
How Vulnerable Are Patients with COPD to Weather Extremities?—A Pilot Study from Hungary

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Design
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Local Climatological Data of the Studied City (Pécs) in 2017
3.2. Demographic and Clinical Characteristics of Patients Visiting the ED in the Studied City (Pécs) in 2017
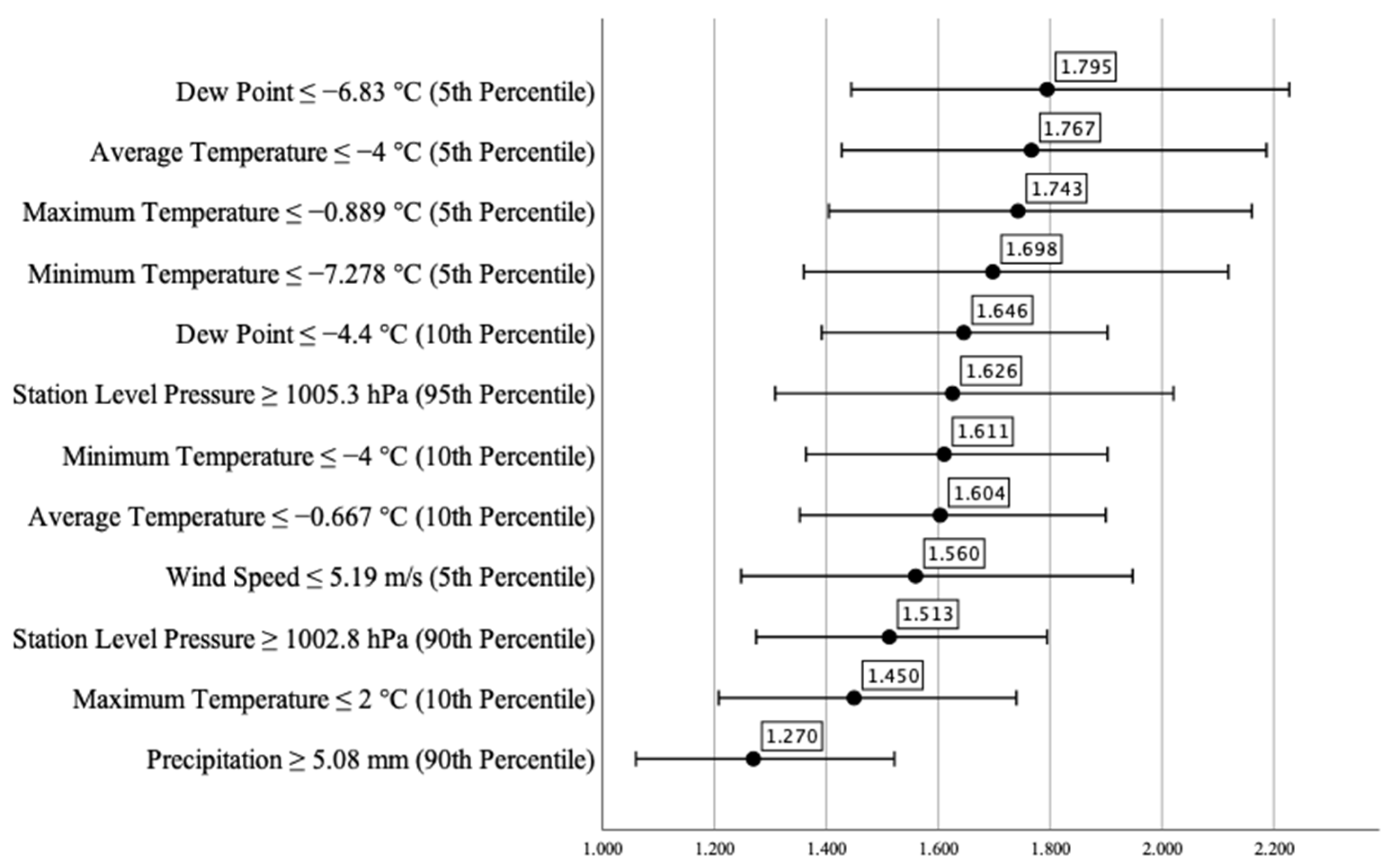
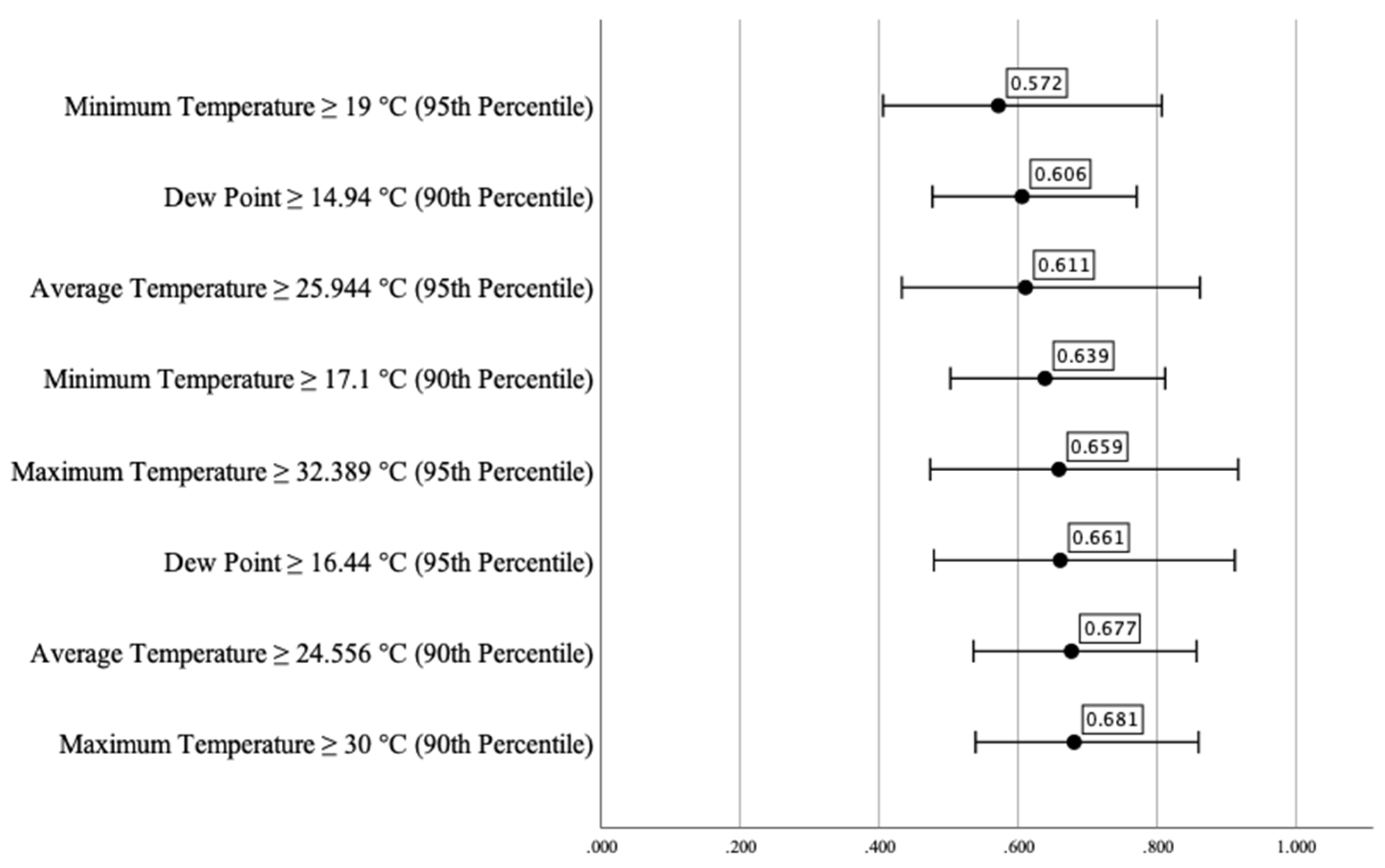
3.3. Association between Extremes of Meteorological Parameters and the Number of ED Visits
3.4. Association between Extremes of Meteorological Parameters and Number of COPD-Related ED Visits
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Le Tertre, A.; Lefranc, A.; Eilstein, D.; Declercq, C.; Medina, S.; Blanchard, M.; Chardon, B.; Fabre, P.; Filleul, L.; Jusot, J.-F.; et al. Impact of the 2003 Heatwave on All-Cause Mortality in 9 French Cities. Epidemiology 2006, 17, 75–79. [Google Scholar] [CrossRef] [PubMed]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; de’Donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramón, M.; Paldy, A.; et al. The Impact of Heat Waves on Mortality in 9 European Cities: Results from the EuroHEAT Project. Environ. Health 2010, 9, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bittner, M.-I.; Nübling, M.; Stössel, U. Heat-Related Mortality in Freiburg and Rostock in 2003 and 2005—Methodology and Results. Gesundheitswesen 2013, 75, e126–e130. [Google Scholar] [CrossRef] [PubMed]
- Steul, K.; Schade, M.; Heudorf, U. Mortality during Heatwaves 2003–2015 in Frankfurt-Main—The 2003 Heatwave and Its Implications. Int. J. Hyg. Environ. Health 2018, 221, 81–86. [Google Scholar] [CrossRef]
- Cheng, J.; Xu, Z.; Bambrick, H.; Prescott, V.; Wang, N.; Zhang, Y.; Su, H.; Tong, S.; Hu, W. Cardiorespiratory Effects of Heatwaves: A Systematic Review and Meta-Analysis of Global Epidemiological Evidence. Environ. Res. 2019, 177, 108610. [Google Scholar] [CrossRef]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat Waves and Morbidity: Current Knowledge and Further Direction—A Comprehensive Literature Review. IJERPH 2015, 12, 5256–5283. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Zhou, J.; Yang, S.; Yu, Z.; Wang, F.; Zhou, J. Effects of Extreme Temperatures on Hospital Emergency Room Visits for Respiratory Diseases in Beijing, China. Environ. Sci. Pollut. Res. 2019, 26, 3055–3064. [Google Scholar] [CrossRef]
- Liang, W.-M.; Liu, W.-P.; Chou, S.-Y.; Kuo, H.-W. Ambient Temperature and Emergency Room Admissions for Acute Coronary Syndrome in Taiwan. Int. J. Biometeorol. 2008, 52, 223–229. [Google Scholar] [CrossRef]
- Liang, W.-M.; Liu, W.-P.; Kuo, H.-W. Diurnal Temperature Range and Emergency Room Admissions for Chronic Obstructive Pulmonary Disease in Taiwan. Int. J. Biometeorol. 2009, 53, 17–23. [Google Scholar] [CrossRef]
- Feng, F.; Ma, Y.; Zhang, Y.; Shen, J.; Wang, H.; Cheng, B.; Jiao, H. Effects of Extreme Temperature on Respiratory Diseases in Lanzhou, a Temperate Climate City of China. Environ. Sci. Pollut. Res. 2021, 28, 49278–49288. [Google Scholar] [CrossRef]
- Giamello, J.D.; Melchio, R.; Bertolaccini, L.; Caraccio, P.; Rendina, C.; Lauria, G. Climatic Factors Influence on Emergency Department Visits. Hong Kong J. Emerg. Med. 2022, 29, 323–324. [Google Scholar] [CrossRef]
- Global, Regional, and National Deaths, Prevalence, Disability-Adjusted Life Years, and Years Lived with Disability for Chronic Obstructive Pulmonary Disease and Asthma, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [CrossRef] [Green Version]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef] [Green Version]
- Rabe, K.F.; Watz, H. Chronic Obstructive Pulmonary Disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Donaldson, G.; Wedzicha, J. The Causes and Consequences of Seasonal Variation in COPD Exacerbations. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1101–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almagro, P.; Hernandez, C.; Martinez-Camblor, P.; Tresserras, R.; Escarrabill, J. Seasonality, Ambient Temperatures and Hospitalizations for Acute Exacerbation of COPD: A Population-Based Study in a Metropolitan Area. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 899. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, C.; Hanisch, M.; Heinsohn, J.B.; Dostal, V.; Jehn, M.; Liebers, U.; Pankow, W.; Donaldson, G.C.; Witt, C. Increased Vulnerability of COPD Patient Groups to Urban Climate in View of Global Warming. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 3493–3501. [Google Scholar] [CrossRef] [Green Version]
- Hansel, N.N.; McCormack, M.C.; Kim, V. The Effects of Air Pollution and Temperature on COPD. COPD J. Chronic Obstr. Pulm. Dis. 2016, 13, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Lam, H.C.; Chan, E.Y.; Goggins, W.B. Comparison of Short-Term Associations with Meteorological Variables between COPD and Pneumonia Hospitalization among the Elderly in Hong Kong—A Time-Series Study. Int. J. Biometeorol. 2018, 62, 1447–1460. [Google Scholar] [CrossRef]
- Tseng, C.-M.; Chen, Y.-T.; Ou, S.-M.; Hsiao, Y.-H.; Li, S.-Y.; Wang, S.-J.; Yang, A.C.; Chen, T.-J.; Perng, D.-W. The Effect of Cold Temperature on Increased Exacerbation of Chronic Obstructive Pulmonary Disease: A Nationwide Study. PLoS ONE 2013, 8, e57066. [Google Scholar] [CrossRef]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-Analysis of Epidemiological Evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.-H.; Du, X.L.; Chan, W.; Zhang, K. Impacts of Cold Weather on Emergency Hospital Admission in Texas, 2004–2013. Environ. Res. 2019, 169, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Ikäheimo, T.M.; Jokelainen, J.; Näyhä, S.; Laatikainen, T.; Jousilahti, P.; Laukkanen, J.; Jaakkola, J.J.K. Cold Weather-Related Cardiorespiratory Symptoms Predict Higher Morbidity and Mortality. Environ. Res. 2020, 191, 110108. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Xu, Z.; Bambrick, H.; Su, H.; Tong, S.; Hu, W. Impacts of Exposure to Ambient Temperature on Burden of Disease: A Systematic Review of Epidemiological Evidence. Int. J. Biometeorol. 2019, 63, 1099–1115. [Google Scholar] [CrossRef] [PubMed]
- Javorac, J.; Jevtić, M.; Živanović, D.; Ilić, M.; Bijelović, S.; Dragić, N. What Are the Effects of Meteorological Factors on Exacerbations of Chronic Obstructive Pulmonary Disease? Atmosphere 2021, 12, 442. [Google Scholar] [CrossRef]
- Brzezińska-Pawłowska, O.E.; Rydzewska, A.D.; Łuczyńska, M.; Majkowska-Wojciechowska, B.; Kowalski, M.L.; Makowska, J.S. Environmental Factors Affecting Seasonality of Ambulance Emergency Service Visits for Exacerbations of Asthma and COPD. J. Asthma 2016, 53, 139–145. [Google Scholar] [CrossRef]
- Islam, M.S.; Chaussalet, T.J.; Koizumi, N. Towards a Threshold Climate for Emergency Lower Respiratory Hospital Admissions. Environ. Res. 2017, 153, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, U.; Exner, T.; Wanka, E.R.; Bergemann, C.; Meyer-Arnek, J.; Hildenbrand, B.; Tufman, A.; Heumann, C.; Huber, R.M.; Bittner, M.; et al. Influence of Air Pressure, Humidity, Solar Radiation, Temperature, and Wind Speed on Ambulatory Visits Due to Chronic Obstructive Pulmonary Disease in Bavaria, Germany. Int. J. Biometeorol. 2012, 56, 137–143. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, X.; Kong, D.; Fu, J.; Liu, Y.; Zhao, Y.; Lian, H.; Zhao, X.; Yang, J.; Fan, Z. Effects of Ambient Temperature on Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Results from a Time-Series Analysis of 143318 Hospitalizations. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Zhang, X.; Chen, C.; Lin, Q.; Li, X.; Qu, W.; Liu, X.; Zhao, L.; Chang, S. The Relationship between Ambient Temperature and Acute Respiratory and Cardiovascular Diseases in Shenyang, China. Environ. Sci. Pollut. Res. 2021, 28, 20058–20071. [Google Scholar] [CrossRef]
- Zhan, Z.-Y.; Tian, Q.; Chen, T.-T.; Ye, Y.; Lin, Q.; Han, D.; Ou, C.-Q. Temperature Variability and Hospital Admissions for Chronic Obstructive Pulmonary Disease: Analysis of Attributable Disease Burden and Vulnerable Subpopulation. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 2225–2235. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Avg.Temp. (°C) | Max.Temp. (°C) | Min.Temp. (°C) | DTR (°C) | DewP. (°C) | PRCP (mm) | STP (hPa) | Avg.WdSp. (m/s) | |
|---|---|---|---|---|---|---|---|---|
| 5th percentile | −4 | −0.889 | −7.278 | 2.778 | −6.833 | 0 | 983.3 | 5.186 |
| 10th percentile | −0.667 | 2 | −4 | 4.111 | −4.444 | 0.1 | 985 | 6.297 |
| 90th percentile | 24.056 | 30 | 17.111 | 14 | 14.944 | 5.08 | 1002.8 | 17.224 |
| 95th percentile | 25.944 | 32.389 | 19 | 15 | 16.444 | 9.906 | 1005.3 | 20.372 |
| Avg.Temp. (°C) | Max.Temp. (°C) | Min.Temp. (°C) | DTR (°C) | DewP. (°C) | PRCP (mm) | STP (hPa) | Avg.WdSp. (m/s) | |
|---|---|---|---|---|---|---|---|---|
| Mean | 11.73 | 16.39 | 7 | 9.39 | 5.36 | 1.71 | 993.93 | 11.03 |
| Median | 12 | 17 | 7.28 | 9.61 | 5.33 | 0 | 993.6 | 10 |
| Mode | −0.33 | 23 | 4 | 12.39 | 1.11 | 0 | 993.9 | 7.22 |
| Standard deviation | 9.15 | 10.33 | 8.01 | 3.64 | 7.17 | 5.46 | 6.71 | 4.75 |
| Min | −10.83 | −7.39 | −14.39 | 1 | −20.28 | 0 | 970.5 | 2.04 |
| Max | 29.72 | 36 | 24.39 | 17.61 | 19.44 | 59.69 | 1012.4 | 32.04 |
| Daily Emergency Visits | COPD Cases | Relative Frequency of COPD (%) | |
|---|---|---|---|
| Sum | 51,436 | 1076 | 2.1 |
| Mean | 140.92 | 3.32 | 2.37 |
| Median | 137 | 3 | 2 |
| Standard deviation | 22.7 | 2.19 | 1.55 |
| Min | 92 | 0 | 0 |
| Max | 229 | 12 | 7.94 |
| Weather Parameter | Phi Correlation Coefficient |
|---|---|
| Dew Point ≤ −4.4 °C (10th Percentile) | 0.026 |
| Minimum Temperature ≤ −4 °C (10th Percentile) | 0.025 |
| Average Temperature ≤ −0.667 °C (10th Percentile) | 0.024 |
| Dew Point ≤ −6.83 °C (5th Percentile) | 0.024 |
| Average Temperature ≤ −4 °C (5th Percentile) | 0.023 |
| Maximum Temperature ≤ −0.889 °C (5th Percentile) | 0.023 |
| Minimum Temperature ≤ −7.278 °C (5th Percentile) | 0.021 |
| Station Level Pressure ≥ 1002.8 hPa (90th Percentile) | 0.021 |
| Station Level Pressure ≥ 1005.3 hPa (95th Percentile) | 0.020 |
| Maximum Temperature ≤ 2 °C (10th Percentile) | 0.018 |
| Wind Speed ≤ 5.19 m/s (5th Percentile) | 0.017 |
| Precipitation ≥ 5.08 mm (90th Percentile) | 0.011 |
| Weather Parameter | Phi Correlation Coefficient |
|---|---|
| Average Temperature ≥ 24.556 °C (90th Percentile) | −0.140 |
| Maximum Temperature ≥ 30 °C (90th Percentile) | −0.140 |
| Average Temperature ≥ 25.944 °C (95th Percentile) | −0.130 |
| Dew Point ≥ 14.94 °C (90th Percentile) | −0.018 |
| Minimum Temperature ≥ 17.1 °C (90th Percentile) | −0.016 |
| Minimum Temperature ≥ 19 °C (95th Percentile) | −0.014 |
| Maximum Temperature ≥ 32.389 °C (95th Percentile) | −0.011 |
| Dew Point ≥ 16.44 °C (95th Percentile) | −0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Márovics, G.; Pozsgai, É.; Németh, B.; Czigány, S.; Németh-Simon, S.; Girán, J. How Vulnerable Are Patients with COPD to Weather Extremities?—A Pilot Study from Hungary. Healthcare 2022, 10, 2309. https://doi.org/10.3390/healthcare10112309
Márovics G, Pozsgai É, Németh B, Czigány S, Németh-Simon S, Girán J. How Vulnerable Are Patients with COPD to Weather Extremities?—A Pilot Study from Hungary. Healthcare. 2022; 10(11):2309. https://doi.org/10.3390/healthcare10112309
Chicago/Turabian StyleMárovics, Gergely, Éva Pozsgai, Balázs Németh, Szabolcs Czigány, Szilvia Németh-Simon, and János Girán. 2022. "How Vulnerable Are Patients with COPD to Weather Extremities?—A Pilot Study from Hungary" Healthcare 10, no. 11: 2309. https://doi.org/10.3390/healthcare10112309