
Deep Learning Chest CT for Clinically Precise Prediction of Sepsis-Induced Acute Respiratory Distress Syndrome: A Protocol for an Observational Ambispective Cohort Study

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
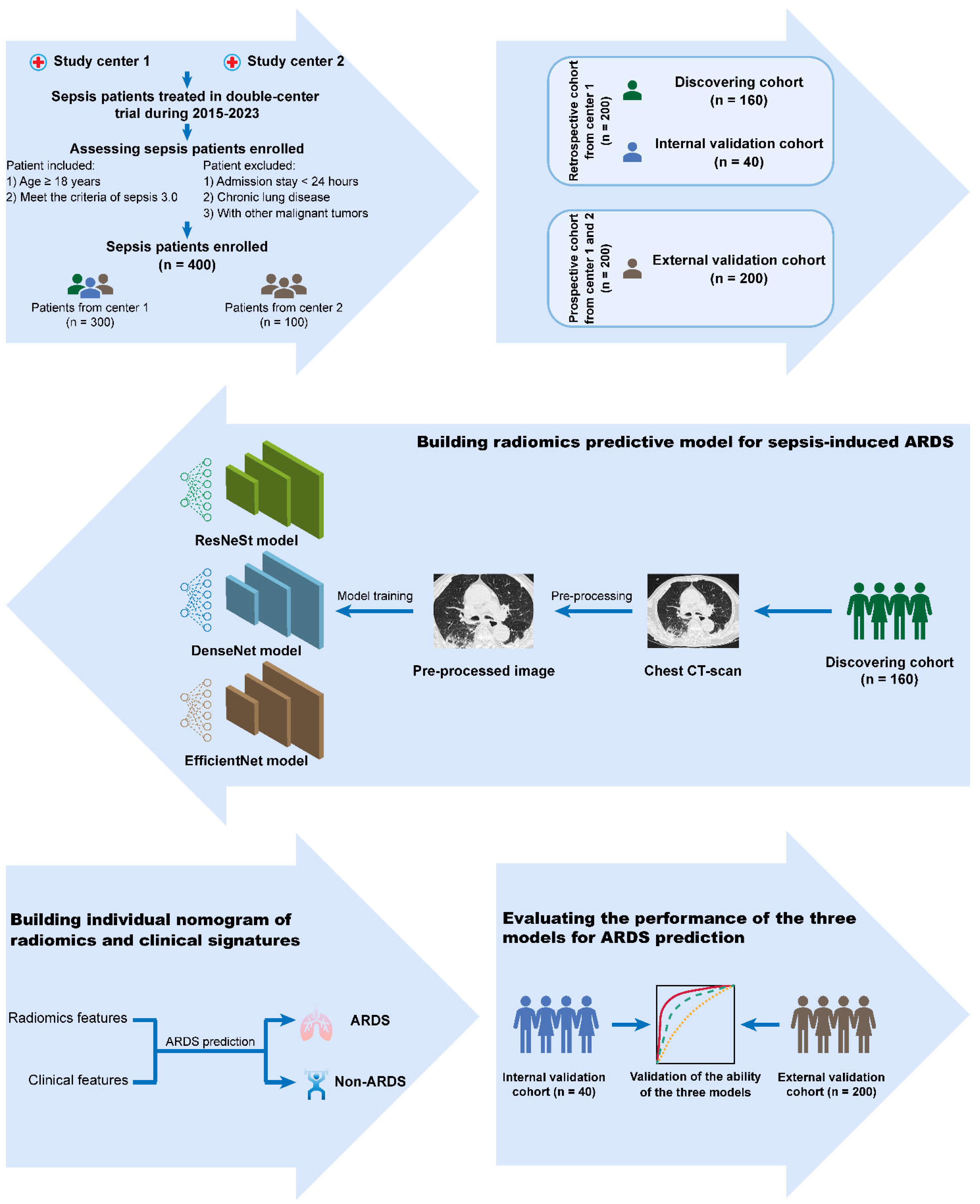
2.1. Study Design
2.2. Cohort Descriptions and Definitions
2.3. Sample Size Calculation
2.4. Data Collection
2.5. Work-Flow of Radiomics Analysis
2.6. Outcome Measures
- (1)
- Grade of pulmonary damage: patients will be classified as mild (200 < PaO2/FiO2 ≤ 300 mmHg), moderate (100 < PaO2/FiO2 ≤ 200 mmHg), or severe (PaO2/FiO2 ≤ 100 mmHg) at the moment of diagnosis of ARDS [2];
- (2)
- Ventilator-free days, VFD: defined as the number of days between successful weaning from mechanical ventilation and day 28 after ICU admission;
- (3)
- Respiratory organ failure-free days, RFFD: defined as the number of days between a day without evidence of respiratory organ failure [27];
- (4)
- 28-day mortality: all-cause mortality within 28 days following enrolment.
2.7. Statistical Analysis
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Su, G.; Atakilit, A.; Li, J.T.; Wu, N.; Bhattacharya, M.; Zhu, J.; Shieh, J.E.; Li, E.; Chen, R.; Sun, S.; et al. Absence of integrin alphavbeta3 enhances vascular leak in mice by inhibiting endothelial cortical actin formation. Am. J. Respir. Crit. Care Med. 2012, 185, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; ARDS Definition of Task Force; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zhang, M.; Girardi, C.; Bouhemad, B.; Kesecioglu, J.; Rouby, J.J. Computed tomography assessment of exogenous surfactant-induced lung reaeration in patients with acute lung injury. Crit. Care 2010, 14, R135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Pais, F.M.; Sinha, P.; Liu, K.D.; Matthay, M.A. Influence of Clinical Factors and Exclusion Criteria on Mortality in ARDS Observational Studies and Randomized Controlled Trials. Respir. Care 2018, 63, 1060–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajic, O.; Dabbagh, O.; Park, P.K.; Adesanya, A.; Chang, S.Y.; Hou, P.; Anderson, H.; Hoth, J.J.; Mikkelsen, M.E.; Gentile, N.T.; et al. Early identification of patients at risk of acute lung injury: Evaluation of lung injury prediction score in a multicenter cohort study. Am. J. Respir. Crit. Care Med. 2011, 183, 462–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Venet, F.; Monneret, G. Advances in the understanding and treatment of sepsis-induced immunosuppression. Nat. Rev. Nephrol. 2018, 14, 121–137. [Google Scholar] [CrossRef]
- Leissinger, M.; Kulkarni, R.; Zemans, R.L.; Downey, G.P.; Jeyaseelan, S. Investigating the role of nucleotide-binding oligomerization domain-like receptors in bacterial lung infection. Am. J. Respir. Crit. Care Med. 2014, 189, 1461–1468. [Google Scholar] [CrossRef] [Green Version]
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A. Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir. Med. 2014, 2, 611–620. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, P.; Goodwin, A.J.; Cook, J.A.; Halushka, P.V.; Chang, E.; Zingarelli, B.; Fan, H. Exosomes from endothelial progenitor cells improve outcomes of the lipopolysaccharide-induced acute lung injury. Crit. Care 2019, 23, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bos, L.D.; Schouten, L.R.; van Vught, L.A.; Wiewel, M.A.; Ong, D.; Cremer, O.; Artigas, A.; Martin-Loeches, I.; Hoogendijk, A.J.; van der Poll, T.; et al. Identification and validation of distinct biological phenotypes in patients with acute respiratory distress syndrome by cluster analysis. Thorax 2017, 72, 876–883. [Google Scholar] [CrossRef]
- Laffey, J.G.; Madotto, F.; Bellani, G.; Pham, T.; Fan, E.; Brochard, L.; Amin, P.; Arabi, Y.; Bajwa, E.K.; Bruhn, A.; et al. Geo-economic variations in epidemiology, patterns of care, and outcomes in patients with acute respiratory distress syndrome: Insights from the LUNG SAFE prospective cohort study. Lancet Respir. Med. 2017, 5, 627–638. [Google Scholar] [CrossRef] [Green Version]
- Fialkow, L.; Fochesatto, F.L.; Bozzetti, M.C.; Milani, A.R.; Rodrigues, F.E.; Ladniuk, R.M.; Pierozan, P.; de Moura, R.M.; Prolla, J.C.; Vachon, E.; et al. Neutrophil apoptosis: A marker of disease severity in sepsis and sepsis-induced acute respiratory distress syndrome. Crit. Care 2006, 10, R155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamarellos-Bourboulis, E.J.; Tsaganos, T.; Spyridaki, E.; Mouktaroudi, M.; Plachouras, D.; Vaki, I.; Karagianni, V.; Antonopoulou, A.; Veloni, V.; Giamarellou, H. Early changes of CD4-positive lymphocytes and NK cells in patients with severe Gram-negative sepsis. Crit. Care 2006, 10, R166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, M.A.; Datta, D.; Shankar-Hari, M.; Stephen, J.; Weir, C.J.; Rennie, J.; Antonelli, J.; Bateman, A.; Warner, N.; Judge, K.; et al. Cell-surface signatures of immune dysfunction risk-stratify critically ill patients: INFECT study. Intensiv. Care Med. 2018, 44, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Wang, D.C.; Huang, Q.; Wang, X. Significance of clinical phenomes of patients with COVID-19 infection: A learning from 3795 patients in 80 reports. Clin. Transl. Med. 2020, 10, 28–35. [Google Scholar] [CrossRef]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Cunliffe, A.; Armato, S.R.; Castillo, R.; Pham, N.; Guerrero, T.; Al-Hallaq, H.A. Lung texture in serial thoracic computed tomography scans: Correlation of radiomics-based features with radiation therapy dose and radiation pneumonitis development. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 1048–1056. [Google Scholar] [CrossRef]
- Sevransky, J.E.; Levy, M.M.; Marini, J.J. Mechanical ventilation in sepsis-induced acute lung injury/acute respiratory distress syndrome: An evidence-based review. Crit. Care Med. 2004, 32, S548–S553. [Google Scholar] [CrossRef] [PubMed]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005, 353, 1685–1693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Wu, C.R.; Zhang, Z.Y.; Zhu, Y.; Lin, H.B.; Zhang, Z.; Sun, Y.; He, T.; Mueller, J.; Manmatha, R.; et al. ResNeSt: Split-Attention Networks. arXiv 2020, arXiv:2004.08955. [Google Scholar]
- Iandola, F.; Moskewicz, M.; Karayev, S.; Girshick, R.; Darrell, T.; Keutzer, K. Densenet: Implementing efficient convnet descriptor pyramids. arXiv 2014, arXiv:1404.1869. [Google Scholar]
- Tan, M.; Le, Q.V. Efficientnet: Rethinking model scaling for convolutional neural networks. arXiv 2019, arXiv:1905.11946. [Google Scholar]
- Perkins, G.D.; Gates, S.; Park, D.; Gao, F.; Knox, C.; Holloway, B.; McAuley, D.F.; Ryan, J.; Marzouk, J.; Cooke, M.W.; et al. The beta agonist lung injury trial prevention. A randomized controlled trial. Am. J. Respir. Crit. Care Med. 2014, 189, 674–683. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Tibshirani, R. Regression shrinkage and selection via the LASSO. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Shekar, K.; Davies, A.R.; Mullany, D.V.; Tiruvoipati, R.; Fraser, J.F. To ventilate, oscillate, or cannulate? J. Crit. Care 2013, 28, 655–662. [Google Scholar] [CrossRef]
- Matthay, M.A.; McAuley, D.F.; Ware, L.B. Clinical trials in acute respiratory distress syndrome: Challenges and opportunities. Lancet Respir. Med. 2017, 5, 524–534. [Google Scholar] [CrossRef]
- Guerin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Davies, A.; Jones, D.; Bailey, M.; Beca, J.; Bellomo, R.; Blackwell, N.; Forrest, P.; Gattas, D.; Granger, E.; Jackson, A.; et al. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA 2009, 302, 1888–1895. [Google Scholar] [CrossRef] [PubMed]
- Trillo-Alvarez, C.; Cartin-Ceba, R.; Kor, D.J.; Kojicic, M.; Kashyap, R.; Thakur, S.; Thakur, L.; Herasevich, V.; Malinchoc, M.; Gajic, O. Acute lung injury prediction score: Derivation and validation in a population-based sample. Eur. Respir. J. 2011, 37, 604–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolinay, T.; Kim, Y.S.; Howrylak, J.; Hunninghake, G.M.; An, C.H.; Fredenburgh, L.; Massaro, A.F.; Rogers, A.; Gazourian, L.; Nakahira, K.; et al. Inflammasome-regulated cytokines are critical mediators of acute lung injury. Am. J. Respir. Crit. Care Med. 2012, 185, 1225–1234. [Google Scholar] [CrossRef] [Green Version]
- Kangelaris, K.N.; Prakash, A.; Liu, K.D.; Aouizerat, B.; Woodruff, P.G.; Erle, D.J.; Rogers, A.; Seeley, E.J.; Chu, J.; Liu, T.; et al. Increased expression of neutrophil-related genes in patients with early sepsis-induced ARDS. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 308, L1102–L1113. [Google Scholar] [CrossRef] [Green Version]
- Bos, L.; Scicluna, B.P.; Ong, D.; Cremer, O.; van der Poll, T.; Schultz, M.J. Understanding Heterogeneity in Biologic Phenotypes of Acute Respiratory Distress Syndrome by Leukocyte Expression Profiles. Am. J. Respir. Crit. Care Med. 2019, 200, 42–50. [Google Scholar] [CrossRef]
- Colen, R.R.; Fujii, T.; Bilen, M.A.; Kotrotsou, A.; Abrol, S.; Hess, K.R.; Hajjar, J.; Suarez-Almazor, M.E.; Alshawa, A.; Hong, D.S.; et al. Radiomics to predict immunotherapy-induced pneumonitis: Proof of concept. Investig. New Drugs 2018, 36, 601–607. [Google Scholar] [CrossRef]
- Hirano, Y.; Aziz, M.; Yang, W.L.; Wang, Z.; Zhou, M.; Ochani, M.; Khader, A.; Wang, P. Neutralization of osteopontin attenuates neutrophil migration in sepsis-induced acute lung injury. Crit. Care 2015, 19, 53. [Google Scholar] [CrossRef] [Green Version]
- Park, I.; Kim, M.; Choe, K.; Song, E.; Seo, H.; Hwang, Y.; Ahn, J.; Lee, S.-H.; Lee, J.H.; Jo, Y.H.; et al. Neutrophils disturb pulmonary microcirculation in sepsis-induced acute lung injury. Eur. Respir. J. 2019, 53, 1800786. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Gu, Y.; Liu, X.; Yi, X.; Li, Z.; Yu, Y.; Yu, T.; Li, L. Deep Learning Chest CT for Clinically Precise Prediction of Sepsis-Induced Acute Respiratory Distress Syndrome: A Protocol for an Observational Ambispective Cohort Study. Healthcare 2022, 10, 2150. https://doi.org/10.3390/healthcare10112150
Li H, Gu Y, Liu X, Yi X, Li Z, Yu Y, Yu T, Li L. Deep Learning Chest CT for Clinically Precise Prediction of Sepsis-Induced Acute Respiratory Distress Syndrome: A Protocol for an Observational Ambispective Cohort Study. Healthcare. 2022; 10(11):2150. https://doi.org/10.3390/healthcare10112150
Chicago/Turabian StyleLi, Han, Yang Gu, Xun Liu, Xiaoling Yi, Ziying Li, Yunfang Yu, Tao Yu, and Li Li. 2022. "Deep Learning Chest CT for Clinically Precise Prediction of Sepsis-Induced Acute Respiratory Distress Syndrome: A Protocol for an Observational Ambispective Cohort Study" Healthcare 10, no. 11: 2150. https://doi.org/10.3390/healthcare10112150