
Formative Usability Evaluation of a Three-Way Digital Healthcare System for the People with Disabilities and Their Caregivers: A Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
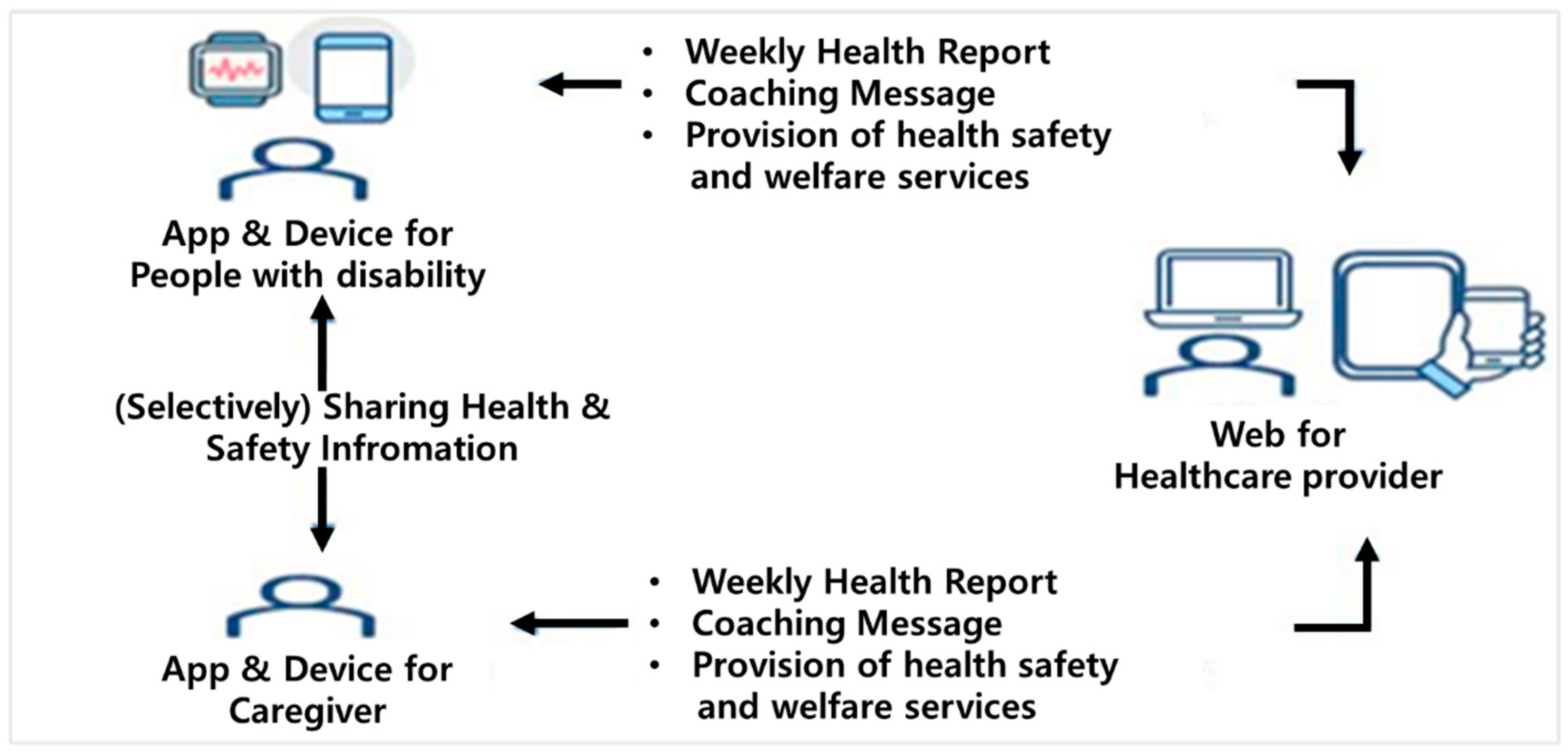
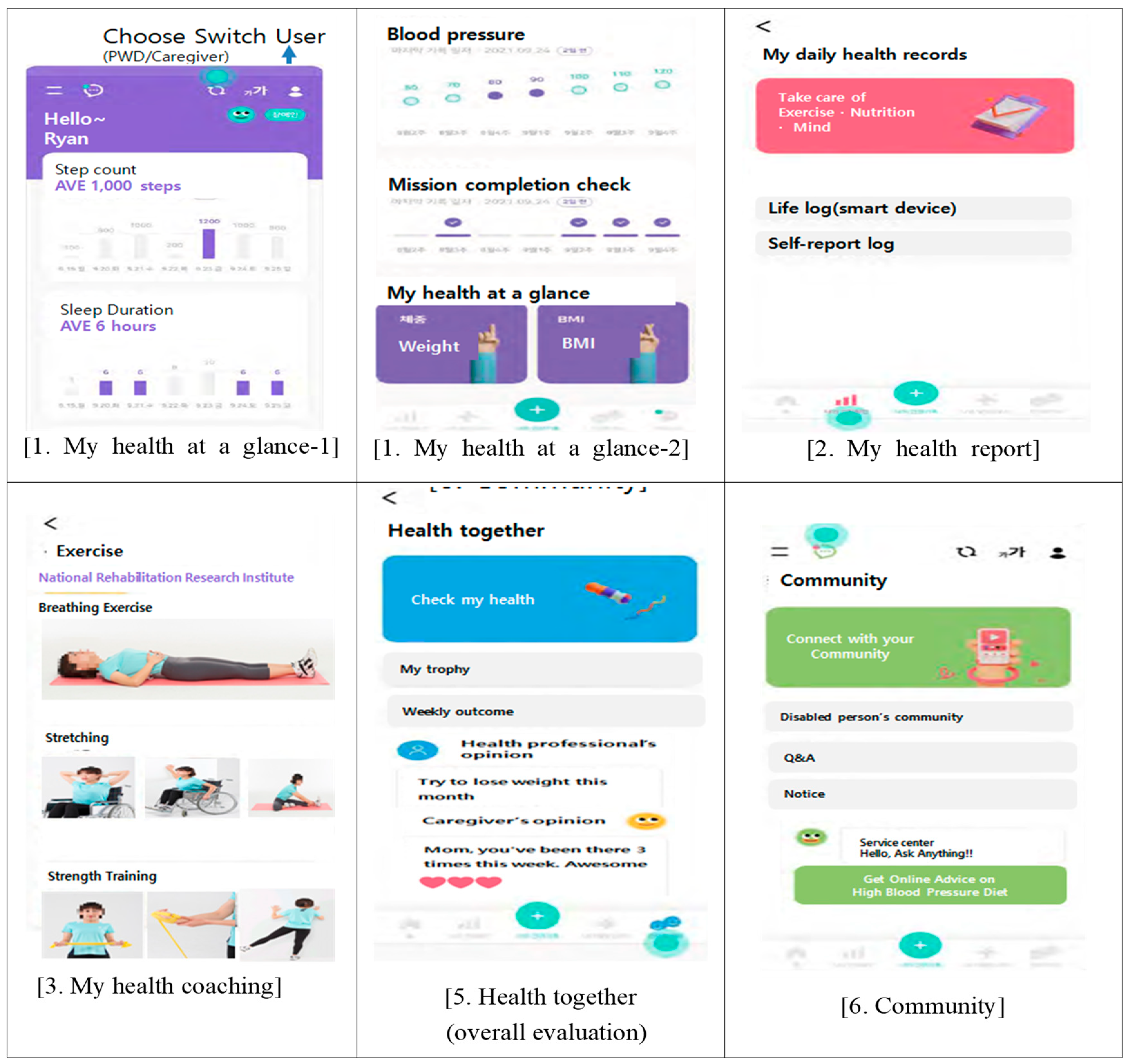
2.2. A Three-Way Digital Healthcare System for the People with Disabilities and Their Caregivers
2.3. Evaluation Instruments
2.4. Satisfaction Evaluation
2.5. Data Analysis
3. Results
3.1. Participants Sociodemographic Characteristics
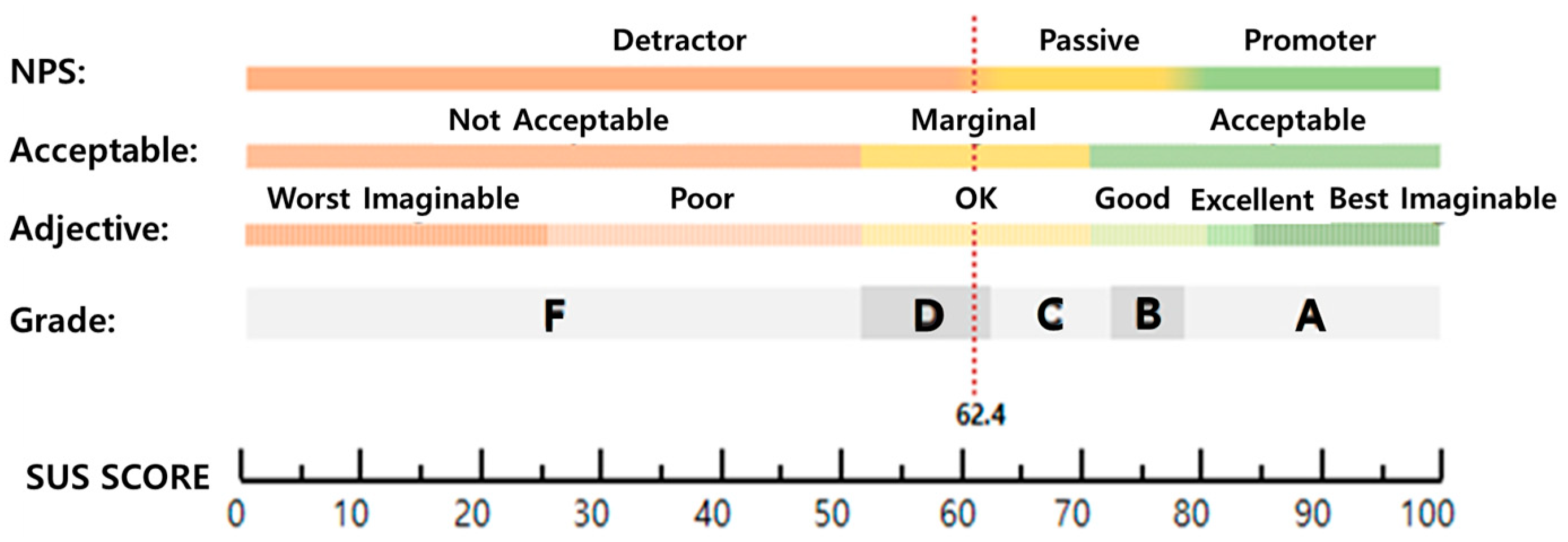
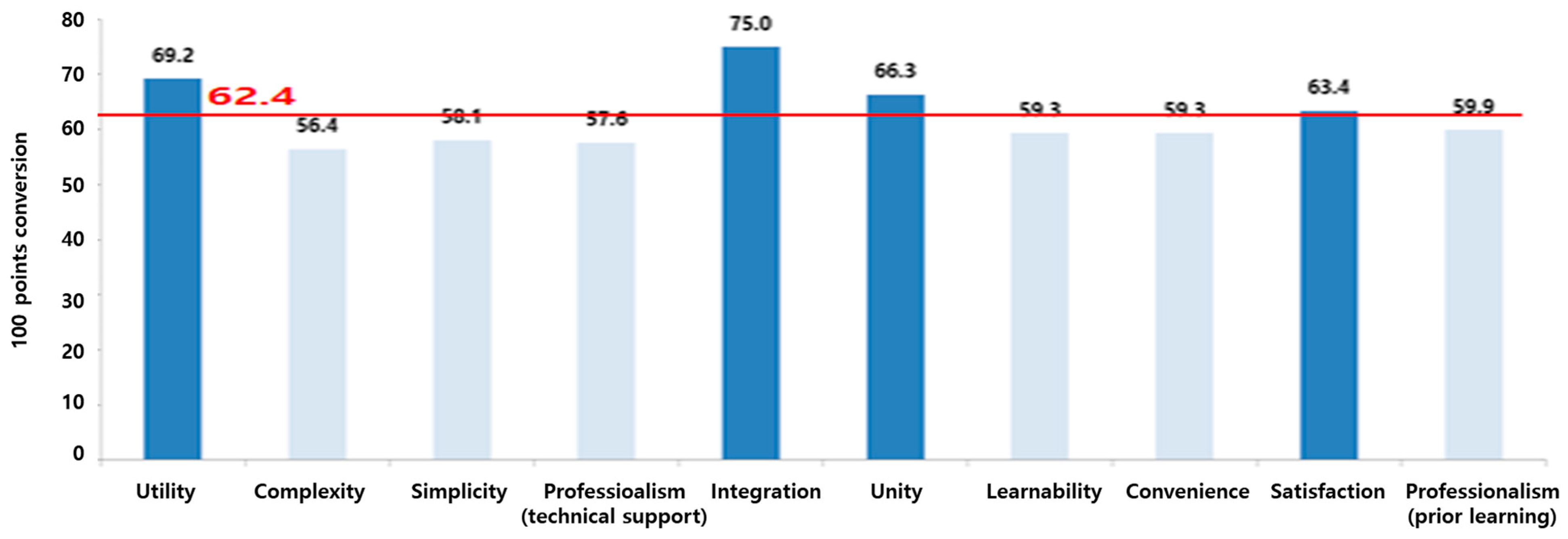
3.2. Usability Scale Rating
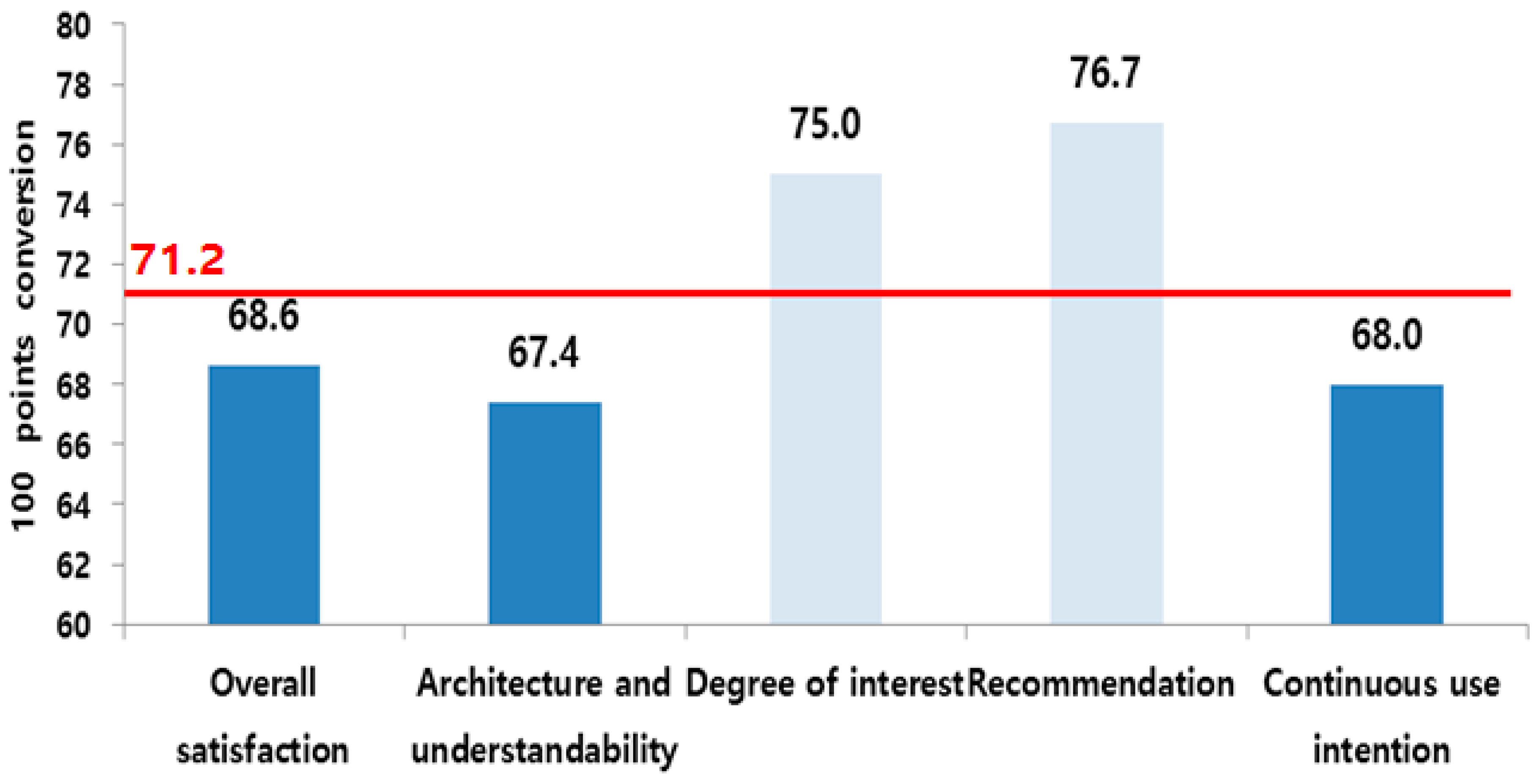
3.3. User Satisfaction Evaluation
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rotarou, E.S.; Sakellariou, D.; Kakoullis, E.J. Disabled people in the time of COVID-19: Identifying needs, promoting inclusivity. J. Glob. Health 2021, 11, 03007. [Google Scholar] [CrossRef] [PubMed]
- Landes, S.D.; Turk, M.A.; Formica, M.K. COVID-19 outcomes among people with intellectual and developmenta disability living in residential group homes in New York State. Disabil. Health J. 2020, 13, 100969. [Google Scholar] [CrossRef] [PubMed]
- Glover, R.E.; van Schalkwyk, M.C.; Akl, E.A. A framework for identifying and mitigating the equity harms of COVID-19 policy interventions. J. Clin. Epidemiol. 2020, 128, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; Lee, Y.; Kim, M. AI·IoT-Based Pilot Project for Elderly Health Management; Korea Health Promotion Institute: Seoul, Republic of Korea, 2020. [Google Scholar]
- Oh, Y.; Im, H.; Kim, D. A Guide for the Community Health Center Mobile Healthcare Project; Korea Health Promotion Institute: Seoul, Republic of Korea, 2021. [Google Scholar]
- Ward, R.E.; Setiawan, I.M.A.; Quinby, E. Mobile Health to Support Community-Integration of Individuals with Disabilities Using iMHere 2.0: Focus Group Study. JMIR Hum. Factors 2022, 9, e31376. [Google Scholar] [CrossRef] [PubMed]
- Hans, P.K.; Gray, C.S.; Gill, A. The provider perspective: Investigating the effect of the Electronic Patient-Reported Outcome (ePRO) mobile application and portal on primary care provider workflow. Prim. Health Care Res. Dev. 2018, 19, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.Y.; Chaar, D.; Kedroske, J. Harnessing mobile health technology to support long-term chronic illness management: Exploring family caregiver support needs in the outpatient setting. JAMIA Open 2020, 3, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Sabo, K.; Chin, E. Self-care needs and practices for the older adult caregiver: An integrative review. Geriatr. Nurs. 2021, 42, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-Y.; Chen, S.-P. Health promotion behaviors in Chinese family caregivers of patients with stroke. Health Promot. Int. 2002, 17, 329–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottle, E.-M.; James, J.E. Role of the family support person during resuscitation. Nurs. Stand. 2008, 23, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.H.; Kim, D.-A.; Bae, Y.-H.; Kim, J.H. Development of Digital Health Care System Based on Online Health and Safety Net for People with Disabilities in the COVID-19 Era; Korea National Rehabilitation Research Institute: Seoul, Republic of Korea, 2021. [Google Scholar]
- Lewis, J.R. Usability: Lessons Learned … and Yet to Be Learned. Int. J. Hum.-Comput. Interact. 2014, 30, 663–684. [Google Scholar] [CrossRef]
- Park, Y.; Kim, D.; Park, S. Development and Usability Test of IoT-based Mobile Applications for Persons with Mild Physical Disabilities and their Caregivers. In Proceedings of the 19th International Conference on Ubiquitous Robots (UR), Jeju, Republic of Korea, 4–6 July 2022; pp. 243–247. [Google Scholar]
- Brooke, J. SUS-A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Sauro, J. 5 Ways to Interpret a SUS Score. Available online: https://measuringucom/interpret-sus-score (accessed on 12 April 2022).
- Bangor, A.; Kortum, P.T.; Miller, J.T. An empirical evaluation of the system usability scale. Int. J. Hum.-Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A retrospective. J. Usability Stud. 2013, 8, 29–40. [Google Scholar]
- Do, Y.-I.; Geum, S.-E.; Lee, S.-U. Exploratory research on factors affecting usability and sustainability of wearable devices for health management. Commun. Korean Inst. Inf. Sci. Eng. 2014, 32, 37–45. [Google Scholar]
- Jeon, S.-H.; Kang, J.-Y.; Lim, J.-I. Analysis of factors affecting intention of continuous use for mobile wallet based on the information system success model. J. Inf. Technol. Serv. 2014, 13, 325–340. [Google Scholar]
- Kang, M.; Kim, Y.-N.; Park, S.-K. The Effect of Application on Smart Phone Repurchase Intention. Cust. Satisf. Manag. Res. 2012, 14, 19–39. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Depth 1 | Depth 2 | Depth 3 |
|---|---|---|
| 1. My health at a glance ((Step count, sleep duration, weight, BMI) *, blood glucose, blood pressure, ten-mission checklist, favorites) | ||
| 2. My profile | Account management | Basic information |
| Information sharing selection * (People with disabilities or their caregiver’s) | ||
| My health checks (People with disabilities, caregiver) | Evaluation date * | |
| Activities of daily living evaluation (MBI) | ||
| Quality of life evaluation (EQ-5D) | ||
| Motor function evaluation (MAS) | ||
| Depression (PHQ-9) * | ||
| Anxiety (GAD-7) * | ||
| Cognitive function index | ||
| Health behavior * (Drinking, smoking, blood pressure, blood glucose level, height, weight, BMI, pain, daily calorie intake, calorie intake check against the recommended level, sodium content, sugar content) | ||
| Medication (compliance, drug type) | ||
| Consultation log (required items check) | ||
| 3. My health | My health coaching | Exercise |
| Nutrition | ||
| Mind * | ||
| My daily health records | Mission setting and notice ((Drinking, smoking, nutrition, exercise, medication, mental health, smart band, smart scale) *, smart blood pressure monitor, smart blood glucose monitor) | |
| Life log ((Smart band, smart scale) *, smart blood pressure monitor, smart blood glucose monitor) | ||
| Self-report log * (Nutrition log, medication log, other required items) | ||
| My routine health checks | Mission completion check* | |
| Life log records check * | ||
| Self-report outcome check * | ||
| 4. My wellbeing assistant | Health information | Disability-related disease management * |
| Chronic disease management * | ||
| Safety and welfare information | Infectious disease crisis response * | |
| Welfare and policy information at a glance * | ||
| Assistive and exercise equipment* | ||
| Disability-friendly healthcare and welfare facilities * | ||
| Mobility and transportation* | ||
| Guide for emergency response* | ||
| Improving disability-related information/awareness * | ||
| Sport facilities* | ||
| 5. Health together (Comparison of records) | My trophy | Frequency of mission completion (Caregiver + disabled person) * |
| Weekly health life evaluation outcome (Weekly Report) | Visualized “My health at a glance” data of people with disabilities (Caregiver’s opinion) * | |
| Visualized “My health at a glance” data of Caregiver (People with disabilities’ opinion) | ||
| 6. Community | People with disabilities community | |
| Caregiver community * | ||
| Questions and answers * | ||
| Items | Statement |
|---|---|
| 1. Utility | I think that I would like to use this system frequently. |
| 2. Complexity | I found the system unnecessarily complex. |
| 3. Simplicity | I thought the system was easy to use. |
| 4. Professionalism (Technician support) | I think that I would need the support of a technical person to be able to use this system. |
| 5. Integration | I found the various functions in the system were well integrated. |
| 6. Unity | I thought there was too much inconsistency in this system. |
| 7. Learnability | I would imagine that most people would learn to use this system very quickly. |
| 8. Convenience | I found the system very cumbersome to use. |
| 9. Satisfaction | I felt very confident using the system. |
| 10. Professionalism (Prior learning) | I needed to learn a lot of things before I could get going with this system. |
| Grade Scale | Range | Percentile Range | Adjective Rating | Acceptance Level | Recommendation |
|---|---|---|---|---|---|
| A+ | 84.1–100 | 96–100 | Best imaginable | Acceptable | Recommendable |
| A | 80.8–84.0 | 90–95 | Excellent | ||
| A− | 78.9–80.7 | 85–89 | |||
| B+ | 77.2–78.8 | 80–84 | Neutral | ||
| B | 74.1–77.1 | 70–79 | |||
| B− | 72.6–74.0 | 65–69 | |||
| C+ | 71.1–72.5 | 60–64 | Good | ||
| C | 65.0–71.0 | 41–59 | Nearly acceptable | ||
| C− | 62.7–64.9 | 35–40 | |||
| D | 51.7–62.6 | 15–34 | Fair | Unrecommendable |
| Category | Frequency (%) | |
|---|---|---|
| Gender | M | 38 (88.4%) |
| F | 5 (11.6%) | |
| Age Group | 30 s | 5 (11.6%) |
| 40 s | 25 (58.1%) | |
| 50 s | 12 (27.9%) | |
| 60 s | 1 (2.3%) | |
| Occupation | Academia | 26 (60.5%) |
| Public health and welfare | 9 (20.9%) | |
| Industry | 8 (18.6%) | |
| Career | <10 years | 7 (16.3%) |
| 10–19 years | 22 (51.2%) | |
| 20–29 years | 10 (23.3%) | |
| 30–39 years | 3 (7.0%) | |
| ≥40 years | 1 (2.3%) |
| Item | Min | Max | M ± SD | Scaled M ± SD |
|---|---|---|---|---|
| Total | - | - | 3.10 ± 0.88 | 62.4 ± 15.7 |
| Utility | 2.00 | 5.00 | 3.77 ± 0.68 | 69.2 ± 17.1 |
| Complexity | 1.00 | 4.00 | 2.74 ± 0.88 | 56.4 ± 21.9 |
| Simplicity | 1.00 | 5.00 | 3.33 ± 0.81 | 58.1 ± 20.2 |
| Professionalism (technician support) | 1.00 | 5.00 | 2.70 ± 1.17 | 57.6 ± 29.1 |
| Integration | 2.00 | 5.00 | 4.00 ± 0.69 | 75.0 ± 17.3 |
| Unity | 1.00 | 4.00 | 2.35 ± 0.69 | 66.3 ± 17.2 |
| Learnability | 1.00 | 5.00 | 3.37 ± 1.05 | 59.3 ± 26.2 |
| Convenience | 1.00 | 4.00 | 2.63 ± 1.02 | 59.3 ± 25.6 |
| Satisfaction | 2.00 | 5.00 | 3.53 ± 0.77 | 63.4 ± 19.2 |
| Professionalism (prior learning) | 1.00 | 5.00 | 2.60 ± 1.00 | 59.9 ± 25.1 |
| Item | Min | Max | M ± SD | Scaled M ± SD |
|---|---|---|---|---|
| Total | - | - | 3.85 ± 0.73 | 71.2 ± 20.7 |
| Overall satisfaction | 2.00 | 5.00 | 3.74 ± 0.76 | 68.6 ± 19.0 |
| Architecture and understandability | 2.00 | 5.00 | 3.70 ± 0.77 | 67.4 ± 19.3 |
| Degree of interest | 3.00 | 5.00 | 4.00 ± 0.69 | 75.0 ± 17.3 |
| Recommendation | 3.00 | 5.00 | 4.07 ± 0.59 | 76.7 ± 14.8 |
| Continuous use intention | 2.00 | 5.00 | 3.72 ± 0.85 | 68.0 ± 21.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Bae, Y.-H.; Kim, S.S.; Lee, M.; Ho, S.H. Formative Usability Evaluation of a Three-Way Digital Healthcare System for the People with Disabilities and Their Caregivers: A Cross-Sectional Study. Healthcare 2022, 10, 2325. https://doi.org/10.3390/healthcare10112325
Kim JH, Bae Y-H, Kim SS, Lee M, Ho SH. Formative Usability Evaluation of a Three-Way Digital Healthcare System for the People with Disabilities and Their Caregivers: A Cross-Sectional Study. Healthcare. 2022; 10(11):2325. https://doi.org/10.3390/healthcare10112325
Chicago/Turabian StyleKim, Ju Hee, Young-Hyeon Bae, Sung Shin Kim, Minyoung Lee, and Seung Hee Ho. 2022. "Formative Usability Evaluation of a Three-Way Digital Healthcare System for the People with Disabilities and Their Caregivers: A Cross-Sectional Study" Healthcare 10, no. 11: 2325. https://doi.org/10.3390/healthcare10112325