

Uncovering the Hidden Burden of Pharmaceutical Poisoning in High-Income and Low-Middle-Income Countries: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
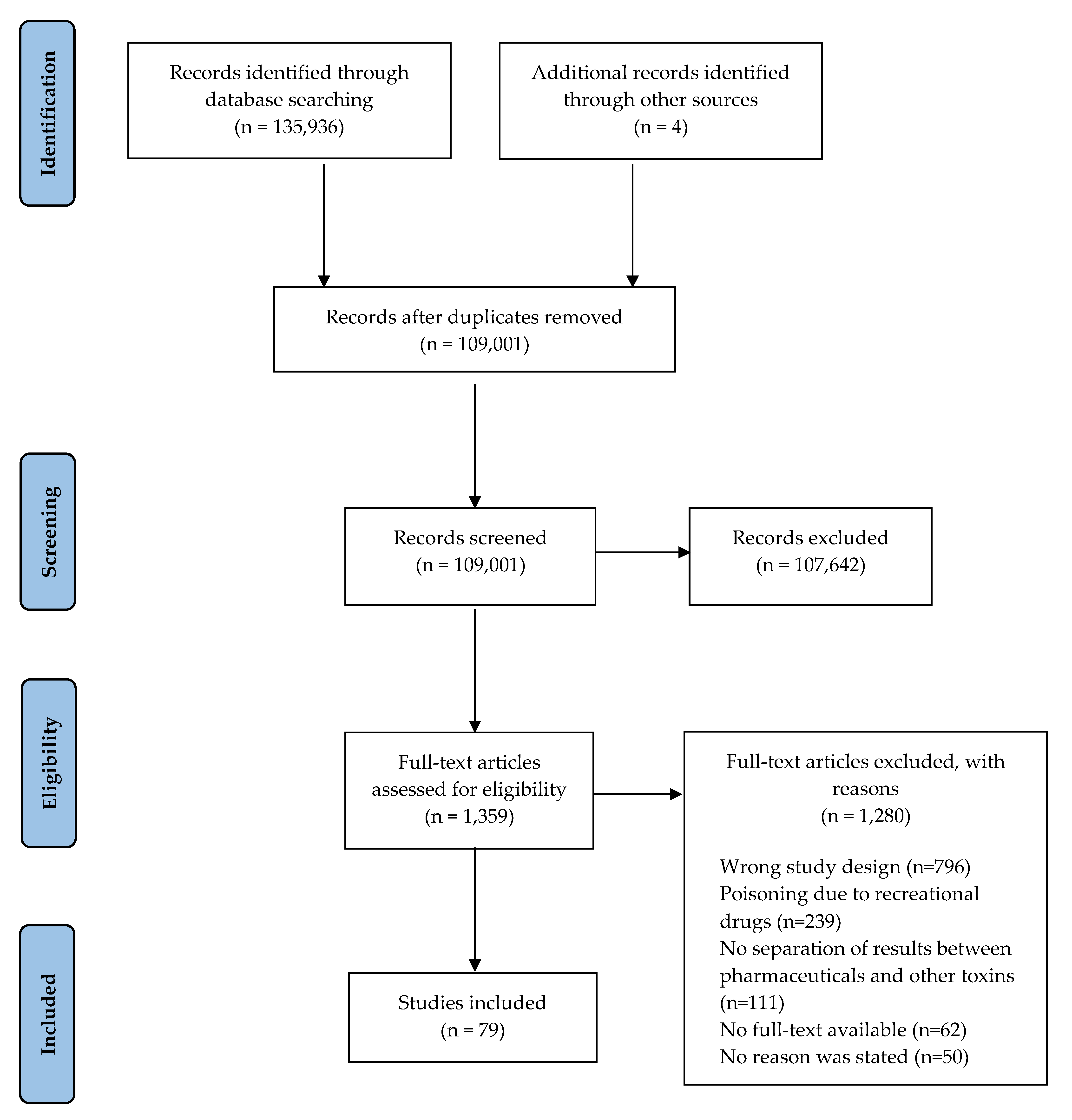
2.2. Study Selection
2.3. Data Extraction and Synthesis
3. Results
3.1. Characteristics of Included Studies
3.2. Overview
3.3. Trends
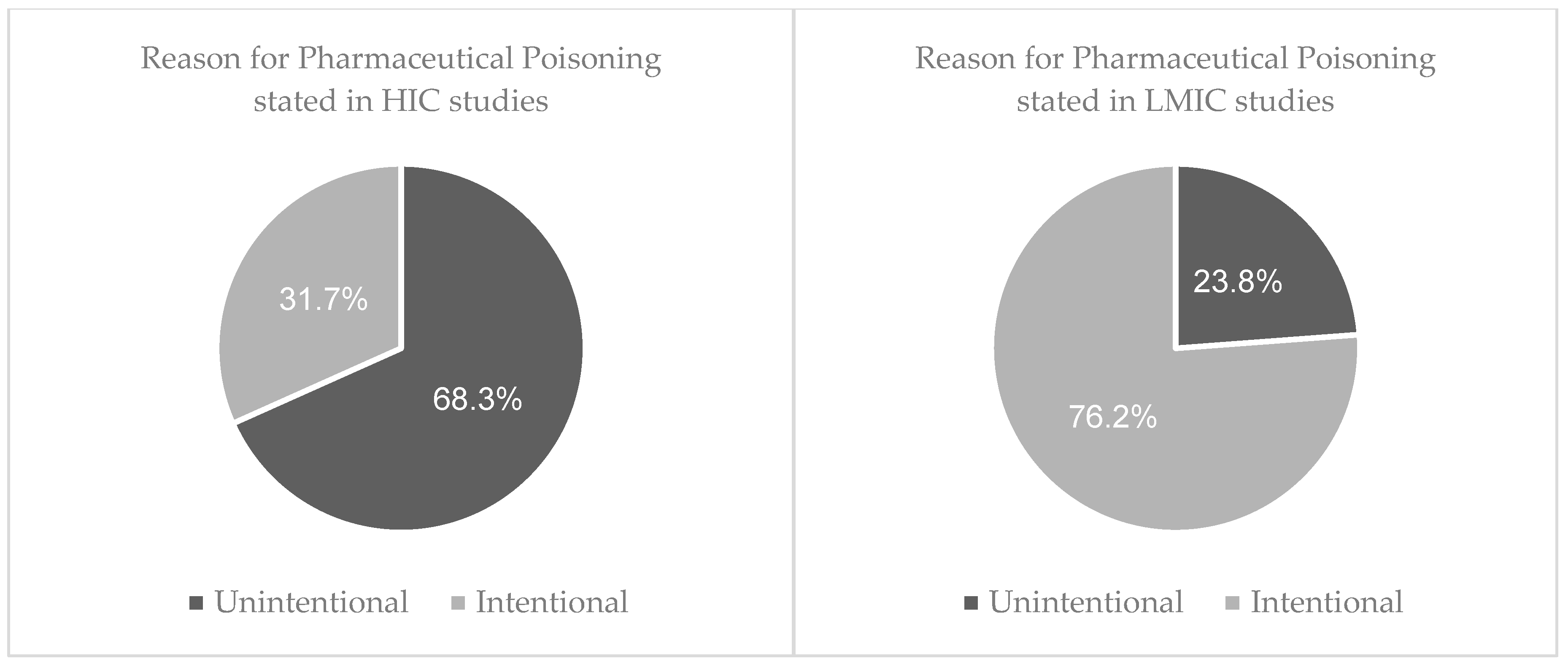
3.3.1. Reason behind Toxic Exposure
3.3.2. Types of Pharmaceuticals Responsible for Poisoning
3.3.3. Outcome of Pharmaceutical Poisoning
4. Discussion
4.1. Reason behind Toxic Exposure
4.2. Types of Pharmaceuticals Responsible for Poisoning
4.3. The Outcome of Pharmaceutical Poisoning
4.4. Future Research and Recommendations
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADR | Adverse drug reaction |
| AKI | Acute kidney injury |
| ATC | Anatomic Therapeutic Chemical |
| BB | Beta blocker |
| CCB | Calcium channel blocker |
| CVS | Cardiovascular |
| CNS | Central nervous system |
| DDD | Defined Daily Dose |
| ED | Emergency departments |
| ENT | Ear, nose, and throat |
| GI | Gastrointestinal |
| HICs | High-income countries |
| ICU | Intensive care unit |
| LMICs | Low-middle-income countries |
| MI | Myocardial infarction |
| MALA | Metformin associated lactic acidosis |
| NSAID | Non-steroidal anti-inflammatory |
| OTC | Over the counter |
| POU | Pyrexia of unknown origin |
| PSS | Poisoning Severity Score |
| SSRI | Selective serotonin reuptake inhibitor |
| TCA | Tricyclic antidepressant |
| TB | Tuberculosis |
| UK | United Kingdom |
| USA | United States of America |
Appendix A. Search Strategy
| 1. | Poison*.mp. |
| 2. | toxic.mp. |
| 3. | overdose.mp or intoxication/ |
| 4. | excessive.mp. |
| 5. | substance abuse/ |
| 6. | drug misuse/ |
| 7. | 1 or 2 or 3 or 4 or 5 or 6 |
| 8. | pharmaceutical.mp. |
| 9. | medicine/ |
| 10. | drug/ |
| 11. | opioid.mp. |
| 12. | 8 or 9 or 10 or 11 |
| 13. | 7 and 12 |
| 14. | limit 13 to (English and yr = 2011–2020) |
Appendix B

{kind=link}
{kind=link}
| Author (Year) | Study Design | Setting | Sample Size | Patient Demographics (Age (Years) * and Gender a) | Reason for Exposure | Drug Responsible for Poisoning b | Outcome from Exposure c |
|---|---|---|---|---|---|---|---|
| Ghaemia et al. [42] | A prospective cross-sectional study at a tertiary toxicology centre in Northeast Iran | Northeast Iran | 126 | Ages 1–14: 126 Mean age: 2.8
| Accidental: 126
|
| Symptoms:
Hospitalised 126Deaths: 3 |
| Hamedi et al. [49] | Cross-sectional study on children admitted to EDb of Imam Reza Hospital. Data was collected from laboratory results and subjective data from parents’ responses. | Northeast Iran | 79 | (3 months–15 years)
| Accidental: 74
Intentional (suicide attempt): 1Unknown: 4 |
| Hospitalised: 79
Deaths: 2 (due to prolonged hypoxia and delay in hospitalisation) |
| Jabbehdari et al. [43] | Descriptive-sectional study on hospital admissions with methadone poisoning at Loghman-Hakim Hospital in the second half of 2012. | Iran | 31 | Mean age: 4.6
| Accidental: 31 |
| Hospitalised: 31
|
| Bilel et al. [38] | A retrospective descriptive study on poisonings received at the Oran University Hospital over 8 years using a pre-established information sheet on patient and circumstances of poisoning along with biological samples. | Algeria | 400 |
| Accidental: 72 Intentional (suicide attempts): 328 |
| Hospitalised: 400
Death: 5 |
| Kara et al. [124] | Retrospective study comprised records of patients admitted to ED of Konya Numune Hospital between 2009–2011. | Turkey | 932 |
| Intentional (suicide attempts): 932 |
| Hospitalised: 932
Death: 1 |
| Buffone et al. [39] | Descriptive, retrospective study based on the data collected from reviewing the medical records of patients 10–19 years at ED of Municipal Hospital of Bahia Blanca. | Argentina | 72 | Mean age: 16 (10–19)
| Intentional: 72
|
| Hospitalised: 72
|
| Hocaoglu et al. [54] | Cross-sectional descriptive study reviewing theophylline exposure cases reported to Dokuz Eylul University Drug and Poison Information Centre (DPIC). | Turkey | 354 |
| Intentional: 291 Accidental: 46 Unknown: 17 |
| Hospitalised: 354
Death: 2 |
| Mehrpour et al. [44] | Retrospective cross-sectional review based on hospital records of acute poisonings managed in ICU during a 7-year period in a single center in Birjand, Iran | Iran | 267 |
| Accidental: 22 Intentional: 151
|
| ICU: 267 Death: 52 |
| Azekour et al. [51] | Epidemiological retrospective study reviewing medicinal poisoning registered with the Provincial Delegation of Health in Errachidia between 2004–2016 | Morocco | 180 | Mean age: 21 (2–75)
| Accidental: 101 Intentional: 72 Unknown: 7 |
| Hospitalised: 132 Death: 3 |
| Taheri et al. [125] | Descriptive analytical study performed from 2010–2012 in the poisoning emergency and clinical toxicology departments of Noor Hospital affiliated with Isfahan University of Medical Sciences. | Iran | 385 | Mean age: 32.1 (1–90)
| Intentional: 222 Accidental: 153 |
| Hospitalised: 385
Death: 7 |
| Weerasinghe et al. [53] | Retrospective analysis of self-harm cases. Data collected from primary and referral hospitals. | Sri Lanka | 54 |
| Intentional: 52 Accidental: 2 |
| Hospitalised: 54
|
| Bagherian Rad et al. [45] | Cross sectional retrospective study carried out on all patients referred to Loghman Hakim Hospital from 2011–2016. | Iran | 229 | Mean age: 24 (13–90)
| Intentional: 224 Unintentional: 5 |
| Hospitalised: 229 ICU: 8 Duration of hospital stay:
Death: 1 |
| Nagaralu et al. [40] | Retrospective review using data from ED at four tertiary care hospitals | India | 708 |
| Intentional: 484 Accidentall: 149 Homicidal: 20 Unknown: 55 |
| Hospitalised: 708 Death: 42 |
| Anthony et al. [41] | Observational retrospective review using records from a tertiary care hospital over 15 months | India | 91 | Mean age: 28.1
| Intentional: 72 Accidental: 19 |
| ICU: 61
Deaths: 3 |
| Shadnia et al. [46] | Retrospective cohort study using data from patients admitted to Loghman Hakim Hospital Poison Centre over 4-month period. | Iran | 100 |
| Intentional (suicide attempt): 93 Unknown: 7 |
| Hospitalised: 100
|
| Yehya et al. [50] | Retrospective descriptive study using data from PharmacyOne Poison call centre, 2014–2018 | Jordan | 900 |
| Intentional: 236
|
| PSS
|
| Van hoving et al. [11] | Retrospective review extracting data from Khayelitsha Hospital Emergency Care database | South Africa | 192 |
| Intentional: 192 |
| Hospitalised: 192
Death: 4 |
| Hashemneiad et al. [47] | Cross sectional study using data from patients admitted with drug poisoning at Karaj Shariati Hospital over 1 year | Iran | 172 | Mean age 29.8 (12–80)
| Intentional: 172 |
| Hospitalised: 172
Death: 10 |
| Yaylaci et al. [55] | Retrospective study of patients at follow-up admitted with intoxication to the ICU between 2009–2011 | Turkey | 153 |
| Intentional (suicide attempt): 144 Accidental: 9 |
| ICU: 153 Average length of stay: 2.4 days |
| Khodabandeh et al. [48] | Prospective cross-sectional study among acute drug poisoning patients at a single hospital over 1 year | Iran | 410 |
| Accidental: 35 Intentional: 375
|
| Hospitalised: 410
|
| Sorodoc et al. [52] | Retrospective review using data from a single tertiary center from Iasi County, Romania | Romania | 811 |
| Accidental: 63 Intentional (Suicide attempt): 748 |
| Hospitalised: 811
Death: 2 |
| Author (Year) | Study Design | Setting a | Sample Size | Patient Demographics (Age (Years) * and Gender b) | Reason for Exposure | Drug Responsible for Poisoning c | Outcome from Exposure d |
|---|---|---|---|---|---|---|---|
| Jensen et al. [62] | A retrospective nationwide descriptive study using 2 databases; the Danish Poison and Information Centre (DPIC) and the State Serum Institute of Denmark. (SSI) | Denmark | 1505 |
| Intentional: 1142
Unknown: 71 |
| Hospitalised: 456
Deaths: 14 |
| Martin et al. [86] | Retrospective review of all paediatric admission at Eastern Maine Medical Centre (EMMC) from 1999–2009. | USA | 22 |
| Accidental: 16 (All aged between 1–12) Intentional: 6 (All aged between 13–17) Drug source was family or friend for 82% of cases |
| Hospitalisation: 22
|
| Gregoriano et al. [94] | Retrospective analysis of reports to a National Poison Centre 1995–2013 | Switzerland | 40 |
| Children:
| Children:
| Hospitalised: 40
|
| Martos et al. [78] | An observational study reported to national poison centre between 1995–2013 | Switzerland | 75 |
| Accidental: 22
Intentional: 50
|
| No effect:
|
| Cairns et al. [56] | Retrospective observational study. Data collected from NSW poisons information centre 2004–2014 | Australia | 1735 | Mean age: 17
| Intentional: 1735 |
| Hospitalised: 1594 Referred to toxicologist: 60 |
| Alruwaili et al. [81] | Prospective, descriptive cross-sectional study looking at 2 paediatric ED in Riyadh over 2 years | Saudi Arabia | 1035 |
| Unintentional: 906 Intentional: 22 Unknown: 104 |
| Hospitalised: 1035
|
| Eluri et al. [87] | Retrospective analysis of errors reported to USA poison control centre from 2000–2012 | USA | 533,763 |
| Accidental:
|
|
|
| Ichikura et al. [72] | Cohort study from an ICU in Japan from 2006–2013 | Japan | 676 |
| Intentional: 676
|
| ICU: 676 |
| Post et al. [88] | Retrospective analysis of calls to USA poison control centres (NPDS) from 2007–2016 | USA | 11,275 |
| Accidental: 10,053 Intentional: 1001 |
| Hospitalised: 8401 Deaths: 11 |
| Kamour et al. [85] | Retrospective study using NPIS telephone enquires related to 4 NSAIDs between 2007–2013 | UK | 22,937 | (14–98)
| Intentional: 11,104 Drug misuse: 65 Accidental: 9826 Unknown: 602 |
|
|
| Tan et al. [83] | Retrospective review of paracetamol overdose presenting to a tertiary hospital in Singapore | Singapore | 177 | Mean age: 25 (21–36)
| Intentional: 136 Unintentional: 40 Intent unclear: 1 |
| Hospitalised: 177
|
| Madadi et al. [58] | Retrospective study using the Office of the Chief Coroner of Ontario. All deaths coded drug-related were reviewed. | Canada | 1359 | Mean age: 44 Age range: 16–89
| Accident: 924 Unknown: 221 Suicide: 214 |
| Death: 1359 |
| Austin et al. [89] | Population based study using North Carolina death certificate data to identify drug overdose decedents | USA | 1221 |
| Intentional: 207 Accidental: 1014 |
| Death: 1221 |
| Friedrich et al. [90] | Retrospective database analysis of NPDS from 2000–2015 | USA | 296,838 |
Gender not stated | Intentional: 142,482 Accidental: 154,356 |
| Death: 253
|
| Torrents et al. [67] | A 6-year prospective national study. Patients identified using records reported to poison centre and contacted to complete survey | France | 87 | Mean age 2 (0.5–17 years)
| Accidental: 87 |
| Emergency unit: 42 Paediatric unit: 21 ICU: 13 Death: 5 |
| Toce et al. [91] | Retrospective cohort study at a single paediatric tertiary care centre of children between 6 months and 7 years between 2006–2014 | USA | 88 | Mean age: 2 (10 months–6.4 years)
| Accidental: 88 |
| Hospitalised: 88
|
| Gomes et al. [59] | Population-based cross-sectional study of patients admitted for acute care in hospitals across Canada due to prescribed opioids | Canada | 2599 |
| Accidental: 648 Intentional: 291 Unknown: 248 |
| Hospitalised: 2599 |
| Shipton et al. [74] | Population based cohort study using records from the Coronial Services Office in Wellington from 2008–2012 | New Zealand | 325 |
| Unintentional: 179 Intentional: 110 Unknown: 37 |
| Death: 325 |
| Tadros et al. [92] | Retrospective study using data from the Nationwide ED Sample (NEDS) from 2006–2012 | USA | 21,928 | Mean age: 9 (0–17)
| Intentional: 5316 Accidental: 13,524 Unknown: 2126 |
| All ED visits
Deaths: 11 |
| Tadros et al. [93] | Retrospective cohort study utilising 2006–2011 data from the Nationwide ED Sample | USA | 259,093 |
| Unintentional: 138,603 Intentional: 68,641 Unknown: 51,849 |
| All ED visits
|
| Vakkalanka et al. [99] | Retrospective review of loperamide exposures reported to NPDS between 2010 and 2015. | USA | 1736 |
| Abuse: 228 Misuse: 569 Attempted suicide: 848 Other: 91 |
| PSS
|
| Creswell et al. [126] | Cross sectional study. Data of children aged 0–19 exposed to opioids was collected using hospital admissions and Wisconsin Poison Control Centre (WPC) | USA | 3320 |
| Accidental: 2522
|
| ICU: 3320 Death: 3 |
| Feingold et al. [70] | Retrospective study. Data was obtained from the National database on causes of death. Drug poisoning deaths were coded as opioid-related | Israel | 875 |
| Accidental: 9 Intentional: 4 Unknown: 409 |
|
|
| Koskela et al. [65] | Retrospective study. Data was collected from Cause of Death Registry death certificates provided by Statistics Finland from 2007–2011. | Northern Finland | 684 | Urban:
Rural:
| Urban: Intentional (suicide attempt): 82 Rural: Intentional (suicide attempt): 40 | Urban:
| Death: 684 |
| Tobaiqy et al. [82] | Retrospective study. Chart review of all acute paediatric poisoning incidence in ED at East Jeddah Hospital over 4-year period | Saudi Arabia | 69 |
| Accidental: 46
|
| Hospitalised: 69
Death: 1 |
| Kriikku et al. [66] | Retrospective review of post-mortem toxicology cases positive for urinary buprenorphine between 2010–2014 | Finland | 775 | Mean age: 31
| Accidental: 463 Intentional parenteral instead of sublingual: 167 suicide: 90 other: 55 |
| Death: 369 |
| Thongprayoon et al. [127] | Retrospective review. Data extracted from the National Inpatient Sample (NIS) coded as ICD-9 diagnosis. | USA | 13,805 |
| Intentional (suicide attempt): 9029 Unknown: 4776 |
| Hospitalised: 13,805
Death: 132 |
| Miller et al. [102] | Prospective cross-sectional study. Analysis of censuses of live emergency department and inpatient discharges for 11 USA states as well as Multiple Cause of Death census data between 2011–2012 | USA | 10,525 |
| Intentional (suicide attempt): 6716 Unknown: 3809 |
| Death: 10,525 |
| Manini et al. [128] | Prospective cohort study looking at two tertiary care hospitals over 12 months. | USA | 274 | Mean age: 40.3
| Intentional: 217 Accidental: 57 |
| Hospitalised: 274
Death: 2 |
| Lee et al. [57] | Retrospective review using data from calls to Victorian Poisons Information Centre (VPIC) over a 10-year period. | Australia | 4412 |
| Accidental: 781
|
co-ingested with:
| Hospitalised: 4412 Death: 1066 |
| Vilay et al. [129] | Retrospective case-control study of exposures reported to the NPDS between 2001–2007 | USA | 9074 |
| Intentional: 5009 Accidental: 3152 |
|
|
| Wheatley et al. [130] | Retrospective review of poison centre records between 2001–2010 | USA | 162 | Mean age: 27
| Intentional: 49 Accidental: 113 |
| ICU: 9 Coma: 1 |
| Kominek et al. [75] | Retrospective analysis of patients hospitalised with paracetamol poisoning in a Paediatric Clinic between 2004–2012 | Poland | 44 |
| Intentional: 30 Accidental: 10 Dosing error: 4 |
| Hospitalised: 44 |
| Haoka et al. [73] | Retrospective observational study analysisng medical records in a single tertiary hospital in Japan | Japan | 145 |
| Accidental: 102 Intentional: 43 |
| Hospital visits: 145
|
| Mroczkowska-Juchkiewicz et al. [76] | Retrospective evaluation of intentional poisoning cases in department of paediatrics, Childrens University Hospital in Lubin from 2007–2012 | Poland | 145 | Mean age: 15.1 (12–15)
| Intentional: 145 reasons including psychiatric disorders, family conflicts, school conflicts, sexual assault, lack of self-acceptance from chronic disease |
| Hospitalisation: 145
|
| Lasoff et al. [98] | Retrospective review using state-wide poison control system electronic database from 2002–2015 | USA | 224 | Mean age: 41 (18–90)
| Intentional.
|
| Hospitalised: 64
Deaths: 3 |
| Feng et al. [131] | Cross-sectional study. Cases were identified from a database by ICD-9-CM diagnosis codes | USA | 9647 |
| Accidental: 2305 ADR: 1663 Suicidal: 930 |
| Death: 53 |
| Lavon et al. [71] | Prospective observational follow-up study of all medication errors outside healthcare facilities reported to IPIC | Israel | 1381 |
| Accidental (therapeutic error): 1381 |
|
|
| Stevens et al. [68] | Retrospective study analysing metformin poisoning reported to Western France PCC from 1999–2016 | France | 382 |
| Accidental: 197 Intentional: 127 Therapeutic error: 58 |
|
Death: 21 |
| Torrents et al. [69] | Retrospective descriptive study of cases of methadone exposure reported to French poison centres over a 7-year-period | France | 1415 | Mean age: 34 (10–74)
| Misuse: 670 Suicide attempt: 584 Unintentional: 12 Medication errors: 140 |
|
Death: 219 |
| Zakharov et al. [61] | Retrospective review using the database of the Czech Toxicological Information Centre from 2007–2011 | Czech Republic | 2339 |
| Intentional (suicide attempt): 2339 |
| Medical care: 2339 |
| Caupp et al. [100] | Retrospective review using Poison Control Centre Data in Ohio from 2002–2014 | USA | 619 |
| Accidental: 97 Intentional: 504 Other/unknown: 37 |
| PSS:
|
| Okic et al. [103] | Retrospective review of descents from forensic pathology in Kansas City autopsied between 2001–2011 | USA | 789 | Mean age: 43 (2–92)
| Accident 332 Intentional (suicide attempt): 43 Unknown: 101 |
| Death: 789 |
| Christenses et al. [63] | Retrospective review looking at enquires concerning CBBs reported to the Danish Poisons Information Centre (DPIC) from 2009–2015 | Denmark | 339 |
| Intentional (suicide attempt): 156 Accidental: 183 | CCB;
| Hospitalised: 275
Death: 7 |
| Truitt et al. [132] | Retrospective chart review of PCC charts by running a search on all calls received between 2007–2009 | USA | 436 |
| Accidental: 436 |
| Hospitalised: 32 Death: 1 |
| Christensen et al. [64] | Retrospective study of drug poisoning cases reported to Danish Poison Information Centre (DPIC) | Denmark | 239 |
| Intentional (suicide attempt): 175 Accidental: 64 | aripiprazole: 239 combined with:
| Hospital visits: 239
|
| King et al. [101] | Retrospective review of NPDS data from 2000–2014 to identify paediatric ADHD medication exposures | USA | 156,365 |
| Accidental: 128,119 Intentional: 23,034 ADR: 4040 Unknown: 1172 |
| PSS:
|
| Vohra et al. [95] | Retrospective study of exposures using electronic health records and reports to NPDS (2004–2014) | USA | 99 |
| Accidental: 88
|
|
|
| Lin et al. [84] | Retrospective evaluation of medical records of children under 18 who presented to the ED with pharmaceutical poisoning (2001–2008) | Taiwan | 87 | Mean age: 11.26
| Accidental: 34 Intentional: 53 |
| Hospitalised: 87
|
| Conner et al. [96] | Retrospective review of intentional self-poisoning (ISP) cases aged 13–65 treated at a USA University Medical Centre | USA | 673 |
| Intentional (suicide attempt): 673 |
| PSS:
|
| Piotrowska et al. [79] | Retrospective, observational study of patients presenting to ED of Bern University Hospital. Cases were identified using electronic database. | Switzerland | 181 | Mean age: 25 (16–85)
| Accidental: 38 Intentional: 143 |
| Hospitalised: 181
Deaths: 2 |
| Patel et al. [97] | Retrospective, cross-sectional analysis using NPDS from 2010–2014 identifying patients <18 years with exposure to opioid. | USA | 83,418 |
| Accidental: 61,206 Intentional: 20,064 ADR: 1088 Other: 227 |
| PSS:
|
| Reichert et al. [80] | Retrospective review of acute single-agent exposures to pharmaceutical reported to Swiss Toxicological Information Centre (STIC) between 1997–2012 | Switzerland | 313 |
| Accidental: 42 Intentional: 266 Other: 5 |
| Seizures: 313 |
| Sinyor et al. [60] | Retrospective review of drug induced suicides in Toronto using Coroner’s data | Canada | 397 |
| Intentional (suicide attempt): 397 |
| Death: 397 |
| Glaizal et al. [133] | Retrospective review using results of a 2-year national survey by the toxicovigilance network (2008–2010) | USA | 135 | Mean age: 31 (13–58)
| Intentional (suicide attempt): 135 |
| ED: 85 ICU: 38 Death: 10 |
| Cassidy et al. [77] | Prospective study over 3-years on medication errors reported to NPIC | Republic of Ireland | 2348 |
| Accidental (medication error): 2348 |
| PSS:
|
| Calcaterra et al. [134] | Retrospective chart review of data from NPDS between 2001–2014 | USA | 188,452 | Mean age: 31.5
| Intentional: 188,452 |
| Coma: 6264 Respiratory depression: 6766 Death: 124 |
| Eigner et al. [135] | Retrospective review of overdose deaths using Indiana State Department of Health death certificates available through Allen County Coroner’s Office. | USA | 418 |
| Accidental: 336 Intentional: 66 Unknown: 16 |
| Death: 418 |
References
- Alwan, I.A.; Awadh, A.I.; Tangiisuran, B.; Khan, H.R.M.; Yahaya, N.; Majid, M.I. Pharmaceuticals Poisoning: Reported by the National Poison Centre in Malaysia between 2010 and 2015. J. Pharm. Bioallied Sci. 2020, 12, 475–481. [Google Scholar] [CrossRef]
- Darke, S.; Mattick, R.P.; Degenhardt, L. The ratio of non-fatal to fatal heroin overdose. Addiction 2003, 98, 1169–1171. [Google Scholar] [CrossRef]
- Martins, S.S.; Sampson, L.; Cerdá, M.; Galea, S. Worldwide Prevalence and Trends in Unintentional Drug Overdose: A Systematic Review of the Literature. Am. J. Public Health 2015, 105, e29–e49. [Google Scholar] [CrossRef] [PubMed]
- Thanacoody, R.; Anderson, M. Epidemiology of poisoning. Medicine 2020, 48, 153–155. [Google Scholar] [CrossRef]
- Okumura, Y.; Shimizu, S.; Ishikawa, K.B.; Matsuda, S.; Fushimi, K.; Ito, H. Comparison of emergency hospital admissions for drug poisoning and major diseases: A retrospective observational study using a nationwide administrative discharge database. BMJ Open 2012, 2, e001857. [Google Scholar] [CrossRef] [PubMed]
- Mintegi, S.; Esparza, M.J.; González, J.C.; Rubio, B.; Sánchez, F.; Vila, J.J.; Yagüe, F.; Benítez, M.T. Recommendations for the prevention of poisoning. An. Pediatría Engl. Ed. 2015, 83, 440.e441–440.e445. [Google Scholar] [CrossRef]
- Assar, S.; Hatami, S.; Lak, E.; Pipelzadeh, M.; Joorabian, M. Acute poisoning in children. Pak. J. Med. Sci. 2009, 25, 51–54. [Google Scholar]
- Kent, D.A. Out of Sight and Locked Up Tight: Pediatric Pharmaceutical Poisoning. BC Med. J. 2013, 55, 33. [Google Scholar]
- Kurt, M.; Akdeniz, M.; Kavukcu, E. Assessment of Comorbidity and Use of Prescription and Nonprescription Drugs in Patients Above 65 Years Attending Family Medicine Outpatient Clinics. Gerontol. Geriatr. Med. 2019, 5, 2333721419874274. [Google Scholar] [CrossRef]
- Duerden, M. What is the place for monitored dosage systems? Drug Ther. Bull. 2018, 56, 102. [Google Scholar] [CrossRef] [PubMed]
- van Hoving, D.J.; Hunter, L.D.; Gerber, R.E.J.; Lategan, H.J.; Marks, C.J. The burden of intentional self-poisoning on a district-level public Hospital in Cape Town, South Africa. Afr. J. Emerg. Med. 2018, 8, 79–83. [Google Scholar] [CrossRef]
- Hedegaard, H.; Miniño, A.M.; Spencer, M.R.; Warner, M. Drug Overdose Deaths in the United States, 1999–2020; Statistics, N.C.F.H., Ed.; Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2021; Volume NCHS Data Brief, no 428. [CrossRef]
- Rehm, J.; Shield, K.D. Global Burden of Disease and the Impact of Mental and Addictive Disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Mental Health ATLAS 2017; World Health Organisation: Geneva, Switzerland, 2018; p. 68. [Google Scholar]
- Mak, K.K.; Ho, C.S.H.; Zhang, M.W.B.; Day, J.R.; Ho, R.C.M. Characteristics of overdose and non-overdose suicide attempts in a multi-ethnic Asian society. Asian J. Psychiatr. 2013, 6, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, J.; Smyth, R.S. 23—Suicide and self-harm. In Companion to Psychiatric Studies, 8th ed.; Johnstone, E.C., Owens, D.C., Lawrie, S.M., McIntosh, A.M., Sharpe, M., Eds.; Churchill Livingstone: St. Louis, MO, USA, 2010; pp. 693–713. [Google Scholar]
- Sharareh, N.; Sabounchi, S.S.; McFarland, M.; Hess, R. Evidence of Modeling Impact in Development of Policies for Controlling the Opioid Epidemic and Improving Public Health: A Scoping Review. Subst. Abus. Res. Treat. 2019, 13, 1178221819866211. [Google Scholar] [CrossRef]
- World Health Organisation. Opioid Overdose; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]
- Keen, C.; Kinner, S.A.; Young, J.T.; Snow, K.; Zhao, B.; Gan, W.; Slaunwhite, A.K. Periods of altered risk for non-fatal drug overdose: A self-controlled case series. Lancet Public Health 2021, 6, e249–e259. [Google Scholar] [CrossRef]
- Martin, J.; Cunliffe, J.; Décary-Hétu, D.; Aldridge, J. Effect of restricting the legal supply of prescription opioids on buying through online illicit marketplaces: Interrupted time series analysis. BMJ 2018, 361, k2270. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction. Drug-Induced Deaths—The Current Situation in Europe (European Drug Report 2023); European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2023. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. Drug-Related Deaths and Mortality in Europe: Update from the EMCDDA Expert Network; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2021. [Google Scholar]
- Dayasiri, K.; Jayamanne, S.F.; Jayasinghe, C.Y. Accidental and Deliberate Self-Poisoning with Medications and Medication Errors among Children in Rural Sri Lanka. Emerg. Med. Int. 2020, 2020, 9872821. [Google Scholar] [CrossRef]
- Waktola, L.G.; Melese, E.B.; Mesfin, N.; Altaye, K.D.; Legese, G.L. Prevalence of unfavorable outcome in acute poisoning and associated factors at the University of Gondar comprehensive specialized hospital, Gondar, Northwest Ethiopia: A hospital-based cross-sectional study. Front. Public Health 2023, 11, 1160182. [Google Scholar] [CrossRef]
- Mariam, E.T. Global Epidemiology of Acute Poisoning with an Emphasis to Ethipia: Systematic Review. Int. J. Pharma Sci. Sci. Res. 2016, 2, 161–171. [Google Scholar]
- Mittal, C.; Singh, S.; Kumar, -M.P.; Varthya, S.B. Toxicoepidemiology of poisoning exhibited in Indian population from 2010 to 2020: A systematic review and meta-analysis. BMJ Open 2021, 11, e045182. [Google Scholar] [CrossRef]
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Rahman, F.; Rivara, F.; Bartolomeos, K. World Report on Child Injury Prevention; World Health Organisation: Geneva, Switzerland, 2008; Volume 6. [Google Scholar]
- Ndomondo-Sigonda, M.; Miot, J.; Naidoo, S.; Dodoo, A.; Kaale, E. Medicines Regulation in Africa: Current State and Opportunities. Pharmaceut. Med. 2017, 31, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Sithole, T.; Salek, S.; Mahlangu, G.; Walker, S. Comparison of the registration process of the medicines control authority of Zimbabwe with Australia, Canada, Singapore, and Switzerland: Benchmarking best practices. Expert. Rev. Clin. Pharmacol. 2021, 15, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Mao, W.; Vu, H.; Xie, Z.; Chen, W.; Tang, S. Systematic review on irrational use of medicines in China and Vietnam. PLoS ONE 2015, 10, e0117710. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- World Health Organisation. Guidelines for Poison Control; World Health Organisation: Geneva, Switzerland, 1997. [Google Scholar]
- World Health Organisation. Guidelines for Establishing a Posion Centre; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]
- Hamadeh, N.; van Rompaey, C.; Metreau, E. New World Bank Country Classifications by Income Level: 2021–2022. Available online: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2021-2022 (accessed on 31 December 2021).
- World Health Organisation. Anatomical Therapeutic Chemical (ATC) Classidication; World Health Organisation: Geneva, Switzerland, 2021; Volume 2021. [Google Scholar]
- Cairns, R.; Buckley, N.A. The Poisoning Severity Score: If It Did Not Exist, We Would Have To Invent It. J. Med. Toxicol. 2017, 13, 131–134. [Google Scholar] [CrossRef]
- World Health Organsiation. Recognizing Adolescence; World Health Organsiation: Geneva, Switzerland, 2014; Volume 2022. [Google Scholar]
- Bilel, C.; Zergui, A.; Rahmani, C.; Belmessabih, M.; Rezk-Kallah, H. Acute paracetamol poisonings received at the Oran University Hospital. Toxicol. Rep. 2020, 7, 1172–1177. [Google Scholar] [CrossRef]
- Buffone, I.; Dejter, M.; Fortunatti, E.; García Elliot, F.; Irazabal, C.; Marlia, R.; Mujica, D.; Parrou, M.; Romano, M.; Speciale, G.; et al. Characterization of drug poisoning among adolescents seen at the municipal hospital of Bahía Blanca, Province of Buenos Aires, Argentina. Arch. Argent. Pediatr. 2018, 116, 275–282. [Google Scholar] [CrossRef]
- Nagaraju, K.; Ganapathy, R.S. Pattern of pharmaceutical drug poisoning in south indian tertiary care hospitals. Int. Res. J. Pharm. 2016, 7, 44–47. [Google Scholar] [CrossRef]
- Anthony, L.; Kulkarni, C. Patterns of poisoning and drug overdosage and their outcome among in-patients admitted to the emergency medicine department of a tertiary care hospital. Indian. J. Crit. Care Med. 2012, 16, 130–135. [Google Scholar] [CrossRef]
- Ghaemi, N.; Alikhani, S.; Bagheri, S.; Sezavar, M. A Cross Sectional Study of Opioid Poisoning in Children at a Tertiary Center. Asia Pac. J. Med. Toxicol. 2016, 5, 115–118. [Google Scholar] [CrossRef]
- Jabbehdari, S.; Farnaghi, F.; Shariatmadari, S.F.; Jafari, N.; Mehregan, F.-F.; Karimzadeh, P. Accidental children poisoning with methadone: An Iranian pediatric sectional study. Iran. J. Child. Neurol. 2013, 7, 32–34. [Google Scholar]
- Mehrpour, O.; Akbari, A.; Jahani, F.; Amirabadizadeh, A.; Allahyari, E.; Mansouri, B.; Ng, P.C. Epidemiological and clinical profiles of acute poisoning in patients admitted to the intensive care unit in eastern Iran (2010 to 2017). BMC Emerg. Med. 2018, 18, 30. [Google Scholar] [CrossRef]
- Bagherian Rad, N.; Rahimi, M. Pattern of NSAID Poisoning in a Referral Poisoning Center of Iran: Solutions to Reduce the Suicide. Iran. J. Pharm. Res. 2019, 18, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Shadnia, S.; Brent, J.; Mousavi-Fatemi, K.; Hafezi, P.; Soltaninejad, K. Recurrent Seizures in Tramadol Intoxication: Implications for Therapy Based on 100 Patients. Basic. Clin. Pharmacol. Toxicol. 2012, 111, 133–136. [Google Scholar] [CrossRef]
- Hashmnejad, M.; Fatehi, R. Epidemiological Study of Poisoning in Patients of Karaj Shariati Hospital in 2011 to 2012. Int. J. Med. Toxicol. Forensic Med. 2014, 4, 17–22. [Google Scholar] [CrossRef]
- Khodabandeh, F.; Agin, K. Assessment of Aspiration-Induced Lung Injuries among Acute Drug Poisoning Patients.; Loghman Hakim Hospital, Poisoning Center. Int. J. Med. Toxicol. Forensic Med. 2016, 6, 209–216. [Google Scholar]
- Hamedi, A.; Ghahremani, S.; Nakhaei, A.A.; Balali, M.R.; Ghahremani, S. A Cross Sectional Study on Pediatric Methadone Poisoning in Northeast of Iran. Asia Pac. J. Med. Toxicol. 2016, 5, 75–78. [Google Scholar]
- Yehya, A.; Albals, D.; Issa, R.; Fawadleh, A. Retrospective assessment of acute poisoning incidents by pharmaceutical agents in Jordan: Data from Pharmacy OneTM Poison Call Center, 2014 to 2018-Part II. Pharmacol. Res. Perspect. 2020, 8, e00583. [Google Scholar] [CrossRef] [PubMed]
- Azekour, K.; Belamalem, S.; Soulaymani, A.; El Houate, B.; El Bouhali, B. Epidemiological Profile of Drug Overdose Reported in South-East Morocco from 2004 to 2016. Drugs Real World Outcomes 2019, 6, 11–17. [Google Scholar] [CrossRef]
- Sorodoc, V.; Jaba, I.M.; Lionte, C.; Mungiu, O.C.; Sorodoc, L. Epidemiology of acute drug poisoning in a tertiary center from Iasi County, Romania. Hum. Exp. Toxicol. 2011, 30, 1896–1903. [Google Scholar] [CrossRef]
- Weerasinghe, M.; Konradsen, F.; Eddleston, M.; Pearson, M.; Agampodi, T.; Storm, F.; Agampodi, S. Overdose of oral contraceptive pills as a means of intentional self-poisoning amongst young women in Sri Lanka: Considerations for family planning. J. Fam. Plan. Reprod. Health Care 2017, 43, 147–150. [Google Scholar] [CrossRef]
- Hocaoğlu, N.; Yıldıztepe, E.; Bayram, B.; Aydın, B.; Tunçok, Y.; Kalkan, Ş. Demographic and Clinical Characteristics of Theophylline Exposures between 1993 and 2011. Balk. Med. J. 2014, 31, 322–327. [Google Scholar] [CrossRef]
- Yaylaci, S.; Genc, A.B.; Demir, M.V.; Cinemre, H.; Tamer, A. Retrospective evaluation of patients at follow-up with acute poisoning in Intensive Care Unit. Niger. J. Clin. Pract. 2016, 19, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Cairns, R.; Daniels, B.; Wood, D.A.; Brett, J. ADHD medication overdose and misuse: The NSW poisons information centre experience, 2004–2014. Med. J. Aust. 2016, 204, 154.e151–154.e157. [Google Scholar] [CrossRef]
- Lee, J.; Pilgrim, J.; Gerostamoulos, D.; Robinson, J.; Wong, A. Increasing rates of quetiapine overdose, misuse, and mortality in Victoria, Australia. Drug Alcohol. Depend. 2018, 187, 95–99. [Google Scholar] [CrossRef]
- Madadi, P.; Hildebrandt, D.; Lauwers, A.E.; Koren, G. Characteristics of Opioid-Users Whose Death Was Related to Opioid-Toxicity: A Population-Based Study in Ontario, Canada. PLoS ONE 2013, 8, e60600. [Google Scholar] [CrossRef]
- Gomes, T.; Khuu, W.; Craiovan, D.; Martins, D.; Hunt, J.; Lee, K.; Tadrous, M.; Mamdani, M.; Paterson, J.; Juurlink, D. Comparing the contribution of prescribed opioids to opioid-related hospitalizations across Canada: A multi-jurisdictional cross-sectional study. Drug Alcohol. Depend. 2018, 191, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Sinyor, M.; Howlett, A.; Cheung, A.H.; Schaffer, A. Substances used in completed suicide by overdose in Toronto: An observational study of coroner’s data. Can. J. Psychiatry 2012, 57, 184–191. [Google Scholar] [CrossRef]
- Zakharov, S.; Navratil, T.; Pelclova, D. Non-fatal suicidal self-poisonings in children and adolescents over a 5-year period (2007–2011). Basic. Clin. Pharmacol. Toxicol. 2013, 112, 425–430. [Google Scholar] [CrossRef]
- Jensen, L.L.; Rømsing, J.; Dalhoff, K. A Danish Survey of Antihistamine Use and Poisoning Patterns. Basic. Clin. Pharmacol. Toxicol. 2017, 120, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.B.; Petersen, K.M.; Bøgevig, S.; Al-Gibouri, S.; Jimenez-Solem, E.; Dalhoff, K.P.; Petersen, T.S.; Andersen, J.T. Outcomes following calcium channel blocker exposures reported to a poison information center. BMC Pharmacol. Toxicol. 2018, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Christensen, A.P.; Boegevig, S.; Christensen, M.B.; Petersen, K.M.; Dalhoff, K.P.; Petersen, T.S. Overdoses with Aripiprazole: Signs, Symptoms and Outcome in 239 Exposures Reported to the Danish Poison Information Centre. Basic. Clin. Pharmacol. Toxicol. 2018, 122, 293–298. [Google Scholar] [CrossRef]
- Koskela, L.; Raatiniemi, L.; Bakke, H.K.; Ala-Kokko, T.; Liisanantti, J. Fatal poisonings in Northern Finland: Causes, incidence, and rural-urban differences. Scand. J. Trauma. Resusc. Emerg. Med. 2017, 25, 90. [Google Scholar] [CrossRef] [PubMed]
- Kriikku, P.; Hakkinen, M.; Ojanpera, I. High buprenorphine-related mortality is persistent in Finland. Forensic Sci. Int. 2018, 291, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Torrents, R.; Picot, C.; Glaizal, M.; Courne, M.A.; Schmitt, C.; Richard, N.; Simon, N.; Cardona, F.; De Haro, L. Child poisonings with methadone in France: A 6-year prospective national survey since the availability of capsules in 2008. Clin. Toxicol. 2015, 53, 819–822. [Google Scholar] [CrossRef]
- Stevens, A.; Hamel, J.F.; Toure, A.; Hadjadj, S.; Boels, D. Metformin overdose: A serious iatrogenic complication-Western France Poison Control Centre Data Analysis. Basic. Clin. Pharmacol. Toxicol. 2019, 125, 466–473. [Google Scholar] [CrossRef]
- Torrents, R.; Glaizal, M.; Sinno-Tellier, S.; Richard, N.; Nisse, P.; Vodovar, D.; Bloch, J.; Simon, N.; de Haro, L. Methadone poisonings: A seven-year retrospective study of the French poison center network focusing on suicide attempts vs. misuses. Fundam. Clin. Pharmacol. 2020, 34, 290–295. [Google Scholar] [CrossRef]
- Feingold, D.; Goldberger, N.; Haklai, Z.; Lev-Ran, S. Fatal Overdoses of Opioids in Israel 2005–2014. Eur. Addict. Res. 2017, 23, 276–283. [Google Scholar] [CrossRef]
- Lavon, O.; Ben-Zeev, A.; Bentur, Y. Medication errors outside healthcare facilities: A national poison centre perspective. Basic. Clin. Pharmacol. Toxicol. 2014, 114, 288–292. [Google Scholar] [CrossRef]
- Ichikura, K.; Okumura, Y.; Takeuchi, T. Associations of Adverse Clinical Course and Ingested Substances among Patients with Deliberate Drug Poisoning: A Cohort Study from an Intensive Care Unit in Japan. PLoS ONE 2016, 11, e0161996. [Google Scholar] [CrossRef]
- Haoka, T.; Sakata, N.; Okamoto, H.; Oshiro, A.; Shimizu, T.; Naito, Y.; Onishi, S.; Morishita, Y.; Nara, S. Intentional or unintentional drug poisoning in elderly people: Retrospective observational study in a tertiary care hospital in Japan. Acute Med. Surg. 2019, 6, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Shipton, E.E.; Shipton, A.J.; Williman, J.A.; Shipton, E.A. Deaths from Opioid Overdosing: Implications of Coroners’ Inquest Reports 2008–2012 and Annual Rise in Opioid Prescription Rates: A Population-Based Cohort Study. Pain Ther. 2017, 6, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Kominek, K.; Pawłowska-Kamieniak, A.; Mroczkowska-Juchkiewicz, A.; Krawiec, P.; Pac-Kożuchowska, E. Intentional and accidental paracetamol poisoning in childhood—A retrospective analysis. Postep. Hig Med Dosw Online 2015, 69, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Mroczkowska-Juchkiewicz, A.; Krawiec, P.; Pawłowska-Kamieniak, A.; Gołyska, D.; Kominek, K.; Pac-Kożuchowska, E. Intentional poisonings in urban and rural children—A 6-year retrospective single centre study. Ann. Agric. Environ. Med. 2016, 23, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, N.; Duggan, E.; Williams, D.J.P.; Tracey, J.A. The epidemiology and type of medication errors reported to the National Poisons Information Centre of Ireland. Clin. Toxicol. 2011, 49, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Martos, V.; Hofer, K.E.; Rauber-Lüthy, C.; Schenk-Jaeger, K.M.; Kupferschmidt, H.; Ceschi, A. Acute toxicity profile of tolperisone in overdose: Observational poison centre-based study. Clin. Toxicol. 2015, 53, 470–476. [Google Scholar] [CrossRef]
- Piotrowska, N.; Klukowska-Rötzler, J.; Lehmann, B.; Krummrey, G.; Haschke, M.; Exadaktylos, A.K.; Liakoni, E. Presentations Related to Acute Paracetamol Intoxication in an Urban Emergency Department in Switzerland. Emerg. Med. Int. 2019, 2019, 3130843. [Google Scholar] [CrossRef]
- Reichert, C.; Reichert, P.; Monnet-Tschudi, F.; Kupferschmidt, H.; Ceschi, A.; Rauber-Luthy, C. Seizures after single-agent overdose with pharmaceutical drugs: Analysis of cases reported to a poison center. Clin. Toxicol. 2014, 52, 629–634. [Google Scholar] [CrossRef]
- Alruwaili, N.D.; Halimeh, B.; Al-Omar, M.; Alhatali, B.; Sabie, I.I.; Alsaqoub, M. An epidemiological snapshot of toxicological exposure in children 12 years of age and younger in Riyadh. Ann. Saudi Med. 2019, 39, 229–235. [Google Scholar] [CrossRef]
- Tobaiqy, M.; Asiri, B.A.; Sholan, A.H.; Alzahrani, Y.A.; Alkatheeri, A.A.; Mahha, A.M.; Alzahrani, S.S.; MacLure, K. Frequency and Management of Acute Poisoning among Children Attending an Emergency Department in Saudi Arabia. Pharm 2020, 8, 189. [Google Scholar] [CrossRef]
- Tan, C.J.; Sklar, G.E. Characterisation and outcomes of adult patients with paracetamol overdose presenting to a tertiary hospital in Singapore. Singap. Med. J. 2017, 58, 695–702. [Google Scholar] [CrossRef]
- Lin, Y.R.; Liu, T.H.; Liu, T.A.; Chang, Y.J.; Chou, C.C.; Wu, H.P. Pharmaceutical poisoning exposure and outcome analysis in children admitted to the pediatric emergency department. Pediatr. Neonatol. 2011, 52, 11–17. [Google Scholar] [CrossRef]
- Kamour, A.; Crichton, S.; Cooper, G.; Lupton, D.J.; Eddleston, M.; Vale, J.A.; Thompson, J.P.; Thomas, S.H.L. Central nervous system toxicity of mefenamic acid overdose compared with other NSAIDs: An analysis of cases reported to the United Kingdom National Poisons Information Service. Br. J. Clin. Pharmacol. 2017, 83, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.C.; Rocque, M. Accidental and non-accidental ingestion of methadone and buprenorphine in childhood: A single center experience, 1999-2009. Curr. Drug Saf. 2011, 6, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Eluri, M.; Spiller, H.A.; Casavant, M.J.; Chounthirath, T.; Conner, K.A.; Smith, G.A. Analgesic-Related Medication Errors Reported to US Poison Control Centers. Pain. Med. 2018, 19, 2357–2370. [Google Scholar] [CrossRef] [PubMed]
- Post, S.; Spiller, H.A.; Casavant, M.J.; Chounthirath, T.; Smith, G.A. Buprenorphine exposures among children and adolescents reported to us poison control centers. Pediatrics 2018, 142, e20173652. [Google Scholar] [CrossRef] [PubMed]
- Austin, A.E.; Proescholdbell, S.K.; Creppage, K.E.; Asbun, A. Characteristics of self-inflicted drug overdose deaths in North Carolina. Drug Alcohol. Depend. 2017, 181, 44–49. [Google Scholar] [CrossRef]
- Friedrich, J.M.; Sun, C.; Geng, X.; Calello, D.P.; Gillam, M.; Medeiros, K.L.; Smith, M.; Ruck, B.; Mazer-Amirshahi, M. Child and adolescent benzodiazepine exposure and overdose in the United States: 16 years of poison center data. Clin. Toxicol. 2020, 58, 725–731. [Google Scholar] [CrossRef]
- Toce, M.S.; Burns, M.M.; O’Donnell, K.A. Clinical effects of unintentional pediatric buprenorphine exposures: Experience at a single tertiary care center. Clin. Toxicol. 2017, 55, 12–17. [Google Scholar] [CrossRef]
- Tadros, A.; Layman, S.M.; Davis, S.M.; Bozeman, R.; Davidov, D.M. Emergency department visits by pediatric patients for poisoning by prescription opioids. Am. J. Drug Alcohol. Abus. 2016, 42, 550–555. [Google Scholar] [CrossRef]
- Tadros, A.; Layman, S.M.; Davis, S.M.; Davidov, D.M.; Cimino, S. Emergency Visits for Prescription Opioid Poisonings. J. Emerg. Med. 2015, 49, 871–877. [Google Scholar] [CrossRef]
- Gregoriano, C.; Ceschi, A.; Rauber-Lüthy, C.; Kupferschmidt, H.; Banner, N.R.; Krähenbühl, S.; Taegtmeyer, A.B. Acute thiopurine overdose: Analysis of reports to a National Poison Centre 1995–2013. PLoS ONE 2014, 9, e86390. [Google Scholar] [CrossRef]
- Vohra, R.; Huntington, S.; Koike, J.; Le, K.; Geller, R.J. Pediatric Exposures to Topical Benzocaine Preparations Reported to a Statewide Poison Control System. West. J. Emerg. Med. 2017, 18, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Conner, K.R.; Wiegand, T.J.; Gorodetsky, R.; Schult, R.F.; Kaukeinen, K. Poisoning Severity Associated with a Range of Medications in Suicide Attempts by Ingestion. Suicide Life Threat. Behav. 2019, 49, 635–642. [Google Scholar] [CrossRef]
- Patel, A.M.; Wheeler, D.C.; Rose, S.R.; Nadpara, P.A.; Pakyz, A.L.; Carroll, N.V. Prevalence and Characteristics of Pediatric Opioid Exposures and Poisonings in the United States. J. Pediatr. 2019, 206, 148–155.e144. [Google Scholar] [CrossRef] [PubMed]
- Lasoff, D.R.; Koh, C.H.; Corbett, B.; Minns, A.B.; Cantrell, F.L. Loperamide Trends in Abuse and Misuse Over 13 Years: 2002–2015. Pharmacotherapy 2017, 37, 249–253. [Google Scholar] [CrossRef]
- Vakkalanka, J.P.; Charlton, N.P.; Holstege, C.P. Epidemiologic Trends in Loperamide Abuse and Misuse. Ann. Emerg. Med. 2017, 69, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Caupp, S.; Steffan, J.; Shi, J.; Wheeler, K.K.; Spiller, H.A.; Casavant, M.J.; Xiang, H. Opioid drug poisonings in Ohio adolescents and young adults, 2002–2014. Clin. Toxicol. 2018, 56, 765–772. [Google Scholar] [CrossRef]
- King, S.A.; Casavant, M.J.; Spiller, H.A.; Hodges, N.L.; Chounthirath, T.; Smith, G.A. Pediatric ADHD Medication Exposures Reported to US Poison Control Centers. Pediatrics 2018, 141, e20173872. [Google Scholar] [CrossRef]
- Miller, T.R.; Swedler, D.I.; Lawrence, B.A.; Ali, B.; Rockett, I.R.H.; Carlson, N.N.; Leonardo, J. Incidence and Lethality of Suicidal Overdoses by Drug Class. JAMA Netw. Open 2020, 3, e200607. [Google Scholar] [CrossRef]
- Okic, M.; Cnossen, L.; Crifasi, J.A.; Long, C.; Mitchell, E.K. Opioid Overdose Mortality in Kansas, 2001–2011: Toxicologic Evaluation of Intent. J. Anal. Toxicol. 2013, 37, 629–635. [Google Scholar] [CrossRef]
- Iemmi, V.; Bantjes, J.; Coast, E.; Channer, K.; Leone, T.; McDaid, D.; Palfreyman, A.; Stephens, B.; Lund, C. Suicide and poverty in low-income and middle-income countries: A systematic review. Lancet Psychiatry 2016, 3, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Patel, I.; Balkrishnan, R. Medication Error Management around the Globe: An Overview. Indian J. Pharm. Sci. 2010, 72, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Pawer, S.; Rajabali, F.; Zheng, A.; Pike, I.; Purssell, R.; Zargaran, A.; Babul, S. Socioeconomic factors and substances involved in poisoning-related emergency department visits in British Columbia, Canada. Health Promot. Chronic Dis. Prev. Can. 2021, 41, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Getie, A.; Belayneh, Y.M. A Retrospective Study of Acute Poisoning Cases and Their Management at Emergency Department of Dessie Referral Hospital, Northeast Ethiopia. Drug Healthc. Patient Saf. 2020, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Social Determinants of Mental Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Bhadelia, A.; De Lima, L.; Arreola-Ornelas, H.; Kwete, X.J.; Rodriguez, N.M.; Knaul, F.M. Solving the Global Crisis in Access to Pain Relief: Lessons from Country Actions. Am. J. Public. Health 2019, 109, 58–60. [Google Scholar] [CrossRef]
- Knaul, F.M.; Farmer, P.E.; Krakauer, E.L.; De Lima, L.; Bhadelia, A.; Jiang Kwete, X.; Arreola-Ornelas, H.; Gómez-Dantés, O.; Rodriguez, N.M.; Alleyne, G.A.O.; et al. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: The Lancet Commission report. Lancet 2018, 391, 1391–1454. [Google Scholar] [CrossRef]
- OECD. Addressing Problematic Opioid Use in OECD Countries; OECD: Paris, France, 2019. [Google Scholar]
- Gunnell, D.; Ho, D.; Murray, V. Medical management of deliberate drug overdose: A neglected area for suicide prevention? Emerg. Med. J. 2004, 21, 35. [Google Scholar] [CrossRef]
- Espinosa-Jovel, C.; Toledano, R.; Aledo-Serrano, Á.; García-Morales, I.; Gil-Nagel, A. Epidemiological profile of epilepsy in low income populations. Seizure 2018, 56, 67–72. [Google Scholar] [CrossRef]
- Rathod, S.; Pinninti, N.; Irfan, M.; Gorczynski, P.; Rathod, P.; Gega, L.; Naeem, F. Mental Health Service Provision in Low- and Middle-Income Countries. Health Serv. Insights 2017, 10, 1178632917694350. [Google Scholar] [CrossRef]
- Zhao, P.; Li, S.; Liu, D. Unequable spatial accessibility to hospitals in developing megacities: New evidence from Beijing. Health Place 2020, 65, 102406. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Poison Control and Unintentional Poisoning; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- National Academiesof-Sciences, Engineering and Medicine; Healthand-Medicine-Division; Board-on-Health-Sciences-Policy; Committee on Pain Management and-Regulatory Strategies-to-Address Prescription Opioid Abuse. 5. Evidence on Strategies for Addressing the Opioid Epidemic. In Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use; Jonathan, K., Phillips, M.A.F., Richard, J.B., Eds.; National Academies Press (US): Washington, DC, USA, 2017. [Google Scholar]
- Tabeefar, H.; Chang, F.; Cooke, M.; Patel, T. Community pharmacists and chronic pain: A qualitative study of experience, perception, and challenges. Can. J. Pain. 2020, 4, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, N.; Beletsky, L.; Ciccarone, D. Opioid Crisis: No Easy Fix to Its Social and Economic Determinants. Am. J. Public Health 2018, 108, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.; Goodman, C. Performance of retail pharmacies in low- and middle-income Asian settings: A systematic review. Health Policy Plan. 2016, 31, 940–953. [Google Scholar] [CrossRef]
- Leisinger, K.M.; Garabedian, L.F.; Wagner, A.K. Improving access to medicines in low and middle income countries: Corporate responsibilities in context. South. Med. Rev. 2012, 5, 3–8. [Google Scholar]
- Hamid, H.; Masood, R.A.; Tariq, H.; Khalid, W.; Rashid, M.A.; Munir, M.U. Current pharmacy practices in low- and middle-income countries; recommendations in response to the COVID-19 pandemic. Drugs Ther. Perspect. 2020, 36, 355–357. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Guidelines on the Prevention of Toxic Exposures: Education and Public Awareness Activities; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Kara, H.; Bayir, A.; Degirmenci, S.; Akinci, M.; Ak, A.; Kayis, S.; Agacayak, A.; Azap, M. Causes of poisoning in patients evaluated in a hospital emergency department in Konya, Turkey. J. Pak. Med. Assoc. 2014, 64, 1042–1048. [Google Scholar]
- Taheri, F.; Yaraghi, A.; Sabzghabaee, A.M.; Moudi, M.; Eizadi-Mood, N.; Gheshlaghi, F.; Farajzadegan, Z. Methadone toxicity in a poisoning referral center. J. Res. Pharm. Pract. 2013, 2, 130–134. [Google Scholar] [CrossRef]
- Creswell, P.D.; Gibson, C.; Theobald, J.; Meiman, J.G. Exposures to Opioids among Wisconsin Children and Adolescents, 2002-2016. Wmj 2019, 118, 9–15. [Google Scholar]
- Thongprayoon, C.; Petnak, T.; Kaewput, W.; Mao, M.A.; Kovvuru, K.; Kanduri, S.R.; Boonpheng, B.; Bathini, T.; Vallabhajosyula, S.; Pivovarova, A.I.; et al. Hospitalizations for Acute Salicylate Intoxication in the United States. J. Clin. Med. 2020, 9, 2638. [Google Scholar] [CrossRef]
- Manini, A.F.; Nelson, L.S.; Stimmel, B.; Vlahov, D.; Hoffman, R.S. Incidence of adverse cardiovascular events in adults following drug overdose. Acad. Emerg. Med. 2012, 19, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Vilay, A.; Wong, C.; Schrader, R.; Mercier, R.-C.; Seifert, S. Indicators for serious kidney complications associated with toxic exposures: An analysis of the National Poison Data System. Clin. Toxicol. 2013, 51, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, M.A.; Shah, B.B.; Morgan, B.W.; Houry, D.; Kazzi, Z.N. Injury secondary to antiretroviral agents: Retrospective analysis of a regional poison center database. West. J. Emerg. Med. 2011, 12, 293–295. [Google Scholar] [PubMed]
- Feng, J.; Iser, J.; Yang, W. Medical encounters for opioid-related intoxications in Southern Nevada: Sociodemographic and clinical correlates. BMC Health Serv. Res. 2016, 16, 438. [Google Scholar] [CrossRef]
- Truitt, C.A.; Brooks, D.E.; Dommer, P.; LoVecchio, F. Outcomes of unintentional beta-blocker or calcium channel blocker overdoses: A retrospective review of poison center data. J. Med. Toxicol. 2012, 8, 135–139. [Google Scholar] [CrossRef]
- Glaizal, M.; Gazin, V.; Aymard, I.; Messina-Gourlot, C.; Richard, N.; Mallaret, M.; Saviuc, P.; De Haro, L. Suicidal poisonings with methadone in France: Results of a two year national survey by the Toxicovigilance Network. Clin. Toxicol. 2012, 50, 841–846. [Google Scholar] [CrossRef]
- Calcaterra, S.L.; Severtson, S.G.; Bau, G.E.; Margolin, Z.R.; Bucher-Bartelson, B.; Green, J.L.; Dart, R.C. Trends in intentional abuse or misuse of benzodiazepines and opioid analgesics and the associated mortality reported to poison centers across the United States from 2000 to 2014. Clin. Toxicol. 2018, 56, 1107–1114. [Google Scholar] [CrossRef]
- Eigner, G.; Henriksen, B.; Huynh, P.; Murphy, D.; Brubaker, C.; Sanders, J.; McMahan, D. Who is Overdosing? An Updated Picture of Overdose Deaths from 2008 to 2015. Health Serv. Res. Manag. Epidemiol. 2017, 4, 233339281772742. [Google Scholar] [CrossRef]


| Poison Terms | Pharmaceutical Terms |
|---|---|
| Poison * | Pharmaceutical |
| Toxic | Medicine |
| Overdose | Drug |
| Intoxication | Opioid |
| Excessive | |
| Substance abuse | |
| Drug Misuse |
| Low-Middle-Income Countries (n = 21) | High-Income Countries * (n = 58) |
|---|---|
| Algeria: 1 [38] Argentina: 1 [39] India: 2 [40,41] Iran: 9 [42,43,44,45,46,47,48,49] Jordan: 1 [50] Morocco: 1 [51] Romania: 1 [52] South Africa: 1 [11] Sri Lanka: 1 [53] Turkey: 3 [54,55] | Australia: 2 [56,57] Canada: 3 [58,59,60] Czech Republic: 1 [61] Denmark: 3 [62,63,64] Finland: 2 [65,66] France: 3 [67,68,69] Israel: 2 [70,71] Japan: 2 [72,73] New Zealand: 1 [74] Poland: 2 [75,76] Republic of Ireland: 1 [77] Switzerland: 4 [78,79,80] Saudi Arabia: 2 [81,82] Singapore: 1 [83] Taiwan: 1 [84] UK: 1 [85] USA: 27 [86,87,88,89,90,91,92,93] |
| ATC 1st Level Classification | LMIC (n) | HIC (n) |
|---|---|---|
| A. Alimentary tract and metabolism | 336 | 2721 |
| B. Blood and blood forming organs | 15 | 29 |
| C. Cardiovascular system | 193 | 2947 |
| D. Dermatological | 0 | 219 |
| G. Genito urinary system and sex hormones | 60 | 79 |
| H. Systemic hormonal preparations, excluding sex hormones and insulins | 66 | 30 |
| J. Anti-infective for systemic use | 185 | 635 |
| L. Antineoplastic and immunomodulating agents | 0 | 43 |
| M. Musculo-skeletal system | 496 | 37,736 |
| N. Nervous System | 3096 | 1,365,780 |
| R. Respiratory system | 478 | 2775 |
| Combination of pharmaceuticals ingested | 844 | 27,168 |
| Nervous System | LMIC (n, %) | HIC (n, %) |
|---|---|---|
| Analgesics | 1236 (39.9) | 783,654 (57.3) |
| Antiepileptics | 287 (9.27) | 1194 (0.87) |
| Anti-Parkinson drugs | 0 (0) | 194 (0.01) |
| Psycholeptics | 618 (20.0) | 105,036 (7.69) |
| Psychoanaleptics | 383 (12.4) | 461,019 (33.8) |
| Drugs used in opioid dependence | 572 (18.5) | 14,683 (10.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cowans, C.; Love, A.; Tangiisuran, B.; Jacob, S.A. Uncovering the Hidden Burden of Pharmaceutical Poisoning in High-Income and Low-Middle-Income Countries: A Scoping Review. Pharmacy 2023, 11, 184. https://doi.org/10.3390/pharmacy11060184
Cowans C, Love A, Tangiisuran B, Jacob SA. Uncovering the Hidden Burden of Pharmaceutical Poisoning in High-Income and Low-Middle-Income Countries: A Scoping Review. Pharmacy. 2023; 11(6):184. https://doi.org/10.3390/pharmacy11060184
Chicago/Turabian StyleCowans, Claire, Anya Love, Balamurugan Tangiisuran, and Sabrina Anne Jacob. 2023. "Uncovering the Hidden Burden of Pharmaceutical Poisoning in High-Income and Low-Middle-Income Countries: A Scoping Review" Pharmacy 11, no. 6: 184. https://doi.org/10.3390/pharmacy11060184