
Human-in-Loop Decision-Making and Autonomy: Lessons Learnt from the Aviation Industry Transferred to Cyber-Physical Systems

Abstract
:1. Introduction
- Main research question (RQ): What are the important considerations in the design of future autonomous and intelligent systems (CPSs) when focusing on the results regarding the safety of decision-making processes and the accountability of these decisions?
- Sub-RQ1: What can we learn from the aviation industry in regard to human-in-the-loop decision-making by reviewing accident reports and considering accountability and safety as the main two metrics?
- Sub-RQ2: How can these findings then be translated to developing a methodological approach to be used in the design of autonomous CPSs?
2. Literature Review
2.1. Human-in-the-Loop Decision-Making
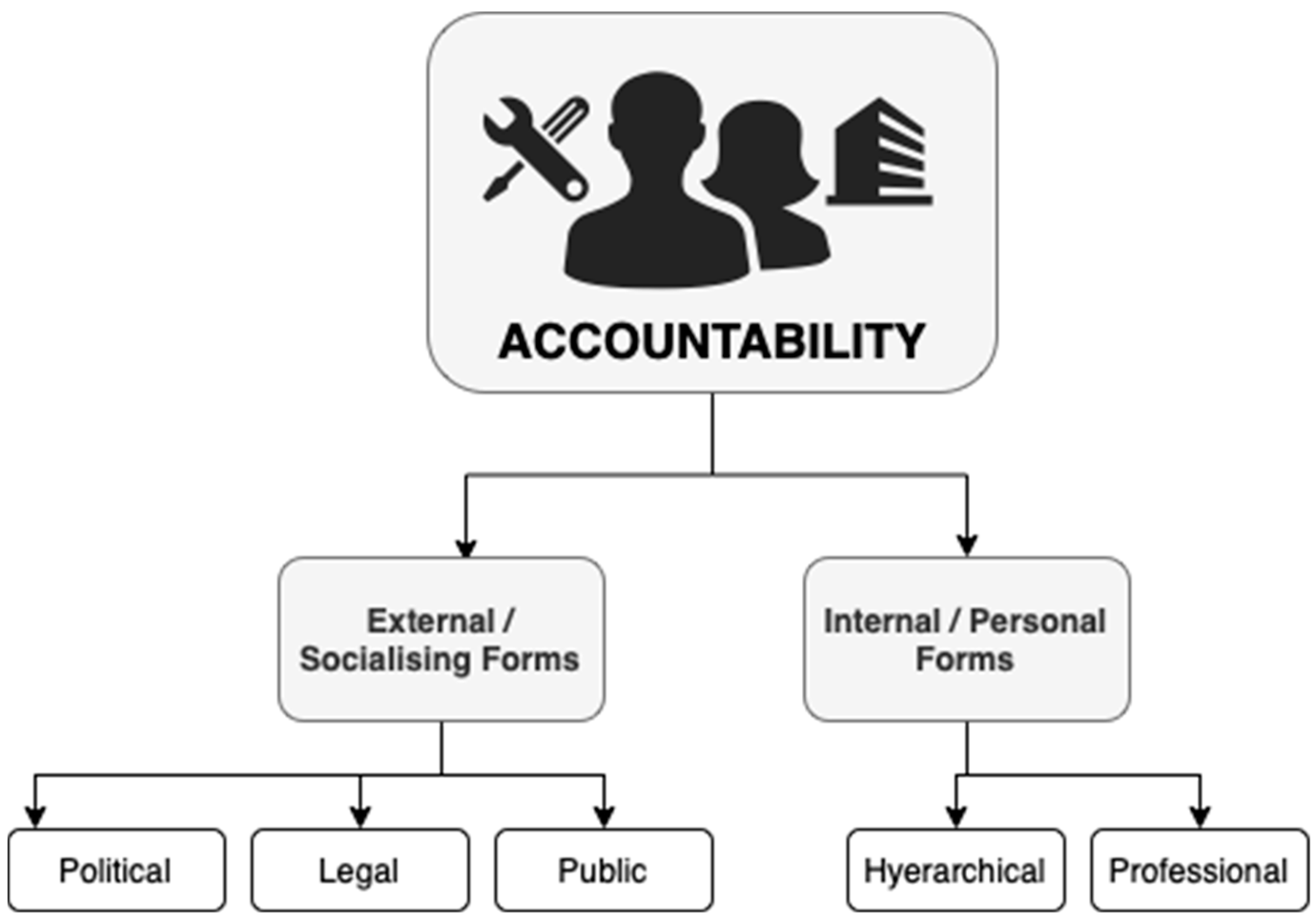
2.2. Accountability
2.3. Safety
3. Methodology
4. Data Analysis and Results
4.1. Data Collection
4.2. Preliminary Analysis and Results
4.3. Detailed Accident Report Analysis and Results
- Non-adherence to SOPs: Despite the strict standard operating processes that exist in the aviation industry, in our study we identified several cases in which one or more of the actors involved decided to deviate from at least one standard operating procedure. This category was the most frequent contributing factor to accidents. This category refers to any of the actors involved in an accident, for example, the crew, ATC, the airline, or even the supervisory authority, etc., and includes cases in which a process was not followed in day-to-day operations, in certification processes, during maintenance, during incident reporting, etc. Some examples are mentioned below:
“The majority of the air operator’s procedures, and in particular its safety management system, were only formal in nature and were not properly applied”
“The flight crew was accustomed to not complying with recognised rules for safe flight operations and taking high risks”
“The current regulation related to the personnel qualification for aerodrome personnel had not included several items as required by the ICAO standard, including requirement for radio telephony”
“Numerous incidents, including several serious incidents, were not reported to the competent bodies and authorities. This meant that they were unable to take measures to improve safety”
- Poor handling: This category refers to the poor handling of a situation by one or more of the actors involved in the accident. It can involve, for instance, poor decision-making, poor handling of equipment, poor crew resource management (CRM) on behalf of the crew, or even poor handling due to emotional or behavioural issues. Some examples are mentioned below:
Emotional/Behavioural Issues: “The first officer’s long history of training performance difficulties and his tendency to respond impulsively and inappropriately when faced with an unexpected event during training scenarios at multiple employers suggest an inability to remain calm during stressful situations—a tendency that may have exacerbated his aptitude-related performance difficulties”
CRM: “The flight crew did not effectively scan and monitor the primary flight instrumentation parameters during the landing and the attempted go-around”
Equipment: “use of the automatic flight mode (autopilot, autothrottle) in the flight under the windshear conditions which resulted in the aircraft being unstable (excess thrust) when turning to the manual control”
Decision-making: “The captain demonstrated inadequate aeronautical decision-making skills regarding which runway to use for landing and a lack of flight deck leadership by continuing the landing to a runway with a significant tailwind”
Operational: “Lack of effective oversight was observed in the part of operator as well as regulator at the departing airport”
- Failure to identify safety issues: This category refers to cases in which at least one of the involved actors had the opportunity to identify a safety issue but failed to do so.
“Performance reviews were conducted by those responsible in a manner which lacked critical rigour and ignored errors”
- Lack of SOP: This category refers to cases in which there were no proper SOPs available to one or more of the actors involved in the accident.
“In case of a missed approach, the OM (Operations Manual) - A Missed Approach flight procedures requires that the pilots shall advise air traffic control as soon as practicable. There was no guidance in the OM-A on what should be reported in case of a go-around”
- Lack of proper training: This category refers to cases in which there were deficiencies in the training of one or more of the actors involved in the accident. This could include not just the flight crew, but also emergency services, ATC, etc.
“Experienced flight crews who often made mistakes regarding basic flying skills (airspace violations, non-compliance with basic rules) during flight operations showed deficits in terms of operation-specific training and collaboration”
- Lack of proper equipment: This category refers to cases in which the proper equipment was not available at the time of the accident, contributing to the sequence of events. This could include equipment in the aircraft, the airport, ATC, training, etc.
“The absence of visual and aural alerts from both airplanes’ traffic display systems, while operating in a geographic area with a high concentration of air tour activity”
- Lack of proper communication: This category refers to cases in which there was a lack of proper communication between two or more of the actors involved in the incident.
“If the flight crew or the flight attendants had communicated after the airplane came to a stop, the flight crew could have become aware of the severity of the fire on the right side of the airplane and the need to expeditiously shut down the engines”
- Mechanical issue: This category refers to cases in which a mechanical issue also contributed to the accident.
“Contributing to the accident were (1) Saab’s design of the wheel speed transducer wire harnesses, which did not consider and protect against human error during maintenance”
- Lack of safety culture: In this study, we adopted the definition proposed by Cox and Cox [51] for “safety culture”, defining it as the reflection of “the attitudes, beliefs, perceptions, and values that employees share in relation to safety”. This category therefore refers to cases in which one or more of the involved organisations or actors did not exhibit an appropriate culture that promoted a culture of safety.
“The flight crews who did not adhere to generally accepted principles for safe flying in mountainous areas when operating the type ‘Ju 52/3m g4e’ aircraft were often those who had trained as Air Force pilots. In particular, they systematically and significantly flew below safe altitudes and violated the minimum separation from obstacles”
- Poor weather conditions: This category refers to cases in which poor weather conditions may have also contributed to the accident.
“An extreme loss of braking friction due to heavy rain and the water depth on the ungrooved runway, which resulted in viscous hydroplaning”
- Loss of situational awareness: This category refers to any cases in which the flight crew had lost the ability to have an “accurate perception and understanding of all the factors and conditions within the four fundamental risk elements (pilot, aircraft, environment, and type of operation) that affect safety before, during, and after the flight” [61].
“During the critical phase of final approach PIC (PF) lost situational awareness and deviated to the right by almost 15 degree and also descended below threshold height. He could not even pay attention to the FO’s call out alerting the excessive descend”
- Lack of proper maintenance: This category refers to cases in which any related equipment (including aircraft or airport equipment, emergency services equipment, etc.) may have contributed to the accident.
“In many instances, the quality of the remanufactured and reconditioned aircraft parts was poor.”
- Lack of required personnel: This category refers to cases in which a lack of required personnel contributed to the accident. This could be, for example, the case for the airline, the airport, the maintenance team, or even the supervisory authority.
“Though Lukla Tower was supposed to be two-man console, there was only one ATS Officer on duty at the time of accident.”
- Hierarchy issues: This category refers to cases in which an individual may have had to question a superior officer and therefore refrained from taking any action. Despite the strict hierarchical structures of authority that exist in the aerospace industry, this category only contributed to four of the analyzed accidents.
“Inability of the copilot (PM) to take control of the aircraft and proper action to execute go-around”
- Design issue(s): This category refers to cases in which an aircraft design issue contributed to the accident; this was found to be relevant to only three accidents.
“Although the aircraft’s ice-protection systems were activated on the approach to CZFD, the aircraft’s de-icing boots were not designed to shed all of the ice that can accumulate, and the anti-icing systems did not prevent ice accumulation on unprotected surfaces. As a result, some residual ice began to accumulate on the aircraft.”
“The accident was caused by insufficient operational prerequisites for the management of a failure in a redundant system”
5. Discussion
“Safety is the process of constantly driving towards zero incidents by managing both expected and unexpected hazards.”
6. Conclusions
- It is necessary to consider the actors, causes, and possible factors which may contribute to safety-related issues from the very beginning of the CPS design and implementation processes. The list of actors and factors identified in this study can form the basis for further analyses towards this goal in relation to CPSs.
- Although there should be well-defined procedures and supporting processes to identify accountability when safety-related issues arise in CPSs, there is also a need for both well-defined reporting procedures/practices and different levels of mechanisms that can be checked by diverse stakeholders in order to minimise the cascading nature of events and to be able to address stakeholder accountability and improve safety. Further research into high-reliability organisations (HROs) [67] can provide further insights for CPS. The HRO literature emerged following a number of tragic accidents, such as NASA’s Challenger explosion [67], when a new group of scholars proposed the HRO paradigm and focused their research on organisations that could not afford to fail [68,69,70]. A relevant point regarding the HRO literature is that its focus has shifted from identifying how accidents happen to identifying successful organisations [67]. HRO scholars have suggested that successful organisations that operate in hazardous conditions require the following characteristics: a culture of continuous improvement and learning, flexible structures, commitment to results and safety, a culture of reporting failures, effective communication, in-built human and system redundancy, outstanding technology, a commitment to standard operating procedures, and the establishment of minimum requirements [64,67,68,70,71,72,73,74,75,76,77,78,79]. The attributes identified in this study are clearly relevant to further research in this area, especially in regard to finding the right balance between flexible structures and standard procedures, as well as reporting incidents can provide further insights to ensure the safety of CPSs.
- We also propose the following definition of safety: “Safety is the process of constantly driving towards zero incidents by managing both expected and unexpected hazards.”
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Accident Code | Year | Manufacturer | Operator | From (Country) | Into (Country) | Fatalities |
|---|---|---|---|---|---|---|
| N59 | 2016 | Bombardier | West Air Sweden | Norway | Sweden | 2 |
| N61 | 2016 | DHC | Tara Air | Nepal | Nepal | 23 |
| N64 | 2016 | Boeing | Flydubai | UAE | Russia | 62 |
| N66 | 2016 | Boeing | Batik Air | Indonesia | Indonesia | 0 |
| N72 | 2016 | Boeing | Emirates | India | UAE | 1 |
| N75 | 2016 | Boeing | American Airlines | US | US | 0 |
| N78 | 2016 | BAE | LaMia Airlines | Bolivia | Colombia | 71 |
| N79 | 2016 | ATR | Pakistan International Airlines | Pakistan | Pakistan | 47 |
| N82 | 2017 | Boeing | Turkish Airlines | Kyrgyzstan | Kyrgyzstan | 4 |
| N86 | 2017 | Let Kunovice | Summit air | Nepal | Nepal | 2 |
| N87 | 2017 | Airbus | Air Canada | Canada | US | 0 |
| N88 | 2017 | Airbus | Air France | France | Canada | 0 |
| N91 | 2017 | ATR | West Wind Aviation | Canada | Canada | 1 |
| N97 | 2018 | Bombardier | US-Bangla Airlines | Bangladesh | Nepal | 51 |
| N98 | 2018 | Boeing | Southwest Airlines | US | US | 1 |
| N104 | 2018 | Junkers | Horizon Air | Switzerland | Switzerland | 20 |
| N107 | 2018 | Boeing | Utair | Russia | Russia | 0 |
| N109 | 2018 | Boeing | Lion Air | Indonesia | Indonesia | 189 |
| N112 | 2019 | Boeing | Atlas Air | US | US | 3 |
| N116 | 2019 | Boeing | Miami Air | Cuba | US | 0 |
| N118 | 2019 | Bombardier | Biman Bangladesh Airlines | Bangladesh | Bangladesh | 0 |
| N119 | 2019 | DHC | Mountain Air Service | US | US | 1 |
| N122 | 2019 | Antonov State Enterprise | Ukraine Air | Spain | Ukraine | 5 |
| N123 | 2019 | Saab | PenAir | US | US | 1 |
| N128 | 2020 | McDonnell Douglas | Caspian Airlines | Iran | Iran | 0 |
| N133 | 2020 | Boeing | Air India Express | UAE | India | 20 |
References
- Vagia, M.; Transeth, A.A.; Fjerdingen, S.A. A literature review on the levels of automation during the years. What are the different taxonomies that have been proposed? Appl. Ergon. 2016, 53, 190–202. [Google Scholar] [CrossRef]
- Cambridge Dictionary. Available online: https://dictionary.cambridge.org/dictionary/english/autonomy (accessed on 2 May 2022).
- Albus, J.; Antsaklis, P.J.; Meystel, A.; Passino, K.; Samad, T. Autonomy in Engineering Systems: What is it and Why it is Important? Proc. 1998 IEEE ISIC/CIRA/ISAS Jt. Conf. 1998, 520–521. [Google Scholar]
- Parasuraman, R. Designing automation for human use: Empirical studies and quantitative models. Ergonomics 2000, 43, 931–951. [Google Scholar] [CrossRef] [PubMed]
- Parasuraman, R.; Riley, V. Humans and automation: Use, misuse, disuse, abuse. Hum. Factors 1997, 39, 230–253. [Google Scholar] [CrossRef]
- Lee, E.A.; Seshia, S.A. Introduction to Embedded Systems Embedded Systems—A Cyber-Physical Systems Approach; Lulu.com: Morrisville, NC, USA, 2013; ISBN 9780557708574. [Google Scholar]
- Goyal, M. Behavioral Validation in Cyber-Physical Systems: Safety Violations And Beyond. Ph.D. Thesis, University of North Carolina at Chapel Hill Graduate School, Chapel Hill, NC, USA, 2022. [Google Scholar] [CrossRef]
- Ali, N.; Hussain, M.; Hong, J.E. SafeSoCPS: A Composite Safety Analysis Approach for System of Cyber-Physical Systems. Sensors 2022, 22, 4474. [Google Scholar] [CrossRef]
- Furrer, F.J. Cyber-Physical Systems. In Safety and Security of Cyber-Physical Systems; Springer: Wiesbaden, Germany, 2022; pp. 9–76. [Google Scholar]
- Petrovic, D.; Mijailović, R.; Pešić, D. Traffic Accidents with Autonomous Vehicles: Type of Collisions, Manoeuvres and Errors of Conventional Vehicles’ Drivers. Transp. Res. Procedia 2020, 45, 161–168. [Google Scholar] [CrossRef]
- Dixit, V.V.; Chand, S.; Nair, D.J. Autonomous vehicles: Disengagements, accidents and reaction times. PLoS ONE 2016, 11, e0168054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favarò, F.; Eurich, S.; Nader, N. Autonomous vehicles’ disengagements: Trends, triggers, and regulatory limitations. Accid. Anal. Prev. 2018, 110, 136–148. [Google Scholar] [CrossRef]
- Insaurralde, C.C. Intelligent autonomy for aerospace engineering systems: Technologies from different application domains to the aviation sector. In Proceedings of the 2018 IEEE/AIAA 37th Digital Avionics Systems Conference (DASC), London, UK, 23–27 September 2018. [Google Scholar] [CrossRef]
- Gil, M.; Albert, M.; Fons, J.; Pelechano, V. Engineering human-in-the-loop interactions in cyber-physical systems. Inf. Softw. Technol. 2020, 126, 106349. [Google Scholar] [CrossRef]
- Jirgl, M.; Bradac, Z.; Fiedler, P. Human-in-the-Loop Issue in Context of the Cyber-Physical Systems. IFAC-PapersOnLine 2018, 51, 225–230. [Google Scholar] [CrossRef]
- Feng, L.; Wiltsche, C.; Humphrey, L.; Topcu, U. Synthesis of Human-in-the-Loop Control Protocols for Autonomous Systems. IEEE Trans. Autom. Sci. Eng. 2016, 13, 450–462. [Google Scholar] [CrossRef]
- Sousa Nunes, D.S.; Zhang, P.; Sa Silva, J. A Survey on human-in-The-loop applications towards an internet of all. IEEE Commun. Surv. Tutor. 2015, 17, 944–965. [Google Scholar] [CrossRef]
- Emmanouilidis, C.; Pistofidis, P.; Bertoncelj, L.; Katsouros, V.; Fournaris, A.; Koulamas, C.; Ruiz-Carcel, C. Enabling the human in the loop: Linked data and knowledge in industrial cyber-physical systems. Annu. Rev. Control 2019, 47, 249–265. [Google Scholar] [CrossRef]
- Romero, D.; Stahre, J.; Wuest, T.; Noran, O.; Bernus, P.; Fast-Berglund, Å.; Gorecky, D. Towards an operator 4.0 typology: A human-centric perspective on the fourth industrial revolution technologies. In Proceedings of the International Conference on Computers and Industrial Engineering (CIE46), Tianjin, China, 29–31 October 2016; pp. 1–11. [Google Scholar]
- Tranfield, D.; Denyer, D.; Smart, P. Towards a Methodology for Developing Evidence-Informed Management Knowledge by Means of Systematic Review. Br. J. Manag. 2003, 14, 207–222. [Google Scholar] [CrossRef]
- Roberts, J.T. Accountability in Athenian Government; University of Wisconsin Press: Madison, WI, USA, 1982. [Google Scholar]
- Zzamel, M.A.E. Accounting, Control and Accountability: Preliminary Evidence from Ancient Egypt. Crit. Perspect. Account. 1997, 8, 563–601. [Google Scholar] [CrossRef]
- Bovens, M.; Goodin, R.E.; Schillemans, T. The Oxford Handbook of Public Accountability, 1st ed.; Oxford Handbooks in Politics & International Relations; Oxford University Press: Oxford, UK, 2014; ISBN 9780199641253. [Google Scholar]
- Sinclair, A. The chameleon of accountability: Forms and discourses. Account. Organ. Soc. 1995, 20, 219–237. [Google Scholar] [CrossRef]
- Mulgan, R. “Accountability”: An Ever-Expanding Concept? Public Adm. 2000, 78, 555–573. [Google Scholar] [CrossRef]
- Roberts, J. The possibilities of Accountability. Account. Organ. Soc. 1991, 16, 355–368. [Google Scholar] [CrossRef]
- Romzek, B.S.; Ingraham, P.W. Cross Pressures of Accountability: Initiative, Command, and Failure in the Ron Brown Plane Crash. Public Adm. Rev. 2000, 60, 240–253. [Google Scholar] [CrossRef]
- Lindkvist, L.; Llewellyn, S. Accountability, responsibility and organization. Scand. J. Manag. 2003, 19, 251–273. [Google Scholar] [CrossRef]
- Shearer, T. Ethics and accountability: From the for-itself to the for-the-other. Account. Organ. Soc. 2002, 27, 541–573. [Google Scholar] [CrossRef]
- Thomas, A. Styles of Accountability. Account. Organ. Soc. 1996, 21, 139–173. [Google Scholar]
- Messner, M. The limits of accountability. Account. Organ. Soc. 2009, 34, 918–938. [Google Scholar] [CrossRef]
- Hall, A.T.; Bowen, M.G.; Ferris, G.R.; Royle, M.T.; Fitzgibbons, D.E. The accountability lens: A new way to view management issues. Bus. Horiz. 2007, 50, 405–413. [Google Scholar] [CrossRef]
- Koppell, J. Pathologies of Accountability: ICANN and the Challenge of “Multiple Accountabilities Disorder”. Public Adm. Rev. 2005, 65, 94–108. [Google Scholar] [CrossRef]
- Wettenhall, R.L. Quangos, Quagos And The Problems Of Non-Ministerial Organisation. Aust. J. Public Adm. 1983, 42, 5–52. [Google Scholar] [CrossRef]
- Behn, R. Rethinking Democratic Accountability; Brookings Institution Press: Washington, DC, USA, 2001. [Google Scholar]
- Ebrahim, A. Accountability In Practice: Mechanisms for NGOs. World Dev. 2003, 31, 813–829. [Google Scholar] [CrossRef]
- Bovens, M.; Hix, S. Analysing and assessing public accountability: A conceptual framework. Eur. Gov. Pap. 2006, 1–37. [Google Scholar]
- Flight Safety Foundation—Flight Safety Digest. Available online: https://aviation-safety.net/database/record.php?id=19960403-0 (accessed on 1 September 2022).
- Fuse, J. Managing Accountability for Service Through-Life; University of Cambridge: Cambridge, UK, 2013. [Google Scholar]
- Fielder, P.; Roper, A.; Walby, B.; Fuse, J.; Neely, A.; Pearson, C. Product Safety in a World of Services: Through-Life Accountability; Cambridge Service Alliance Newsletter Volume February; Cambridge Service Alliance, University of Cambridge: Cambridge, UK, 2014. [Google Scholar]
- Davidson, I. UK Parliament. Available online: https://publications.parliament.uk/pa/cm199798/cmhansrd/vo981020/debtext/81020-14.htm (accessed on 17 November 2014).
- Grose, G. The Future Of Through-Life Accountability In Commercial Aviation & Defense… No Matter The Buzzword. Available online: https://blog.ifsworld.com/2017/05/the-future-of-through-life-accountability-in-commercial-aviation-defense-no-matter-the-buzzword/ (accessed on 22 May 2017).
- Roberts, J. No one is perfect: The limits of transparency and an ethic for ‘intelligent’ accountability. Account. Organ. Soc. 2009, 34, 957–970. [Google Scholar] [CrossRef]
- O’Neill, O. A Question of Trust: The Bbc Reith Lectures 2002; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Hollnagel, E.; Leonhardt, J.; Licu, T.; Shorrock, S. From Safety-I to Safety-II: A white paper. Bruss. Eur. Organ. Saf. Air Navig. 2013. [Google Scholar]
- Amundrud, Ø.; Aven, T.; Flage, R. How the definition of security risk can be made compatible with safety definitions. Proc. Inst. Mech. Eng. Part O J. Risk Reliab. 2017, 231, 286–294. [Google Scholar] [CrossRef] [Green Version]
- Oxford Living Dictionaries. Available online: https://en.oxforddictionaries.com (accessed on 28 March 2017).
- Business Dictionary. Available online: http://www.businessdictionary.com (accessed on 17 November 2017).
- ICAO. Safety Management Manual (SMM); International Civil Aviation Organization: Montreal, QC, Canada, 2013. [Google Scholar]
- IAEA. Terminology Used in Nuclear Safety and Radiation Protection; International Atomic Energy Agency: Vienna, Austria, 2007. [Google Scholar]
- Cox, S.; Cox, T. The structure of employee attitudes to safety: A european example. Work Stress 1991, 5, 93–106. [Google Scholar] [CrossRef]
- Baksteen, B. Flying is not safe. Saf. Sci. 1995, 19, 287–294. [Google Scholar] [CrossRef]
- Lanzisero, T. Applied Safety Science and Engineering Techniques (ASSET): Taking Hazard Based Safety Engineering (HBSE) to the Next Level. IEEE Consum. Electron. Mag. 2014, 3, 36–46. [Google Scholar] [CrossRef]
- International Civil Aviation Organization. Model Aircraft Accident and Incident Investigation (AIG) Act; International Civil Aviation Organization: Montreal, QC, Canada, 2013. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.; Lewis, P.; Thornhill, A. Research Methods for Business Students, 5th ed.; Prentice Hall: Essex, UK, 2009. [Google Scholar]
- Welsh, E. Dealing with Data: Using NVivo in the Qualitative Data Analysis Process. Forum Qual. Sozialforsch. Forum Qual. Soc. Res. 2002, 3. [Google Scholar]
- Makri, C.; Neely, A. Grounded Theory: A Guide for Exploratory Studies in Management Research. Int. J. Qual. Methods 2021, 20, 1–14. [Google Scholar] [CrossRef]
- Saldaña, J. The Coding Manual for Qualitative Researchers; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2015; ISBN 9781473902497. [Google Scholar]
- List of Accidents and Incidents Involving Commercial Aircraft. Available online: https://en.wikipedia.org/wiki/List_of_accidents_and_incidents_involving_commercial_aircraft#2006 (accessed on 1 March 2022).
- Bartlett, A. Aviation Safety Magazine. Available online: https://www.aviationsafetymagazine.com/features/situational-awareness/ (accessed on 2 September 2022).
- Hackitt, J. Health and Safety: The Journey Back to Common Sense and Personal Responsibility. Royal Academy of Engineering. Available online: https://www.youtube.com/watch?v=J4xQnulGYdg&feature=youtu.be (accessed on 25 May 2016).
- Senders, J.; Moray, N. Human Error: Cause, Prediction, and Reduction; Taylor & Francis: Boca Raton, FL, USA, 1991. [Google Scholar]
- Sullivan, J.; Beach, R. Improving project outcomes through operational reliability: A conceptual model. Int. J. Proj. Manag. 2009, 27, 765–775. [Google Scholar] [CrossRef]
- Downer, J. On audits and airplanes: Redundancy and reliability-assessment in high technologies. Account. Organ. Soc. 2011, 36, 269–283. [Google Scholar] [CrossRef]
- Stultz, J. High Reliability Organization Toolkit. MHA. Available online: https://web.mhanet.com/media-library/high-reliability-organization-toolkit/ (accessed on 1 September 2022).
- Saleh, J.H.; Marais, K.B.; Bakolas, E.; Cowlagi, R.V. Highlights from the literature on accident causation and system safety: Review of major ideas, recent contributions, and challenges. Reliab. Eng. Syst. Saf. 2010, 95, 1105–1116. [Google Scholar] [CrossRef]
- Hall, J.L. Columbia and Challenger: Organizational failure at NASA. Space Policy 2003, 19, 239–247. [Google Scholar] [CrossRef]
- Rochlin, G.I.; La Porte, T.R.; Roberts, K.; LaPorte, T.R. The Self-Designing High-Reliability Organization: Aircraft Carrier Flight Operations at Sea. Nav. War Coll. Rev. 2005, 75–90. [Google Scholar]
- Weick, K.E.; Sutcliffe, K.M. Managing the Unexpected: Resilient Performance in an Age of Uncertainty, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2007. [Google Scholar]
- Roberts, K.; Rousseau, D.M.; La Porte, T.R. The culture of high reliability: Quantitative and qualitative assessment aboard nuclear-powered aircraft carriers. J. High Technol. Manag. Res. 1994, 5, 141–161. [Google Scholar] [CrossRef]
- Pidgeon, N.; O’Leary, M. Man-made disasters: Why technology and organizations (sometimes) fail. Saf. Sci. 2000, 34, 15–30. [Google Scholar] [CrossRef]
- Roberts, K.; Bea, R.; Bartles, D. Must accidents happen? Lessons from high-reliability organizations. Acad. Manag. Exec. 2001, 15, 70–78. [Google Scholar] [CrossRef]
- Tranfield, D.; Denyer, D.; Marcos, J. Management and Development of High Reliability Organisations; Cranfield School of Management: Cranfield, UK, 2003. [Google Scholar]
- Hopkins, A. The Problem of Defining High Reliability Organisations; WP51: Canberra, Australia, 2007. [Google Scholar]
- Lekka, C.; Sugden, C. The successes and challenges of implementing high reliability principles: A case study of a UK oil refinery. Process. Saf. Environ. Prot. 2011, 89, 443–451. [Google Scholar] [CrossRef]
- Sutcliffe, K.M. High reliability organizations (HROs). Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 133–144. [Google Scholar] [CrossRef]
- Sutcliffe, K.M.; Christianson, M.K. Managing the Unexpected: Executive White Paper Series; Michigan Ross School of Business: Ann Arbor, MI, USA, 2013. [Google Scholar]
- Makri, C.; Neely, A. Through-life accountability: Managing complex services. In Proceedings of the EurOMA Conference, Neuchâtel, Switzerland, 26 June–1 July 2015; pp. 1–10. [Google Scholar]

| Continent | Fatalities | % of Fatalities | Number of Accidents | % of Accidents |
|---|---|---|---|---|
| Asia | 3034 | 38.09% | 91 | 32.85% |
| Africa | 1623 | 20.38% | 45 | 16.25% |
| America | 1170 | 14.69% | 69 | 24.91% |
| Europe | 1073 | 13.47% | 30 | 10.83% |
| Eurasia | 901 | 11.31% | 31 | 11.19% |
| Mediterranean Sea | 90 | 1.13% | 1 | 0.36% |
| Oceania | 74 | 0.93% | 10 | 3.61% |
| Australia | 0 | 0.00% | 0 | 0.00% |
| Antarctica | 0 | 0.00% | 0 | 0.00% |
| Country | Continent | Number of Accidents | Fatalities |
|---|---|---|---|
| US | America | 28 | 122 |
| Russia | Eurasia | 24 | 807 |
| Indonesia | Asia | 18 | 658 |
| Nepal | Asia | 13 | 212 |
| Democratic Republic of Congo | Africa | 13 | 333 |
| Iran | Asia | 12 | 598 |
| Pakistan | Asia | 7 | 501 |
| Brazil | America | 6 | 566 |
| Canada | America | 6 | 16 |
| Turkey | Eurasia | 5 | 60 |
| Airline | Country | Number of Accidents |
|---|---|---|
| Southwest Airlines | US | 6 |
| Merpati Nusantara Airlines | Indonesia | 4 |
| Turkish Airlines | Turkey | 4 |
| Asiana Airlines | South Korea | 3 |
| EgyptAir | Egypt | 3 |
| Ethiopian Airlines | Ethiopia | 3 |
| FedEx Express | US | 3 |
| Iran Air | Iran | 3 |
| Pakistan International Airlines | Pakistan | 3 |
| Qantas | Australia | 3 |
| Contributing Factors | Number of Accidents | Number of References in Accident Reports |
|---|---|---|
| Non-adherence to SOPs 1 | 20 | 150 |
| Operational | 16 | 92 |
| Behaviours/Skills | 8 | 23 |
| Certifications | 6 | 8 |
| Maintenance/Service/Performance | 4 | 13 |
| Incident Reporting | 4 | 10 |
| General | 3 | 4 |
| Poor Handling | 20 | 139 |
| CRM | 15 | 52 |
| Emotional/Behavioural Issues | 12 | 30 |
| Equipment-Plane | 10 | 21 |
| Decision Making | 9 | 18 |
| Operational | 9 | 18 |
| Failure to identify safety issues | 19 | 119 |
| Lack of SOP | 17 | 58 |
| Lack of proper training | 15 | 42 |
| Lack of proper equipment | 12 | 28 |
| Lack of proper communication | 10 | 33 |
| Mechanical issue | 9 | 32 |
| Lack of safety culture | 9 | 28 |
| Poor weather conditions | 9 | 11 |
| Loss of situational awareness | 6 | 15 |
| Lack of proper maintenance | 5 | 22 |
| Lack of required personnel | 5 | 6 |
| Hierarchy issues | 4 | 7 |
| Design issue(s) | 3 | 11 |
| Actors | Number of Accidents | Number of References in Accident Reports |
|---|---|---|
| Flight Crew | 21 | 198 |
| Airline | 18 | 137 |
| Supervisory Authority | 15 | 67 |
| Air Traffic Control (ATC) | 12 | 40 |
| Aircraft Manufacturer | 8 | 43 |
| Airport | 5 | 22 |
| Maintenance Team | 3 | 23 |
| Emergency Services | 3 | 13 |
| Passengers | 2 | 3 |
| Airport Crew | 2 | 4 |
| Flight Crew (previous flight) | 1 | 3 |
| Multiple Actors | 1 | 2 |
| Accident Code | Actors | Contributing Factors |
|---|---|---|
| N109 | 8 | 13 |
| N72 | 8 | 13 |
| N59 | 7 | 8 |
| N87 | 6 | 12 |
| N61 | 5 | 13 |
| N75 | 5 | 9 |
| N104 | 4 | 14 |
| N107 | 4 | 9 |
| N123 | 4 | 8 |
| N128 | 4 | 10 |
| N79 | 4 | 7 |
| N112 | 3 | 7 |
| N133 | 3 | 13 |
| N66 | 3 | 5 |
| N78 | 3 | 10 |
| N82 | 3 | 12 |
| N91 | 3 | 11 |
| N97 | 3 | 12 |
| N64 | 2 | 10 |
| N116 | 2 | 4 |
| N122 | 2 | 2 |
| N86 | 2 | 6 |
| N118 | 1 | 4 |
| N119 | 1 | 3 |
| N98 | 1 | 2 |
| N88 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makri, C.; Gürdür Broo, D.; Neely, A. Human-in-Loop Decision-Making and Autonomy: Lessons Learnt from the Aviation Industry Transferred to Cyber-Physical Systems. Technologies 2022, 10, 120. https://doi.org/10.3390/technologies10060120
Makri C, Gürdür Broo D, Neely A. Human-in-Loop Decision-Making and Autonomy: Lessons Learnt from the Aviation Industry Transferred to Cyber-Physical Systems. Technologies. 2022; 10(6):120. https://doi.org/10.3390/technologies10060120
Chicago/Turabian StyleMakri, Chara, Didem Gürdür Broo, and Andy Neely. 2022. "Human-in-Loop Decision-Making and Autonomy: Lessons Learnt from the Aviation Industry Transferred to Cyber-Physical Systems" Technologies 10, no. 6: 120. https://doi.org/10.3390/technologies10060120