
Association between Sleep Duration and Symptoms of Depression Aged between 18 and 49: The Korea National Health and Nutrition Examination Survey (KNHANES Ⅶ) from 2016 to 2018
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
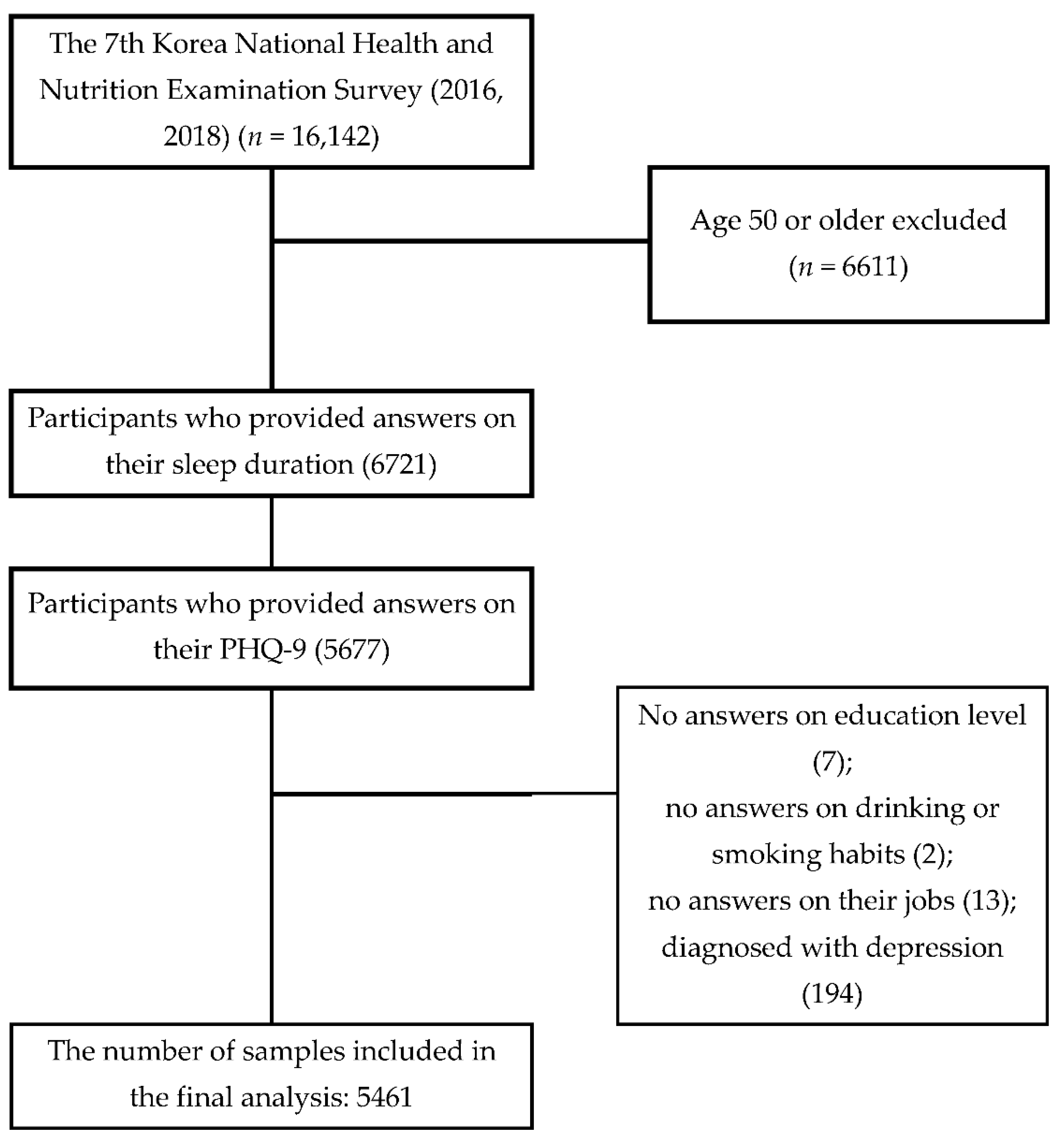
2.2. Sample Selection
2.3. Analysis Items
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
3.2. Characteristics of the Subjects with and without Symptoms of Depression
3.3. The Factors That Affect Symptoms of Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Augner, C. Associations of subjective sleep quality with depression score, anxiety, physical symptoms and sleep onset latency in students. Cent. Eur. J. Public Health 2011, 19, 115–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Pickering, T.G.; Rundle, A.G.; Zammit, G.K.; Malaspina, D. Short sleep duration as a risk factor for hypertension: Analyses of the first National Health and Nutrition Examination Survey. Hypertension 2006, 47, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesarwi, O.; Polak, J.; Jun, J.; Polotsky, V.Y. Sleep disorders and the development of insulin resistance and obesity. Endocrinol. Metab. Clin. N. Am. 2013, 42, 617–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Yadav, D.; Ahn, S.V.; Koh, S.B.; Park, J.T.; Yoon, J.; Yoo, B.S.; Lee, S.H. A prospective study of total sleep duration and incident metabolic syndrome: The ARIRANG study. Sleep Med. 2015, 16, 1511–1515. [Google Scholar] [CrossRef]
- Yeo, Y.; Ma, S.H.; Park, S.K.; Chang, S.H.; Shin, H.R.; Kang, D.; Yoo, K.Y. A prospective cohort study on the relationship of sleep duration with all-cause and disease-specific mortality in the Korean Multi-center Cancer Cohort study. J. Prev. Med. Public Health 2013, 46, 271–281. [Google Scholar] [CrossRef]
- Epstein, R.; Chillag, N.; Lavie, P. Starting times of school: Effects on daytime functioning fifth-grade children in Israel. Sleep 1998, 21, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Philips. How COVID-19 Changed Sleep around the World. Available online: https://www.philips.com/c-dam/corporate/newscenter/global/standard/resources/healthcare/2021/wsd/philips-wsd-2021-report.download.pdf (accessed on 27 March 2022).
- Kim, H.K. Comparison of physical, psychosocial and cognitive factors, and depression between middle-aged women and middle aged men. Korean J. Adults Nurs. 2006, 18, 446–456. [Google Scholar]
- Korea Centers for Disease Control and Prevention. 2017 National Health Statistics Reports, The 6th Korea National Health and Nutrition Examination Survey; Centers for Disease Control and Prevention: Osong, Republic of Korea, 2017. Available online: https://knhanes.kdca.go.kr/knhanes/sub03/sub03_02_05.do (accessed on 27 March 2022).
- Li, S.; Xu, Y.; Zheng, L.; Pang, H.; Zhang, Q.; Lou, L.; Huang, X. Sex difference in global burden of major depressive disorder: Findings from the global burden of disease study 2019. Front. Psychiatry 2022, 13, 789305. [Google Scholar] [CrossRef]
- Jung., S.H.; Park, J.H.; Yoon, H.J.; Kim, J.H.; Kim, N.C.; Kim, S.H. The relationship between sleep quality and depressive symptoms among university students: Moderating effect of the positive psychology. Korean Soc. Biol. Ther. Psychiatry 2018, 24, 173–183. [Google Scholar]
- Breslau, N.; Roth, T.; Rosenthal, L.; Andreski, P. Daytime sleepiness: An epidemiological study of young adults. Am. J. Public Health 1997, 87, 1649–1653. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Mayer, T.G.; Williams, M.J.; Gatchel, R.J. What is the best screening test for depression in chronic spinal pain patients? Spine J. 2014, 14, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- de Man-van Ginkel, J.M.; Gooskens, F.; Schepers, V.P.; Schuurmans, M.J.; Lindeman, E.; Hafsteinsdóttir, T.B. Screening for poststroke depression using the Patient Health Questionnaire. Nurs. Res. 2012, 61, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Wheaton, A.G.; Keenan, N.L.; Greenlund, K.J.; Perry, G.S.; Croft, J.B. Association of sleep duration and hypertension among US adults varies by age and sex. Am. J. Hypertens. 2012, 25, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redeker, N.S.; McEnany, G.P. Sleep Disorders and Sleep Promotion in Nursing Practice, 1st ed.; Springer Publishing Company: New York, NY, USA, 2011. [Google Scholar]
- Dong, L.; Xie, Y.; Zou, X. Association between sleep duration and depression in US adults: A cross-sectional study. J. Affect. Disord. 2022, 296, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Shi, L.; Bao, Y.; Sun, Y.; Shi, J.; Lu, L. The bidirectional relationship between sleep duration and depression in community-dwelling middle-aged and elderly individuals: Evidence from a longitudinal study. Sleep Med. 2018, 52, 221–229. [Google Scholar] [CrossRef]
- Zhai, L.; Zhang, H.; Zhang, D. Sleep duration and depression among adults: A meta-analysis of prospective studies. Depress. Anxiety 2015, 32, 664–670. [Google Scholar] [CrossRef]
- Dement, W.C.; Vaughan, C. The promise of Sleep: A Pioneer in Sleep Medicine Explores the Vital Connection between Health, Happiness, and a Good Night’s Sleep; Dell Publishing Co.: New York, NY, USA, 1999. [Google Scholar]
- Mai, Q.D.; Hill, T.D.; Vila-Henninger, L.; Grandner, M.A. Employment insecurity and sleep disturbance: Evidence from 31 European countries. J. Sleep Res. 2019, 28, e12763. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.R. The impact of working mother’s work-family spillover and depression on parenting. Korean Council Soc. Welfare Edu. 2014, 25, 99–121. [Google Scholar]
- Bea, S.S. Relationships between Sleep Duration and Depression or Suicidal Thoughts in Korean Adults. Korean J. Health Serv. Manag. 2018, 12, 219–228. [Google Scholar] [CrossRef]
- Seoul Metropolitan Big Data Division. 2018 Seoul Survey Report; Seoul Metropolitan Government: Seoul, Republic of Korea, 2018.
- Kim, J.S.; Hong, H.S.; Na, Y.K. A study of fatigue, depression and sleep disorders in patients with chronic liver diseases. J. Korean BioNurs. Sci. 2012, 14, 1–7. [Google Scholar]
- Statistics Korea. Time Use Survey; Statistics Korea: Daejeon, Republic of Korea, 2019.
- Cho, H.S.; Kim, Y.W.; Park, H.W.; Lee, K.H.; Jeong, B.G.; Kang, Y.S.; Park, K.S. The relationship between job stress, sleep quality and the depressive symptoms among female workers. Ann. Occup. Environ. Med. 2013, 25, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.S.; Lee, D.B.; Kwon, I.S.; Cho, Y.C. Depressive symptoms and their association with sleep quality, occupational stress and fatigue among small-scaled manufacturing male workers. Korean J. Occup. Envion. Med. 2011, 23, 99–111. [Google Scholar] [CrossRef]
- DeLongis, A.; Folkman, S.; Lazarus, R.S. The impact of daily stress on health and mood: Psychological and social resources as mediators. J. Pers. Soc. Psychol. 1988, 54, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S.; Girgus, J.S.; Seligman, M.E. Predictors and consequences of childhood depressive symptoms: A 5-year longitudinal study. J.Abnorm. Psychol. 1992, 101, 405–422. [Google Scholar] [CrossRef]
- Suh, M.; Choi-Kwon, S. Sleep-wake disturbance in post-stroke patients. J. Korean Biol. Nurs. Sci. 2009, 11, 23–31. [Google Scholar]
- Han, E.K. An analysis of convergence factors on depressive symptoms women in the postmenopausal: Based on the theory of unpleasant symptoms. J. Converg. Inf. Technol. 2018, 8, 59–67. [Google Scholar]
- Shin, K.A. Effect of the cinema therapy program for middle-aged women with depression. J. Digital Converg. 2018, 16, 511–522. [Google Scholar]
- Gallo, L.C.; Bogart, L.M.; Vranceanu, A.M.; Matthews, K.A. Socioeconomic status, resources, psychological experiences, and emotional responses: A test of the reserve capacity model. J. Personal. Soc. Psychol. 2005, 88, 386. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, G.A.; Shema, S.J.; Leite, C.M.A. Socioeconomic determinants of psychological well-being: The role of income, income change, and income sources during the course of 29 years. Ann. Epidemiol. 2008, 18, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Pearlin, L.I.; Menaghan, E.G.; Lieberman, M.A.; Mullan, J.T. The stress process. J. Health Soc. Behav. 1981, 22, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.Y.; Park, I.S. Analysis of risk factors affecting suicidal ideation in South Korea by life cycle stage. Osong. Public Health Res. Perspect. 2021, 12, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Yang, C.K.; Kim, J.I.; Hong, Y.S.; Kim, J.M. Effects of health on shift-work: General and psychological health, sleep, stress, quality of life. Korean J. Occup. Environ. Med. 2002, 14, 247–256. [Google Scholar] [CrossRef]
- Antunes, L.C.; Levandovski, R.; Dantas, G.; Caumo, W.; Hidalgo, M.P. Obesity and shift work: Chronobiological aspects. Nutr. Res. Rev. 2010, 23, 155–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philip, P. Sleepiness of occupational drivers. Ind. Health 2005, 43, 30–33. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J. The effects of shift work and hours of sleep on metabolic syndrome in Korean workers. Korean J. Occup. Health Nurs. 2016, 25, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Harrington, J.M. Health effects of shift work and extended hours of work. Occup. Environ. Med. 2001, 58, 68–72. [Google Scholar] [CrossRef]
- Kalmbach, D.A.; Pillai, V.; Cheng, P.; Arnedt, J.T.; Drake, C.L. Shift work disorder depression, and anxiety in the transition to rotating shifts: The role of sleep reactivity. Sleep Med. 2015, 16, 1532–1538. [Google Scholar] [CrossRef] [Green Version]
- Fluharty, M.; Taylor, A.E.; Grabski, M.; Munafo, M.R. The association of cigarette smoking with depression and anwiety: A systematic review. Nicotine Tob. Res. 2017, 19, 3–13. [Google Scholar] [CrossRef]


{kind=link}
| Category | Frequency | % | Sleep Duration | p | |||
|---|---|---|---|---|---|---|---|
| Less Than 6 Hours n (%) | 6–8 Hours n (%) | 9 Hours or Longer n (%) | |||||
| Gender | Male | 2435 | 52.5 | 654 (27.1) | 1518 (62.1) | 263 (10.8) | <0.0001 |
| Female | 3026 | 47.5 | 751 (25.1) | 1795 (58.9) | 480 (16.0) | ||
| Age | Under 30 | 1361 | 31.1 | 346 (24.3) | 798 (59.5) | 217 (16.1) | <0.0001 |
| 30~39 | 1840 | 31.0 | 414 (24.1) | 1126 (60.8) | 300 (15.0) | ||
| 40 and up | 2260 | 38.0 | 645 (29.3) | 1389 (61.2) | 226 (9.4) | ||
| Education | Less than university | 2321 | 44.7 | 620 (26.1) | 1345 (59.1) | 356 (14.8) | =0.0218 |
| University graduate or higher | 3140 | 55.3 | 785 (26.2) | 1968 (61.8) | 387 (12.0) | ||
| Household income | Low | 389 | 8.4 | 99 (23.9) | 214 (58.5) | 76 (17.6) | =0.0104 |
| Mid-low | 1253 | 23.2 | 340 (27.2) | 723 (57.7) | 190 (15.1) | ||
| Mid-high | 1872 | 34.0 | 465 (25.7) | 1138 (60.8) | 269 (13.5) | ||
| High | 1947 | 34.5 | 501 (26.5) | 1238 (62.8) | 208 (10.7) | ||
| Marital status | Not married | 1796 | 39.3 | 471 (25.4) | 1078 (61.0) | 247 (13.5) | =0.8996 |
| Married (including common-law relationships) | 3497 | 58.0 | 888 (26.6) | 2136 (60.4) | 473 (13.1) | ||
| Separated, windowed, or divorced | 168 | 2.7 | 46 (28.3) | 99 (58.4) | 23 (13.3) | ||
| Monthly drinking habits | Not drinking | 1865 | 32.5 | 512 (26.9) | 1075 (58.1) | 278 (15.0) | =0.0300 |
| Drinking | 3596 | 67.5 | 893 (25.8) | 2238 (61.8) | 465 (12.4) | ||
| Smoking habits | Smoking | 1262 | 25.9 | 348 (28.9) | 748 (58.6) | 166 (12.5) | =0.0498 |
| Smoked in the past | 935 | 18.1 | 232 (24.7) | 596 (63.8) | 107 (11.5) | ||
| No smoking | 3264 | 56.0 | 825 (25.4) | 1969 (60.4) | 470 (14.2) | ||
| Job | Employed | 3864 | 70.9 | 973 (25.8) | 2445 (63.0) | 446 (11.2) | <0.0001 |
| Unemployed | 1597 | 29.1 | 432 (27.2) | 868 (54.7) | 297 (18.1) | ||
| Shifts | Day shift | 3597 | 65.7 | 852 (24.6) | 2337 (64.5) | 408 (10.8) | <0.0001 |
| Nonregular shifts | 823 | 16.5 | 264 (29.7) | 423 (52.7) | 136 (17.7) | ||
| Unemployed (housewives, students) | 1041 | 17.8 | 289 (28.5) | 553 (53.3) | 199 (18.1) | ||
| Symptoms of depression | No | 5247 | 96.2 | 1325 (25.5) | 3214 (61.3) | 708 (13.1) | <0.0001 |
| Yes (PHQ ≥ 10) | 214 | 3.8 | 80 (41.6) | 99 (42.0) | 35 (16.4) | ||
| Perceived | No | 3747 | 68.8 | 889 (24.0) | 2309 (61.5) | 549 (14.5) | <0.0001 |
| Yes | 1714 | 31.2 | 516 (30.9) | 1004 (58.5) | 194 (10.6) | ||
| Category | Without Symptoms of Depression(PHQ < 10) n (%) | With Symptoms of Depression (PHQ ≥ 10) n (%) | p | |
|---|---|---|---|---|
| Gender | Male | 2364 (97.12) | 71 (2.88) | =0.0013 |
| Female | 2883 (95.08) | 143 (4.92) | ||
| Age | Under 30 | 1294 (95.34) | 67 (4.66) | =0.0130 |
| 30–39 | 1757 (95.60) | 83 (4.40) | ||
| 40 and up | 2196 (97.26) | 64 (2.74) | ||
| Education | Less than university | 2213 (95.82) | 108 (4.18) | =0.3083 |
| University graduate or higher | 3034 (96.42) | 106 (3.58) | ||
| Household income | Low | 362 (93.02) | 27 (6.98) | =0.0003 |
| Mid-low | 1186 (95.57) | 67 (4.43) | ||
| Mid-high | 1791 (95.79) | 81 (4.21) | ||
| High | 1908 (97.66) | 39 (2.34) | ||
| Marital status | Not married | 1704 (95.15) | 92 (4.85) | <0.0001 |
| Common-law relationship | 3389 (97.06) | 108 (2.94) | ||
| Separated, windowed, or divorced | 154 (91.28) | 14 (8.72) | ||
| Monthly drinking habits | Not drinking | 1798 (96.57) | 67 (3.43) | =0.3177 |
| Drinking | 3449 (95.95) | 147 (4.05) | ||
| Smoking habits | Smoking | 1184 (94.16) | 78 (5.84) | =0.0005 |
| Smoked in the past | 896 (96.34) | 39 (3.66) | ||
| No smoking | 3167 (97.01) | 97 (2.99) | ||
| Job | Employed | 3746 (97.17) | 118 (2.83) | <0.0001 |
| Unemployed | 1501 (93.66) | 96 (6.34) | ||
| Shifts | Day shift | 3483 (96.81) | 114 (3.19) | =0.0130 |
| Nonregular shifts | 770 (94.96) | 53 (5.04) | ||
| Unemployed (housewives, students) | 994 (94.83) | 47 (5.17) | ||
| Sleep duration | Short (<6 h/day) | 1325 (93.87) | 80 (6.13) | <0.0001 |
| Normal (6–8 h/day) | 3214 (97.33) | 99 (2.67) | ||
| Long (≥9 h/day) | 708 (95.25) | 35 (4.75) | ||
| Perceived | No | 3721 (99.28) | 26 (0.72) | <0.0001 |
| Yes | 1526 (89.27) | 188 (10.73) | ||
| Category | Ref | Variable | Model 1 | Model 2 | Model 3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% Confidence Interval | p | OR | 95% Confidence Interval | p | OR | 95% Confidence Interval | p | ||||||
| Lower Limit | Upper Limit | Lower Limit | Upper Limit | Lower Limit | Upper Limit | |||||||||
| Sleep duration | Normal (6–8 h/day) | Short (<6 h/day) | 2.381 | 1.649 | 3.437 | <0.0001 | 2.471 | 1.709 | 3.572 | <0.0001 | 1.979 | 1.322 | 2.964 | =0.0010 |
| Long (≥9 h/day) | 1.821 | 1.189 | 2.789 | =0.006 | 1.620 | 1.053 | 2.493 | =0.0284 | 1.849 | 1.16 | 2.947 | =0.0099 | ||
| Gender | Male | Female | 1.777 | 1.252 | 2.52 | =0.0014 | 2.581 | 1.703 | 3.912 | <0.0001 | ||||
| Age | Under 30 | 30~39 | 0.946 | 0.629 | 1.420 | =0.7866 | 1.534 | 0.863 | 2.727 | =0.1442 | ||||
| 40 and up | 0.551 | 0.369 | 0.823 | =0.0038 | 1.193 | 0.659 | 2.160 | =0.5584 | ||||||
| Education | University graduate or higher | Less than university | 0.795 | 0.548 | 1.154 | =0.2272 | ||||||||
| Household income | Mid-high | Low | 1.347 | 0.730 | 2.487 | =0.3395 | ||||||||
| Mid-low | 0.881 | 0.582 | 1.334 | =0.5487 | ||||||||||
| High | 0.597 | 0.373 | 0.957 | =0.0322 | ||||||||||
| Marital status | Common-law relationship | Not married | 1.765 | 1.062 | 2.934 | =0.0286 | ||||||||
| Separated, windowed, or divorced | 2.875 | 1.421 | 5.819 | =0.0034 | ||||||||||
| Monthly drinking habits | Not drinking | Drinking | 0.815 | 0.562 | 1.182 | =0.2792 | ||||||||
| Smoking habits | No smoking | Smoking | 2.902 | 1.882 | 4.475 | <0.0001 | ||||||||
| Smoked in the past | 1.851 | 1.138 | 3.011 | =0.0133 | ||||||||||
| Job | Employed | Unemployed | 3.295 | 2.032 | 5.342 | <0.0001 | ||||||||
| Shifts | Day shift | Nonregular shifts | 1.580 | 1.035 | 2.411 | =0.0341 | ||||||||
| Unemployed (housewives, students) | 0.696 | 0.391 | 1.240 | =0.2183 | ||||||||||
| Perceived | No | No | 15.903 | 10.083 | 25.082 | <0.0001 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.-Y.; Han, J.-E.; Choi, J.; Park, M.; Sung, S.-H.; Sung, A.D.-M. Association between Sleep Duration and Symptoms of Depression Aged between 18 and 49: The Korea National Health and Nutrition Examination Survey (KNHANES Ⅶ) from 2016 to 2018. Healthcare 2022, 10, 2324. https://doi.org/10.3390/healthcare10112324
Choi S-Y, Han J-E, Choi J, Park M, Sung S-H, Sung AD-M. Association between Sleep Duration and Symptoms of Depression Aged between 18 and 49: The Korea National Health and Nutrition Examination Survey (KNHANES Ⅶ) from 2016 to 2018. Healthcare. 2022; 10(11):2324. https://doi.org/10.3390/healthcare10112324
Chicago/Turabian StyleChoi, Sung-Yong, Ji-Eun Han, Jiae Choi, Minjung Park, Soo-Hyun Sung, and Angela Dong-Min Sung. 2022. "Association between Sleep Duration and Symptoms of Depression Aged between 18 and 49: The Korea National Health and Nutrition Examination Survey (KNHANES Ⅶ) from 2016 to 2018" Healthcare 10, no. 11: 2324. https://doi.org/10.3390/healthcare10112324