yes | 84(42) | 46(46.50) | 11(42.30) | 130(66.70) | 63(64.30) | 13(48.10) | |||
| Dyslipidemia | |||||||||
| No | 140(70) | 76(76.80) | 12(46.2) | 0.002 a | 72(36.90) | 66(67.0) | 11(40.70) | 0.012 a | |
| Yes | 60(30) | 23(23.20) | 14(53.8) | 123(63.10) | 32(32.70) | 16(59.0) | |||
| Mini Nutritional Assessment-Short Form(MNA-SF) | |||||||||
| Malnutrition | 59(29.50) | 12(12.10) | 17(65.40) | 0.000 a | 65(33.30) | 24(24.50) | 10(37) | 0.297 a | |
| Risky | 59(29.50) | 33(32.30) | 4(19.20) | 45(23.07) | 22(22.40) | 7(25.9) | |||
| Normal | 82(41.0) | 55(55.60) | 4(15.40) | 85(43.50) | 52(53.10) | 10(37) | |||
| FIM motor, median, IQR | |||||||||
| FIM motor | 48(45–72) | 46(56–75) | 38(41–59) | 0.000 b | 55(40–66) | 52(48–70) | 52(40–65) | 0.040 b | |
| FIM cognitive | 31(28–33) | 32(30–34) | 24(23–29) | 0.000 b | 31(29–33) | 31(30–33) | 20(28–33) | 0.207 b | |
| FIM total | 81(72–105) | 98(87–108) | 51(65–89) | 0.000 b | 62(69–100) | 61(77–101) | 60(67–96) | 0.037 b | |
| Modified Rankin scale | 2(1–4) | 2(1–3) | 4(2–5) | 0.000 b | 4(3–4) | 4(3–4) | 4(3–4) | 0.288 b | |
| Time from stroke onset per month, median, IQR | 57(34–43) | 47(36–44) | 35(35–43) | 0.400 b | 49(35–44) | 36(36–45) | 30(38–46) | 0.153 b | |
| Weight/kg mean ± SD | 71.62 ± 11.0 | 77.01 ± 8.50 | 63.9 ± 8.70 | 0.000 c | 69.9 ± 12.12 | 74.88 ± 10.10 | 76.92 ± 11.07 | 0.365 c | |
| Height/m | 167.60 ± 8.1 | 172.03 ± 5.38 | 171.79 ± 5.60 | 0.779 c | 170.0 ± 7.26 | 173.76 ± 3.7 | 176.4 ± 2.6 | 0.001 c | |
| BMI (kg/m2) | 25.3 ± 4.20 | 26.33 ± 3.30 | 21.01 ± 2.80 | 0.000 c | 24.0 ± 3.04 | 24.7 ± 2.9 | 24.3 ± 3.40 | 0.902 c | |
| SMI (kg/m2) | 7.1 ± 1.50 | 8.3 ± 0.822 | 6.2 ± 0.45 | 0.000 c | 7.19 ± 1.24 | 7.9 ± 0.51 | 6.13 ± 0.75 | 0.000 c | |
| HG strength/kg | 23.32 ± 17.7 | 33.9 ± 17.27 | 14.8 ± 13.10 | 0.000 c | 29.2 ± 9.34 | 31.86 ± 8.9 | 28.88 ± 0.02 | 0.129 c | |
| Calf affected | 36.02 ± 4.7 | 37.96 ± 2.90 | 31.23 ± 2.17 | 0.000 c | 35.7 ± 3.40 | 37.84 ± 2.2 | 32.68 ± 4.30 | 0.000 c | |
| Calf unaffected | 36.3 ± 3.9 | 38.21 ± 2.80 | 31.53 ± 2.10 | 0.000 c | 35.56 ± 3.40 | 37.65 ± 1.9 | 31.18 ± 2.98 | 0.000 c | |
| CCI, median IQR | 4(3–5) | 4(3–4) | 5(4–6) | 0.000 b | 4(3–5) | 3(3–5) | 6(3–5) | 0.177 b | |
| SARC-F, median, IQR | 4(0–8) | 2(0–4) | 8(5–10) | 0.000 b | 4(2–8) | 4(2–8) | 8(2–8) | 0.343 b | |
| NIHSS, median, IQR | 5(3–9) | 4(3–6) | 8(6–14) | 0.000 b | 6(4–8) | 6(4–8) | 10(4–9) | 0.961 b | |
| Variables | Stroke Survivors in Egyptian Patients | Stroke Survivors in Chinese Patients | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total, n (%) | Without Sarcopenic | With Sarcopenic | p-Value | Total | Without Sarcopenic | With Sarcopenic | p-Value | ||
| Gender | 200 | 195 | |||||||
| Males | 125(62.50) | 125(64.10) | |||||||
| Females | 75(37.50) | 49 | 26 | 70(35.90) | 60 | 10 | |||
| Age mean ± SD | 55.54 ± 13.1 | 56.5 ± 14.1 | 57.1 ± 15.6 | 0.857 c | 52.8 ± 15.15 | 53.4 ± 15.15 | 45 ± 13.7 | 0.143 c | |
| Modified Rankin median, IQR | 3(1–4) | 4(1–4) | 0.763 b | 4(3–4) | 4(3–4) | 4(3–4) | 0.467 b | ||
| Stroke type, n (%) | |||||||||
| Ischemic | 121(60.50) | 26(53.10) | 21(80.8%) | 0.018 a | 84(43.10) | 25(41.7%) | 8(80%) | 0.193 a | |
| Hemorrhagic | 79(39.50) | 23(46.9) | 5(19.2%) | 111(56.9) | 35(58.3%) | 2(20%) | |||
| Affected side, n (%) | |||||||||
| Right side Left side | 102(51) 98(49) | 20(40.8%) 29(59.2%) | 13(50%) 13(50%) | 0.446 a | 66(32.80) 129(66.20) | 16(26.6%) 44(73.3%) | 2(20%) 8(80%) | 0.438 a | |
| Smoking n (%) | |||||||||
| No | 110(55) | 49(100%) | 25(96.2%) | 0.167 a | 120(61.50) | 45(75%) | 7 (70%) | 0.738 a | |
| Yes | 90(45) | 0(0%) | 1(3.8%) | 75(38.50) | 15(25%) | 3(30%) | |||
| Drinking history, n (%) | |||||||||
| No | 200(100%) | 46(100%) | 29(100%) | ------ | 99(50.70) | 45(75%) | 4(60%) | 0.323 a | |
| Yes | 0(0.0) | 0(0.0) | 0(0%) | 96(49.20) | 15(25%) | 6(40%) | |||
| HTN, n (%) | |||||||||
| No | 29(14.50) | 9(18.4%) | 3(11.5%) | 0.443 a | 49(24.70) | 7(11.7%) | 1(10%) | 0.785 a | |
| Yes | 171(85.5%) | 40(81.6%) | 23(88.5%) | 146(73.7%) | 53(88.7%) | 9(90%) | |||
| DM, n (%) | |||||||||
| No | 118(59) | 25(51%) | 13(50%) | 0.933 a | 24(12.30) | 21(35%) | 3(30%) | 0.878 a | |
| Yes | 82(41) | 24(49%) | 13(50%) | 171(87.70) | 39(65%) | 7(70%) | |||
| IHD, n (%) | |||||||||
| No | 142(71) | 33(67.3%) | 16(61.5%) | 0.615 a | 165(84.60) | 55(91.7%) | 90(90%) | 0.862 a | |
| Yes | 58(29) | 16(32.7%) | 10(38.5%) | 30(15.40) | 5(8.6%) | 1(10%) | |||
| Performed conventional rehabilitation in the early phase, n (%) | |||||||||
| No | 116(58) | 30(61.2%) | 18(69.2%) | 0.492 a | 65(33.30) | 15(25%) | 8(80%) | 0.001 a | |
| Yes | 84(42) | 19(38.8%) | 8(30.8%) | 130(66.70) | 45(75%) | 2(20%) | |||
| Dyslipidemia | |||||||||
| NO | 140(70) | 35(71.4%) | 17(65.4%) | 0.589 a | 72(36.90) | 37(63.8%) | 9(75%) | 0.064 a | |
| Yes | 60(30) | 14(28.6%) | 10(34.6%) | 123(63.10) | 21(36.2%) | 3(25%) | |||
| Mini Nutritional Assessment-Short Form(MNA-SF) | |||||||||
| Malnutrition | 59(29.50) | 18(36.7%) | 13(46.2%) | 0.727 a | 65(33.30) | 23(38.3%) | 8(80%) | 0.027 a | |
| Risky | 59(29.50) | 15(30.6%) | 7(26.9%) | 45(23.07) | 14(23.3%) | 2(20%) | |||
| Normal | 82(41.0) | 15(32.7%) | 7(26.9%) | 85(43.50) | 23(38.3%) | 0 | |||
| FIM, median, IQR | |||||||||
| FIM motor | 48(45–72) | 60(41–71) | 42(42–71) | 0.683 b | 55(40–66) | 55(39–70) | 40(40–60) | 0.620 b | |
| FIM cognitive, | 31(28–33) | 31(29–32) | 30(27–34) | 0.884 b | 31(29–33) | 31(28–34) | 28(29–32) | 0.819 b | |
| FIM total | 81(72–105) | 60(71–103) | 78(69–104) | 0.781 b | 62(69–100) | 65(65–105) | 47(70–92) | 0.559 b | |
| Time from stroke onset per month, median, IQR | 57(34–43) | 38(33–42) | 35(34–44) | 0.492 b | 49(35–44) | 43(33–43) | 34(33–37) | 0.485 b | |
| Weight /KG | 71.62 ± 11.0 | 66.5 ± 10.5 | 68.12 ± 12.38 | 0.493 c | 69.9 ± 12.12 | 60.3 ± 9.1 | 59. 8 ± 4.8 | 0.886 c | |
| Height/M | 167.60 ± 8.1 | 159.1 ± 5.9 | 162.5 ± 7.2 | 0.036 c | 170.0 ± 7.26 | 161.7 ± 5.5 | 166.62 ± 3.7 | 0.010 c | |
| BMI (kg/m2) | 25.3 ± 4.20 | 25.4 ± 4.2 | 25.5 ± 5.7 | 0.883 c | 24.0 ± 3.04 | 22.9 ± 2.7 | 21.5 ± 1.9 | 0.123 c | |
| SMI (kg/m2) | 7.1 ± 1.50 | 6.5 ± 0.8 | 4.4 ± 0.56 | 0.000 c | 7.19 ± 1.24 | 6.8 ± 0.78 | 4.6 ± 0.57 | 0.000 c | |
| HG strength /kg | 23.32 ± 17.7 | 12.2 ± 9.1 | 12.2 ± 10.5 | 0.995 c | 29.2 ± 9.34 | 27.3 ± 8.3 | 14.8 ± 0.421 | 0.000 c | |
| Calf affected | 36.02 ± 4.7 | 37.6 ± 3.1 | 30.2 ± 6.5 | 0.000 c | 35.7 ± 3.40 | 34.6 ± 1.5 | 29.7 ± 2.34 | 0.000 c | |
| Calf unaffected | 36.3 ± 3.9 | 37.8 ± 3.1 | 31.4 ± 2.1 | 0.000 c | 35.56 ± 3.40 | 35.2 ± 2.01 | 29.1 ± 2.22 | 0.000 c | |
| CCI, median IQR | 4(3–5) | 4(2–5) | 6(3–6) | 0.069 b | 4(3–5) | 4(3–5) | 5(4–8) | 0.000 b | |
| SARC-F, median, IQR | 4(0–8) | 4(2–8) | 10(3–8) | 0.567 b | 4(2–8) | 4(3–8) | 6(7–8) | 0.000 b | |
| NIHSS, median, IQR | 5(3–9) | 5(4–10) | 10(4–10) | 0.567 b | 6(4–8) | 5(4–7) | 9(8–15) | 0.000 b | |
| Pre-Stroke Variables | Post-Stroke Variables | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Age | Smoking | Drinking | HTN | DM | IHD | Dyslipidemia | Rehabilitation | FIM Motor | FIM Cognitive | MNA-SF | NIHSS |
| HG in Egyptian | −0.405 ** | 0.294 ** | ----- | −0.058 | −0.450 ** | −0.375 ** | −0.363 ** | 0.037 | 0.568 ** | 0.455 ** | 0.624 ** | −0.664 ** |
| HG in Chinese | −0.222 ** | 0.280 ** | 0.229 ** | 0.003 | −0.094 | −0.003 | −0.254 ** | 0.153* | 0.233 ** | 0.173 * | 0.583 ** | −0.173 * |
| SMI in Egyptian | −0.303 ** | 0.458 ** | ---- | −0.110 | −0.173 ** | −0.184 ** | −0.063 | 0.110 | 0.171 * | 0.198 ** | 0.298 ** | −0.268 ** |
| SMI in Chinese | 0.030 | 0.161 * | 0.169 * | 0.053 | −0.015 | 0.087 | −0.148* | 0.022 | 0.111 | 0.046 | 0.215 ** | −0.048 |
| Variables | HGS in Egyptian | HGS In Chineses | SMI in Egyptian | SMI in Chinese |
|---|---|---|---|---|
| ꞵ | ꞵ | ꞵ | ꞵ | |
| -Age Sig CI | −0.250 0.000 (−0.499)–(−0.175) | −0.290 0.000 (−0.258)–(−0.100) | −0.271 0.000 (−0.047)–(−0.018) | |
| -Smoking history Sig CI | 0.303 0.0004 (6.906)–(14.634) | 0.293 0.000 (3.133)–(8.085) | 0.462 0.000 (1.080)–(1.831) | |
| -Drinking History Sig CI | ||||
| -HTN Sig CI | ||||
| -DM Sig CI | −0.198 0.002 (−11.579)–(−2.624) | |||
| -IHD Sig CI | −0.192 0.001 (−12.003)-(−2.940) | |||
| -Dyslipidemia Sig CI | −0.213 0.000 (−12.736)–(−3.698) | −0.225 0.001 (−6.832)–(−1.884) | ||
| -Rehabilitation Sig CI | 0.147 0.032 (0.042)–(0.892) | |||
| -MNA-SF Sig CI | 0.319 0.000 (3.659)–(9.884) | 0.586 0.000 (5.048)–(7.511) | 0.303 0.000 (0.319)–(0.823) | 0.244 0.000 (0.137)–(0.491) |
| -FIM Cognitive | ||||
| FIM Motor | ||||
| -NIHSS Sig CI | −0.408 0.000 (−2.685)–(−1.266) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammed, M.; Li, J. Stroke-Related Sarcopenia among Two Different Developing Countries with Diverse Ethnic Backgrounds (Cross-National Study in Egypt and China). Healthcare 2022, 10, 2336. https://doi.org/10.3390/healthcare10112336
Mohammed M, Li J. Stroke-Related Sarcopenia among Two Different Developing Countries with Diverse Ethnic Backgrounds (Cross-National Study in Egypt and China). Healthcare. 2022; 10(11):2336. https://doi.org/10.3390/healthcare10112336
Chicago/Turabian StyleMohammed, Marwa, and Jianan Li. 2022. "Stroke-Related Sarcopenia among Two Different Developing Countries with Diverse Ethnic Backgrounds (Cross-National Study in Egypt and China)" Healthcare 10, no. 11: 2336. https://doi.org/10.3390/healthcare10112336