
Risk Analysis and Assessment of Lipid Abnormalities as the Earliest Complication in Newly Diagnosed Diabetic and Non-Diabetic Individuals of a Local Population
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Subjects and Data Retrieval
2.3. Statistical Analyses
3. Results
3.1. Clinical Analyses of Subjects
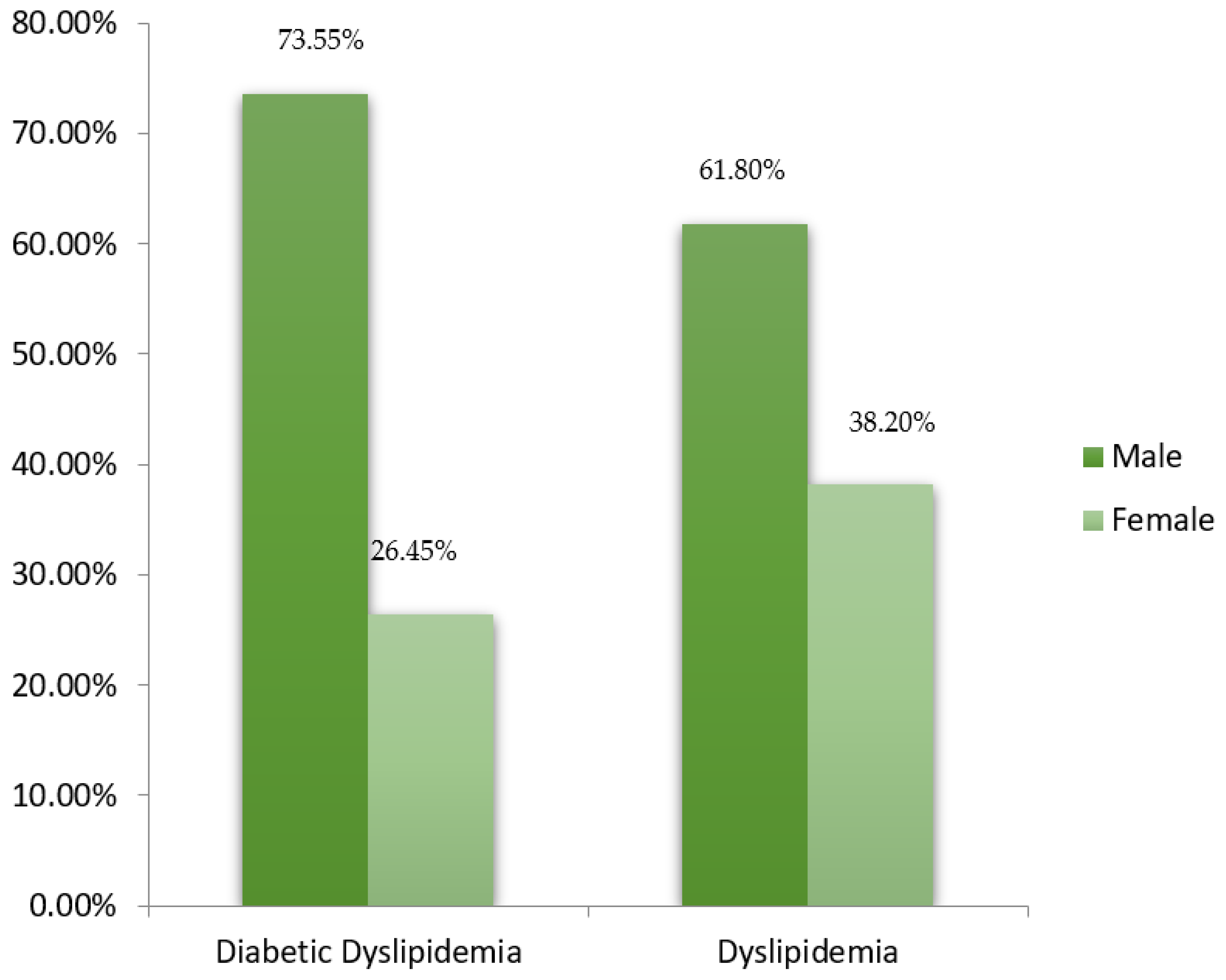
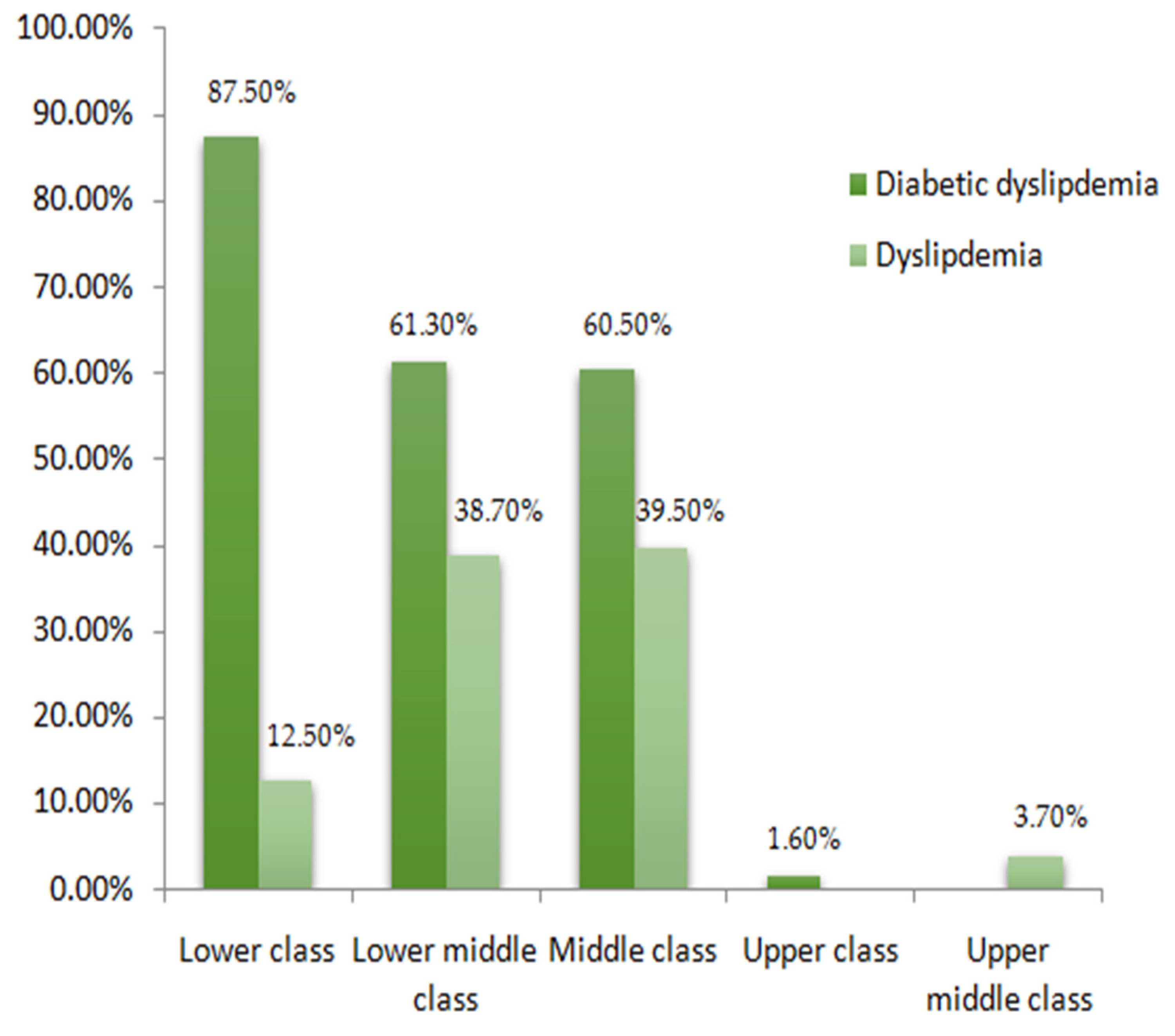
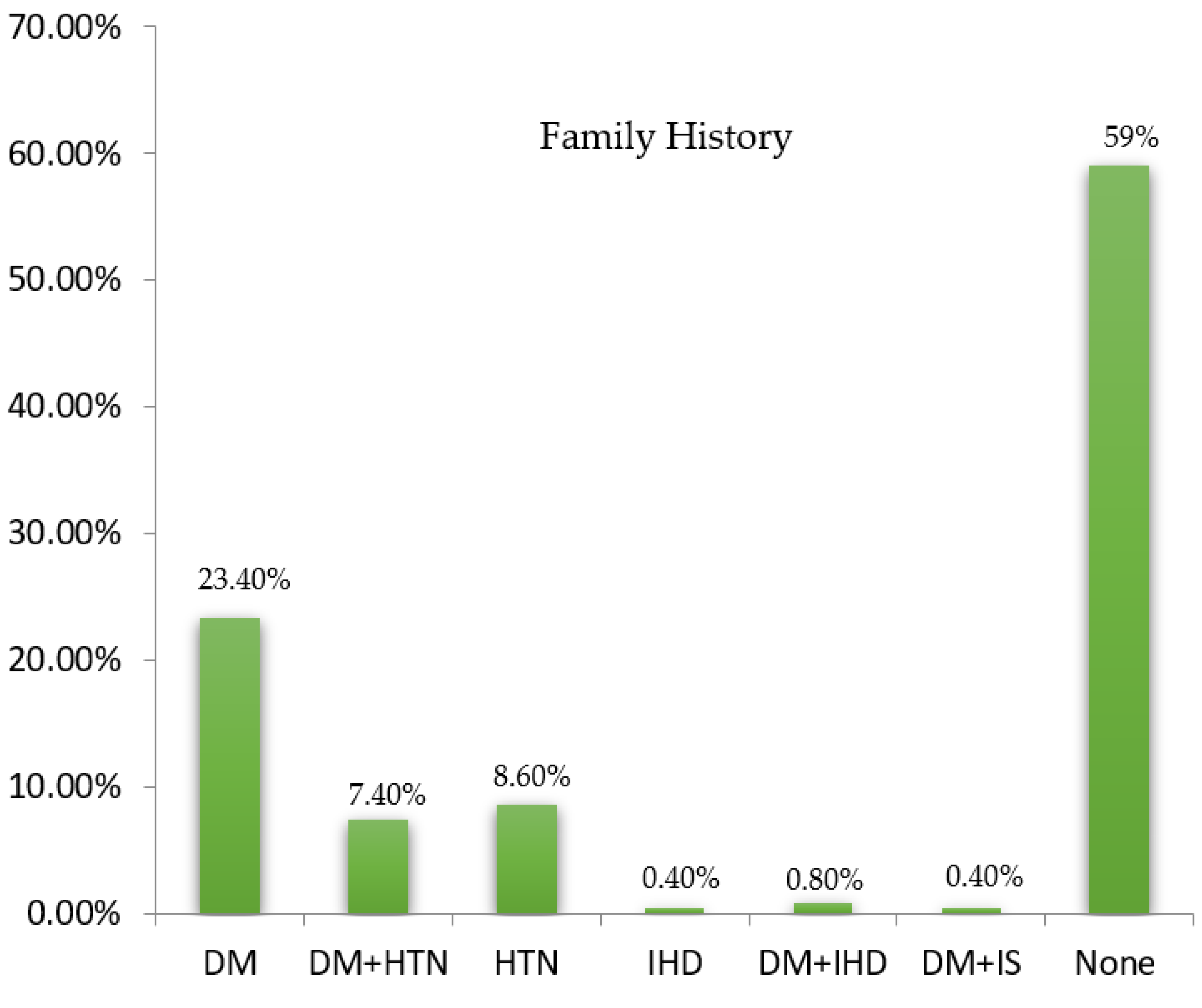
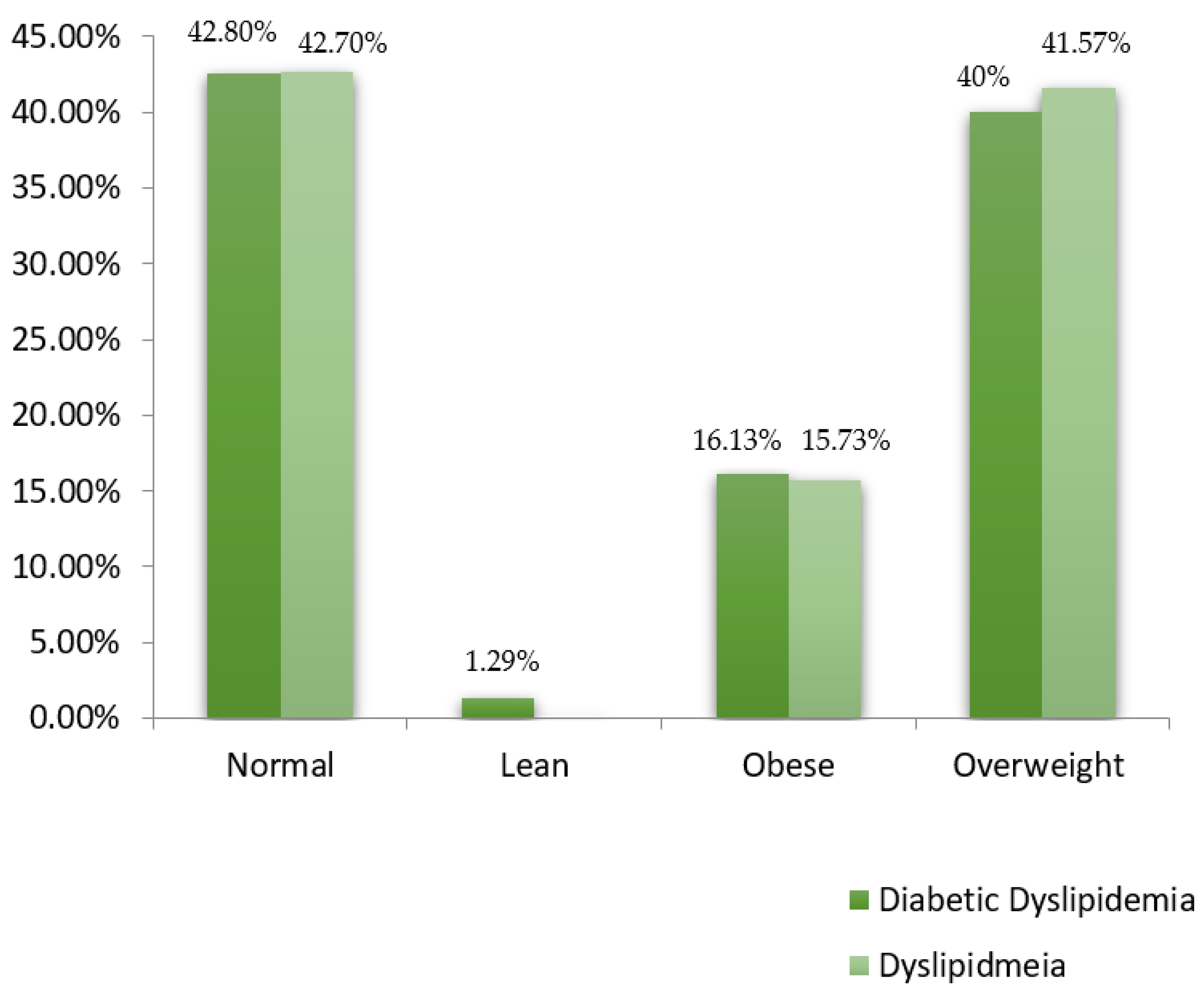
3.2. Demographic Analyses of Subjects
3.3. Statistical Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Noncommunicable Disease. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 25 May 2021).
- Chori, B.; Danladi, B.; Nwakile, P.; Okoye, I.; Abdullahi, U.; Zawaya, K.; Essien, I.; Sada, K.; Nwegbu, M.; Ogedengbe, J.; et al. Prevalence, patterns and predictors of dyslipidaemia in Nigeria: A report from the REMAH study. Cardiovasc. J. Afr. 2022, 33, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Soliman, H.; Ibrahim, A. Prevalence and pattern of dyslipidemia in an Egyptian children and adolescents with type1 diabetes. Egypt Pediatr. Assoc. Gaz. 2021, 69, 21. [Google Scholar] [CrossRef]
- Mahmoud, I.; Sulaiman, N. Dyslipidaemia prevalence and associated risk factors in the United Arab Emirates: A population-based study. BMJ Open. 2019, 9, e031969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, H.; Wang, H.; Shan, G.; Liu, R.; Chen, H.; Sun, S.; Liu, Y. Prevalence of dyslipidemia and associated risk factors among adult residents of Shenmu City, China. PLoS ONE 2021, 16, e0250573. [Google Scholar] [CrossRef] [PubMed]
- Shahwan, M.J.; Jairoun, A.A.; Farajallah, A.; Shanabli, S. Prevalence of dyslipidemia and factors affecting lipid profile in patients with type 2 diabetes. Diabetes Metab Syndr. Clin Res. Rev. 2019, 13, 2387–2392. [Google Scholar] [CrossRef]
- Sarfraz, M.; Sajid, S.; Ashraf, M.A. Prevalence and pattern of dyslipidemia in hyperglycemic patients and its associated factors among Pakistani population. Saudi. J. Biol. Sci. 2016, 23, 761–766. [Google Scholar] [CrossRef] [Green Version]
- Zaid, M.; Hasnain, S. Plasma lipid abnormalities in Pakistani population: Trends, associated factors, and clinical implications. Braz. J. Med. Biol. Res. 2018, 51, e7239. [Google Scholar] [CrossRef]
- Hedayatnia, M.; Asadi, Z.; Zare-Feyzabadi, R.; Yaghooti-Khorasani, M.; Ghazizadeh, H.; Ghaffarian-Zirak, R.; Nosrati-Tirkani, A.; Mohammadi-Bajgiran, M.; Rohban, M.; Sadabadi, F.; et al. Dyslipidemia and cardiovascular disease risk among the MASHAD study population. Lipids Health Dis. 2020, 19, 42. [Google Scholar] [CrossRef] [Green Version]
- Lee, Z.V.; Llanes, E.J.; Sukmawan, R.; Thongtang, N.; Ho, H.Q.T.; Barter, P. Prevalence of plasma lipid disorders with an emphasis on LDL cholesterol in selected countries in theAsia-Pacific region. Lipids. Health. Dis. 2021, 20, 33. [Google Scholar] [CrossRef]
- Raised Cholesterol-WHO Global Health Observatory (GHO) Data. Available online: https://ww.who.int/data/gho/indicator-metadata-registry/imr-details/3236 (accessed on 23 December 2021).
- Mohamed-Yassin, M.S.; Baharudin, N.; Daher, A.M.; Abu Bakar, N.; Ramli, A.S.; Abdul-Razak, S.; Mohamed Noor Khan, N.A.; Mohamad, M.; Yusoff, K. High prevalence of dyslipidaemia subtypes and their associated personal and clinical attributes in Malaysian adults: The REDISCOVER study. BMC. Cardiovas. Dis. 2021, 21, 149. [Google Scholar] [CrossRef]
- Shahid, S.U.; Sarwar, S. The abnormal lipid profile in obesity and coronary heart disease (CHD) in Pakistan is ubjects. Lipids Health Dis. 2020, 19, 73. [Google Scholar]
- Sultana, R. Impact of duration of type2 diabetes mellitus on lipid profile. Gomal. J. Med. Sci. 2018, 8, 57. [Google Scholar]
- Naheed, T.; Khan, A.; Masood, G.; Yunus, B.B.; Chaudry, M. Dyslipidemias in type II diabetes mellitus patients in a teaching hospital of Lahore, Pakistan. Pak. J. Med. Sci. 2003, 19, 283–286. [Google Scholar]
- Nadeem, A.; Mumtaz, S.; Naveed, A.K.; Aslam, M.; Siddiqui, A.; Lodhi, G.M. Pattern of dyslipidaemia and impact of increasing age and duration of type2 diabetes mellitus on dyslipidaemia, insulin levels and insulin resistance. J. Pak. Med. Assoc. 2015, 65, 928–932. [Google Scholar] [PubMed]
- Brady, R.P.; Shah, A.S.; Jensen, E.T.; Stafford, J.M.; D’Agostino, R.B.; Dolan, L.M.; Knight, L.; Imperatore, G.; Turley, C.B.; Liese, A.D.; et al. Glycemic control is associated with dyslipidemia overtime in youth with type2 diabetes: The SEARCH for diabetes in youth study. Pediatr. Diabetes. 2021, 22, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Naeem, N.; Butt, A.; Zafar, A.B.; Fawwad, A.; Tahir, B.; Basit, A. Dyslipidemia Pattern Among Newly Diagnosed and Known Type2 Diabetics: A Comparative Analysis from a Tertiary Care Hospital of Karachi, Pakistan. Pak. J. Med. Res. 2020, 59, 45–50. [Google Scholar]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Nelson, R.H. Hyperlipidemia as a risk factor for cardiovascular disease. Prim Care. Clin. Office Prac. 2013, 40, 195–211. [Google Scholar] [CrossRef] [Green Version]
- Park, J.B.; Kim, D.H.; Lee, H.; Hwang, I.C.; Yoon, Y.E.; Park, H.E.; Choi, S.Y.; Kim, Y.J.; Cho, G.Y.; Han, K.; et al. Mildly abnormal lipid levels, but not high lipid variability, are associated with increased risk of myocardial infarction and stroke in“statin-naive”young population a nationwide cohort study. Circ. Res. 2020, 126, 824–835. [Google Scholar] [CrossRef]
- Howard, B.V.; Ruotolo, G.; Robbins, D.C. Obesity and dyslipidemia. Endocrinol. Metab. Clin. 2003, 32, 855–867. [Google Scholar] [CrossRef]
- Kreisberg, R.A. Diabetic dyslipidemia. Am. J. Cardiol. 1998, 82, 67U–73U. [Google Scholar] [CrossRef]
- Kidwai, S.S.; Nageen, A.; Bashir, F.; Ara, J. HbA1c—A predictor of dyslipidemia in type2 Diabetes Mellitus. Pak. J. Med. Sci. 2020, 36, 1339–1343. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Nawaz, R.; Ghuman, F.D.; Hasan, S.M.; Iqbal, S.; Adnan, S.M. Frequency and pattern of dyslipidemia in diabetes mellitus type 2. Prof. Med. J. 2021, 28, 828–832. [Google Scholar]
- Li, Y.; Zhao, L.; Yu, D.; Ding, G. The prevalence and risk factors of dyslipidemia in different diabetic progression stages among middle-aged and elderly populations in China. PLoS ONE 2018, 13, e0205709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayram, F.; Kocer, D.; Gundogan, K.; Kaya, A.; Demir, O.; Coskun, R.; Sabuncu, T.; Karaman, A.; Cesur, M.; Rizzo, M.; et al. Prevalence of dyslipidemia and associated risk factors in Turkish adults. J. Clin. Lipidol. 2014, 8, 206–216. [Google Scholar] [CrossRef]
- Masilela, C.; Adeniyi, O.V.; Benjeddou, M. Prevalence, patterns and determinants of dyslipidaemia among South African adults with comorbidities. Sci. Rep. 2022, 12, 337. [Google Scholar] [CrossRef]
- Ahmad, B.; Aziz, K.; Hassan, N.U.; Kaiser, R.M.; Alvi, K.Y. Frequency of hypertriglyceridemia in newly diagnosed type 2 diabetics. Pak. Armed Forces J. 2016, 66, 88–91. [Google Scholar]
- Achila, O.O.; Araya, M.; Berhe, A.B.; Haile, N.H.; Tsige, L.K.; Shifare, B.Y.; Bitew, T.A.; Berhe, I.E.; Mengistu, S.T.; Yohaness, E.G. Dyslipidemia and associated risk factors in the elderly population in Asmara, Eritrea: Results from a community-based cross-sectional study. J. Lipids 2021, 2021, 6155304. [Google Scholar] [CrossRef]
- Qiu, L.; Wang, W.; Sa, R.; Liu, F. Prevalence and risk factors of hypertension, diabetes, and dyslipidemia among adults in Northwest China. Intl. J. Hypertens. 2021, 2021, 5528007. [Google Scholar] [CrossRef]
- Goyal, R.; Singhai, M.; Mahmood, T.; Saxena, V. Association between the physical activity and metabolic syndrome in residents of a foot-hill area in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102471. [Google Scholar] [CrossRef]
- Caselli, C.; De Caterina, R.; Smit, J.M.; Campolo, J.; El Mahdiui, M.; Ragusa, R.; Clemente, A.; Sampietro, T.; Clerico, A.; Liga, R.; et al. Triglycerides and low HDL cholesterol predict coronary heart disease risk in patients with stable angina. Sci. Rep. 2021, 11, 20714. [Google Scholar] [CrossRef] [PubMed]
- Shaya, G.E.; Leucker, T.M.; Jones, S.R.; Martin, S.S.; Toth, P.P. Coronary heart disease risk: Low-density lipoprotein and beyond. Trends. Cardiovasc. Med. 2021, 32, 181–194. [Google Scholar] [CrossRef] [PubMed]
- Kifle, Z.D.; Alehegn, A.A.; Adugna, M.; Bayleyegn, B. Prevalence and predictors of dyslipidemia among hypertensive patients in Lumame Primary Hospital, Amhara, Ethiopia: A cross-sectional study. Metab. Open 2021, 11, 100108. [Google Scholar] [CrossRef] [PubMed]
- Poorani, K.; Khokhar, N.A.; Kumar, P.; Goswami, P. Diabetic dyslipidemia and association of glycemic status with lipid profile, body mass index and abdominal obesity. Rawal. Med. J. 2020, 45, 265–268. [Google Scholar]
- Gao, J.; Wang, L.; Liang, H.; He, Y.; Zhang, S.; Wang, Y.; Li, Z.; Ma, Y. The association between a combination of healthy lifestyles and the risks of hypertension and dyslipidemia among adults-evidence from the northeast of China. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1138–1145. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Group I (Diabetic Dyslipidemia) | Group II (Dyslipidemia) | p-Value |
|---|---|---|---|
| Age (years) | 52.13 ± 10.75 | 47.33 ± 12.79 | 0.002 * |
| BMI (kg/m2) | 26.22 ± 4.53 | 26.76 ± 6.20 | 0.440 |
| FBS (mmol/L) | 11.54 ± 4.92 | 5.55 ± 0.47 | 0.000 * |
| HDL-C (mmol/L) | 0.79 ± 0.25 | 0.87 ± 0.24 | 0.035 * |
| LDL-C (mmol/L) | 2.96 ± 1.02 | 2.82 ± 0.96 | 0.287 |
| TC (mmol/L) | 5.09 ± 1.19 | 4.54 ± 1.33 | 0.001 * |
| Triglycerides (mmol/L) | 3.25 ± 1.99 | 2.41 ± 1.24 | 0.000 * |
| HbA1c (mmol/L) | 8.78 ± 2.14 | 5.38 ± 0.64 | 0.000 * |
| Parameter | R2 | Gender Male = 0, Female = 1 | Age | Socio−Economic Status | Family History | Physical Activity | BMI |
|---|---|---|---|---|---|---|---|
| HDL | 0.034 | 0.030 (−0.039, 0.099) | −0.002 (−0.004, 0.001) | 0.018 (−0.018, 0.054) | −0.005 (−0.017, 0.007) | −0.043 (−0.80, −0.006) | 0.000 (−0.042, 0.041) |
| p-value | 0.391 | 0.280 | 0.330 | 0.395 | 0.022 * | 0.994 | |
| LDL | 0.021 | 0.107 (−0.177, 0.391) | −0.004 (−0.015, 0.007) | −0.067 (−0.216, 0.082) | −0.024 (−0.073, 0.025) | −0.043 (−0.194, 0.109) | −0.090 (−0.260, 0.081) |
| p-value | 0.449 | 0.492 | 0.377 | 0.334 | 0.578 | 0.302 | |
| TGs | 0.039 | −0.633 (−1.135, −0.132) | −0.001 (−0.021, 0.09) | 0.120 (−0.143, 0.383) | −0.014 (−0.100, 0.072) | 0.163 (−0.104, 0.431) | 0.058 (−0.244, 0.359) |
| p-value | 0.014 * | 0.889 | 0.369 | 0.751 | 0.230 | 0.706 | |
| TC | 0.040 | 0.334 (−0.021, 0.689) | 0.008 (−0.006, 0.022) | −0.064 (−0.050, 0.122) | −0.062 (−0.123, −0.001) | −0.042 (−0.231, 0.148) | −0.135 (−0.348, 0.079) |
| p-value | 0.065 | 0.275 | 0.496 | 0.045 * | 0.665 | 0.215 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baig, Z.A.; Rashid, A.; Majeed, A.; Masood, Z.; Faryal, A.; Khan, Z.A.; Razaq, A. Risk Analysis and Assessment of Lipid Abnormalities as the Earliest Complication in Newly Diagnosed Diabetic and Non-Diabetic Individuals of a Local Population. Healthcare 2022, 10, 2308. https://doi.org/10.3390/healthcare10112308
Baig ZA, Rashid A, Majeed A, Masood Z, Faryal A, Khan ZA, Razaq A. Risk Analysis and Assessment of Lipid Abnormalities as the Earliest Complication in Newly Diagnosed Diabetic and Non-Diabetic Individuals of a Local Population. Healthcare. 2022; 10(11):2308. https://doi.org/10.3390/healthcare10112308
Chicago/Turabian StyleBaig, Zunaira Ali, Amir Rashid, Asifa Majeed, Zahra Masood, Asma Faryal, Zahra Arshad Khan, and Aden Razaq. 2022. "Risk Analysis and Assessment of Lipid Abnormalities as the Earliest Complication in Newly Diagnosed Diabetic and Non-Diabetic Individuals of a Local Population" Healthcare 10, no. 11: 2308. https://doi.org/10.3390/healthcare10112308