
DESnets: A Graphical Representation for Discrete Event Simulation and Cost-Effectiveness Analysis


Abstract
:1. Introduction
2. DESnets: Definition and Algorithm for CEA
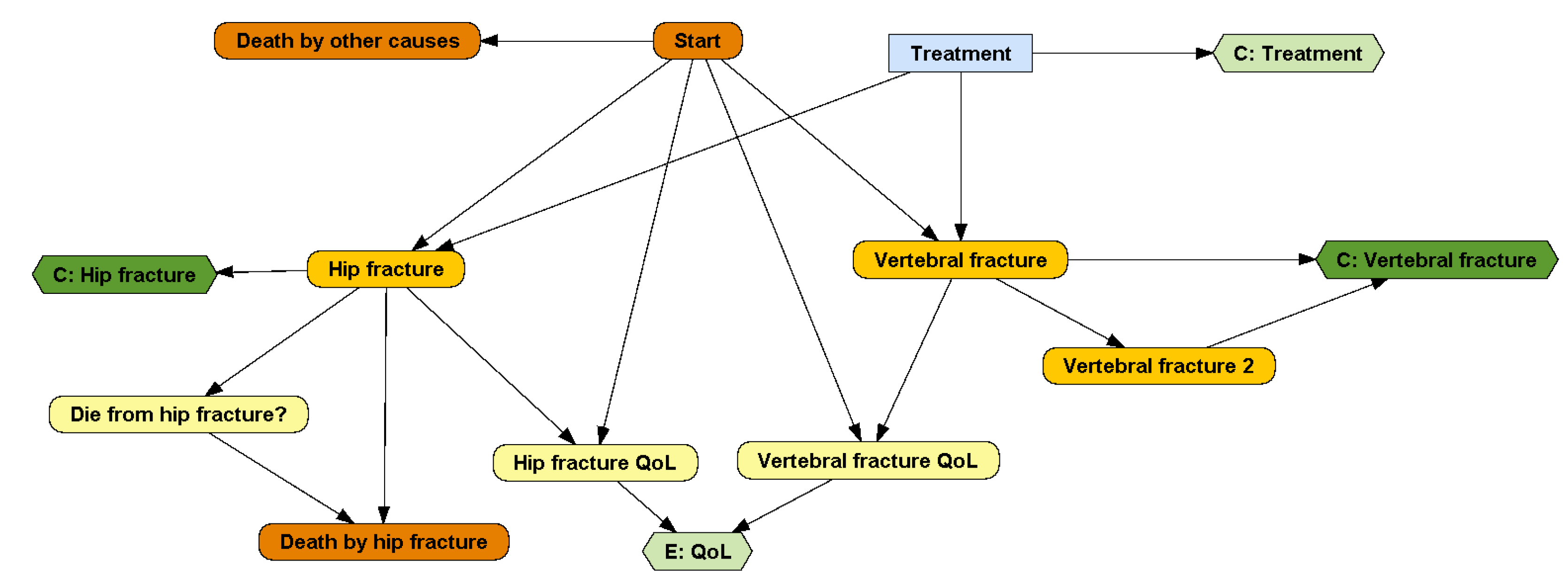
2.1. Representation of DESnets
2.1.1. DESnet Nodes
2.1.2. DESnet Links
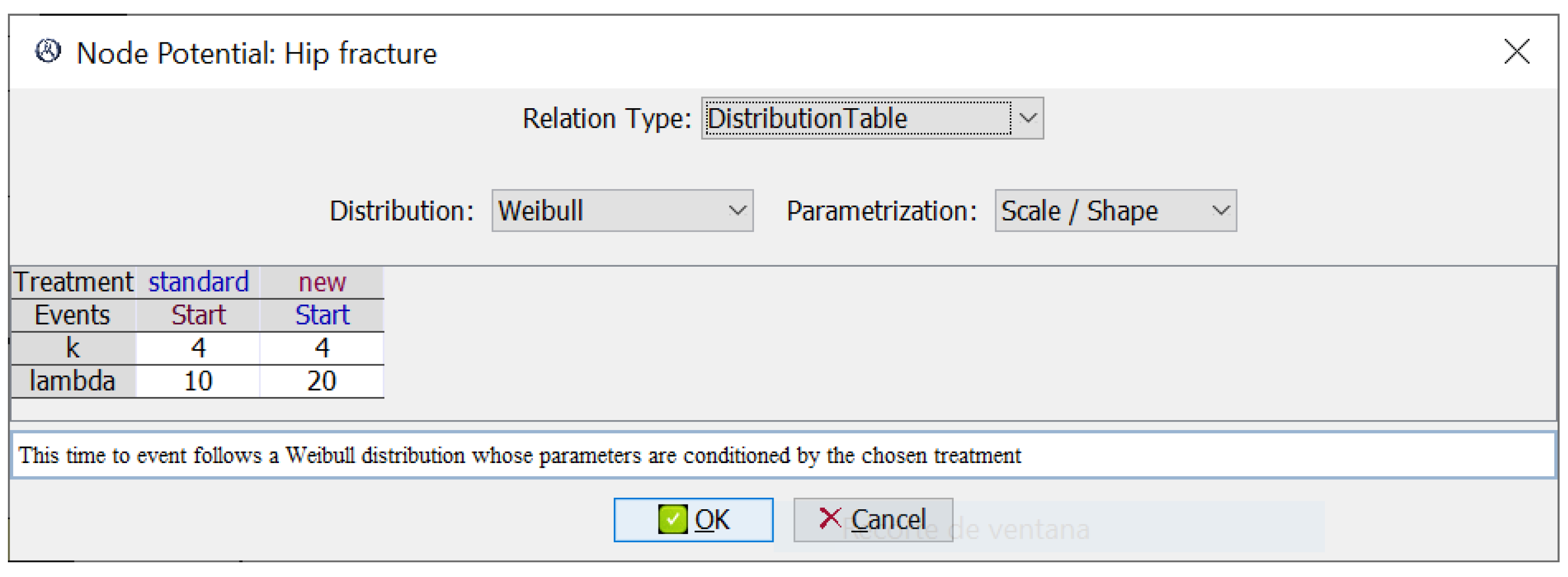
2.1.3. DESnets Potentials
2.2. Algorithm for Evaluating DESnets
| Algorithm 1: Evaluation of a DESnet for a single patient |
 |
| Algorithm 2: Update event-descendants when an event E happens |
 |
3. Comparison with Other Frameworks and Software Tools
- Programming languages (R and VBA);
- General purpose tools for DES (Arena and Simul8);
- Software tools specifically designed for this task (TreeAge Pro and DICE).
3.1. Qualitative Comparison: Ease of Use, Expressiveness, and Transparency
3.1.1. Programming Languages
3.1.2. General-Purpose Tools for DES: Arena and Simul8
3.1.3. TreeAge Pro Healthcare, a Software Tool for CEA with DES
3.1.4. DICE, a Framework with Several Possible Implementations
3.2. Empirical Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| CEA | Cost-effectiveness analysis |
| DES | Discrete event simulation |
| DESnet | Discrete event simulation network |
| DSU | Decision Support Unit |
| GUI | Graphical user interface |
| ICER | Incremental cost-effectiveness ratio |
| ID | Influence diagram |
| MDP | Markov decision process |
| NICE | National Institute for Health and Care Excellence |
| PGM | Probabilistic graphical model |
| POMDP | Partially observable Markov decision process |
| QALY | Quality-adjusted life year |
Appendix A. Constraints for DESnets
- There is only one decision because every option (i.e., every state of the decision node) is one of the interventions evaluated in the CEA. This constraint will be relaxed in upcoming versions of the algorithm by taking as the set of interventions the Cartesian product of the states of all the decisions;
- The initial event is unique and has no parents, because it marks the beginning of the simulation;
- Any other event has at least one event parent;
- Final events have no event children because they end the simulation (but they may have chance and payoff nodes as children);
- Payoff nodes have no children;
- The domain for time-to-event distributions (density functions) is ;
- Every directed cycle involving more than one node contains at least one event.

Appendix B. Implementations of the Osteoporosis Model
- R version 4.1.1, on RStudio 1.4.1717;
- Microsoft Excel Professional Plus 2016 (for VBA and DICE);
- Arena version 16.10;
- TreeAge Pro Healthcare 2022 R1.2.
- No time horizon was set, in order to cover the patients’ whole lifespan;
- Recording of patient-level data was disabled (except for TreeAge, because it was not possible);
- Batch simulation and simulation timing were enabled.
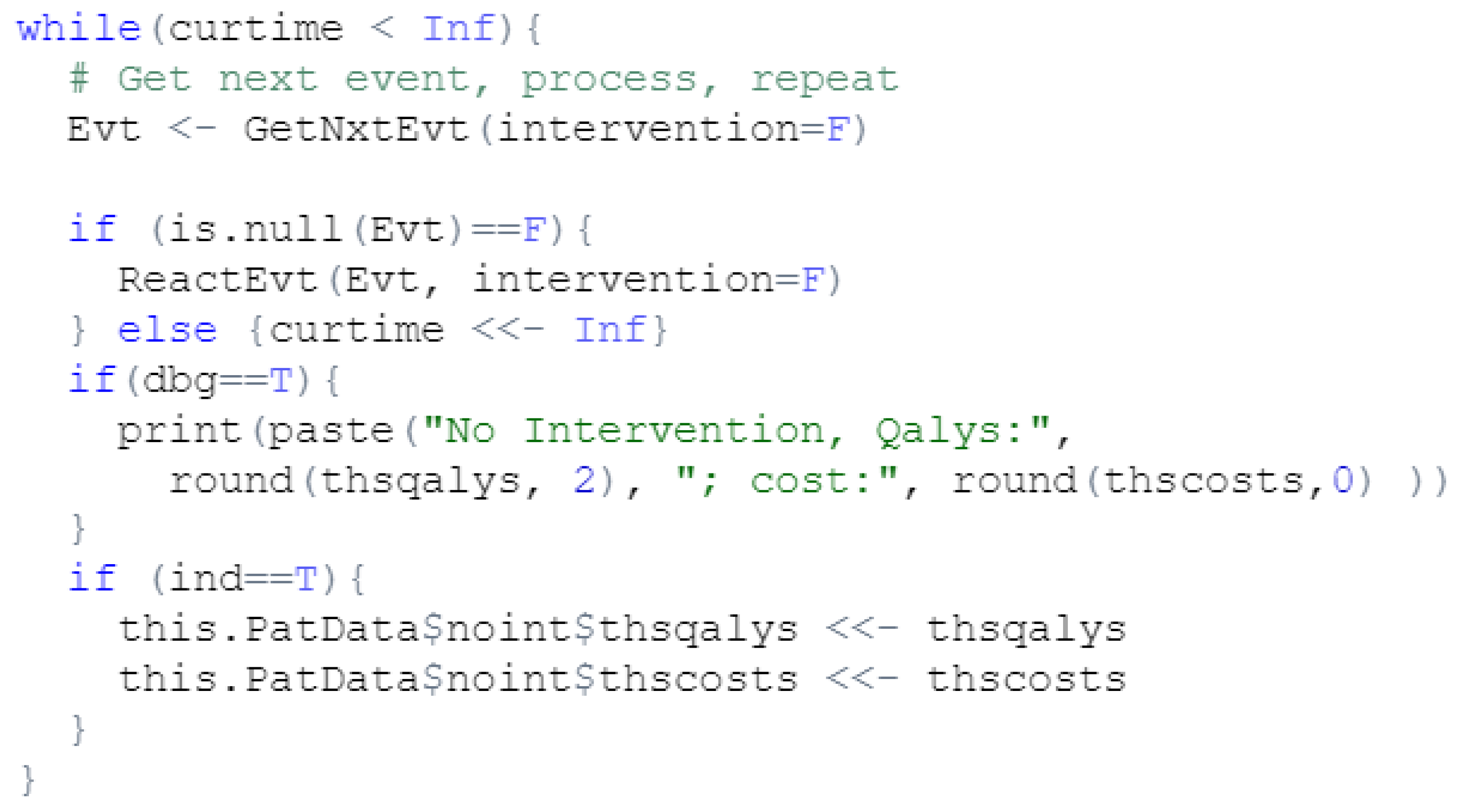
Appendix B.1. R Language

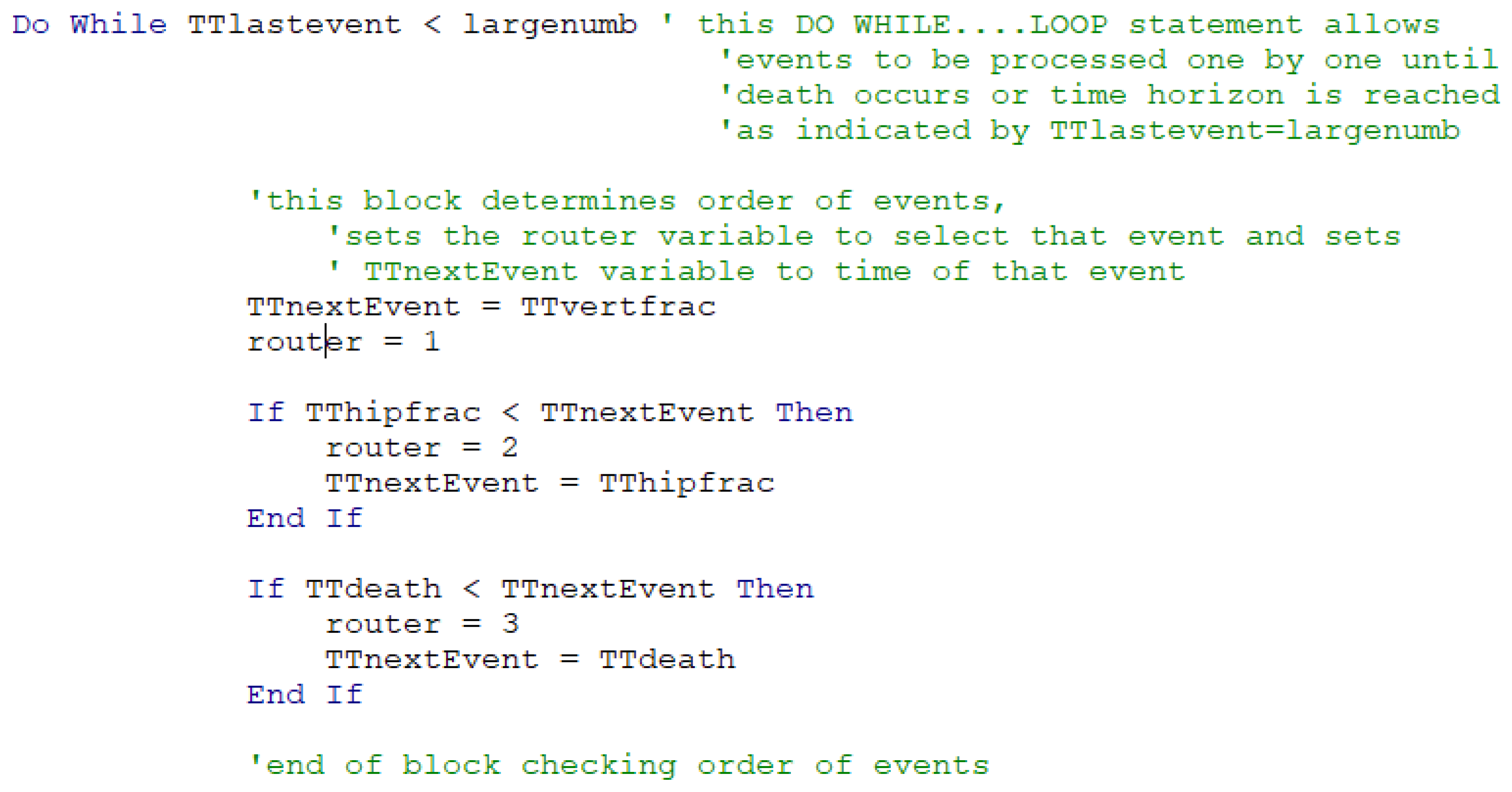
Appendix B.2. VBA Language

Appendix B.3. Simul8
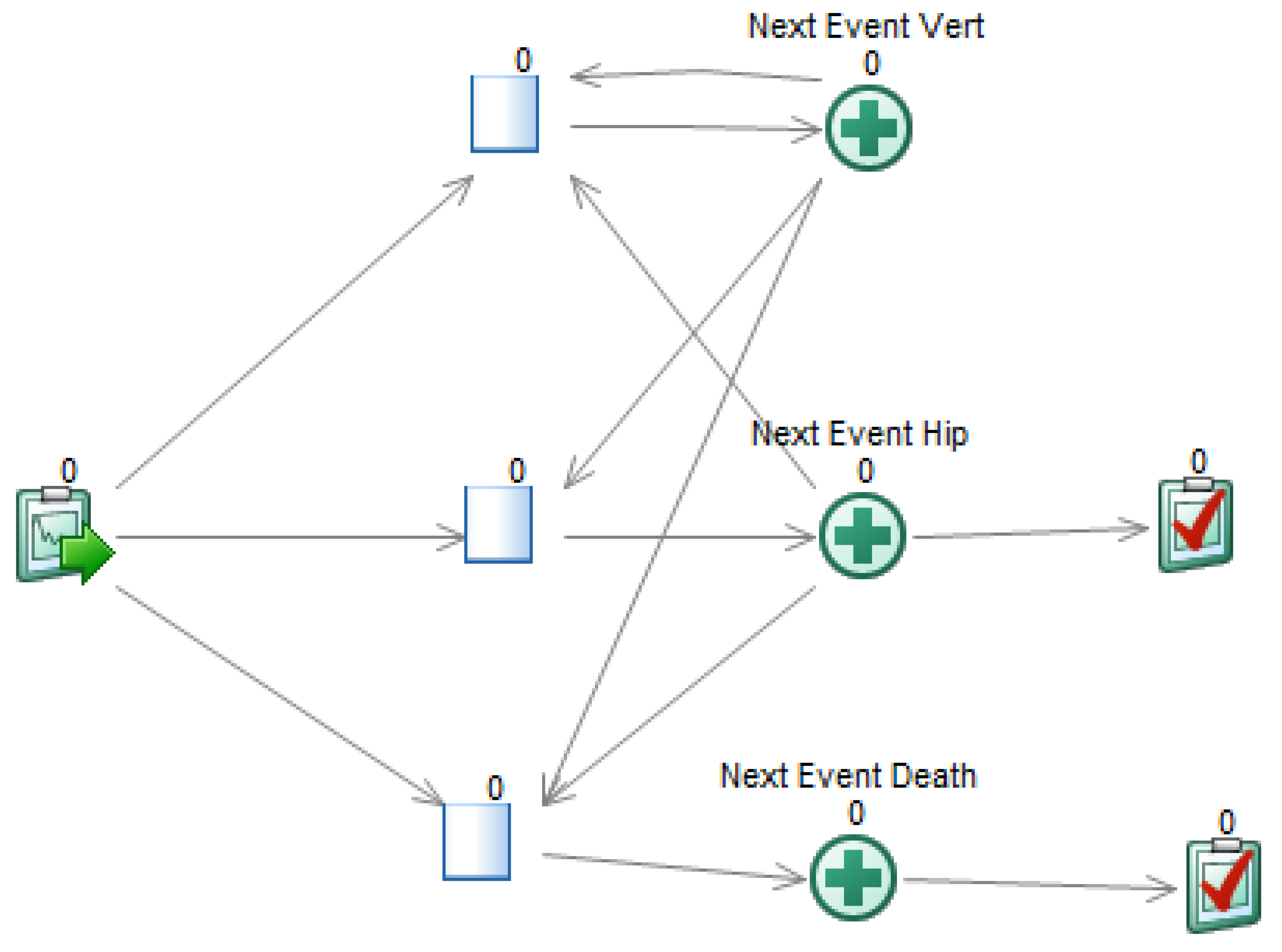
- A graph, which depicts the simulation flow (cf. Figure A4). There is a start point, where the patients enter the model, three ‘activities’ that represent the main events of the model, and two end points. A queue is necessary to connect each activity with the start point;
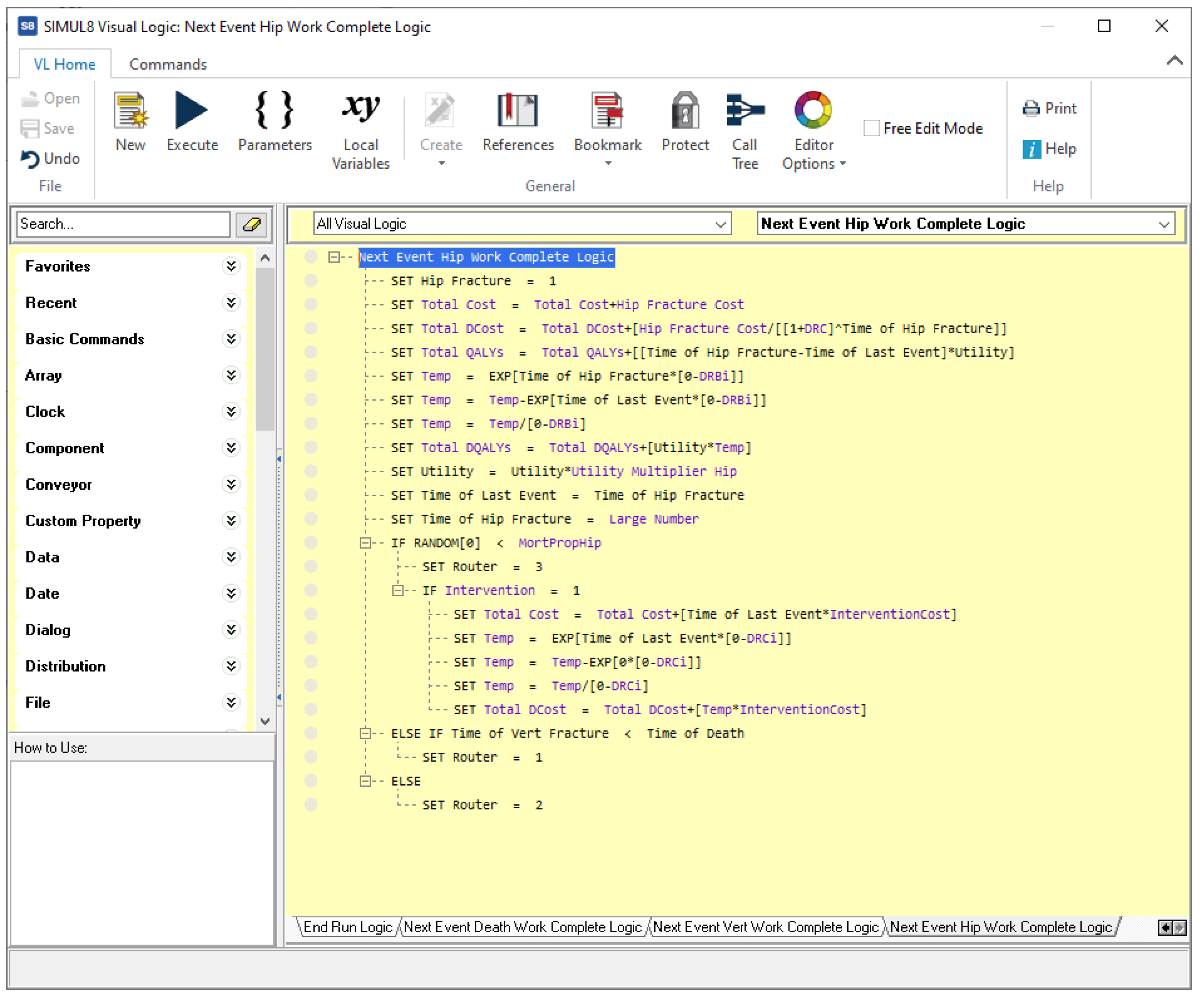
- Visual Logic (VL) code, in several pieces, which specify the behavior of the simulation. For example, Figure A5 shows the code for processing the consequences of the event ‘Hip fracture’. The algorithm implemented in this model is similar to the one in VBA;
- A set of distributions, selected from Simul8’s catalog;
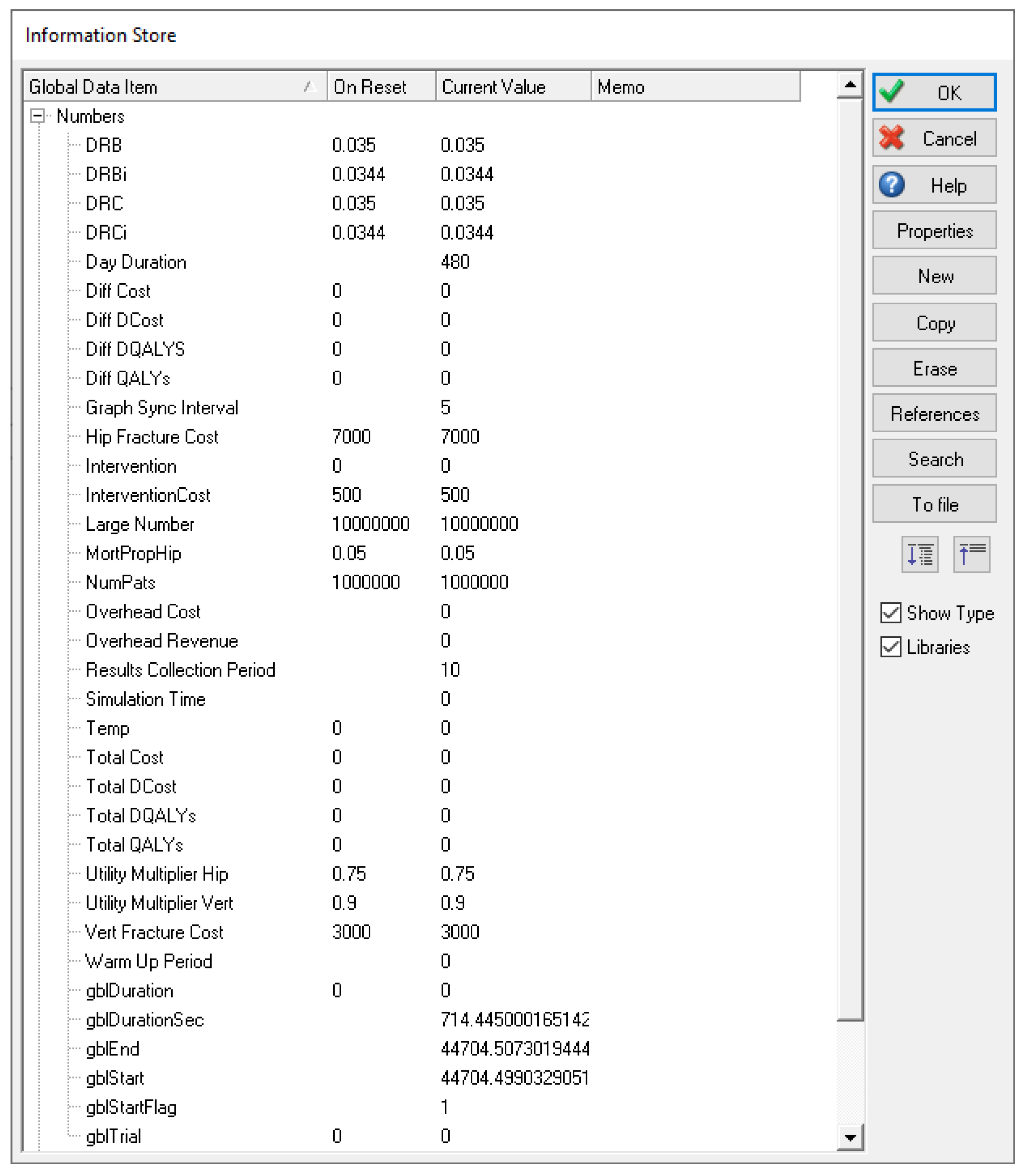
- A set of variables, which store model data, auxiliary values, simulation settings, and results; for example, the number of patients to be simulated, the intervention currently examined, the total cost and effectiveness, etc., as shown in Figure A6.



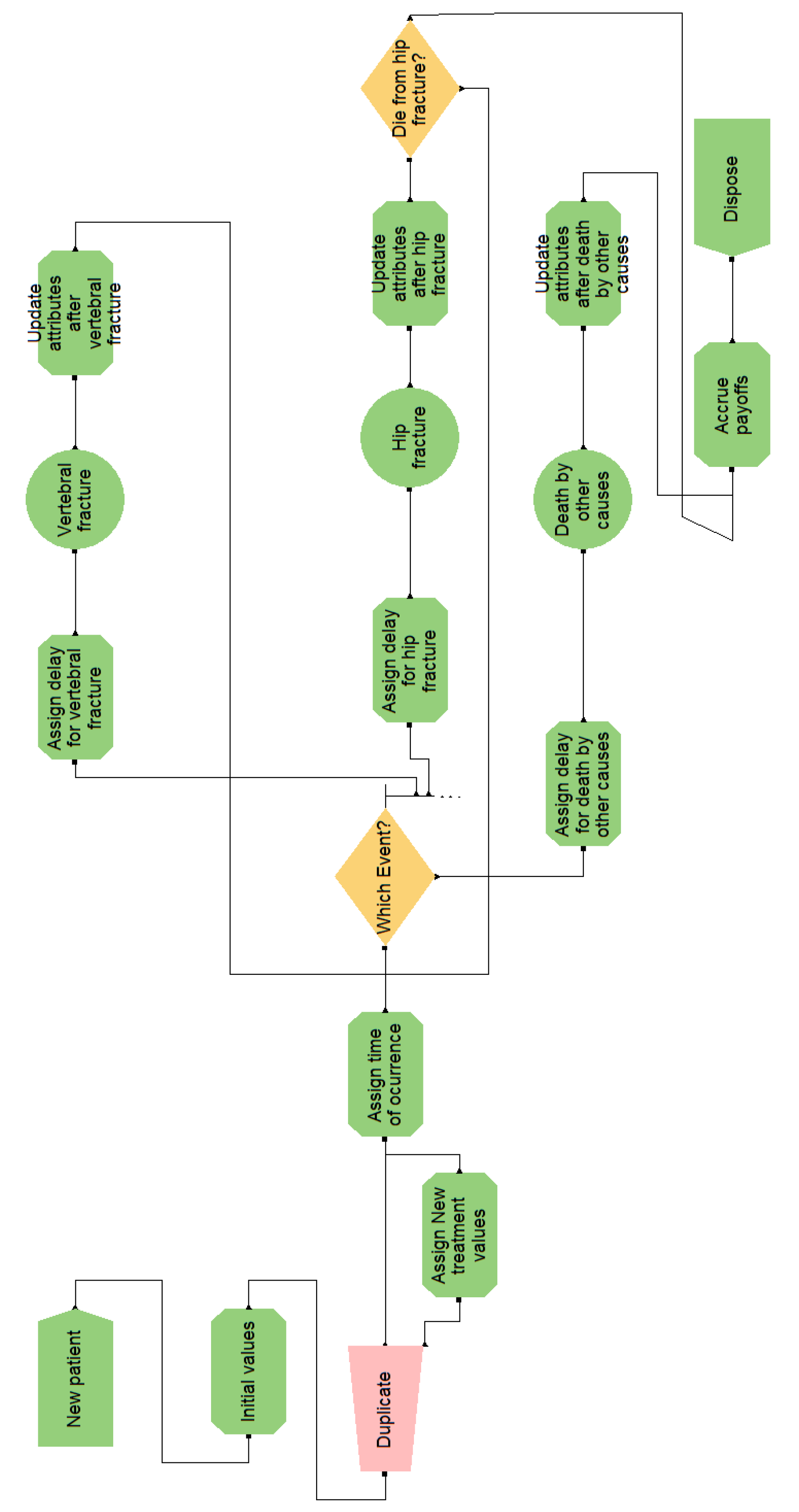
Appendix B.4. Arena
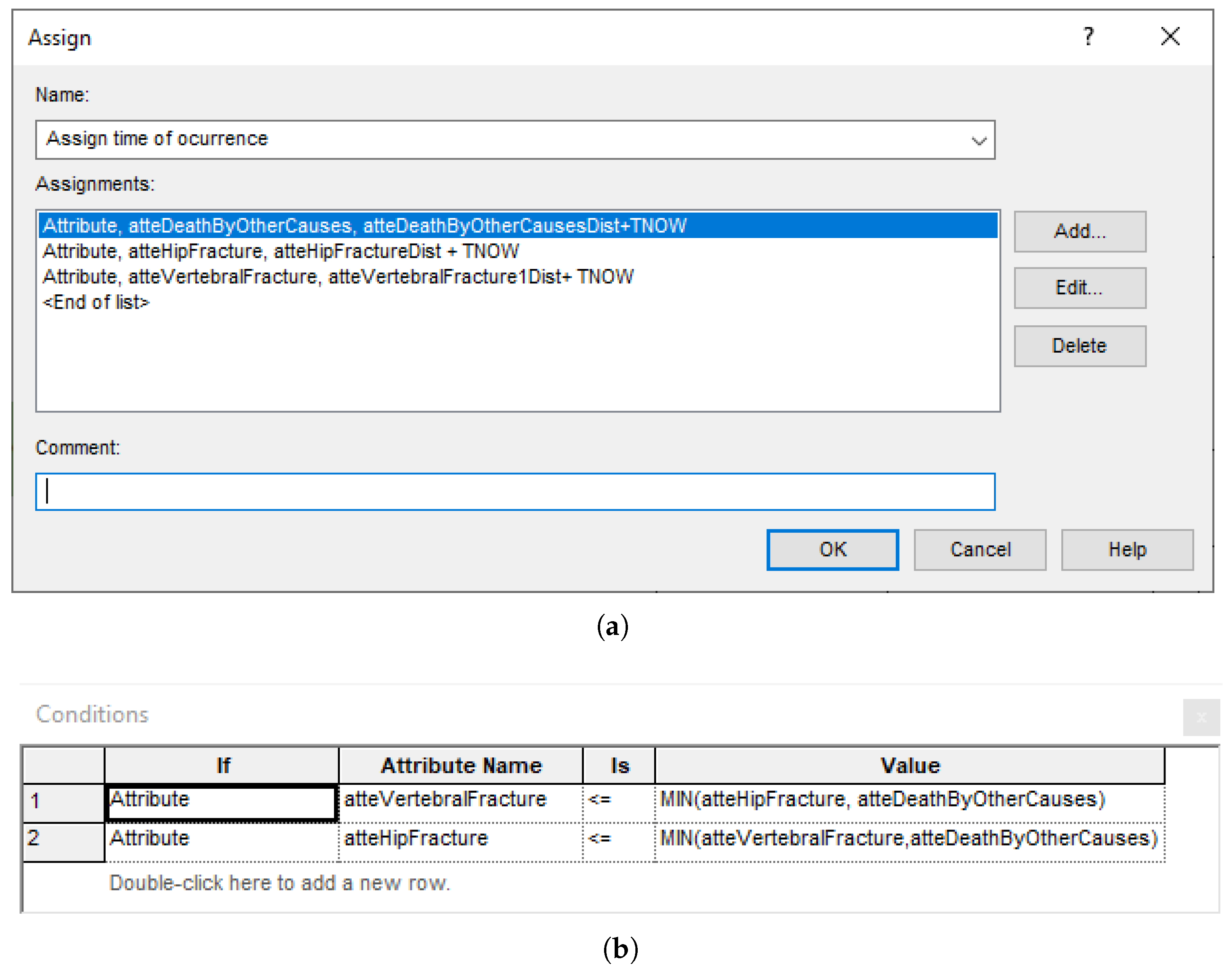
- A graph, which constitutes the flow diagram, built with SIMAN blocks. Entities—patients, in our case—flow through the diagram, triggering actions (such as computing values, assigning variables, and accruing payoffs) in the blocks they traverse. For example, the ‘Which Event?’ block, shown in Figure A7, has some embedded logic (cf. Figure A8) for selecting the next event when a patient arrives. The probability distributions are sampled at the ‘Initial values’ block, placed before ‘Duplicate’, in order to reduce nuisance variance. This allows both interventions to be simulated while ensuring that values change only when needed;
- Variables, which hold the values global to the whole simulation, such as the accrued payoffs;
- Attributes, which hold values for the current patient, including the times of occurrence of the events.


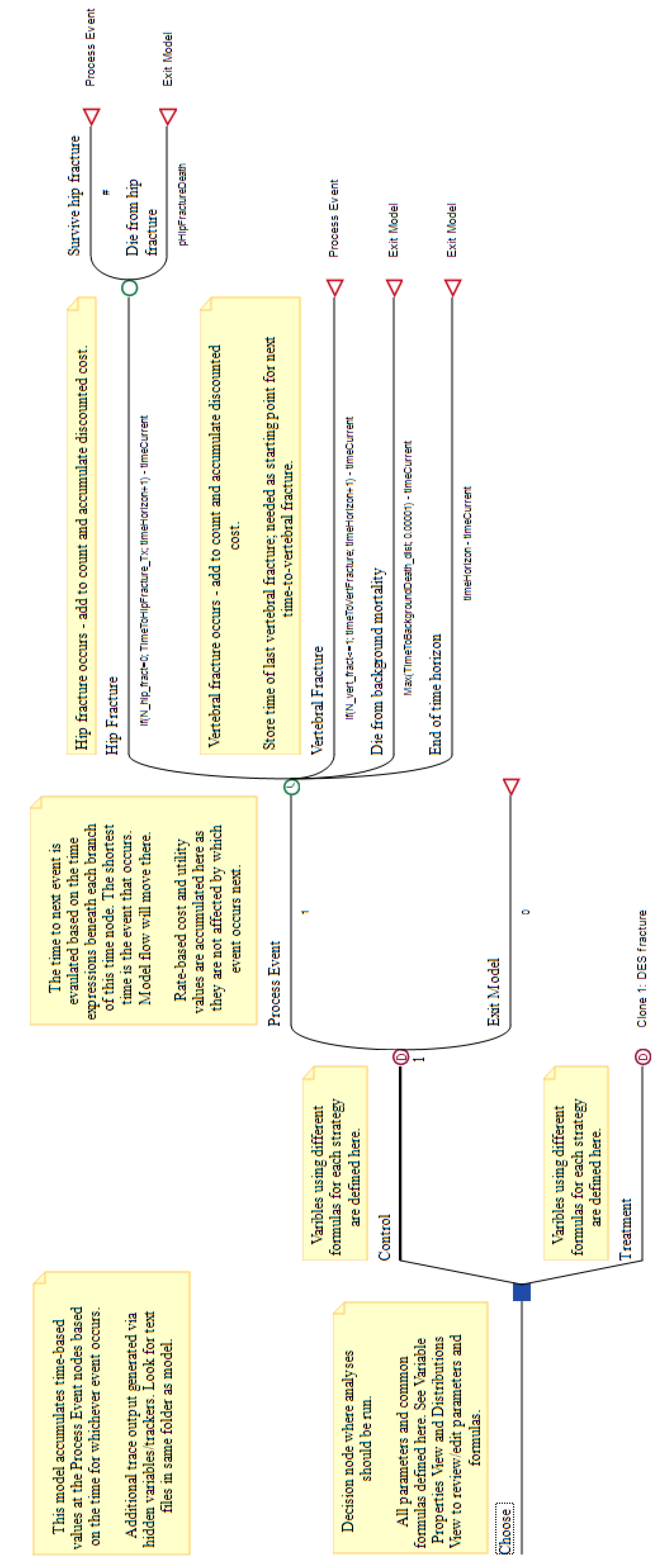
Appendix B.5. TreeAge
- A tree, shown in Figure A9. Its root is a decision node for the two interventions, ‘Control’ and ‘Treatment’. The second branch is a clone, with redefined variables;
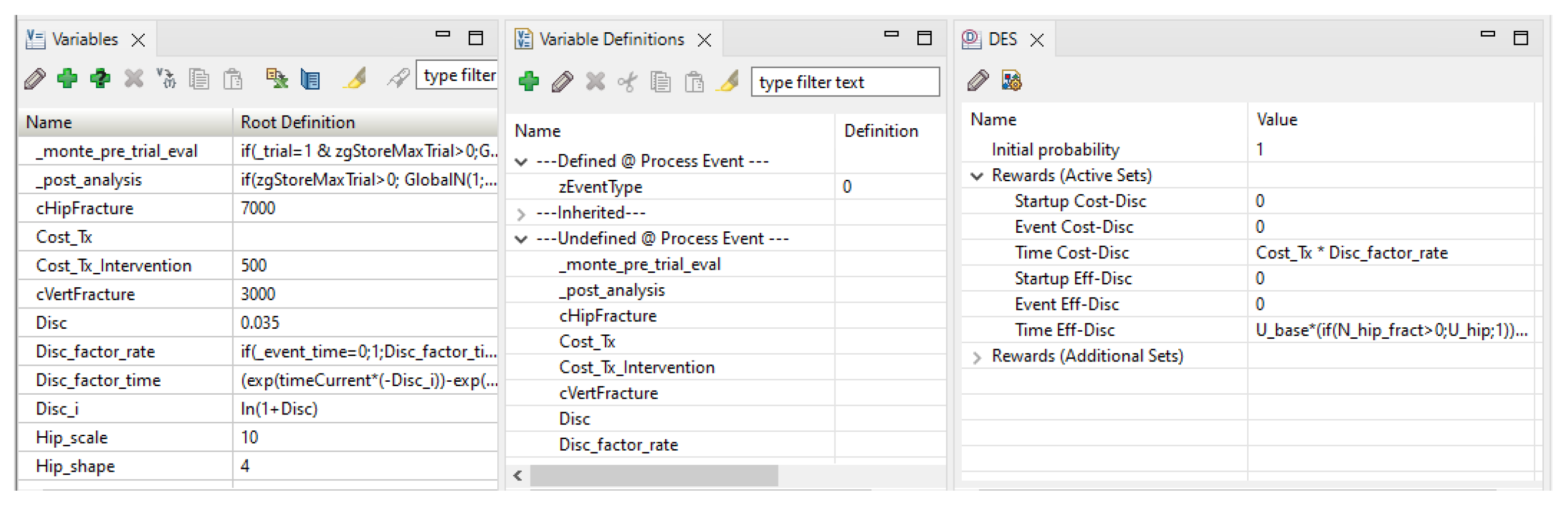
- The bottom pane, shown in Figure A10, with tabs for different element types: variables, variable definitions, distributions, DES payoffs, etc.


Appendix B.6. DICE
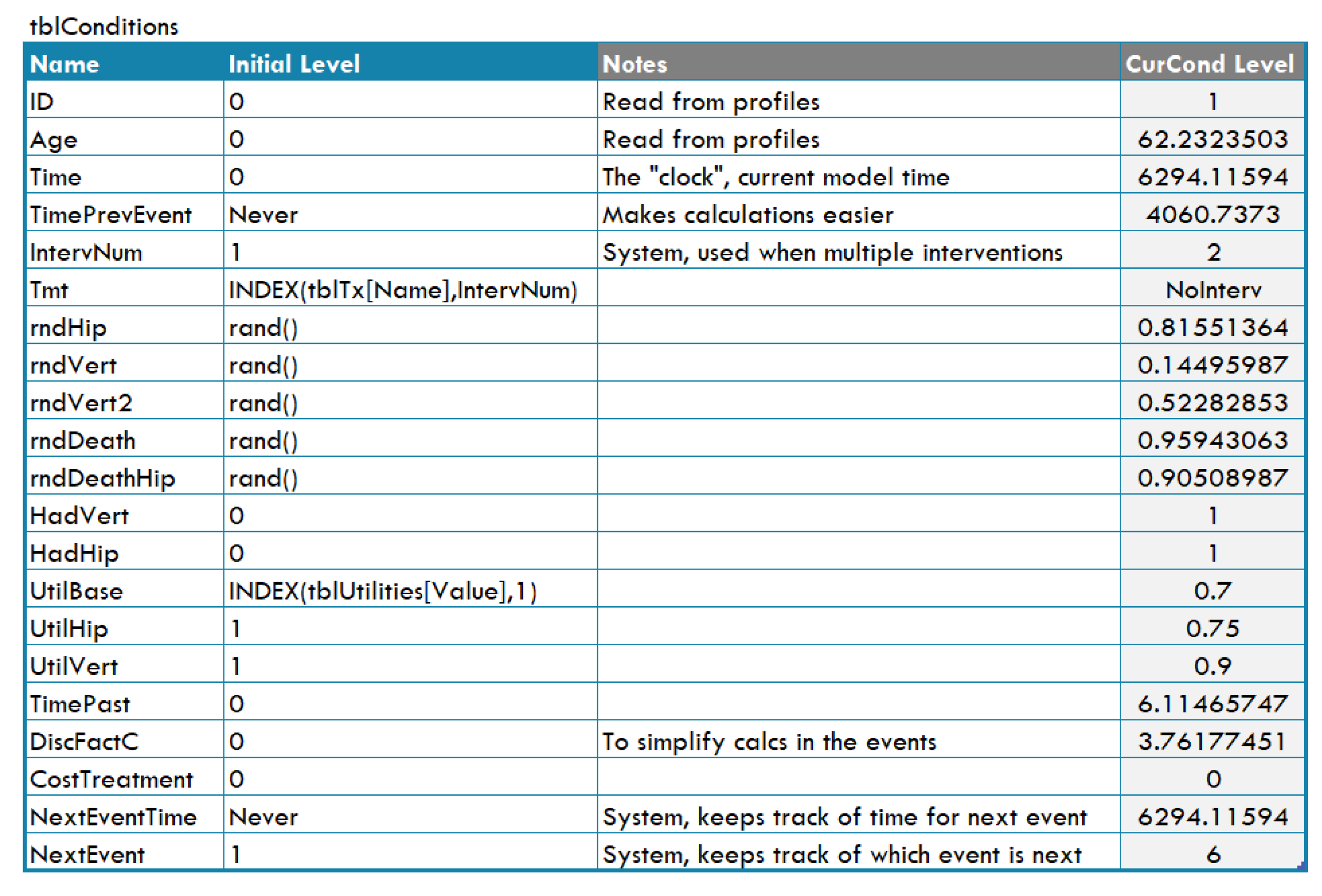
- Conditions, which are variables used to represent real world magnitudes (for instance, ‘Age’) or to implement the flow control (for example, ‘TimePrevEvent’). Each condition has a name and a value (called ‘level’) and appears as a row in the ‘conditions table’, shown in Figure A11;
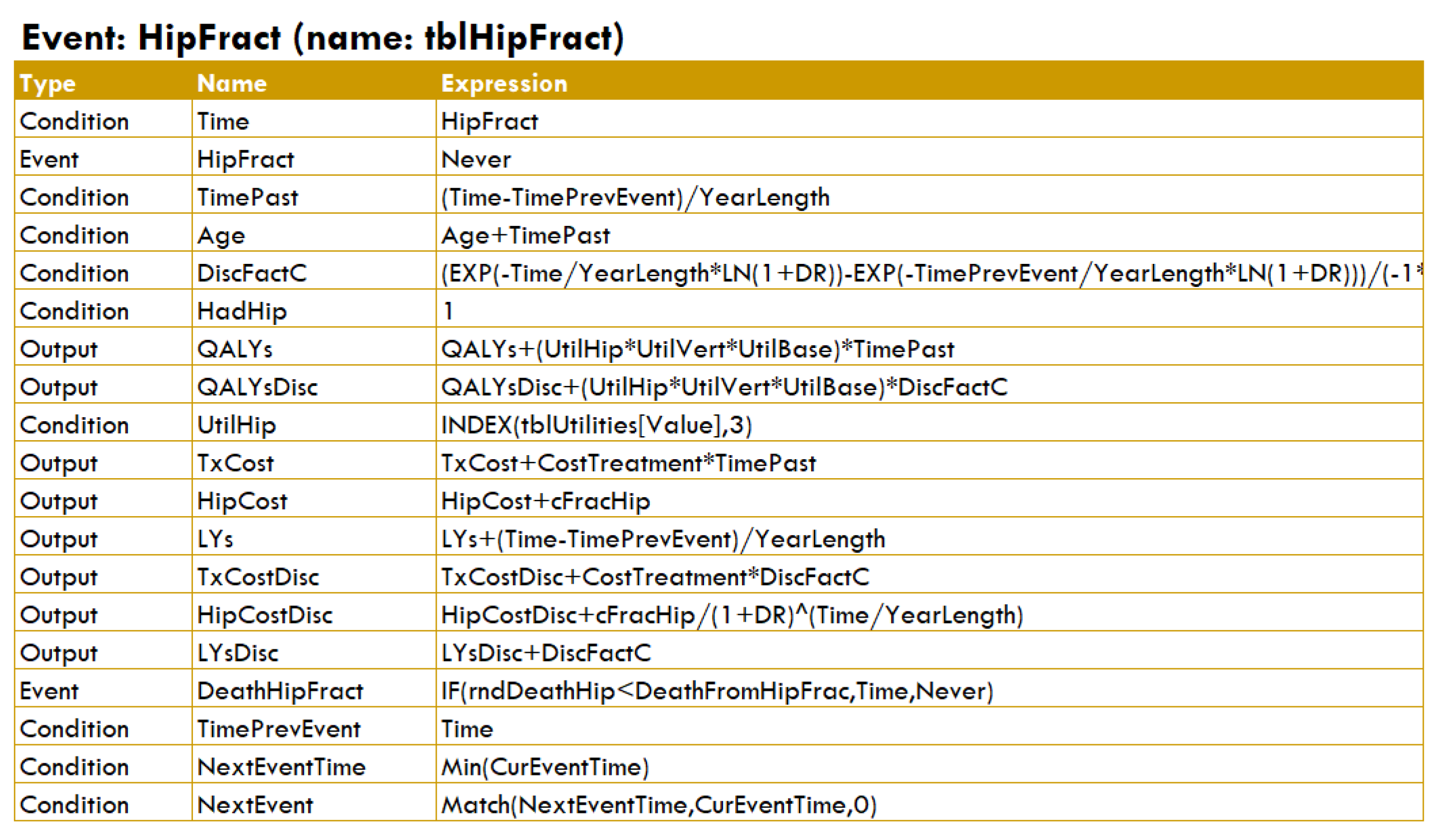
- Events, each having an associated table (see Figure A12) that indicates how to update the simulation when the event occurs; for example, changing the ‘level’ of some conditions, queuing new events, or calculating some outputs;
- Outputs. In DICE each output defines a property for which the evaluation will return a value. In this model, the outputs are not only cost and effectiveness but also some other properties, such as the age of death;
- Results. These are the values (usually numerical) obtained for the different outputs, both patient-level data and accrued values.


References
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes, 4th ed.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Brennan, A.; Chick, S.E.; Davies, R. A taxonomy of model structures for economic evaluation of health technologies. Health Econ. 2006, 15, 1295–1310. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.J.; Briggs, A.H.; Siebert, U.; Kuntz, K.M. Modeling good research practices—Overview: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-1. Value Health 2012, 15, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degeling, K.; Franken, M.D.; May, A.M.; van Oijen, M.G.; Koopman, M.; Punt, C.J.; IJzerman, M.J.; Koffijberg, H. Matching the model with the evidence: Comparing discrete event simulation and state-transition modeling for time-to-event predictions in a cost-effectiveness analysis of treatment in metastatic colorectal cancer patients. Cancer Epidemiol. 2018, 57, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.J.; Begum, N.; Koblbauer, I.; Dranitsaris, G.; Liew, D.; McEwan, P.; Yuan, Y.; Juarez-Garcia, A.; Tyas, D.; Pritchard, C. Cohort versus patient level simulation for the economic evaluation of single versus combination immuno-oncology therapies in metastatic melanoma. J. Med. Econ. 2019, 22, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karnon, J.; Afzali, H. When to use discrete event simulation (DES) for the economic evaluation of health technologies? A review and critique of the costs and benefits of DES. PharmacoEconomics 2014, 32, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Pan, F.; Sorensen, S. Modeling treatment sequences in pharmacoeconomic models. PharmacoEconomics 2016, 35, 15–24. [Google Scholar] [CrossRef]
- Davis, S.; Stevenson, M.; Tappenden, P.; Wailoo, A. Technical Support Document 15: Cost-Effectiveness Modelling Using Patient-Level Simulation; Technical Report; Decision Support Unit, National Institute for Health and Care Excellence (NICE): London, UK, 2014; Available online: https://www.sheffield.ac.uk/nice-dsu/tsds/patient-level-simulation (accessed on 20 February 2023).
- Salleh, S.; Thokala, P.; Brennan, A.; Hughes, R.; Dixon, S. Discrete event simulation-based resource modelling in health technology assessment. PharmacoEconomics 2017, 35, 989–1006. [Google Scholar] [CrossRef]
- Sharp, L.; Tilson, L.; Whyte, S.; Ceilleachair, A.O.; Walsh, C.; Usher, C.; Tappenden, P.; Chilcott, J.; Staines, A.; Barry, M.; et al. Using resource modelling to inform decision making and service planning: The case of colorectal cancer screening in Ireland. BMC Health Serv. Res. 2013, 13, 105. [Google Scholar] [CrossRef] [Green Version]
- Standfield, L.; Comans, T.; Scuffham, P. Markov modeling and discrete event simulation in health care: A sytematic comparison. Int. J. Technol. Assess. Health Care 2014, 30, 165–172. [Google Scholar] [CrossRef] [Green Version]
- von Neumann, J.; Morgenstern, O. Theory of Games and Economic Behavior; Princeton University Press: Princeton, NJ, USA, 1944. [Google Scholar]
- Koller, D.; Friedman, N. Probabilistic Graphical Models: Principles and Techniques; The MIT Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Pearl, J. Probabilistic Reasoning in Intelligent Systems: Networks of Plausible Inference; Morgan Kaufmann: San Mateo, CA, USA, 1988. [Google Scholar]
- Markov, A.A. Rasprostranenie zakona bol’shih chisel na velichiny, zavisyaschie drug ot druga. Izv.-Fiz.-Mat. Obs. Pri Kazan. Univ. 1906, 15, 135–156. [Google Scholar]
- Wright, S. Correlation and causation. J. Agric. Res. 1921, 20, 557–585. [Google Scholar]
- Warner, H.R.; Toronto, A.F.; Veasy, L.G.; Stephenson, R. A mathematical approach to medical diagnosis: Application to congenital heart disease. JAMA 1961, 177, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Bellman, R.E. Dynamic Programming; Princeton University Press: Princeton, NJ, USA, 1957. [Google Scholar]
- Åström, K.J. Optimal control of Markov processes with incomplete state estimation. J. Math. Anal. Appl. 1965, 10, 174–205. [Google Scholar] [CrossRef] [Green Version]
- Kindermann, R.; Snell, J.L. Markov Random Fields and Their Applications; American Mathematical Society: Providence, RI, USA, 1980. [Google Scholar]
- Howard, R.A.; Matheson, J.E. Influence diagrams. In Readings on the Principles and Applications of Decision Analysis; Howard, R.A., Matheson, J.E., Eds.; Strategic Decisions Group: Menlo Park, CA, USA, 1984; pp. 719–762. [Google Scholar]
- Caro, J.J.; Möller, J.; Karnon, J.; Stahl, J.; Ishak, J. Discrete Event Simulation for Health Technology Assessment; Chapman and Hall/CRC: Boca Raton, FL, USA, 2015. [Google Scholar] [CrossRef]
- Pearl, J. Fusion, propagation and structuring in belief networks. Artif. Intell. 1986, 29, 241–288. [Google Scholar] [CrossRef] [Green Version]
- Dean, T.; Kanazawa, K. A model for reasoning about persistence and causation. Comput. Intell. 1989, 5, 142–150. [Google Scholar] [CrossRef]
- Boutilier, C.; Dearden, R.; Goldszmidt, M. Stochastic dynamic programming with factored representations. Artif. Intell. 2000, 121, 49–107. [Google Scholar] [CrossRef] [Green Version]
- Boutilier, C.; Poole, D. Computing optimal policies for partially observable decision processes using compact representations. In Proceedings of the Thirteenth National Conference on Artificial Intelligence (AAAI’96), Portland, OR, USA, 4–8 August 1996; Clancey, W.J., Weld, D.S., Eds.; AAAI Press/MIT Press: Portland, OR, USA, 1996; pp. 1168–1175. [Google Scholar]
- Arias, M.; Díez, F.J. Cost-effectiveness analysis with influence diagrams. Methods Inf. Med. 2015, 54, 353–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díez, F.J.; Yebra, M.; Bermejo, I.; Palacios-Alonso, M.A.; Arias, M.; Luque, M.; Pérez-Martín, J. Markov influence diagrams: A graphical tool for cost-effectiveness analysis. Med. Decis. Mak. 2017, 37, 183–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díez, F.J.; Luque, M.; Bermejo, I. Decision analysis networks. Int. J. Approx. Reason. 2018, 96, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Díez, F.J.; Luque, M.; Arias, M.; Pérez-Martín, J. Cost-effectiveness analysis with unordered decisions. Artif. Intell. Med. 2021, 117, 102064. [Google Scholar] [CrossRef]
- Caro, J.J.; Möller, J. Advantages and disadvantages of discrete-event simulation for health economic analyses. Expert Rev. Pharmacoecon. Outcomes Res. 2016, 16, 327–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karnon, J.; Stahl, J.E.; Brennan, A.; Caro, J.J.; Mar, J.; Möller, J. Modeling using discrete event simulation: A report of the ISPOR-SMDM Modeling Good Research Practices Task Force-4. Value Health 2012, 15, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OpenMarkov. Available online: http://www.openmarkov.org (accessed on 28 February 2023).
- Patient-Level Simulation TSD | NICE Decision Support Unit | The University of Sheffield. Available online: https://www.sheffield.ac.uk/nice-dsu/tsds/patient-level-simulation (accessed on 19 February 2023).
- Jackson, C. flexsurv: A platform for parametric survival modeling. J. Stat. Softw. 2016, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DARTH—Decision Analysis in R for Technologies in Health. Available online: https://darthworkgroup.com (accessed on 28 February 2023).
- Alarid-Escudero, F.; Krijkamp, E.M.; Pechlivanoglou, P.; Jalal, H.; Kao, S.Y.Z.; Yang, A.; Enns, E.A. A need for change! A coding framework for improving transparency in decision modeling. PharmacoEconomics 2019, 37, 1329–1339. [Google Scholar] [CrossRef]
- Simul8|Fast, Intuitive Simulation Software for Desktop and Web. Available online: https://www.simul8.com (accessed on 28 February 2023).
- Arena Simulation Software. Available online: https://www.rockwellautomation.com/es-es/products/software/arena-simulation.html (accessed on 28 February 2023).
- TreeAge Software. Available online: https://www.TreeAge.com (accessed on 28 February 2023).
- León, D. A Probabilistic Graphical Model for Total Knee Arthroplasty. Master’s Thesis, Department of Artificial Intelligence, UNED, Madrid, Spain, 2011. [Google Scholar]
- Luque, M.; Díez, F.J.; Disdier, C. Optimal sequence of tests for the mediastinal staging of non-small cell lung cancer. BMC Med. Inform. Decis. Mak. 2016, 16, 9. [Google Scholar] [CrossRef] [Green Version]
- Caro, J.J. Discretely Integrated Condition Event (DICE) simulation for pharmacoeconomics. PharmacoEconomics 2016, 34, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Caro, J.J.; Maconachie, R.; Woods, M.; Naidoo, B.; McGuire, A. Leveraging DICE (Discretely-Integrated Condition Event) simulation to simplify the design and implementation of hybrid models. Value Health 2020, 23, 1049–1055. [Google Scholar] [CrossRef]
- Discretely Integrated Condition Event (DICE) Simulation. Available online: https://www.evidera.com/dice (accessed on 19 February 2023).
- Arlegui, H.; Nachbaur, G.; Praet, N.; Bégaud, B.; Caro, J.J. Using discretely integrated condition event simulation to construct quantitative benefit-risk models: The example of rotavirus vaccination in France. Clin. Ther. 2020, 42, 1983–1991. [Google Scholar] [CrossRef]
- Möller, J.; Davis, S.; Stevenson, M.; Caro, J.J. Validation of a DICE simulation against a discrete event simulation implemented entirely in code. PharmacoEconomics 2017, 35, 1103–1109. [Google Scholar] [CrossRef]
- Pennington, B.; Filby, A.; Owen, L.; Taylor, M. Smoking cessation: A comparison of two model structures. PharmacoEconomics 2018, 36, 1101–1112. [Google Scholar] [CrossRef]
- Graves, J.; Garbett, S.; Zhou, Z.; Schildcrout, J.S.; Peterson, J. Comparison of decision modeling approaches for health technology and policy evaluation. Med. Decis. Mak. 2021, 41, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Gray, E.; Donten, A.; Karssemeijer, N.; Van Gils, C.; Evans, D.G.; Astley, S.; Payne, K. Evaluation of a stratified national breast screening program in the United Kingdom: An early model-based cost-effectiveness analysis. Value Health 2017, 20, 1100–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glover, M.J.; Jones, E.; Masconi, K.L.; Sweeting, M.J.; Thompson, S.G.; SWAN Collaborators. Discrete event simulation for decision modeling in health care: Lessons from abdominal aortic aneurysm screening. Med. Decis. Mak. 2018, 38, 439–451. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cost (GBP) | Effectiveness (QALY) | Time (s) | |||
|---|---|---|---|---|---|
| New. | Std. | New | Std. | ||
| R | 6876 ± 4 | 6887 ± 5 | 6.642 ± 0.002 | 6.092 ± 0.002 | 55.76 |
| VBA | 6877 ± 5 | 6887 ± 5 | 6.643 ± 0.002 | 6.092 ± 0.002 | 0.76 |
| Simul8 | 6872 ± 5 | 6886 ± 5 | 6.644 ± 0.002 | 6.093 ± 0.002 | 3.21 |
| Arena | 6873 ± 5 | 6884 ± 5 | 6.642 ± 0.002 | 6.092 ± 0.002 | 0.96 |
| TreeAge | 6874 ± 6 | 6886 ± 5 | 6.643 ± 0.002 | 6.092 ± 0.002 | 28.09 |
| DICE | 6875 ± 5 | 6889 ± 4 | 6.644 ± 0.002 | 6.093 ± 0.002 | 8153.67 |
| DESnet | 6875 ± 5 | 6885 ± 4 | 6.643 ± 0.002 | 6.092 ± 0.002 | 1.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yago, C.M.; Díez, F.J. DESnets: A Graphical Representation for Discrete Event Simulation and Cost-Effectiveness Analysis. Mathematics 2023, 11, 1602. https://doi.org/10.3390/math11071602
Yago CM, Díez FJ. DESnets: A Graphical Representation for Discrete Event Simulation and Cost-Effectiveness Analysis. Mathematics. 2023; 11(7):1602. https://doi.org/10.3390/math11071602
Chicago/Turabian StyleYago, Carmen María, and Francisco Javier Díez. 2023. "DESnets: A Graphical Representation for Discrete Event Simulation and Cost-Effectiveness Analysis" Mathematics 11, no. 7: 1602. https://doi.org/10.3390/math11071602