
A Study on Types of Medication Adherence in Hypertension among Older Patients and Influencing Factors

Abstract
:1. Introduction
2. Materials & Methods
2.1. Data
2.2. Variables
2.2.1. Independent Variable: Sociodemographic Characteristics
2.2.2. Dependent Variable: Medication Adherence (Dose, Dosing Frequency, Time of Administration)
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
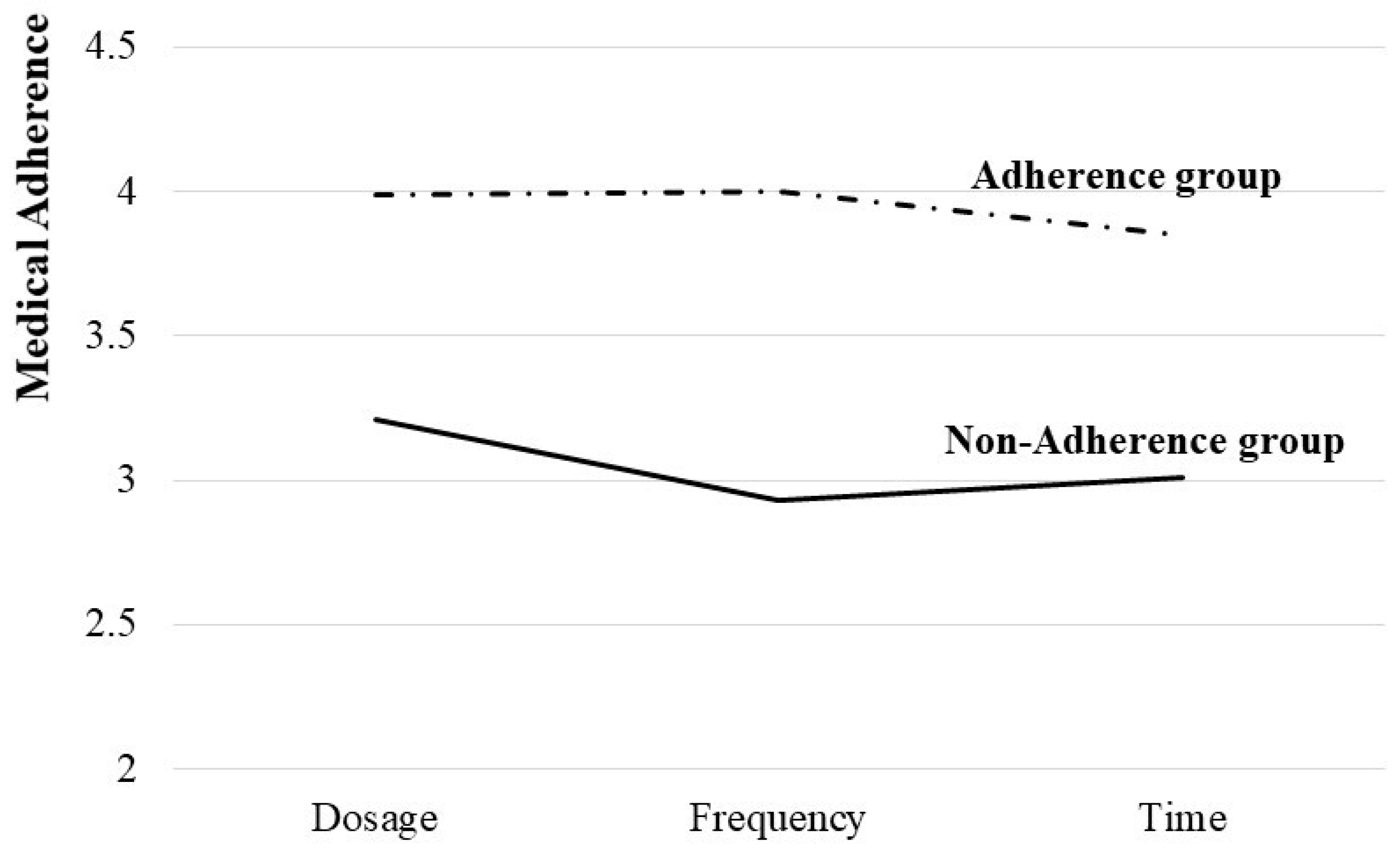
3.2. Types of Medication Adherence in Hypertensive Older Patients
3.3. Analysis of the Study Model
4. Discussion
5. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buford, T.W. Hypertension and aging. Ageing Res. Rev. 2016, 26, 96–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawicka, K.; Szczyrek, M.; Jastrzebska, I.; Prasal, M.; Zwolak, A.; Daniluk, J. Hypertension—The silent killer. J. Pre-Clin. Clin. Res. 2011, 5, 43–46. [Google Scholar]
- Hoel, D.; Howard, R.B.; Gifford, R.W. Hypertension: Stalking the silent killer. Postgrad. Med. 1997, 101, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Kalehoff, J.P.; Oparil, S. The story of the silent killer. Curr. Hypertens. Rep. 2020, 22, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Moore, J. Hypertension: Catching the silent killer. Nurse Pract. 2005, 30, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Lewanczuk, R. Hypertension as a chronic disease: What can be done at a regional level? Can. J. Cardiol. 2008, 24, 483–484. [Google Scholar] [CrossRef] [Green Version]
- Krousel-Wood, M.; Thomas, S.; Muntner, P.; Morisky, D. Medication adherence: A key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr. Opin. Cardiol. 2004, 19, 357–362. [Google Scholar] [CrossRef]
- Brown, M.T.; Bussell, J.K. Medication adherence: WHO cares? In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2011; pp. 304–314. [Google Scholar]
- Lam, W.Y.; Fresco, P. Medication adherence measures: An overview. BioMed Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.V.; Keene, M.S.; Eaddy, M.; Krulewicz, S.; Kraus, J.E.; Carpenter, D.J. Differences in medication adherence and healthcare resource utilization patterns. CNS Drugs 2008, 22, 963–973. [Google Scholar] [CrossRef]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Rolnick, S.J.; Pawloski, P.A.; Hedblom, B.D.; Asche, S.E.; Bruzek, R.J. Patient characteristics associated with medication adherence. Clin. Med. Res. 2013, 11, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, K.J.; Roberts, M.E.; Neiheisel, M.B. Medication adherence part two: Predictors of nonadherence and adherence. J. Am. Assoc. Nurse Pract. 2014, 26, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Gryglewska, B. How can we improve the effectiveness of treatment in elderly hypertensives? Blood Press. 2005, 14, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kwon, O.D.; Han, E.B.; Lee, C.M.; Oh, S.-W.; Joh, H.-K.; Oh, B.; Kwon, H.; Cho, B.; Choi, H.C. Impact of number of medications and age on adherence to antihypertensive medications: A nationwide population-based study. Medicine 2019, 98, e17825. [Google Scholar] [CrossRef] [PubMed]
- MacLaughlin, E.J.; Raehl, C.L.; Treadway, A.K.; Sterling, T.L.; Zoller, D.P.; Bond, C.A. Assessing Medication Adherence in the elderly. Drug Aging 2005, 22, 231–255. [Google Scholar] [CrossRef]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K. Self-report measures of medication adherence behavior: Recommendations on optimal use. Transl. Behav. Med. 2015, 5, 470–482. [Google Scholar] [CrossRef] [Green Version]
- Yap, A.F.; Thirumoorthy, T.; Kwan, Y.H. Systematic review of the barriers affecting medication adherence in older adults. Geriatr. Gerontol. Int. 2016, 16, 1093–1101. [Google Scholar] [CrossRef]
- Korea Institute for Health and Social Affairs and National Health Insurance. Korea Health Panel Annual Data. 2019. Available online: https://www.khp.re.kr:444/eng/faq/faq01.do (accessed on 1 April 2022).
- Muthén, B.; Muthén, L.K. Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcohol. Clin. Exp. Res. 2000, 24, 882–891. [Google Scholar] [CrossRef]
- Newby, L.K.; Allen LaPointe, N.M.; Chen, A.Y.; Kramer, J.M.; Hammill, B.G.; DeLong, E.R.; Muhlbaier, L.H.; Califf, R.M. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation 2006, 113, 203–212. [Google Scholar] [CrossRef] [Green Version]
- Ho, P.M.; Spertus, J.A.; Masoudi, F.A.; Reid, K.J.; Peterson, E.D.; Magid, D.J.; Krumholz, H.M.; Rumsfeld, J.S. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch. Intern. Med. 2006, 166, 1842–1847. [Google Scholar] [CrossRef] [Green Version]
- Schwalm, J.-D.; Ivers, N.M.; Natarajan, M.K.; Taljaard, M.; Rao-Melacini, P.; Witteman, H.O.; Zwarenstein, M.; Grimshaw, J.M. Cluster randomized controlled trial of delayed educational reminders for long-term medication adherence in ST-elevation myocardial infarction (DERLA-STEMI). Am. Heart J. 2015, 170, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.M.; Lambert-Kerzner, A.; Carey, E.P.; Fahdi, I.E.; Bryson, C.L.; Melnyk, S.D.; Bosworth, H.B.; Radcliff, T.; Davis, R.; Mun, H. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Pantuzza, L.L.; Ceccato, M.d.G.B.; Silveira, M.R.; Junqueira, L.M.R.; Reis, A.M.M. Association between medication regimen complexity and pharmacotherapy adherence: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 1475–1489. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jang, J.; Yang, S.; Hahn, J.; Min, K.L.; Jung, E.h.; Oh, K.s.; Cho, R.; Chang, M.J. Development and validation of the Korean version of the medication regimen complexity index. PLoS ONE 2019, 14, e0216805. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Khan, H.; Heydon, E.; Shroufi, A.; Fahimi, S.; Moore, C.; Stricker, B.; Mendis, S.; Hofman, A.; Mant, J. Adherence to cardiovascular therapy: A meta-analysis of prevalence and clinical consequences. Eur. Heart J. 2013, 34, 2940–2948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naderi, S.H.; Bestwick, J.P.; Wald, D.S. Adherence to drugs that prevent cardiovascular disease: Meta-analysis on 376,162 patients. Am. J. Med. 2012, 125, 882–887.e881. [Google Scholar] [CrossRef] [PubMed]
- Burnier, M.; Polychronopoulou, E.; Wuerzner, G. Hypertension and drug adherence in the elderly. Front. Cardiovasc. Med. 2020, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.; Bai, X.; Leung, A.Y.; Liu, B.C.; Chi, I. Prevalence of medication adherence and its associated factors among community-dwelling C hinese older adults in H ong K ong. Geriatr. Gerontol. Int. 2015, 15, 789–796. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Honig, L.S.; Tang, M.X.; Devanand, D.P. Depressive symptoms, vascular risk factors, and Alzheimer’s disease. Int. J. Geriatr. Psychiatry A J. Psychiatry Late Life Allied Sci. 2008, 23, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Lobo-Escolar, A.; Roy, J.F.; Saz, P.; De-la-Cámara, C.; Marcos, G.; Lobo, A. Association of hypertension with depression in community-dwelling elderly persons. Psychother. Psychosom. 2008, 77, 323–325. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; Islam, T.; Muntner, P.; Holt, E.; Joyce, C.; Morisky, D.E.; Webber, L.S.; Frohlich, E.D. Association of depression with antihypertensive medication adherence in older adults: Cross-sectional and longitudinal findings from CoSMO. Ann. Behav. Med. 2010, 40, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Krousel-Wood, M.A.; Frohlich, E.D. Hypertension and depression: Coexisting barriers to medication adherence. J. Clin. Hypertens. 2010, 12, 481. [Google Scholar] [CrossRef] [PubMed]
- Hennein, R.; Hwang, S.J.; Au, R.; Levy, D.; Muntner, P.; Fox, C.S.; Ma, J. Barriers to medication adherence and links to cardiovascular disease risk factor control: The Framingham Heart Study. Intern. Med. J. 2018, 48, 414–421. [Google Scholar] [CrossRef] [PubMed]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenthaler, A.; Ogedegbe, G.; Allegrante, J.P. Self-efficacy mediates the relationship between depressive symptoms and medication adherence among hypertensive African Americans. Health Educ. Behav. 2009, 36, 127–137. [Google Scholar] [CrossRef]
- Turner, B.J.; Hollenbeak, C.; Weiner, M.G.; Ten Have, T.; Roberts, C. Barriers to adherence and hypertension control in a racially diverse representative sample of elderly primary care patients. Pharmacoepidemiol. Drug Saf. 2009, 18, 672–681. [Google Scholar] [CrossRef]
- Shi, L.; Liu, J.; Fonseca, V.; Walker, P.; Kalsekar, A.; Pawaskar, M. Correlation between adherence rates measured by MEMS and self-reported questionnaires: A meta-analysis. Health Qual. Life Outcomes 2010, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.M.U.; Caze, A.L.; Cottrell, N. What are validated self-report adherence scales really measuring?: A systematic review. Br. J. Clin. Pharmacol. 2014, 77, 427–445. [Google Scholar] [CrossRef]
- Giardini, A.; Martin, M.T.; Cahir, C.; Lehane, E.; Menditto, E.; Strano, M.; Pecorelli, S.; Monaco, A.; Marengoni, A. Toward appropriate criteria in medication adherence assessment in older persons: Position Paper. Aging Clin. Exp. Res. 2016, 28, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2571. [Google Scholar] [CrossRef]
- Mancia, G.; Zambon, A.; Soranna, D.; Merlino, L.; Corrao, G. Factors involved in the discontinuation of antihypertensive drug therapy: An analysis from real life data. J. Hypertens. 2014, 32, 1708–1716. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, N.K.; Fischer, M.A.; Avorn, J.; Liberman, J.N.; Schneeweiss, S.; Pakes, J.; Brennan, T.A.; Shrank, W.H. The implications of therapeutic complexity on adherence to cardiovascular medications. Arch. Intern. Med. 2011, 171, 814–822. [Google Scholar] [CrossRef] [Green Version]
- Iadecola, C.; Gottesman, R.F. Neurovascular and cognitive dysfunction in hypertension: Epidemiology, pathobiology, and treatment. Circ. Res. 2019, 124, 1025–1044. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.A.; Goeman, D.; Beanland, C.; Koch, S. Ability of older people with dementia or cognitive impairment to manage medicine regimens: A narrative review. Curr. Clin. Pharmacol. 2015, 10, 213–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.; Lovell, J.; Weller, C.; Kennedy, B.; Winbolt, M.; Young, C.; Ibrahim, J. A systematic review of medication non-adherence in persons with dementia or cognitive impairment. PLoS ONE 2017, 12, e0170651. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| (N = 2300) | |||
|---|---|---|---|
| Variable | Categories | n | % |
| Gender | Male | 944 | 41.0 |
| Female | 1356 | 59.0 | |
| Age (M ± S.D) | 73.58 (5.68) | ||
| USD $ Equalized Annual Income (M ± S.D) | 18,643.12 (16,594.67) | ||
| Living Status | Living with someone | 1729 | 75.2 |
| Living alone | 571 | 24.8 | |
| Educational Background | Below elementary school | 277 | 12.0 |
| Elementary school | 936 | 40.7 | |
| Middle school | 470 | 20.4 | |
| High school | 459 | 20.0 | |
| University or above | 158 | 6.9 | |
| Residential Area | Urban | 1529 | 66.5 |
| Rural | 771 | 33.5 | |
| Subjective health—(M ± S.D) | 2.89 (0.88) | ||
| Level of stress (M ± S.D) | 1.88 (0.81) | ||
| Depressive Symptoms | No | 2083 | 90.6 |
| Yes | 217 | 9.4 | |
| (N = 2300) | ||||
|---|---|---|---|---|
| Variable | Min | Max | M | SD |
| Medication adherence—dose | 1.00 | 4.00 | 3.89 | 0.34 |
| Medication adherence—dosing frequency | 1.00 | 4.00 | 3.86 | 0.38 |
| Medication adherence—time of administration | 1.00 | 4.00 | 3.74 | 0.51 |
| Class | Model Fit | Groups | ||||
|---|---|---|---|---|---|---|
| AIC | BIC | SSABIC | Entropy | BLRT p-Value | n (%) | |
| 1 | 7119.192 | 7153.636 | 7134.573 | - | - | - |
| 2 | 7034.343 | 7069.142 | 7051.549 | 0.987 | <0.001 | 2004 (87.1), 296 (12.9) |
| 3 | 6984.137 | 7021.674 | 7002.967 | 0.839 | <0.001 | 2004 (87.1), 279 (12.1), 17 (0.7) |
| 4 | 6910.765 | 6973.547 | 6943.531 | 0.783 | <0.001 | 1986 (86.3), 279 (12.1), 18 (0.8), 17 (0.7) |
| (N = 2300) | |||
|---|---|---|---|
| Variables | B | S.E. | Exp (B) |
| Gender (ref. Male) | 0.179 | 0.148 | 01.196 |
| Age | −0.054 *** | 0.011 | 0.947 |
| USD $ Equalized Annual Income (log) | −0.200 | 0.104 | 0.818 |
| Living Status (ref. living with someone) | −0.503 ** | 0.147 | 0.605 |
| Educational Background | −0.058 | 0.062 | 0.944 |
| Residential Area (ref. urban) | −0.188 | 0.135 | 0.829 |
| Subjective Health | −0.010 | 0.079 | 0.990 |
| Level of Stress | −0.080 | 0.085 | 0.923 |
| Depressive Symptoms (ref. No) | −0.491 * | 0.208 | 0.612 |
| constant | 8.281 | 1.426 | 3949.787 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Jeong, K.-H.; Lee, S.; Park, H. A Study on Types of Medication Adherence in Hypertension among Older Patients and Influencing Factors. Healthcare 2022, 10, 2322. https://doi.org/10.3390/healthcare10112322
Lee S, Jeong K-H, Lee S, Park H. A Study on Types of Medication Adherence in Hypertension among Older Patients and Influencing Factors. Healthcare. 2022; 10(11):2322. https://doi.org/10.3390/healthcare10112322
Chicago/Turabian StyleLee, Sunmin, Kyu-Hyoung Jeong, Seoyoon Lee, and Hayoung Park. 2022. "A Study on Types of Medication Adherence in Hypertension among Older Patients and Influencing Factors" Healthcare 10, no. 11: 2322. https://doi.org/10.3390/healthcare10112322