Attitudes of Children with Hearing Loss towards Public Inclusive Education



Abstract
:1. Introduction
1.1. Organising Principles of IE for Children and Adolescents with Hearing Loss
1.2. Family Intervention and Participation
1.3. Collaborative Teamwork in a School Centre
1.4. The Implantation of Hearing Assistive Devices
1.4.1. Age of Implementation and Timely Access to Educational Services
1.4.2. Hearing Assistive Devices and Communication Technology for Children and Adolescents with Hearing Loss
1.5. Support of Communication Modes
1.6. Evaluation of Students with Hearing Loss
1.7. Self-Assessment of Perceptions and Attitudes
- (1)
- The theory of “reasoned action” that investigates the determinants of children’s attitudes and behavioural intentions towards classmates with physical disabilities, measured by the Peer Attitudes Toward the Handicapped Scale (PATHS) and Behavioural Intention Scale [26];
- (2)
- The “Contact theory” (i.e., the intergroup contact with students with disabilities) [27];
- (3)
- The “Gestalt therapy theory” which envisions the self-capability of making contact with the environment (e.g., symbolic numerical comparisons, [28]);
- (4)
- The “Dialogical Theory of Self” (i.e., interconnectedness of individuals with society [29] (p. 3). These tools are designed to comprehend how children with difficulties achieve an awareness of their sense of self.
1.8. Problem
2. Method
2.1. Participants
2.2. Process
2.3. Instrumentation
2.4. Analysis of Data
3. Results
3.1. Factor Structure
3.2. Reliability
- (1)
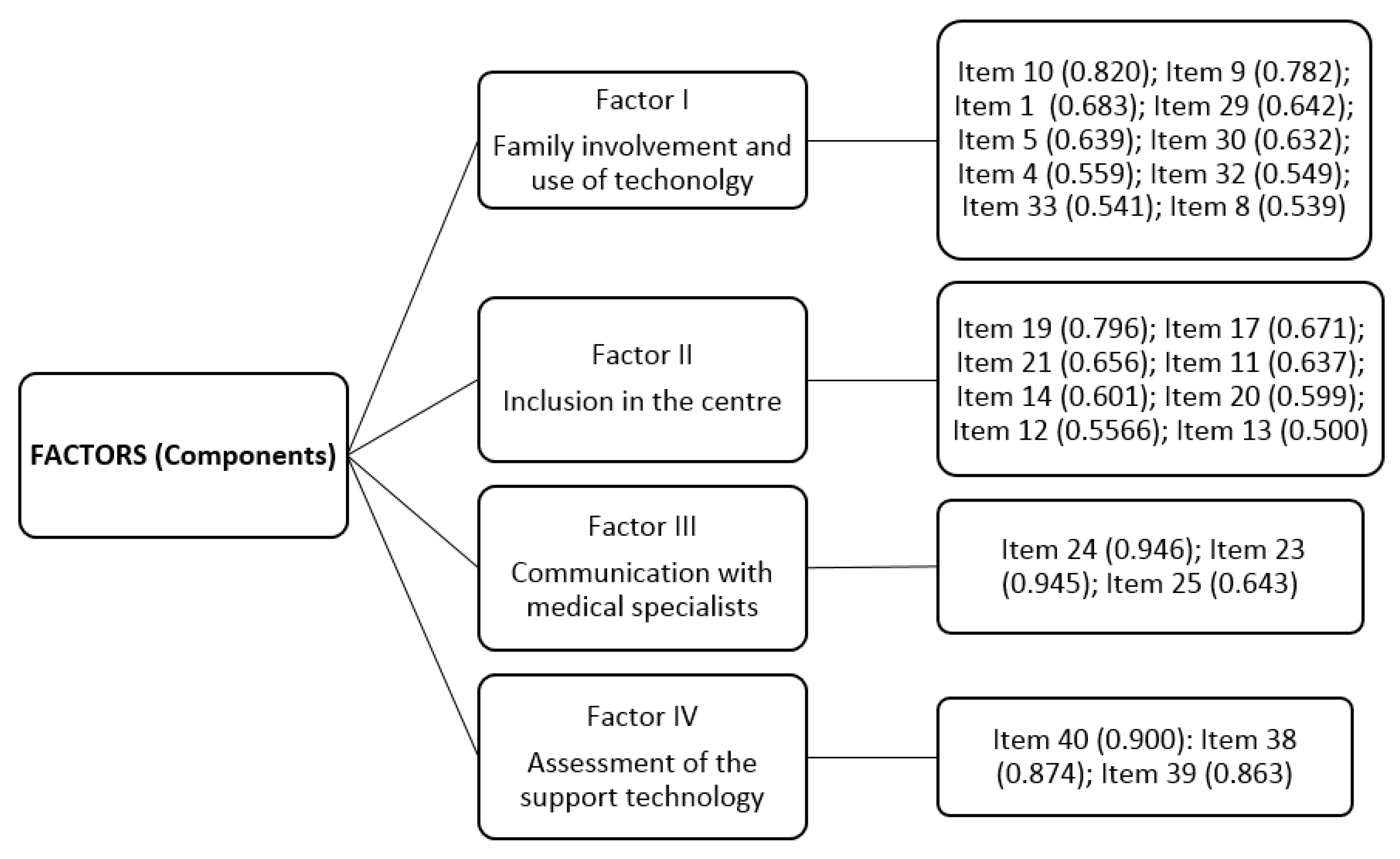
- Factor 1 consisted of 10 items, accounted for 14.038% of the variance, and was named Family involvement and use of technology, with one item weighing the most (“My father helps with housework”), representing 67.24% (0.820), followed by ”My father comes to meetings at school”, which represented 61.15% (0.782);
- (2)
- Factor 2 consisted of eight items, accounted for 13.527% of the variance, and was named Inclusion in the centre. The item “I receive adequate medical attention at school”, represented 63.36% (0.796), followed by the item “I have sufficiently prepared teachers”, which represented 45.02% (0.671);
- (3)
- Factor 3 consisted of three items, accounted for 11.43% of the variance, and was named Communication with medical specialists. The item of the greatest weight was “I received detailed medical chart information of insertion results after implantation”, which represented 89.49% (0.946). This was followed by the item “I received detailed medical chart information of insertion results before implantation”, which represented 89.30% (0.945);
- (4)
- Factor 4 consisted of three items, accounted for 8.057% of the variance, and was named Assessment of the support technology. The item with the greatest weight was “I assess the use of visual aids,” which represented 81% (0.900), followed by the item “I believe the use of digital blackboards,” which represented 76.38% (0.874). (See Figure 1).
4. Discussion
4.1. Limitations
4.2. Recommendations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- LISMI. Ley 13/1982, de 7 de abril, de Integración Social de los Minusválidos. Boletín Oficial del Estado, 20 April 1982. [Google Scholar]
- Woolf, S.B. Critical Skills for Special Educator Effectiveness: Which ones Matter Most and to Whom? Teach. Educ. Spec. Educ. 2019, 42, 132–146. [Google Scholar] [CrossRef]
- Moeller, M.P.; Carr, G.; Seaver, L.; Stredler-Brown, A.; Holzinger, D. Best Practices in Family-Centered Early Intervention for Children Who Are Deaf or Hard of Hearing: An International Consensus Statement. J. Deaf. Stud. Deaf. Educ. 2013, 18, 429–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schick, B.; Skalicky, A.; Edwards, T.; Kushalnagar, P.; Topolski, P.; Patrick, D. School placement and perceived quality of life in youth who are deaf or hard of hearing. J. Deaf Stud. Deaf Educ. 2013, 18, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Davenport, C.A.; Alber-Morgan, S.R. I Have a Child With a Cochlear Implant in My Preschool Classroom. Now What? Teach. Except. Child. 2016, 49, 41–48. [Google Scholar] [CrossRef]
- Scott, J.A.; Kasun, G.S. It’s not enough to move your hands beautifully’: teaching and learning at a school for deaf students in Mexico. Int. J. Biling. Educ. Biling. 2018, 1–19. [Google Scholar] [CrossRef]
- Chute, P.M.; Nevins, M.E. School Professionals Working with Children with Cochlear Implants; Plural Publishing: San Diego, CA, USA, 2006. [Google Scholar]
- Cepa, A.; Heras, D.; Fernández-Hawryla, M. La educación emocional en la infancia: Una estrategia inclusive. Aula Abierta 2017, 46, 73–82. [Google Scholar] [CrossRef]
- Amiama, J.F.; Ledesma, N.; Monzón, J. La participación del alumnado en proyectos educativos vinculados al territorio: Propuestas inclusivas en un centro escolar de secundaria. Aula Abierta 2017, 46, 91–96. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy. In Encyclopedia of Human Behavior; Ramachaudran, V.S., Ed.; Academic Press: New York, NY, USA, 1994; Volume 4, pp. 71–81. [Google Scholar]
- Sharma, U.; Jitoko, F.; Macanawai, S.S.; Forlin, C. How Do we Measure Implementation of Inclusive Education in the Pacific Islands? A Process for Developing and Validating Disability-Inclusive Indicators. Int. J. Disabil. Dev. Educ. 2018, 65, 614–630. [Google Scholar] [CrossRef]
- Radici, E.; Heboyan, V.; Mantovani, F.; De Leo, G. Teachers’ Attitudes Towards Children Who Use AAC in Italian Primary Schools. Int. J. Disabil. Dev. Educ. 2018, 66, 284–297. [Google Scholar] [CrossRef]
- Moore, B.C.J. Cochlear Hearing Loss: Physiological, Psychological and Technical Issues, 2nd ed.; Online; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2008. [Google Scholar]
- Noble, W. Self-Assessment of Hearing, 2nd ed.; Plural Publishing: San Diego, CA, USA, 2013. [Google Scholar]
- Tomblin, J.B.; Barker, B.A.; Spencer, L.J.; Zhang, X.; Gantz, B.J. The Effect of Age at Cochlear Implant Initial Stimulation on Expressive Language Growth in Infants and Toddlers. J. Speech Lang. Hear. Res. 2005, 48, 853–867. [Google Scholar] [CrossRef] [Green Version]
- Bakar, Z.A.; Brown, P.M.; Remine, M.D. Sensitivity in Interactions between Hearing Mothers and their Toddlers with Hearing Loss: The Effect of Cochlear Implantation. Deaf. Educ. Int. 2010, 12, 2–15. [Google Scholar] [CrossRef]
- Geers, A.E.; Nicholas, J.; Tobey, E.; Davidson, L. Persistent Language Delay Versus Late Language Emergence in Children With Early Cochlear Implantation. J. Speech Lang. Hear. Res. 2016, 59, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt, R.F.; Beer, J.; Kronenberger, W.G.; Pisoni, D.B.; LaLonde, K. Contribution of Family Environment to Pediatric Cochlear Implant Users’ Speech and Language Outcomes: Some Preliminary Findings. J. Speech Lang. Hear. Res. 2012, 55, 848–864. [Google Scholar] [CrossRef]
- Moos, R.H.; Moos, B.S. Family Environment Scale Manual, 4th ed.; Mind Garden: Menlo Park, CA, USA, 2009. [Google Scholar]
- Maidment, D.W.; Kang, H.J.; Stewart, H.J.; Amitay, S. Audiovisual Integration in Children Listening to Spectrally Degraded Speech. J. Speech Lang. Hear. Res. 2015, 58, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Hyde, M.; Punch, R. The Modes of Communication Used by Children with Cochlear Implants and Role of Sign in Their Lives. Am. Ann. Deaf. 2011, 155, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Gale, E. Exploring Perspectives on Cochlear Implants and Language Acquisition Within the Deaf Community. J. Deaf Stud. Deaf Educ. 2011, 16, 121–139. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, A.; Nittrouer, S. Speech Perception in Noise by Children With Cochlear Implants. J. Speech, Lang. Hear. Res. 2013, 56, 13–30. [Google Scholar] [CrossRef] [Green Version]
- Bradham, T.S.; Houston, K.T. Assessing Listening and Spoken Language in Children with Hearing Loss; Plural Publishing: San Diego, CA, USA, 2014. [Google Scholar]
- Bellis, T.J. Assessment and Management of Central Auditory Processing Disorders in the Educational Setting: From Science to Practice, 2nd ed.; Plural Publishing: San Diego, CA, USA, 2011. [Google Scholar]
- Roberts, C.M.; Lindsell, J.S. Children’s Attitudes and Behavioural Intentions Towards Peers with Disabilities. Int. J. Disabil. Dev. Educ. 1997, 44, 133–145. [Google Scholar] [CrossRef]
- Hung, H.-L.; Paul, P.V. Inclusion of Students who are Deaf or Hard of Hearing: Secondary School Hearing Students’ Perspectives. Deaf. Educ. Int. 2006, 8, 62–74. [Google Scholar] [CrossRef]
- Arfé, B.; Lucangeli, D.; Genovese, E.; Monzani, D.; Gubernale, M.; Trevisi, P.; Santarelli, R. Analogic and Symbolic Comparison of Numerosity in Preschool Children with Cochlear Implants. Deaf. Educ. Int. 2011, 13, 34–45. [Google Scholar] [CrossRef]
- Grobler, H.B.; Wessels, S. Hear Their Voices: Self-configuration Experiences of Learners with Mild Learning Difficulties within the Learner–Teacher Relationship. Int. J. Disabil. Dev. Educ. 2018, 1–20. [Google Scholar] [CrossRef]
- Nowicki, E.A.; Sandieson, R. A Meta-Analysis of School-Age Children’s Attitudes Towards Persons with Physical or Intellectual Disabilities. Int. J. Disabil. Dev. Educ. 2002, 49, 243–265. [Google Scholar] [CrossRef]
- Beaulieu-Bergeron, R.; Morin, D. A Qualitative Investigation of Fifth- and Sixth-grade Students’ Attitudes towards Intellectual Disability. Int. J. Disabil. Dev. Educ. 2016, 63, 514–528. [Google Scholar] [CrossRef]
- Most, T.; Wiesel, A.; Blitzer, T. Identity and Attitudes towards Cochlear Implant Among Deaf and Hard of Hearing Adolescents. Deaf. Educ. Int. 2007, 9, 68–82. [Google Scholar] [CrossRef]
- Rekkedal, A.M. Assistive Hearing Technologies Among Students With Hearing Impairment: Factors That Promote Satisfaction. J. Deaf. Stud. Deaf. Educ. 2012, 17, 499–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gent, T.; Goedhart, A.W.; Knoors, H.E.T.; Westenberg, P.M.; Treffers, P.D.A. Self-concept and Ego Development in Deaf Adolescents: A Comparative Study. J. Deaf. Stud. Deaf. Educ. 2012, 17, 333–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, R.; Cinamon, R.G.; Most, T. What Shapes Adolescents’ Future Perceptions? The Effects of Hearing Loss, Social Affiliation, and Career Self-Efficacy. J. Deaf. Stud. Deaf. Educ. 2015, 20, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Antia, S.D.; Sabers, D.L.; Stinson, M.S. Validity and Reliability of the Classroom Participation Questionnaire With Deaf and Hard of Hearing Students in Public Schools. J. Deaf. Stud. Deaf. Educ. 2007, 12, 158–171. [Google Scholar] [CrossRef] [PubMed]
- Booth, T.; Ainscow, M. Index for Inclusion: Developing Learning and Participation in Schools; Centre for Studies on Inclusive Education (CSIE): Bristol, UK, 2002. [Google Scholar]
- Deng, M.; Wang, S.; Guan, W.; Wang, Y. The development and initial validation of a questionnaire of inclusive teachers’ competency for meeting special educational needs in regular classrooms in China. Int. J. Incl. Educ. 2017, 21, 416–427. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; SAGE Publications: London, UK, 2009. [Google Scholar]
- Hutcheson, G.; Sofroniou, N. The Multivariate Social Scientist; SAGE Publications: London, UK, 1999. [Google Scholar]
- Yong, A.G.; Pearce, S. A Beginner’s Guide to Factor Analysis: Focusing on Exploratory Factor Analysis. Tutorials Quant. Methods Psychol. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- Thurstone, L.L. Attitudes Can Be Measured. Am. J. Sociol. 1928, 33, 529–554. [Google Scholar] [CrossRef]
- Hintermair, M.; Albertini, J.A. Ethics, Deafness, and New Medical Technologies. J. Deaf. Stud. Deaf. Educ. 2005, 10, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Mouvet, K.; Matthijs, L.; Loots, G.; Taverniers, M.; Van Herreweghe, M. The language development of a deaf child with a cochlear implant. Lang. Sci. 2013, 35, 59–79. [Google Scholar] [CrossRef]
- Kecman, E. Old challenges, changing contexts: Reviewing and reflecting on information provision for parents of children who are deaf or hard-of-hearing. Deaf. Educ. Int. 2019, 21, 3–24. [Google Scholar] [CrossRef]
- Ching, T.Y.C.; Scarinci, N.; Marnane, V.; Sjahalam-King, J.; Button, L.; Whitfield, J. Factors influencing parents’ decisions about communication choices during early education of their child with hearing loss: A qualitative study. Deaf. Educ. Int. 2018, 20, 154–181. [Google Scholar] [CrossRef] [PubMed]
- Wiley, S.; Arjmand, E.; Derr, J.M.; Dixon, M. Findings from multidisciplinary evaluation of children with permanent hearing loss. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 1040–1044. [Google Scholar] [CrossRef]
- Meinzen-Derr, J.; Wiley, S.; McAuley, R.; Smith, L.; Grether, S. Technology-assisted language intervention for children who are deaf or hard-of-hearing; a pilot study of augmentative and alternative communication for enhancing language development. Disabil. Rehabil. Assist. Technol. 2017, 12, 808–815. [Google Scholar] [CrossRef]
- Garberoglio, C.L.; Gobble, M.E.; Cawthon, S.W. A National Perspective on Teachers’ Efficacy Beliefs in Deaf Education. J. Deaf. Stud. Deaf. Educ. 2012, 17, 367–383. [Google Scholar] [CrossRef]
- Mayer, C.; Trezek, B.J. Literacy Outcomes in Deaf Students with Cochlear Implants: Current State of the Knowledge. J. Deaf Stud. Deaf Educ. 2018, 23, 1–16. [Google Scholar] [CrossRef]
- Alegre, O.M.; Rodríguez, M.C.; Villar, L.M.; Pérez, D. Evaluación De La Eficacia Del Implante Coclear En Función De La Edad De Implantación. Eur. Sci. J. ESJ 2016, 12, 42–51. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C. Principles and Guidelines for Early Intervention After Confirmation That a Child Is Deaf or Hard of Hearing. J. Deaf Stud. Deaf Educ. 2014, 19, 143–175. [Google Scholar] [CrossRef] [PubMed]
- Archbold, S.; Mayer, C. Deaf Education: The Impact of cochlear implantation? Deaf. Educ. Int. 2012, 14, 2–15. [Google Scholar] [CrossRef]
- Black, R.D.; Weinberg, L.A.; Brodwin, M.G. Universal Design for Learning and Instruction: Perspectives of Students with Disabilities in Higher Education. Except. Educ. Int. 2015, 25, 1–26. [Google Scholar]


{kind=link}
| ICAQ Items | Factors | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| 10. My father helps with housework | 0.820 | |||
| 9. My father comes to meetings at school | 0.782 | |||
| 1. My father and/or mother reviews homework | 0.683 | |||
| 29. I believe the use of magnetic loop antennas | 0.642 | |||
| 5. My father and/or mother attends and participates at school activities (i.e., shows, sports) | 0.639 | |||
| 30. I believe the use of the Roger system | 0.632 | |||
| 4. My father and/or mother requests meetings with tutors to have information related with logopaedic treatment, implant, adaptations | 0.559 | |||
| 32. I believe the use of digital blackboards | 0.549 | |||
| 33. I believe the use of image presentations | 0.541 | |||
| 8. My mother helps with homework | 0.539 | |||
| 19. I receive adequate medical attention at school | 0.796 | |||
| 17. I have sufficiently prepared teachers | 0.671 | |||
| 21. I have support from specialists who improve communication at school | 0.656 | |||
| 11. I feel welcome at school | 0.637 | |||
| 14. The school makes efforts to avoid discrimination practices | 0.601 | |||
| 20. I have technological aids that help communication | 0.599 | |||
| 12. The school sets high expectations for students | 0.566 | |||
| 13. Schoolteachers think that all students are equally important | 0.500 | |||
| 24. (If you use implanted devices) I received detailed medical chart information of insertion results after implantation | 0.946 | |||
| 23. (If you use implanted devices) I received detailed medical chart information of insertion results before implantation | 0.945 | |||
| 25. (If you use implanted devices) I have satisfactory communication with the medical team because they speak in a clear, direct and understandable way | 0.643 | |||
| 40. I assess the use of visual aids | 0.900 | |||
| 38. I assess the use of the Roger system | 0.874 | |||
| 39. I assess the use of the FM listening systems | 0.863 | |||
| Factors | |||||
|---|---|---|---|---|---|
| t | CI (n = 184) | HA (n = 113) | |||
| t-Student | M | SD | M | SD | |
| 1. Family involvement and use of technology | −0.905 n.s. | 2.77 | 0.725 | 2.85 | 0.752 |
| 2. Inclusion in the Centre | 15.38 *** | 3.31 | 0.543 | 2.29 | 0.575 |
| 3. Communication with medical specialists | 32.13 *** | 1.96 | 0.830 | ||
| 4. Assessment of the support technology | 21.437 *** | 3.30 | 0.965 | 1.23 | 0.430 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alegre de la Rosa, O.M.; Villar Angulo, L.M. Attitudes of Children with Hearing Loss towards Public Inclusive Education. Educ. Sci. 2019, 9, 244. https://doi.org/10.3390/educsci9030244
Alegre de la Rosa OM, Villar Angulo LM. Attitudes of Children with Hearing Loss towards Public Inclusive Education. Education Sciences. 2019; 9(3):244. https://doi.org/10.3390/educsci9030244
Chicago/Turabian StyleAlegre de la Rosa, Olga María, and Luis Miguel Villar Angulo. 2019. "Attitudes of Children with Hearing Loss towards Public Inclusive Education" Education Sciences 9, no. 3: 244. https://doi.org/10.3390/educsci9030244