

Non-Communicable Diseases and Transitioning Health System in the Democratic People’s Republic of Korea during COVID-19 Lockdown

 , ,
, ,
Abstract
:1. Introduction
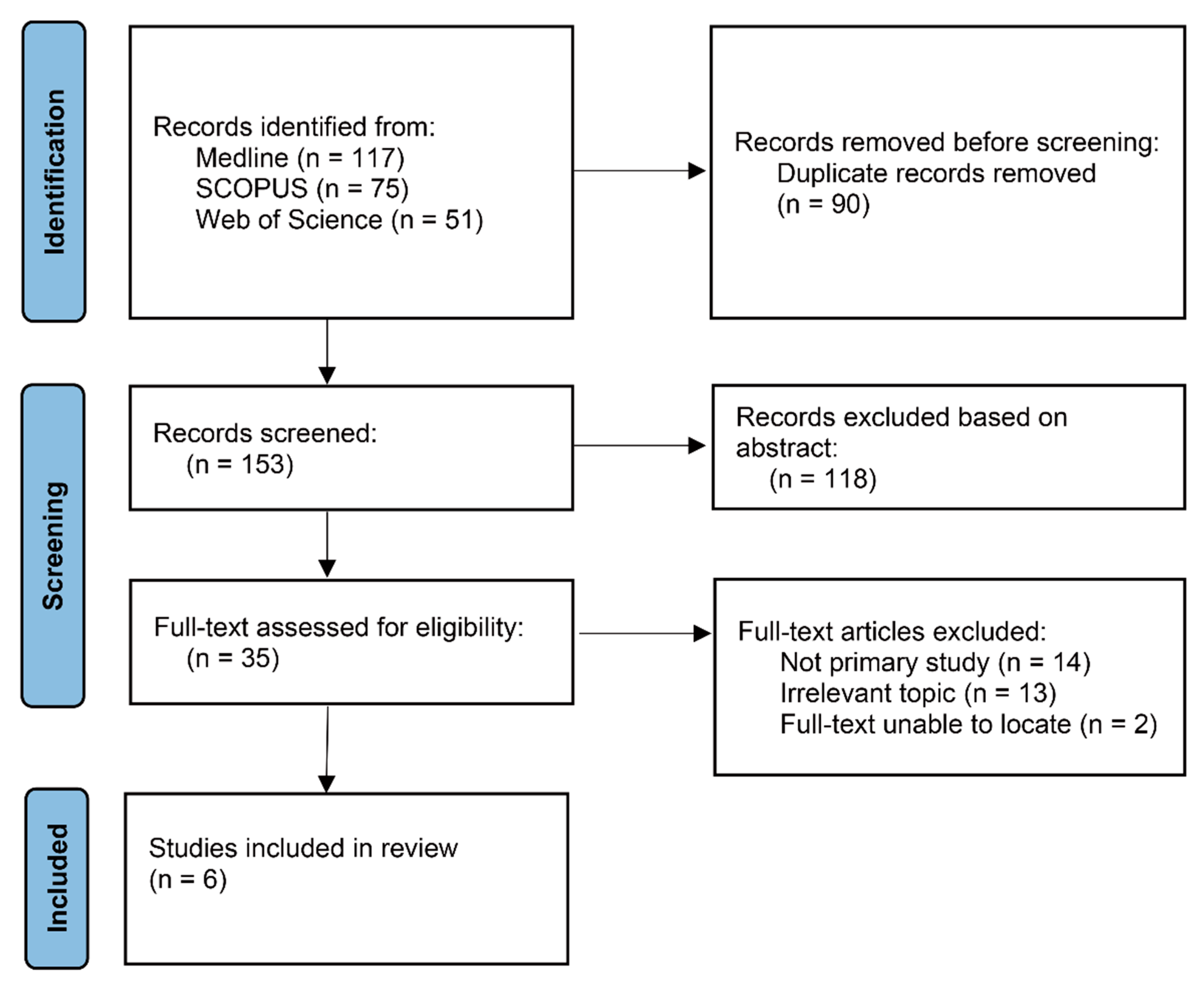
2. Materials and Methods
3. Results
3.1. Transitioning Health System with Financing Failure
3.2. NCDs and Changing Health Disparities

{kind=link}
| Reference | First Author (Published Year) | Study Population | Type of Study | Study Purpose | Main Results | Theme | ||
|---|---|---|---|---|---|---|---|---|
| NCDs Management Status and Policies Change | Health Inequality | Changes in Health Care System | ||||||
| [14] | Lee (2013) | Not applicable | Road map | To establish integrated health care system of Korea Peninsula |
| V | V | |
| [17] | Tran (2011) | 200 women in 6 provinces of DPRK | Cross-sectional study | To measure the level of knowledge and perception of women about cervical cancer |
| V | V | |
| [11] | Lee (2020) | 383 North Korean refugees | Cross-sectional study | To find socio-economic and political determinants of ill health and healthcare access in North Korea. |
| V | V | |
| [15] | Lee (2013) | National statistics of North Korea derived from WHO | Cross-sectional study | To evaluate the overall current disease burden of North Korea through the recent databases |
| V | ||
| [12] | Soh (2016) | 19 North Korean refugees | Cross-sectional study | To examine the emergence of informal healthcare practices in North Korea |
| V | ||
| [13] | Canaway (2017) | Not applicable | Field notes and photos | To impart reflections on North Korea’s healthcare system |
| V | ||
3.3. Impacts of COVID-19 Lockdown
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Key Concepts | Free Text/Natural Language | Controlled Vocabulary (MESH) | |
|---|---|---|---|
| Concept 1 | Health |
|
|
|
| ||
|
| ||
|
| ||
|
| ||
|
| ||
| Concept 2 | Policy |
|
|
|
| ||
|
| ||
| Concept 3 | North Korea |
|
|
Appendix B. Selected Literature of This Review
References
- Martinez, R.; Lloyd-Sherlock, P.; Soliz, P.; Ebrahim, S.; Vega, E.; Ordunez, P.; McKee, M. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990–2017: A population-based study. Lancet Glob. Health 2020, 8, e511–e523. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging (Albany NY) 2020, 12, 6049. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Moore, J.T.; Pilkington, W.; Kumar, D. Diseases with health disparities as drivers of COVID-19 outcome. J. Cell Mol. Med. 2020, 24, 11038–11045. [Google Scholar] [CrossRef] [PubMed]
- Team, E. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. CCDC Weekly 2020, 2, 113. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, Z. Estimation of COVID-19 prevalence in Italy, Spain, and France. Sci. Total Environ 2020, 729, 138817. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018. WHO 2018. License: CC BY-NC-SA 3.0 IGO. Available online: https://apps.who.int/iris/handle/10665/274512 (accessed on 26 September 2022).
- Azarpazhooh, M.R.; Morovatdar, N.; Avan, A.; Phan, T.G.; Divani, A.A.; Yassi, N.; Stranges, S.; Silver, B.; Biller, J.; Belasi, M.T. COVID-19 pandemic and burden of non-communicable diseases: An ecological study on data of 185 countries. J. Stroke Cerebrovasc. Dis. 2020, 29, 105089. [Google Scholar] [CrossRef]
- Robinson, W.C.; Cha, J.; Park, S.; Branchini, C.; Kim, D.; Kim, S.Y.; Kim, T. Lost Generation: The Health and Human Rights of North Korean Children, 1990–2018; Committee for Human Rights in North Korea: Washington, DC, USA, 2019. [Google Scholar]
- Lee, H.; Robinson, C.; Kim, J.; McKee, M.; Cha, J. Health and healthcare in North Korea: A retrospective study among defectors. Confl. Health 2020, 14, 1–8. [Google Scholar] [CrossRef]
- Soh, E.J. The emergence of an informal health-care sector in North Korea. Networks 2016, 14, 3. [Google Scholar]
- Canaway, R. Integration of traditional and ‘modern’ medicine: Reflections on a visit to DPR Korea. Eur. J. Integr. Med. 2017, 15, 32–38. [Google Scholar] [CrossRef]
- Lee, Y.H.; Yoon, S.-J.; Kim, S.H.; Shin, H.-W.; Lee, J.Y.; Kim, B.; Kim, Y.A.; Yoon, J.; Shin, Y.S. A strategy toward reconstructing the healthcare system of a unified Korea. J. Prev. Med. Public Health 2013, 46, 134. [Google Scholar] [CrossRef]
- Lee, Y.H.; Yoon, S.-J.; Kim, Y.A.; Yeom, J.W.; Oh, I.-H. Overview of the burden of diseases in North Korea. J. Prev. Med. Public Health 2013, 46, 111. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Lee, Y.H. Underestimated burden: Non-communicable diseases in North Korea. Yonsei Med. J. 2019, 60, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.T.; Choe, S.I.; Taylor, R.; Ko, W.S.; Pyo, H.S.; So, H.C. Knowledge, attitude and practice (KAP) concerning cervical cancer and screening among rural and urban women in six provinces of the Democratic People’s Republic of Korea. Asian Pac. J. Cancer Prev. 2011, 12, 3029–3033. [Google Scholar]
- Kluge, H.H.P.; Wickramasinghe, K.; Rippin, H.L.; Mendes, R.; Peters, D.H.; Kontsevaya, A.; Breda, J. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet 2020, 395, 1678–1680. [Google Scholar] [CrossRef]
- Hastings, J.V.; Wertz, D.; Yeo, A. Market Activities & the Building Blocks of Civil Society in North Korea; NCNK: Washington, DC, USA, 2021. [Google Scholar]
- Noland, M. The (non-) impact of UN sanctions on North Korea. Asia Policy 2009, 7, 61–88. [Google Scholar] [CrossRef] [Green Version]
- Amnesty International. The Crumbling State of Health Care in North Korea; Amnesty International Publications: London, UK, 2010. [Google Scholar]
- Park, K.B.; Ham, E.I. North Korea’s Surprisingly Robust Healthcare System. Global Asia 2021, 16, 66–72. [Google Scholar]
- Shin, H.-Y.; Shin, J.E.; Baek, S.Y.; Chu, S.H. Promoting health behaviors for preventing and controlling noncommunicable disease among North Korean defectors: A systematic review. Europe Pub. Med. Cent. 2020. [Google Scholar] [CrossRef]
- Devi, S. North Korean health at risk due to border closures. Lancet 2021, 398, 13. [Google Scholar] [CrossRef]
- WHO. COVID-19 Significantly Impacts Health Services for Noncommunicable Diseases. 2020. Available online: https://www.who.int/news/item/01-06-2020-covid-19-significantly-impacts-health-services-for-noncommunicable-diseases (accessed on 26 September 2022).
- Yadav, U.N.; Rayamajhee, B.; Mistry, S.K.; Parsekar, S.S.; Mishra, S.K. A syndemic perspective on the management of non-communicable diseases amid the COVID-19 pandemic in low-and middle-income countries. Front. Public Health 2020, 8, 508. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 26 September 2022).
- Choi, J.-P. Medical education for North Korean defector physicians: Experience at the Seoul Medical Center. KMER 2012, 14, 95–101. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Maddikunta, P.K.R.; Pham, Q.-V.; Gadekallu, T.R.; Chowdhary, C.L.; Alazab, M.; Piran, M.J. Deep learning and medical image processing for coronavirus (COVID-19) pandemic: A survey. Sustain. Cities Soc. 2021, 65, 102589. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, J.-W.; Kim, K.-B.; Jang, H.-E.; Heo, M.-H.; Kim, Y.-J.; Cha, J. Non-Communicable Diseases and Transitioning Health System in the Democratic People’s Republic of Korea during COVID-19 Lockdown. Healthcare 2022, 10, 2095. https://doi.org/10.3390/healthcare10102095
Noh J-W, Kim K-B, Jang H-E, Heo M-H, Kim Y-J, Cha J. Non-Communicable Diseases and Transitioning Health System in the Democratic People’s Republic of Korea during COVID-19 Lockdown. Healthcare. 2022; 10(10):2095. https://doi.org/10.3390/healthcare10102095
Chicago/Turabian StyleNoh, Jin-Won, Kyoung-Beom Kim, Ha-Eun Jang, Min-Hee Heo, Young-Jin Kim, and Jiho Cha. 2022. "Non-Communicable Diseases and Transitioning Health System in the Democratic People’s Republic of Korea during COVID-19 Lockdown" Healthcare 10, no. 10: 2095. https://doi.org/10.3390/healthcare10102095