
One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Variables
2.3. Analysis
2.4. Statistical Analysis
3. Results
3.1. Description of the Two Groups
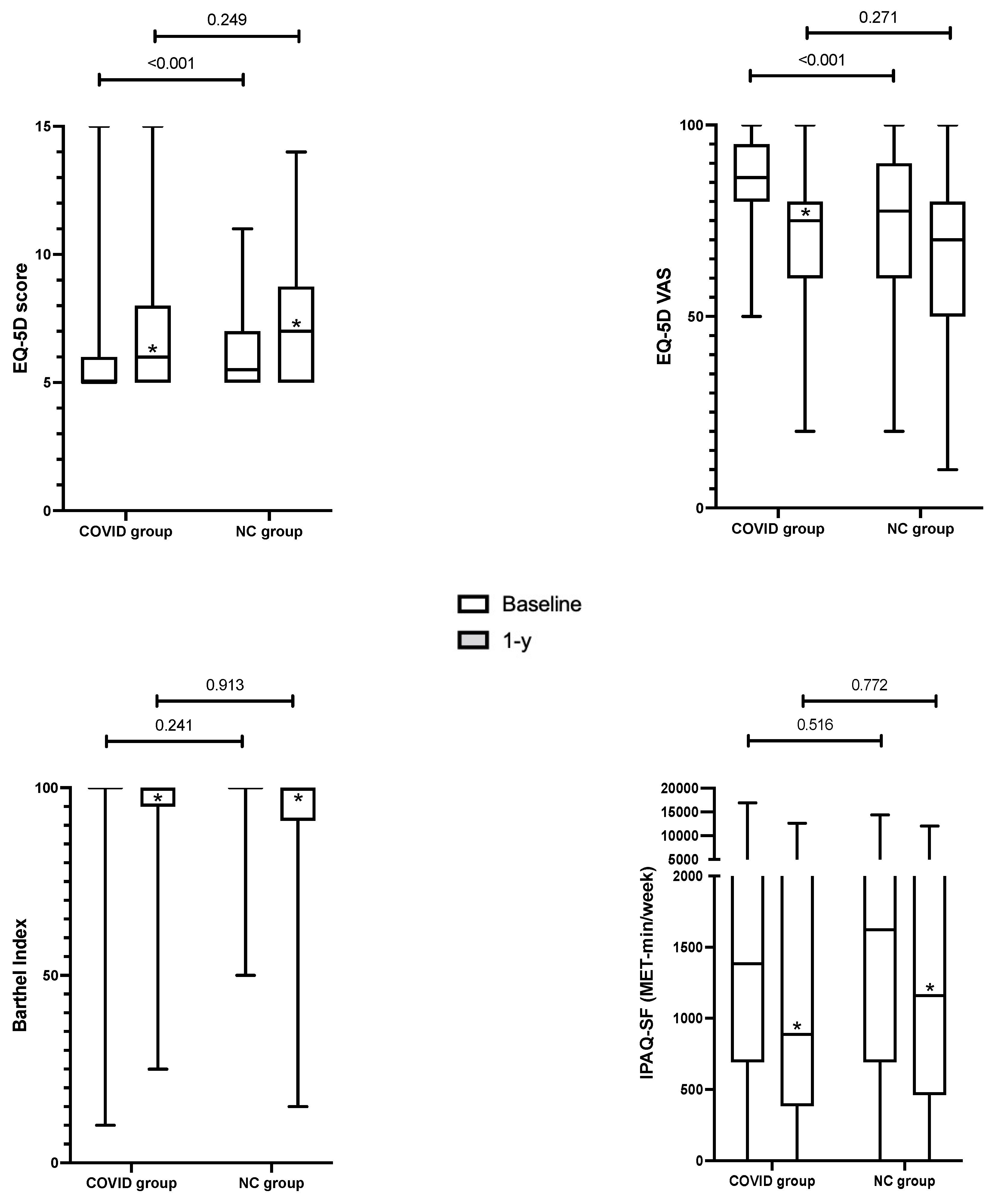
3.2. One-Year Outcomes
3.3. Subgroup Analysis According to Mechanical Ventilation and Inpatient Rehabilitation
3.4. Subgroup Analysis in the COVID Group: Wave 1 vs. Wave 2
3.5. Risk Factors of Functional Decline
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rousseau, A.F.; Prescott, H.C.; Brett, S.J.; Weiss, B.; Azoulay, E.; Creteur, J.; Latronico, N.; Hough, C.L.; Weber-Carstens, S.; Vincent, J.-L.; et al. Long-term outcomes after critical illness: Recent insights. Crit. Care 2021, 25, 108. [Google Scholar] [CrossRef] [PubMed]
- Lambermont, B.; Rousseau, A.F.; Seidel, L.; Thys, M.; Cavalleri, J.; Delanaye, P.; Chase, J.G.; Gillet, P.; Misset, B. Outcome Improvement Between the First Two Waves of the Coronavirus Disease 2019 Pandemic in a Single Tertiary-Care Hospital in Belgium. Crit. Care Explor. 2021, 3, e0438. [Google Scholar] [CrossRef] [PubMed]
- Martillo, M.A.; Dangayach, N.S.; Tabacof, L.; Spielman, L.A.; Dams-O’Connor, K.; Chan, C.C.; Kohli-Seth, R.; Cortes, M.; Escalon, M.X. Postintensive Care Syndrome in Survivors of Critical Illness Related to Coronavirus Disease 2019: Cohort Study From a New York City Critical Care Recovery Clinic. Crit. Care Med. 2021, 49, 1427–1438. [Google Scholar] [CrossRef] [PubMed]
- Writing Committee for the CSG; Morin, L.; Savale, L.; Pham, T.; Colle, R.; Figueiredo, S.; Harrois, A.; Gasnier, M.; Lecoq, A.-L.; Meyrignac, O.; et al. Four-Month Clinical Status of a Cohort of Patients After Hospitalization for COVID-19. JAMA 2021, 325, 1525–1534. [Google Scholar]
- Valent, A.; Dudoignon, E.; Ressaire, Q.; Depret, F.; Plaud, B. Three-month quality of life in survivors of ARDS due to COVID-19: A preliminary report from a French academic centre. Anaesth. Crit. Care Pain Med. 2020, 39, 740–741. [Google Scholar] [CrossRef]
- Gamberini, L.; Mazzoli, C.A.; Sintonen, H.; Colombo, D.; Scaramuzzo, G.; Allegri, D.; Tonetti, T.; Zani, G.; Capozzi, C.; Giampalma, E.; et al. Quality of life of COVID-19 critically ill survivors after ICU discharge: 90 days follow-up. Qual. Life Res. 2021, 30, 2805–2817. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Latronico, N.; Peli, E.; Calza, S.; Rodella, F.; Novelli, M.P.; Cella, A.; Marshall, J.; Needham, D.M.; Rasulo, F.A.; Piva, S. Physical, cognitive and mental health outcomes in 1-year survivors of COVID-19-associated ARDS. Thorax 2021, 77, 300–303. [Google Scholar] [CrossRef]
- Darcis, G.; Bouquegneau, A.; Maes, N.; Thys, M.; Henket, M.; Labye, F.; Rousseau, A.F.; Canivet, P.; Desir, C.; Calmes, D.; et al. Long-term clinical follow-up of patients suffering from moderate-to-severe COVID-19 infection: A monocentric prospective observational cohort study. Int. J. Infect. Dis. 2021, 109, 209–216. [Google Scholar] [CrossRef]
- Heesakkers, H.; van der Hoeven, J.G.; Corsten, S.; Janssen, I.; Ewalds, E.; Simons, K.S.; Westerhof, B.; Rettig, T.C.D.; Jacobs, C.; van Santen, S.; et al. Clinical Outcomes Among Patients With 1-Year Survival Following Intensive Care Unit Treatment for COVID-19. JAMA 2022, 327, 559–565. [Google Scholar] [CrossRef]
- Bels, J.L.M.; van Gassel, R.J.J.; Timmerman, L.; Hemmen, B.; van de Poll, M.C.G.; Peters, N.; Spruit, M.A.; van Santen, S.; Gietema, H.A.; Posthuma, R. One-year Outcomes of Mechanically Ventilated COVID-19 ICU Survivors: A Prospective Cohort Study. Am. J. Respir. Crit. Care Med. 2022, 206, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Eberst, G.; Claude, F.; Laurent, L.; Meurisse, A.; Roux-Claude, P.; Barnig, C.; Vernerey, D.; Paget-Bailly, S.; Bouiller, K.; Chirouze, C.; et al. Result of one-year, prospective follow-up of intensive care unit survivors after SARS-CoV-2 pneumonia. Ann. Intensive Care 2022, 12, 23. [Google Scholar] [CrossRef] [PubMed]
- Bein, T.; Weber-Carstens, S.; Apfelbacher, C. Long-term outcome after the acute respiratory distress syndrome: Different from general critical illness? Curr. Opin. Crit. Care 2018, 24, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Demoule, A.; Morawiec, E.; Decavele, M.; Ohayon, R.; Malrin, R.; Galarza-Jimenez, M.A.; Laveneziana, P.; Morelot-Panzini, C.; Similowski, T.; De Rycke, Y.; et al. Health-related quality of life of COVID-19 two and 12 months after intensive care unit admission. Ann. Intensive Care 2022, 12, 16. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Suri, R.; Suchyta, M.R.; Digrande, K.F.; Sherwood, K.D.; Colantuoni, E.; Dinglas, V.D.; Needham, D.M.; Hopkins, R.O. Return to work after critical illness: A systematic review and meta-analysis. Thorax 2020, 75, 17–27. [Google Scholar] [CrossRef]
- Hodgson, C.L.; Higgins, A.M.; Bailey, M.J.; Mather, A.M.; Beach, L.; Bellomo, R.; Bissett, B.; Boden, I.J.; Bradle, S.; Burrell, A.; et al. Comparison of 6-Month Outcomes of COVID-19 vs Non-COVID-19 Survivors of Critical Illness. Am. J. Respir. Crit. Care Med. 2022, 205, 1159–1168. [Google Scholar] [CrossRef]
- Herridge, M.S.; Moss, M.; Hough, C.L.; Hopkins, R.O.; Rice, T.W.; Bienvenu, O.J.; Azoulay, E. Recovery and outcomes after the acute respiratory distress syndrome (ARDS) in patients and their family caregivers. Intensive Care Med. 2016, 42, 725–738. [Google Scholar] [CrossRef]
- O’Brien, K.; Townsend, L.; Dowds, J.; Bannan, C.; Nadarajan, P.; Kent, B.; Murphy, N.; Sheill, G.; Martin-Loeches, I.; Guinan, E. 1-year quality of life and health-outcomes in patients hospitalised with COVID-19: A longitudinal cohort study. Respir. Res. 2022, 23, 115. [Google Scholar] [CrossRef] [PubMed]
- Sommers, J.; Engelbert, R.H.; Dettling-Ihnenfeldt, D.; Gosselink, R.; Spronk, P.E.; Nollet, F.; van der Schaaf, M. Physiotherapy in the intensive care unit: An evidence-based, expert driven, practical statement and rehabilitation recommendations. Clin. Rehabil. 2015, 29, 1051–1063. [Google Scholar] [CrossRef] [PubMed]
- Tymkew, H.; Sledge, J.A.; Vyers, K.; Arroyo, C.; Schallom, M. One Year Post-Discharge Outcomes After Implementation of an ICU Early Mobility Protocol. Dimens. Crit. Care Nurs. 2022, 41, 209–215. [Google Scholar] [CrossRef]
- Gamberini, L.; Mazzoli, C.A.; Prediletto, I.; Sintonen, H.; Scaramuzzo, G.; Allegri, D.; Colombo, D.; Tonetti, T.; Zani, G.; Capozzi, C.; et al. Health-related quality of life profiles, trajectories, persistent symptoms and pulmonary function one year after ICU discharge in invasively ventilated COVID-19 patients, a prospective follow-up study. Respir. Med. 2021, 189, 106665. [Google Scholar] [CrossRef]
- Zangrillo, A.; Belletti, A.; Palumbo, D.; Calvi, M.R.; Guzzo, F.; Fominskiy, E.V.; Ortalda, A.; Nardelli, P.; Ripa, M.; Redaelli, M.B.; et al. One-Year Multidisciplinary Follow-Up of Patients With COVID-19 Requiring Invasive Mechanical Ventilation. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.S.; Aronson Friedman, L.; Dinglas, V.D.; Hough, C.L.; Shanholtz, C.; Ely, E.W.; Morris, P.E.; Mendez-Tellez, P.A.; Jackson, J.C.; Hopkins, R.O.; et al. Are physical measures related to patient-centred outcomes in ARDS survivors? Thorax 2017, 72, 884–892. [Google Scholar] [CrossRef] [PubMed]
- McPeake, J.; Bateson, M.; Christie, F.; Robinson, C.; Cannon, P.; Mikkelsen, M.; Iwashyna, T.J.; Leyland, A.H.; Shaw, M.; Quasim, T. Hospital re-admission after critical care survival: A systematic review and meta-analysis. Anaesthesia 2022, 77, 475–485. [Google Scholar] [CrossRef]
- Weinfurt, K.P.; Reeve, B.B. Patient-Reported Outcome Measures in Clinical Research. JAMA 2022, 328, 472–473. [Google Scholar] [CrossRef]
- Lawson, A.; Tan, A.C.; Naylor, J.; Harris, I.A. Is retrospective assessment of health-related quality of life valid? BMC Musculoskelet. Disord. 2020, 21, 415. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data | COVID Group n = 132 | NC Group n = 88 | p Value | |
|---|---|---|---|---|
| Age, y | 64 [54–70] | 66 [57–72.5] | 0.13 | |
| Male, n (%) | 85 (64.4) | 63 (71.6) | 0.20 | |
| Weight, kg | 88.4 [78.5–100] | 76 [68–90] | <0.001 | |
| BMI, kg/m2 | 30.3 [26.5–34] | 26.7 [23.1–30.3] | <0.001 | |
| Comorbidities, n (%) | Cardiovascular a | 49 (37.1) | 67 (76.1) | <0.001 |
| Hypertension b | 82 (62.1) | 62 (70.5) | 0.20 | |
| Respiratory | 28 (21.2) | 19 (21.6) | 0.95 | |
| Chronic kidney disease | 19 (14.4) | 10 (11.4) | 0.52 | |
| Diabetes | 62 (47) | 23 (26.1) | 0.002 | |
| Immunosuppression | 6 (4.5) | 2 (2.3) | 0.48 | |
| Retired before ICU admission, n (%) | 70 (53) | 54 (61.4) | 0.22 | |
| Admission type, n (%) | Medical | 132 (100) | 33 (37.5) | |
| Surgical | - | 55 (62.5) | ||
| Admission failure, n (%) | Cardiovascular | - | 48 (54.5) | |
| Pulmonary | 132 (100) | 10 (11.4) | ||
| Neurologic | - | 10 (11.4) | ||
| Other | - | 20 (22.7) | ||
| SOFA at admission | 4 [3–6] | 3 [1–5] | 0.011 | |
| SAPS II | 34 [26–46] | 29 [23–36] | 0.024 | |
| Mechanical ventilation, n (%) | 62 (46.9) | 47 (53.4) | 0.35 | |
| Duration of mechanical ventilation, d | 13 [8–23] | 1 [1–2] | <0.001 | |
| Neuromuscular blocking agent, n(%) | 34 (25.8) | 12 (13.6) | 0.030 | |
| Duration of NMBA, d | 3 [2–4] | 1 [1–3] | 0.021 | |
| Tracheostomy, n (%) | 15 (11.3) | 2 (2.3) | 0.013 | |
| Vasopressor support, n (%) | 46 (34.8) | 33 (37.5) | 0.69 | |
| Duration of norepinephrine administration, d | 3 [2–9] | 1 [1–2] | <0.001 | |
| Renal replacement therapy, n (%) | 10 (7.6) | 2 (2.2) | 0.13 | |
| Duration of renal replacement therapy, d | 19 [18–35] | 3 and 9 | ||
| Extracorporeal membrane oxygenation, n (%) | 0 | 1 (1.1) | 0.40 | |
| Duration of ECMO, d | - | 3 | ||
| ICU LOS, d | 8.5 [4.5–20] | 2 [2–4] | <0.001 | |
| Hospital LOS, d | 22 [12–42] | 11 [8–24] | <0.001 | |
| Destination at hospital discharge, n (%) | Home | 83 (62.9) | 66 (75) | 0.071 |
| Rehabilitation facility | 44 (33.3) | 17 (19.3) | ||
| Other | 5 (3.8) | 5 (5.7) | ||
| Data | COVID Group n = 132 | NC Group n = 88 | p Value | |
|---|---|---|---|---|
| Return to previous level of activities, n (%) | 76 (57.5) | 45 (51.1) | 0.407 | |
| At least one hospital readmission, n (%) | 34 (25.7) | 41 (46.6) | 0.002 | |
| Reason for the first readmission, n (%) | Cardio-vascular | 9 (26.5) | 11 (26.9) | |
| Pulmonary | 3 (8.8) | 1 (2.4) | ||
| Neurologic | 1 (2.9) | 8 (19.5) | ||
| Trauma | 4 (11.8) | 1 (2.4) | ||
| Scheduled surgery | 7 (20.6) | 3 (7.3) | ||
| Sepsis | 7 (20.6) | 6 (14.6) | ||
| Other | 3 (8.8) | 11 (26.9) | ||
| At least one fall, n (%) | 16 (12.1) | 13 (14.8) | 0.685 | |
| At least one fracture, n (%) | 3 (2.3) | 5 (5.7) | 0.271 | |
| Data | COVID Group n = 132 | NC Group n = 88 | |||
|---|---|---|---|---|---|
| MV (n = 62) | Non-MV (n = 70) | MV (n = 47) | Non-MV (n = 41) | ||
| Return to previous level of activities, n (%) | 33 (53.2) | 42 (60) | 25 (53.2) | 20 (48.8) | |
| p = 0.483 | p = 0.831 | ||||
| At least one hospital readmission, n (%) | 18 (29) | 14 (20) | 26 (55.3) | 15 (36.6) | |
| p = 0.309 | p = 0.091 | ||||
| At least one fall, n (%) | 11 (17.7) | 5 (7.1) | 5 (10.6) | 8 (19.5) | |
| p = 0.107 | p = 0.38 | ||||
| At least one fracture, n (%) | 3 (4.8) | 0 | 2 (4.3) | 3 (7.3) | |
| p = 0.101 | p = 0.661 | ||||
| EQ-5D score | baseline | 5 [5–6] | 5 [5–5] | 6 [5–7] | 5 [5–7] |
| 1-y | 7 [6–9] * | 6 [5–7] * | 7 [6–9] * | 7 [5–8] * | |
| EQ-5D VAS | baseline | 90 [80–100] | 85 [73.8–90] | 75 [60–90] | 80 [60–85] |
| 1-y | 72.5 [60–80] * | 75 [60–89.2] * | 75 [50–80] | 70 [60–82.5] | |
| Barthel Index | baseline | 100 [100–100] | 100 [100–100] | 100 [100–100] | 100 [100–100] |
| 1-y | 97.5 [90–100] * | 100 [98.7–100] * | 100 [90–100] * | 100 [95–100] * | |
| IPAQ-SF (MET-min/week) | baseline | 1248 [678.8–3959] | 1413 [689.3–2410] | 1512 [693–3115] | 1732 [693–3333] |
| 1-y | 784.5 [333.8–2946] * | 1093 [427.5–1985] * | 900 [462–2079] * | 1386 [288.5–2948] | |
| Data | COVID Group n = 132 | NC Group n = 88 | |||
|---|---|---|---|---|---|
| Rehab (n = 44) | No Rehab (n = 88) | Rehab (n = 17) | No Rehab (n = 71) | ||
| Return to previous level of activities, n (%) | 19 (43.2) | 57 (64.8) | 7 (41.2) | 38 (53.5) | |
| p = 0.025 | p = 0.424 | ||||
| At least one hospital readmission, n (%) | 15 (34.1) | 19 (21.6) | 8 (47.1) | 33 (46.5) | |
| p = 0.142 | p > 0.999 | ||||
| At least one fall, n (%) | 9 (20.4) | 7 (7.9) | 4 (23.5) | 9 (12.7) | |
| p = 0.049 | p = 0.267 | ||||
| At least one fracture, n (%) | 2 (4.5) | 1 (1.1) | 1 (5.9) | 4 (5.6) | |
| p = 0.258 | p > 0.999 | ||||
| EQ-5D score | baseline | 5 [5–5] | 5 [5–6] | 6 [5–7] | 5 [5–7] |
| 1-y | 7.5 [6–9] * | 6 [5–7.8] *,‡ | 8 [6–10] * | 7 [5–8] * | |
| EQ-5D VAS | baseline | 90 [80–100] | 85 [75.2–93.7] | 80 [60–90] | 75 [60–90] |
| 1-y | 70 [52.5–80] * | 75 [65–85] *,‡ | 70 [45–75] * | 70 [60–80] | |
| Barthel Index | baseline | 100 [100–100] | 100 [100–100] | 100 [100–100] | 100 [100–100] |
| 1-y | 95 [85–100] * | 100 [95–100] *,‡ | 100 [77.5–100] * | 100 [95–100] * | |
| IPAQ-SF (MET-min/week) | baseline | 1494 [743.6–3968] | 1293 [604.5–2611] | 960 [351–2038] | 1820 [693–3192] |
| 1-y | 842 [393.5–3026] * | 936 [376.5–1995] * | 462 [16.5–1143] * | 1386 [480–2555] *,‡ | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavalleri, J.; Treguier, D.; Deliège, T.; Gurdebeke, C.; Ernst, M.; Lambermont, B.; Misset, B.; Rousseau, A.-F. One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment. Healthcare 2022, 10, 2023. https://doi.org/10.3390/healthcare10102023
Cavalleri J, Treguier D, Deliège T, Gurdebeke C, Ernst M, Lambermont B, Misset B, Rousseau A-F. One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment. Healthcare. 2022; 10(10):2023. https://doi.org/10.3390/healthcare10102023
Chicago/Turabian StyleCavalleri, Jonathan, Delphine Treguier, Thibaut Deliège, Christine Gurdebeke, Marie Ernst, Bernard Lambermont, Benoit Misset, and Anne-Françoise Rousseau. 2022. "One-Year Functional Decline in COVID-19 and Non-COVID-19 Critically Ill Survivors: A Prospective Study Incorporating a Pre-ICU Status Assessment" Healthcare 10, no. 10: 2023. https://doi.org/10.3390/healthcare10102023