
An Optimal H-Infinity Controller for Left Ventricular Assist Devices Based on a Starling-like Controller: A Simulation Study

 , ,
, ,
Abstract
:1. Introduction
- Maintaining the circulation of a patient with HF.
- Controlling the flow rate to meet the changes in metabolic demand.
- Making a physiological flow pattern (pulsatile flow).
- Unloading the left ventricle.
- Preventing inflow suction.
- Preventing aortic valve insufficiency.
2. Materials and Methods
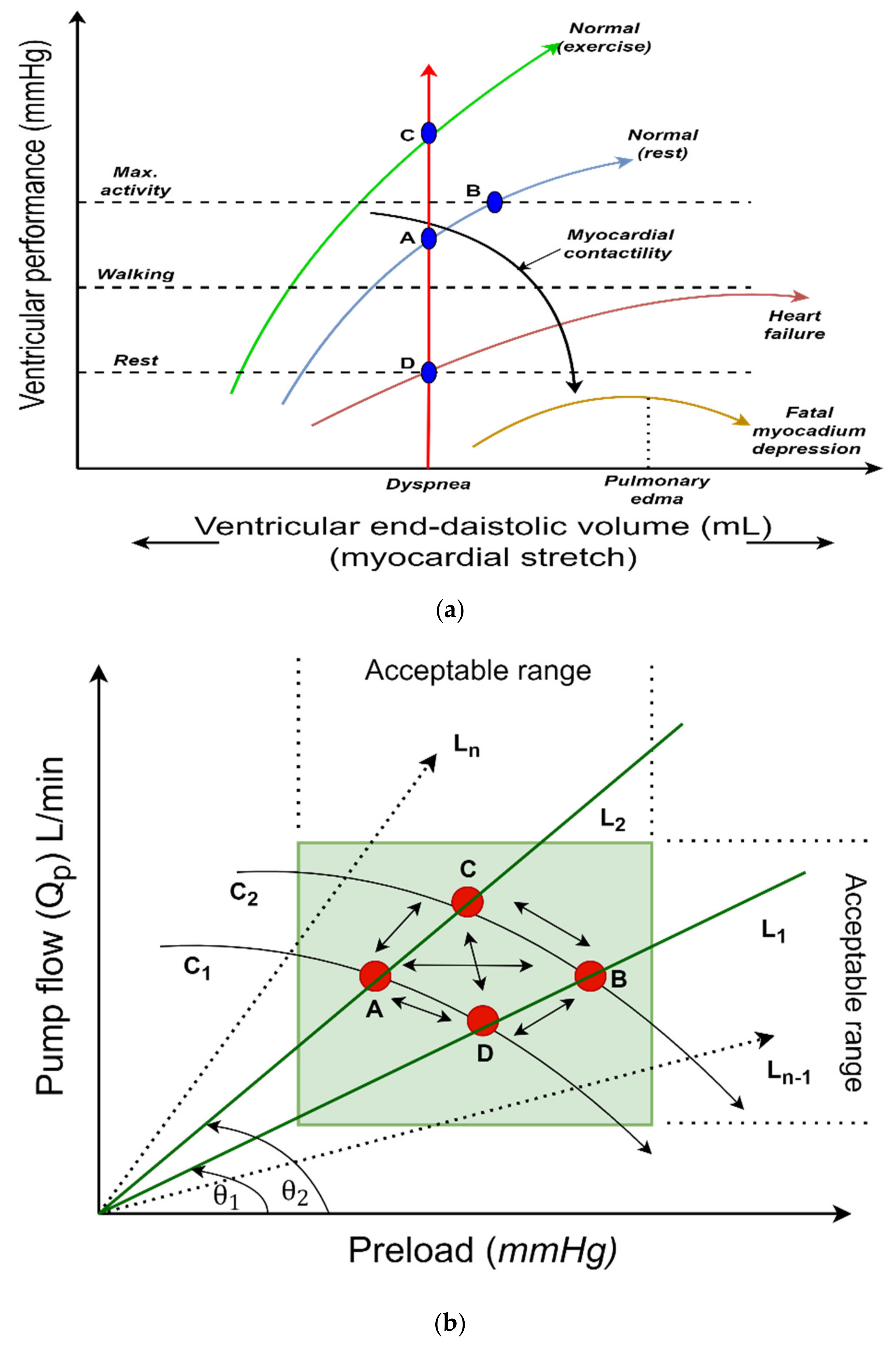
2.1. Control Strategy
2.2. Pump Flow Estimator Model
2.3. Controller Design
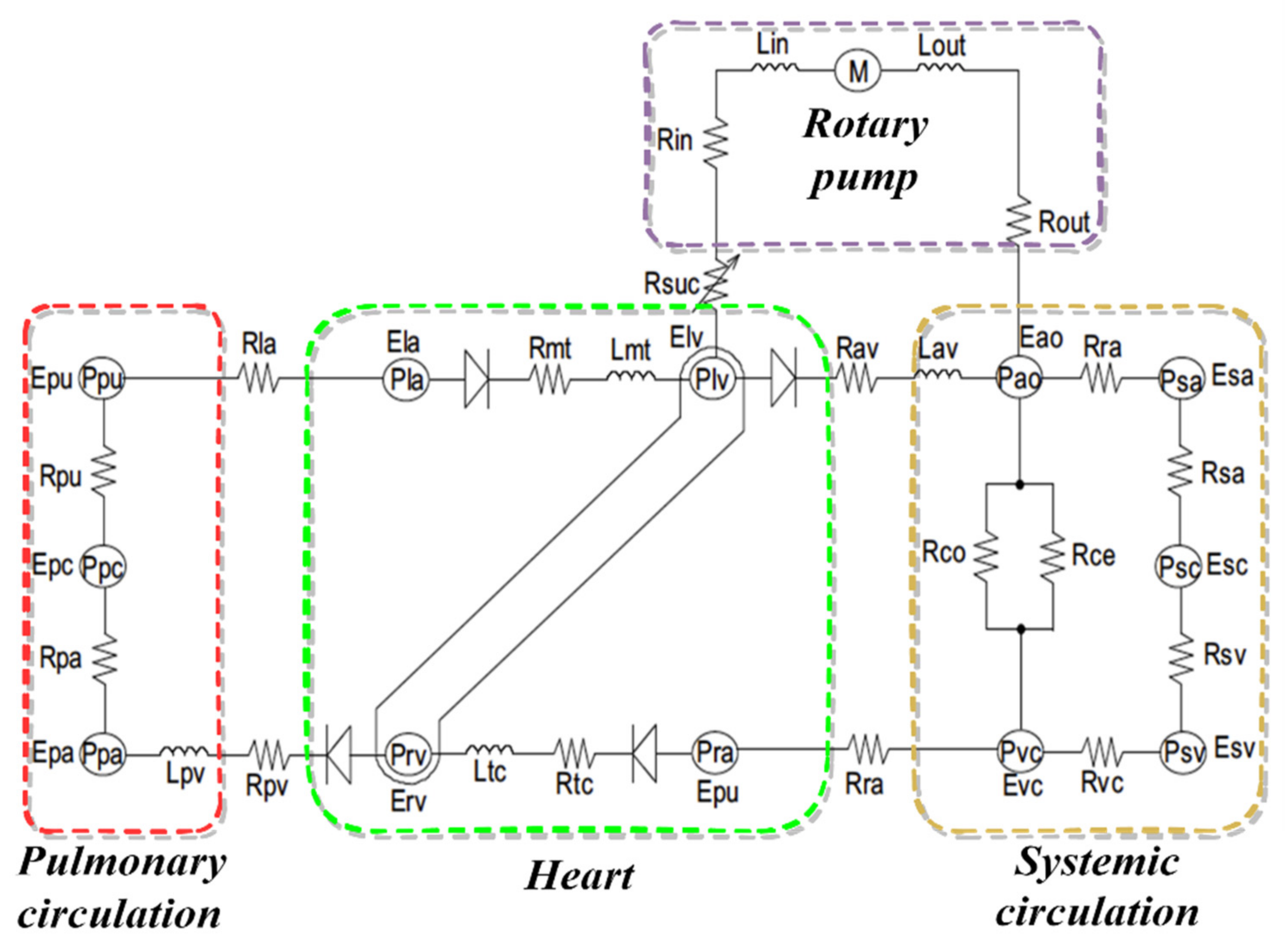
2.4. Cardiovascular System Model
- (a)
- Blood vessel compartment ():where represents one of the following:
- –
- Pulmonary peripheral vessel (pa);
- –
- Pulmonary veins (pvs);
- –
- Vena cava (vc);
- –
- Aorta (ao);
- –
- Systemic veins (svs);
- –
- Systemic peripheral vessel (sa).
is the unstressed volume of the corresponding vessel and is the compliance of the corresponding vessel.
- (b)
- Blood flow across the valves ():where represents one of the following:
- –
- Mitral valve (mt);
- –
- Tricuspid valve (tv);
- –
- Aortic valve (av);
- –
- Pulmonary valve (pv).
is the upstream pressure, is the downstream pressure of the corresponding valve, and is the resistance of the corresponding valve.
- (c)
- Pressure in the heart chamber ()where represents one of the following:
- –
- Left ventricular (lv);
- –
- Right ventricular (rv);
- –
- Left atrium (la);
- –
- Right atrium (ra).
is the slope of the end-systolic pressure–volume, is the volume of the heart chamber, is the end-systolic volume of the heart chamber at zero pressure, is the end-diastolic volume of the heart chamber at zero pressure, and , are the stiffness of the heart chamber at the end diastolic.
2.5. Simulation Protocols
3. Results
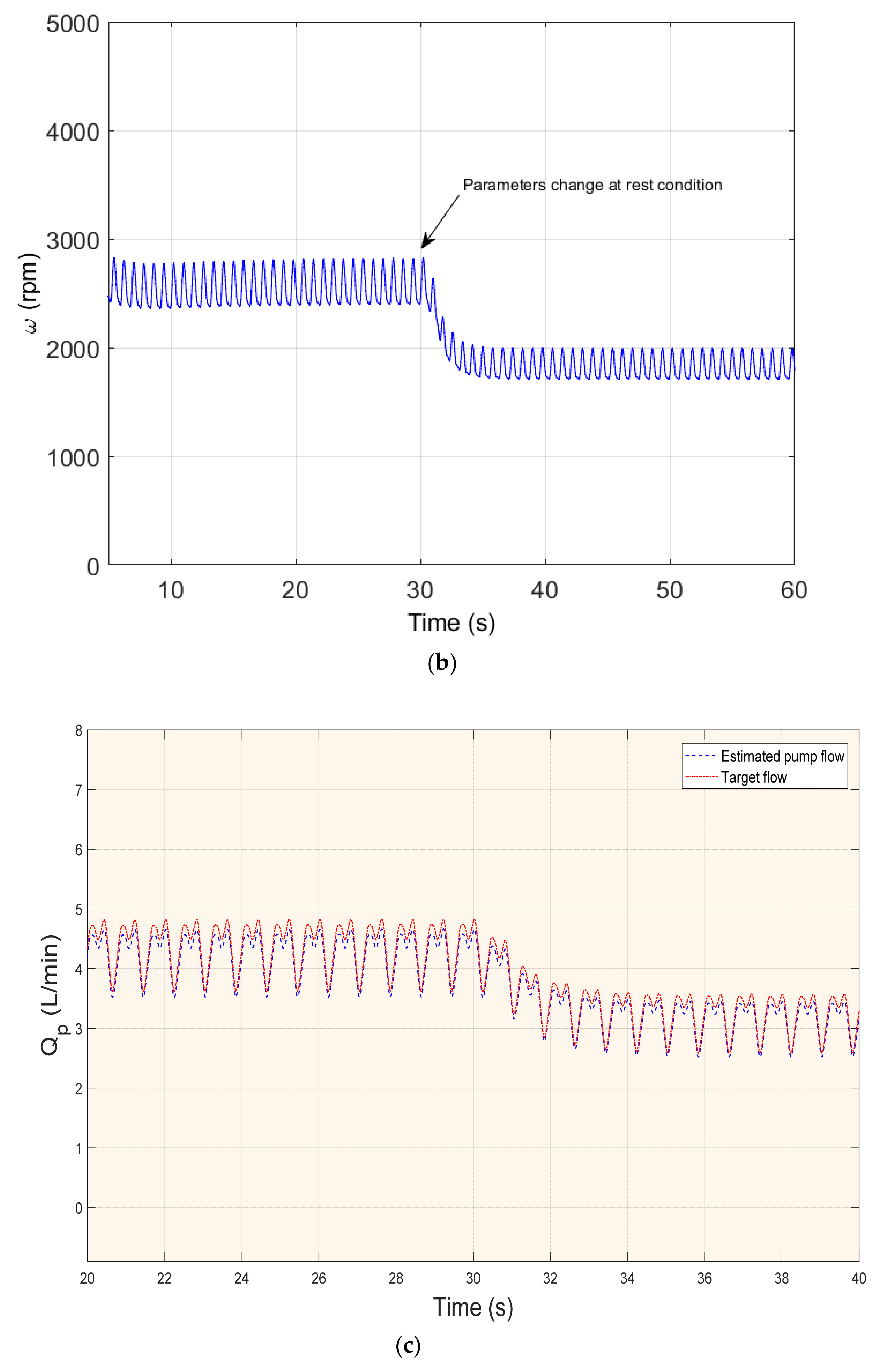
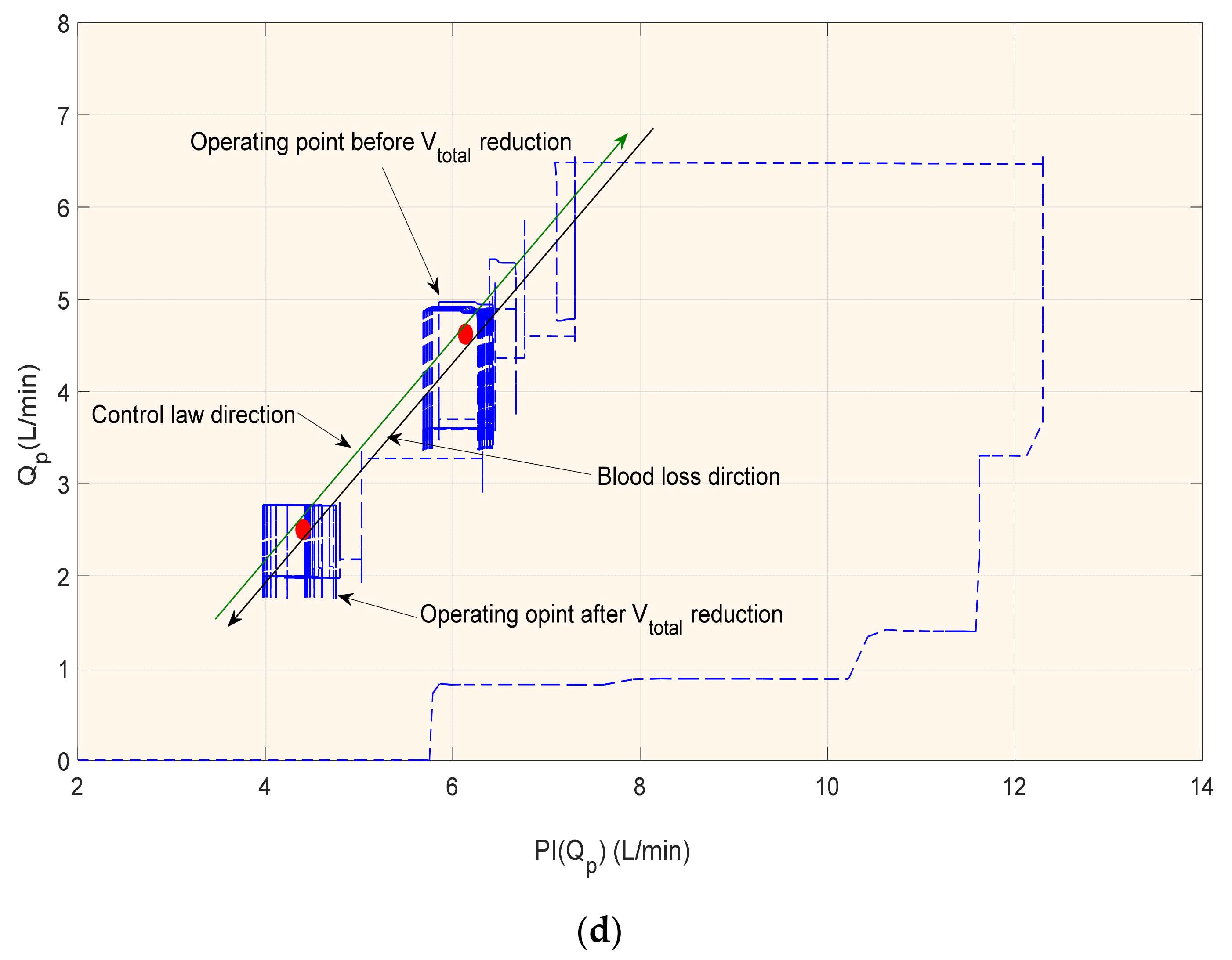
3.1. Rest Scenario or Blood Loss
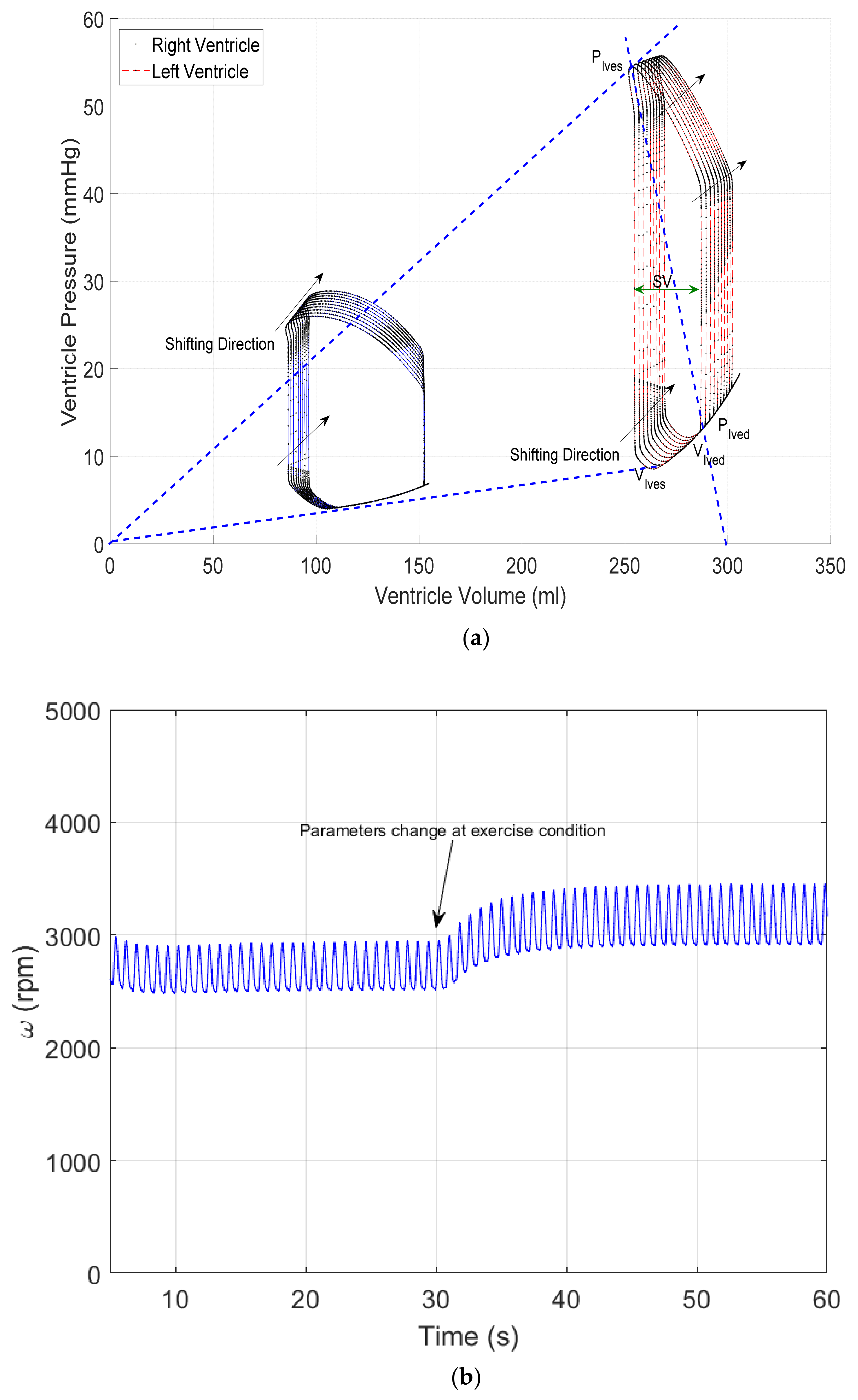
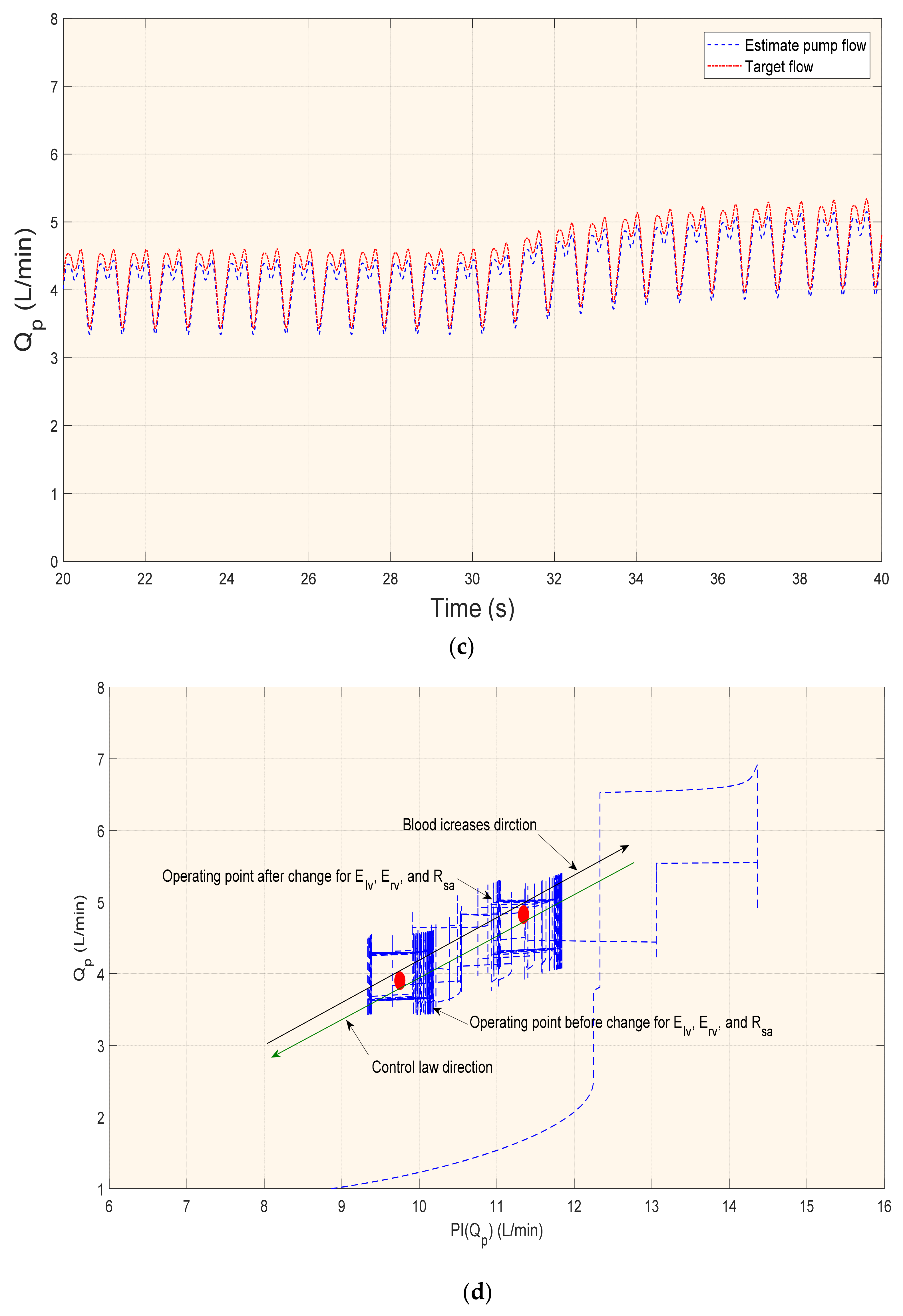
3.2. Exercise Scenario
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Description |
|---|---|
| cardiovascular System Model | |
| inlet cannula resistance | |
| outlet cannula resistance | |
| inlet cannula inductance | |
| outlet cannula inductance | |
| intrathoracic pressures | |
| suction resistance | |
| blood vessel compartment | |
| blood flow across the valves | |
| pressure in heart chamber | |
| Estimator Model | |
| pulse-width modulation | |
| pulsatility index of pump rotational speed | |
| pulsatile flow | |
| states of model estimator | |
| pump control input | |
| system noise | |
| Controller | |
| pulsatility of pump flow | |
| gradient angle | |
| lower linear fractional transformation | |
| positive semi-definite solutions to the Riccati equations | |
| controller gain | |
| estimator gain | |
| positive scalar | |
| controller matrix | |
| plant (LVAD) | |
References
- Cowie, M.R. The heart failure epidemic: A UK perspective. Echo Res. Pract. 2017, 4, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowie, M.R. Incidence and aetiology of heart failure; a population-based study. Eur. Heart J. 1999, 20, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Cowie, M.; Wood, D.; Coats, A.; Gibbs, J.; Underwood, S.; Turner, R.; Poole-Wilson, P.; Davies, S.; Sutton, G. Coronary artery disease as the cause of incident heart failure in the population. Eur. Heart J. 2001, 22, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Schmitto, J.D. The evolution of mechanical circulatory support (MCS): A new wave of developments in MCS and heart failure treatment. J. Thorac. Dis. 2018, 10 (Suppl. S15), S1688. [Google Scholar] [CrossRef]
- Frazier, O.H. Mechanical cardiac assistance: Historical perspectives. Semin. Thorac. Cardiovasc. Surg. 2000, 12, 207–219. [Google Scholar] [CrossRef]
- Mehra, M.R.; Uriel, N.; Naka, Y.; Cleveland, J.C., Jr.; Yuzefpolskaya, M.; Salerno, C.T.; Walsh, M.N.; Milano, C.A.; Patel, C.B.; Hutchins, S.W.; et al. A fully magnetically levitated left ventricular assist device. N. Engl. J. Med. 2019, 380, 1618–1627. [Google Scholar] [CrossRef]
- Pac, M.; Kocabeyoglu, S.S.; Kervan, U.; Sert, D.E.; Koca, S.; Ece, I.; Pac, F.A. Third generation ventricular assist device: Mid-term outcomes of the HeartWare HVAD in pediatric patients. Artif. Organs 2018, 42, 141–147. [Google Scholar] [CrossRef]
- Bozkurt, S. Physiologic outcome of varying speed rotary blood pump support algorithms: A review study. Australas. Phys. Eng. Sci. Med. 2016, 39, 13–28. [Google Scholar] [CrossRef]
- Stevens, M.C.; Stephens, A.; AlOmari, A.H.H.; Moscato, F. Physiological control. In Mechanical Circulatory and Respiratory Support; Elsevier Inc.: Amsterdam, The Netherlands, 2018; pp. 627–657. [Google Scholar]
- AlOmari, A.H.; Savkin, A.V.; Stevens, M.; Mason, D.G.; Timms, D.L.; Salamonsen, R.F.; Lovell, N.H. Developments in control systems for rotary left ventricular assist devices for heart failure patients: A review. Physiol. Meas. 2012, 34, 1. [Google Scholar] [CrossRef]
- Fetanat, M.; Stevens, M.; Hayward, C.; Lovell, N.H. A Sensorless Control System for an Implantable Heart Pump using a Real-time Deep Convolutional Neural Network. IEEE Trans. Biomed. Eng. 2021, 68, 3029–3038. [Google Scholar] [CrossRef]
- Bakouri, M.A.; Salamonsen, R.F.; Savkin, A.V.; AlOmari, A.H.; Lim, E.; Lovell, N.H. A Sliding Mode-Based Starling-Like Controller for Implantable Rotary Blood Pumps. Artif. Organs 2014, 38, 587–593. [Google Scholar] [CrossRef]
- Huang, F.; Ruan, X.; Fu, X. Pulse-pressure–enhancing controller for better physiologic perfusion of rotary blood pumps based on speed modulation. ASAIO J. 2014, 60, 269–279. [Google Scholar] [CrossRef]
- Wu, Y.; Allaire, P.E.; Tao, G.; Olsen, D. Modeling, estimation, and control of human circulatory system with a left ventricular assist device. IEEE Trans. Control Syst. Technol. 2007, 15, 754–767. [Google Scholar] [CrossRef]
- Arndt, A.; Nüsser, P.; Graichen, K.; Müller, J.; Lampe, B. Physiological control of a rotary blood pump with selectable therapeutic options: Control of pulsatility gradient. Artif. Organs 2008, 32, 761–771. [Google Scholar] [CrossRef]
- Chang, Y.; Gao, B.; Gu, K. A model-free adaptive control to a blood pump based on heart rate. Asaio J. 2011, 57, 262–267. [Google Scholar] [CrossRef]
- Son, J.; Du, D.; Du, Y. Feedback Control of Rotary Blood Pump for Preventing Left Ventricular Suction. In Proceedings of the 2019 American Control Conference (ACC), Philadelphia, PA, USA, 10–12 July 2019; pp. 5426–5431. [Google Scholar]
- Petukhov, D.; Korn, L.; Walter, M.; Telyshev, D. A novel control method for rotary blood pumps as left ventricular assist device utilizing aortic valve state detection. BioMed Res. Int. 2019, 2019, 1732160. [Google Scholar] [CrossRef] [Green Version]
- Telyshev, D.V. A Mathematical Model for Estimating Physiological Parameters of Blood Flow through Rotary Blood Pumps. Biomed. Eng. 2020, 54, 163–168. [Google Scholar] [CrossRef]
- Wang, Y.; Peng, J.; Rodefeld, M.D.; Luan, Y.; Giridharan, G.A. A sensorless physiologic control strategy for continuous flow cavopulmonary circulatory support devices. Biomed. Signal Process. Control 2020, 62, 102130. [Google Scholar] [CrossRef]
- Ayre, P.J.; Vidakovic, S.S.; Tansley, G.D.; Watterson, P.A.; Lovell, N.H. Sensorless flow and head estimation in the VentrAssist rotary blood pump. Artif. Organs 2020, 24, 585–588. [Google Scholar] [CrossRef]
- Wang, Y.; Koenig, S.C.; Slaughter, M.S.; Giridharan, G.A. Rotary blood pump control strategy for preventing left ventricular suction. ASAIO J. 2015, 61, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Saito, I.; Isoyama, T.; Nakagawa, H.; Emiko, N.; Ono, T.; Shi, W.; Inoue, Y.; Abe, Y. Development of Normal-Suction Boundary Control Method Based on Inflow Cannula Pressure Waveform for the Undulation Pump Ventricular Assist Device. Artif. Organs 2012, 36, 812–816. [Google Scholar] [CrossRef] [PubMed]
- Reesink, K.; Dekker, A.; Van der Nagel, T.; Beghi, C.; Leonardi, F.; Botti, P.; De Cicco, G.; Lorusso, R.; Van der Veen, F.; Maessen, J. Suction due to left ventricular assist: Implications for device control and management. Artif. Organs 2007, 31, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Meki, M.; Wang, W.; Sethu, P.; El-Baz, A.; Giridharan, G.A.; Wang, Y. A suction index based control system for rotary blood pumps. Biomed. Signal Process. Control 2020, 62, 102057. [Google Scholar] [CrossRef]
- Salamonsen, R.; Mason, D.; Ayre, P. Response of Rotary Blood Pumps to Changes in Preload and Afterload at a Fixed Speed Setting Are Unphysiological When Compared with the Natural Heart. Artif. Organs 2011, 35, E47–E53. [Google Scholar] [CrossRef]
- Salamonsen, R.F.; Lim, E.; Gaddum, E.; Alomari, A.H.; Gregory, S.D.; Stevens, M.; Mason, D.G.; Fraser, J.F.; Timms, D.; Karunanithi, M.K.; et al. Theoretical foundations of a Starling-like controller for rotary blood pumps. Artif. Organs 2012, 36, 787–796. [Google Scholar] [CrossRef]
- Bakouri, M.A.; Savkin, A.V.; Alomari, A.H. Nonlinear modelling and control of left ventricular assist device. Electron. Lett. 2015, 51, 613–615. [Google Scholar] [CrossRef]
- Xu, S.Y.; Chen, T.W. Robust H-infinity control for uncertain stochastic systems with state delay. IEEE Trans. Autom. Control 2002, 47, 2089–2094. [Google Scholar]
- Lim, E.; Dokos, S.; Salamonsen, R.; Rosenfeldt, F.; Ayre, P.; Lovell, N. Numerical Optimization Studies of Cardiovascular-Rotary Blood Pump Interaction. Artif. Organs 2012, 36, E110–E124. [Google Scholar] [CrossRef]
- Giridharan, G.; Skliar, M. Control Strategy for Maintaining Physiological Perfusion with Rotary Blood Pumps. Artif. Organs 2003, 27, 639–648. [Google Scholar] [CrossRef]
- Arndt, A.; Nüsser, P.; Lampe, B. Fully autonomous preload-sensitive control of implantable rotary blood pumps. Artif. Organs 2010, 34, 726–735. [Google Scholar] [CrossRef]
- Wu, Y. Adaptive physiological speed/flow control of rotary blood pumps in permanent implantation using intrinsic pump parameters. Asaio J. 2009, 55, 335–339. [Google Scholar] [CrossRef]
- Pauls, J.P.; Stevens, M.C.; Bartnikowski, N.; Fraser, J.F.; Gregory, S.D.; Tansley, G. Evaluation of physiological control systems for rotary left ventricular assist devices: An in-vitro study. Ann. Biomed. Eng. 2016, 44, 2377–2387. [Google Scholar] [CrossRef]
- Shekar, K.; Gregory, S.D.; Fraser, J.F. Mechanical circulatory support in the new era: An overview. Crit. Care 2016, 20, 66. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Koenig, S.C.; Wu, Z.; Slaughter, M.S.; Giridharan, G.A. Sensor-based physiologic control strategy for biventricular support with rotary blood pumps. Asaio J. 2018, 64, 338–350. [Google Scholar] [CrossRef]
- Fetanat, M.; Stevens, M.; Hayward, C.; Lovell, N.H. A physiological control system for an implantable heart pump that accommodates for interpatient and intrapatient variations. IEEE Trans. Biomed. Eng. 2019, 67, 1167–1175. [Google Scholar] [CrossRef] [Green Version]
- Petrou, A.; Monn, M.; Meboldt, M.; Schmid Daners, M. A novel multi-objective physiological control system for rotary left ventricular assist devices. Ann. Biomed. Eng. 2017, 45, 2899–2910. [Google Scholar] [CrossRef]
- Creager, M.A. Baroreceptor reflex function in congestive heart failure. Am. J. Cardiol. 1992, 69, 10–16. [Google Scholar] [CrossRef]








| Variable | Unit | Healthy | Heart Failure (HF) |
|---|---|---|---|
| mL | 5300 | 5800 | |
| mm Hg/mL | 1.7235 | 0.5322 | |
| mm Hg/mL | 3.5443 | 0.7100 | |
| mm Hg*s/mL | 0.7411 | 1.1100 |
| Variable | Unit | HF + LVAD | ||
|---|---|---|---|---|
| Normal | Rest | Exercise | ||
| Target flow (Qt) | L/min | 4.95 | 3.65 | 5.52 |
| Pump flow (Q) | L/min | 4.5 | 3.40 | 5.05 |
| Left ventricle end-diastolic volume (Vlved) | mL | 120 | 140.00 | 285.3 |
| Left ventricle end-diastolic pressure (Plved) | mmHg | 9.50 | 8.50 | 12.79 |
| Left ventricle end-systolic volume (Vlves) | mL | 65.50 | 50.00 | 252.4 |
| Left ventricle end-systolic pressure (Plves) | mmHg | 120 | 116.5 | 53.50 |
| Stroke volume (SV) | mL | 102.00 | 90.00 | 35.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakouri, M.; Alassaf, A.; Alshareef, K.; Abdelsalam, S.; Ismail, H.F.; Ganoun, A.; Alomari, A.-H. An Optimal H-Infinity Controller for Left Ventricular Assist Devices Based on a Starling-like Controller: A Simulation Study. Mathematics 2022, 10, 731. https://doi.org/10.3390/math10050731
Bakouri M, Alassaf A, Alshareef K, Abdelsalam S, Ismail HF, Ganoun A, Alomari A-H. An Optimal H-Infinity Controller for Left Ventricular Assist Devices Based on a Starling-like Controller: A Simulation Study. Mathematics. 2022; 10(5):731. https://doi.org/10.3390/math10050731
Chicago/Turabian StyleBakouri, Mohsen, Ahmed Alassaf, Khaled Alshareef, Saleh Abdelsalam, Husham Farouk Ismail, Ali Ganoun, and Abdul-Hakeem Alomari. 2022. "An Optimal H-Infinity Controller for Left Ventricular Assist Devices Based on a Starling-like Controller: A Simulation Study" Mathematics 10, no. 5: 731. https://doi.org/10.3390/math10050731