

Adult Patients with Difficulty Swallowing Oral Dosage Forms: A Systematic Review of the Quantitative Literature

Abstract
:1. Introduction
2. Search Strategy
- Quality Appraisal
- Data Synthesis
- Review Criteria
3. Results
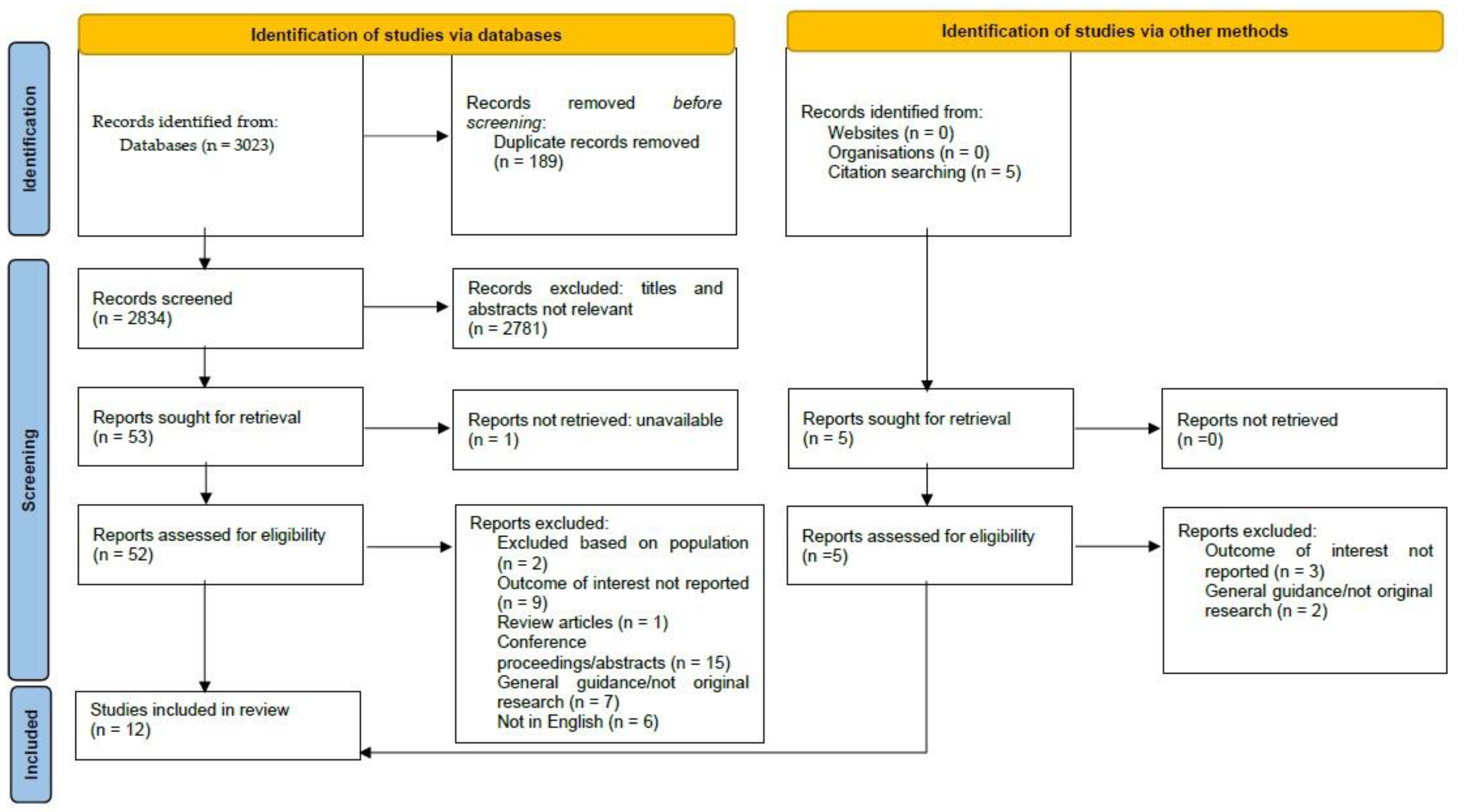
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Dates of Publication
3.2.2. Country
3.2.3. Study Design
3.2.4. Study Participants and Settings
3.2.5. Age of Participants
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Bourdenet et al. [25] 2015; n = 719 patients. | Prospective, observational study. | Patients ≥ 65 years, Inpatients in 23 geriatric units in Rouen University Hospital Centre (acute geriatric medicine, post -acute rehabilitation, nursing homes, long-term care units). |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Carvajal et al., 2016; [33] n = 1875 patients | Quasi-experimental, multicentre, transversal, prospective, before-and-after observational study. | Residents in 10 nursing homes. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Fodil et al., 2016; [26] n = 526 patients for prevalence survey and n = 143 patients for administration survey. | Prospective, observational study. | Inpatients with swallowing difficulties in 17 geriatric units (acute geriatric care, rehabilitation unit, long term care) of the 3 Paris-Sud teaching hospitals. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design and Study Duration | |
| Kelly et al., 2011; [27] n = 625 patients | Undisguised direct observational study. | Inpatients at a care-of-the-elderly ward or stroke unit at each of the four acute hospitals in the east of England. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Kirkevold et al., 2010; [29] n = 1943 residents/patients. | Retrospective data collection performed by nurses. | Inpatients in nursing homes in the South–East Health Region in Norway and nursing homes in the small and large municipalities in rural and urban areas. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Mercovich et al., 2013; [34] n = 160 residents/patients. | Prospective, observational study. | Convenience sample of inpatients and consenting nurses in two aged care facilities that included high-care and dementia unit co-located facilities within the Australian Capital Territory. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Santos et al., 2016; [28] England; n = 166 patients. | Prospective, observational study. | Inpatients with swallowing difficulties in six private care homes in North Yorkshire. Care home provided nursing care and administered medicines to patients with dysphagia or via an enteral feed tube. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Sestili et al., 2018; [35] n = 41 patients at admission, n = 29 patients at discharge. | Retrospective, medical record review. Four months. | Patients hospitalised in two elderly care wards or one neurology unit in the Italian National Research Centre on Aging of Ancona. Age > 79 years Diagnosis of dysphagia carried out by the Speech and Language therapists before hospital admission or during hospitalisation. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Solberg et al., 2021; [30] n = 100 residents. | Prospective, cross sectional, observational study. | Residents in eight nursing home wards across six municipalities in mid-Norway. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants. | Study Design | Participants Included |
| Stuijt et al., 2012; [31] n = 290 for prevalence. Pre-intervention (n = 60) residents. First evaluation (n = 55) and second intervention (n = 62). | Prospective, observational before–after design, study. | Residents with swallowing difficulties in six psychogeriatric wards in two Dutch nursing homes. |
- Relevant Outcomes
- Results
| Author; Year; Number of Participants | Study Design | Participants Included |
| Van Welie et al., 2016; [32] n = 164 patients pre-intervention and n = 150 patients post intervention. | Prospective, uncontrolled, observational study with a pre-intervention and post-intervention measurement. | Inpatients on 18 wards in 3 nursing homes in the North of the Netherlands receiving medication on an observed drug round. |
- Relevant Outcomes
- Results
3.3. Quality Appraisal
3.4. Prevalence of Patients with Dysphagia
3.5. Medicines Manipulation Practices for Administration
3.6. Medication Administration Errors (MAE)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Arnet, I.; Messerli, M.; Oezvegyi, J.; Hersberger, K.; Sahm, L. Translation to English, cross-cultural adaptation, and pilot testing of the self-report questionnaire on swallowing difficulties with medication intake and coping strategies (SWAMECO) for adults with polypharmacy. BMJ Open 2020, 10, e036761. [Google Scholar] [CrossRef]
- Hugtenburg, J.G.; Timmers, L.; Elders, P.J.; Vervloet, M.; van Dijk, L. Definitions, variants, and causes of nonadherence with medication: A challenge for tailored interventions. Patient Prefer. Adherence 2013, 7, 675–682. [Google Scholar] [CrossRef]
- ebin.pub. Optimizing Pharmacotherapy in Older Patients: An Interdisciplinary Approach 3031280601, 9783031280603. 2023. Available online: https://ebin.pub/optimizing-pharmacotherapy-in-older-patients-an-interdisciplinary-approach-3031280601-9783031280603.html (accessed on 8 October 2023).
- Fields, J.; Go, J.T.; Schulze, K.S. Pill properties that cause dysphagia and treatment failure. Curr. Ther. Res. 2015, 77, 79–82. [Google Scholar] [CrossRef] [PubMed]
- James, A. The legal and clinical implications of crushing tablet medication. Nurs. Times 2004, 100, 28–29. [Google Scholar]
- Cross, A.J.; Elliott, R.A.; Petrie, K.; Kuruvilla, L.; George, J. Interventions for improving medication-taking ability and adherence in older adults prescribed multiple medications. Cochrane Database Syst. Rev. 2020, 5, CD012419. [Google Scholar] [CrossRef] [PubMed]
- Jimmy, B.; Jose, J. Patient Medication Adherence: Measures in Daily Practice. Oman Med. J. 2011, 26, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; De Jesus, O. Medication Routes of Administration; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Stegemann, S.; Gosch, M.; Breitkreutz, J. Swallowing dysfunction and dysphagia is an unrecognized challenge for oral drug therapy. Int. J. Pharm. 2012, 430, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Dysphagia (Swallowing Problems). Available online: https://www.nhsinform.scot/illnesses-and-conditions/stomach-liver-and-gastrointestinal-tract/dysphagia-swallowing-problems (accessed on 8 October 2023).
- Christmas, C.; Rogus-Pulia, N. Swallowing disorders in the older population. J. Am. Geriatr. Soc. 2019, 67, 2643–2649. [Google Scholar] [CrossRef]
- Nissen, L.M.; Haywood, A.; Steadman, K.J. Solid medication dosage form modification at the bedside and in the pharmacy of Queensland hospitals. J. Pharm. Pract. Res. 2009, 39, 129–134. [Google Scholar] [CrossRef]
- Wright, D. Medication administration in nursing homes. Nurs. Stand. 2002, 16, 33–38. [Google Scholar] [CrossRef]
- Pharmaceuticalissuesdosageforms-(2).pdf. Available online: https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Support/toolkit/pharmaceuticalissuesdosageforms-%282%29.pdf (accessed on 8 October 2023).
- Gracia-Vásquez, S.L.; González-Barranco, P.; Camacho-Mora, I.A.; González-Santiago, O.; Vázquez-Rodríguez, S.A. Medications that should not be crushed. Med. Univ. 2017, 19, 50–63. [Google Scholar] [CrossRef]
- Wright, D. Tablet crushing is a widespread practice but it is not safe and may not be legal. Pharm. J. 2002, 269, 132. [Google Scholar]
- Johannesson, J.; Hansson, P.; Bergström, C.A.S.; Paulsson, M. Manipulations and age-appropriateness of oral medications in pediatric oncology patients in Sweden: Need for personalized dosage forms. Biomed. Pharmacother. 2022, 146, 112576. [Google Scholar] [CrossRef] [PubMed]
- Richey, R.H.; Hughes, C.; Craig, J.V.; Shah, U.U.; Ford, J.L.; Barker, C.E.; Peak, M.; Nunn, A.J.; Turner, M.A. A systematic review of the use of dosage form manipulation to obtain required doses to inform use of manipulation in paediatric practice. Int. J. Pharm. 2017, 518, 155–166. [Google Scholar] [CrossRef]
- Richey, R.H.; Craig, J.V.; Shah, U.U.; Nunn, A.J.; Turner, M.A.; Barker, C.E.; Ford, J.L.; Peak, M. MODRIC—Manipulation of drugs in children. Int. J. Pharm. 2013, 457, 339–341. [Google Scholar] [CrossRef] [PubMed]
- CASPU Critical Appraisal Skills Programme (CASP) checklist for cohort studies. 2016.
- Akers, J.; Aguiar-Ibáñez, R.; Baba-Akbari, A. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2009. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Prod. ESRC Methods Programme Version 2006, 1, b92. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Hróbjartsson, A.; Lalu, M.M.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Belissa, E.; Vallet, T.; Laribe-Caget, S.; Chevallier, A.; Chedhomme, F.X.; Abdallah, F.; Bachalat, N.; Belbachir, S.-A.; Boulaich, I.; Bloch, V.; et al. Acceptability of oral liquid pharmaceutical products in older adults: Palatability and swallowability issues. BMC Geriatr. 2019, 19, 344. [Google Scholar] [CrossRef] [PubMed]
- Bourdenet, G.; Giraud, S.; Artur, M.; Dutertre, S.; Dufour, M.; Lefèbvre-Caussin, M.; Proux, A.; Philippe, S.; Capet, C.; Fontaine-Adam, M.; et al. Impact of recommendations on crushing medications in geriatrics: From prescription to administration. Fundam. Clin. Pharmacol. 2015, 29, 316–320. [Google Scholar] [CrossRef]
- Fodil, M.; Nghiem, D.; Colas, M.; Bourry, S.; Poisson-Salomon, A.S.; Rezigue, H.; Trivalle, C. Assessment of clinical practices for crushing medication in geriatric units. J. Nutr. Health Aging 2017, 21, 904–908. [Google Scholar] [CrossRef]
- Kelly, J.; Wright, D.; Wood, J. Medicine administration errors in patients with dysphagia in secondary care: A multi-centre observational study. J. Adv. Nurs. 2011, 67, 2615–2627. [Google Scholar] [CrossRef]
- Santos, J.M.S.; Poland, F.; Wright, D.; Longmore, T. Medicines administration for residents with dysphagia in care homes: A small scale observational study to improve practice. Int. J. Pharm. 2016, 512, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Kirkevold, Ø.; Engedal, K. What is the matter with crushing pills and opening capsules? Int. J. Nurs. Pract. 2010, 16, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Solberg, H.; Devik, S.A.; Bell, H.T.; Zeiss, D.H.; Olsen, R.M. Drug modification by nurses in Norwegian nursing homes: A cross-sectional study. Geriatr. Nur. 2021, 42, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Stuijt, C.C.; Klopotowska, J.E.; van Driel, C.K.; Le, N.; Binnekade, J.; van der Kleij, B.; van der Schors, T.; van den Bemt, P.; Lie-A-Huen, L. Improving medication administration in nursing home residents with swallowing difficulties: Sustainability of the effect of a multifaceted medication safety programme. Pharmacoepidemiol. Drug Saf. 2013, 22, 423–429. [Google Scholar] [CrossRef]
- van Welie, S.; Wijma, L.; Beerden, T.; van Doormaal, J.; Taxis, K. Effect of warning symbols in combination with education on the frequency of erroneously crushing medication in nursing homes: An uncontrolled before and after study. BMJ Open 2016, 6, e012286. [Google Scholar] [CrossRef]
- Apolo Carvajal, F.; González Martínez, M.; Capilla Santamaría, E.; Cáliz Hernández, B.; Cañamares Orbis, I.; Martínez Casanova, N.; Martínez Sánchez, E.; Aranguren Oyarzábal, A.; Calvo Alcántara, M.J.; Cruz Martos, E. Adaptation of oral medication in people institutionalized in nursing homes for whom medication is crushed: The ADECUA Study. Farm Hosp. 2016, 40, 514–528. [Google Scholar] [CrossRef] [PubMed]
- Mercovich, N.; Kyle, G.J.; Naunton, M. Safe to crush? A pilot study into solid dosage form modification in aged care. Australas. J. Ageing 2014, 33, 180–184. [Google Scholar] [CrossRef]
- Sestili, M.; Logrippo, S.; Cespi, M.; Bonacucina, G.; Ferrara, L.; Busco, S.; Grappasonni, I.; Palmieri, G.F.; Ganzetti, R.; Blasi, P. Potentially inappropriate prescribing of oral solid medications in elderly dysphagic patients. Pharmaceutics 2018, 10, 280. [Google Scholar] [CrossRef]
- White, R.; Bradnam, V. Handbook of Drug Administration via Enteral Feeding Tubes; Pharmaceutical Press: London, UK, 2015. [Google Scholar]
- Mc Gillicuddy, A.; Crean, A.M.; Sahm, L.J. Older adults with difficulty swallowing oral medicines: A systematic review of the literature. Eur. J. Clin. Pharmacol. 2016, 72, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Krishnaswami, S.; Steger, E.; Conover, E.; Vaezi, M.; Ciucci, M.; Francis, D.O. Economic and survival burden of dysphagia among inpatients in the United States. Dis. Esophagus 2018, 31, dox131. [Google Scholar] [CrossRef]
- Volkert, D.; Saeglitz, C.; Gueldenzoph, H.; Sieber, C.C.; Stehle, P. Undiagnosed malnutrition and nutrition-related problems in geriatric patients. J. Nutr. Health Aging 2010, 14, 387–392. [Google Scholar] [CrossRef] [PubMed]
- GOV.UK. Guidance for ‘Specials’ Manufacturers. Available online: https://www.gov.uk/government/publications/guidance-for-specials-manufacturers/guidance-for-specials-manufacturers (accessed on 1 October 2023).
- NEWT Guidelines—Patients with Swallowing Difficulties. Available online: https://www.newtguidelines.com/SwallowingDifficulties.html (accessed on 8 October 2023).
- Medications. Available online: https://www.bapen.org.uk/nutrition-support/enteral-nutrition/medications (accessed on 8 October 2023).
- Tan, P.L.; Chung, W.L.; Sklar, G.E.; Yap, K.Z.; Chan, S.Y. Development and validation of the INappropriate solid oral dosaGE form modification aSsessmenT (INGEST) Algorithm using data of patients with medication dysphagia from a neurology ward and nursing home in Singapore. BMJ Open 2022, 12, e061774. [Google Scholar] [CrossRef] [PubMed]
- NIOSH. NIOSH List of Antineoplastic and Other Hazardous Drugs in Healthcare Settings; Connor, T.H., MacKenzie, B.A., DeBord, D.G., Trout, D.B., O’Callaghan, J.P., Cincinnati, O.H., Eds.; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH): Washington, DC, USA, 2016. [Google Scholar]
- Schier, J.G.; Howland, M.A.; Hoffman, R.S.; Nelson, L.S. Fatality from administration of labetalol and crushed extended-release nifedipine. Ann. Pharmacother. 2003, 37, 1420–1423. [Google Scholar] [CrossRef]
- Simpson, S.H.; Eurich, D.T.; Majumdar, S.R.; Padwal, R.S.; Tsuyuki, R.T.; Varney, J.; Johnson, J.A. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 2006, 333, 15. [Google Scholar] [CrossRef]
- Strachan, I.; Greener, M. Medication-related swallowing difficulties may be more common than we realise. Pharm. Pract. 2005, 15, 411–414. [Google Scholar]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies where the results of the original research are presented. | Studies that solely involved community-dwelling patients. |
| Studies published in the English language. Studies investigating the oral administration of medicines to inpatients in a variety of healthcare settings, such as (1) hospitals, (2) nursing homes and (3) long-term stay units (LTSUs). Studies including patients over 18 years with swallowing difficulties. Studies in which the outcome included information on all or any of the following: (i) the prevalence of swallowing difficulties, (ii) the medication administration practices used to administer oral medicines to these patients and, where reported, (iii) the prevalence, type, classification, and severity of medication errors associated with SODF manipulation. | Studies that focused solely on medication modification for administration via an enteral feeding tube. Studies in which the medication modification was performed solely to enable covert the administration of medications. Surveys collecting data from healthcare professionals on their medicine administration practices when manipulating medicines for administration. Qualitative studies, systematic reviews, meta-analyses, conference abstracts, editorials, and commentaries. |
| Author; Year; Number of Participants | Study Design | Participants Included |
|---|---|---|
| Belissa et al., 2019 [24]; n = 340 patients. | Multicentre, prospective, cross sectional, non-interventional observational study. | Patients ≥ 65 years, Hospitalised in any of eight French hospitals or residing in any of eight French nursing homes. |
| Belissa 2019 [24] | Bourdenet 2015 [25] | Carvajal 2016 [33] | Fodil 2016 [26] | Kelly 2011 [27] | Kirkevold 2010 [29] | Mercovich 2013 [34] | Santos 2016 [28] | Sestili 2018 [35] | Solberg 2021 [30] | Struijt 2012 [31] | Van Welie 2016 [32] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Did the study address a clearly focused issue? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Was the cohort recruited in an acceptable way? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Was the exposure accurately measured to minimise bias? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Was the outcome accurately measured to minimise bias? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Have the authors identified all important confounding factors? | ✔ | ± | ✔ | ± | ✔ | ± | ✔ | ± | ✔ | ✔ | ✔ | ✔ |
| Have they taken account of the confounding factors in the design and/or analysis? | ✔ | ± | ✔ | ± | ✔ | ± | ✔ | ± | ✔ | ✔ | ✔ | ✔ |
| Was the follow-up of subjects complete enough? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Was the follow-up of subjects long enough? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| What are the results of this study? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| How precise are the results? | N/A | N/A | N/A | N/A | ✔ | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Do you believe the results? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Can the results be applied to the local population? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ± | ✔ | ✔ | ✔ |
| Do the results of the study fit with other available evidence? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| What are the implications of this study to practice? | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harnett, A.; Byrne, S.; O’Connor, J.; Lyons, D.; Sahm, L.J. Adult Patients with Difficulty Swallowing Oral Dosage Forms: A Systematic Review of the Quantitative Literature. Pharmacy 2023, 11, 167. https://doi.org/10.3390/pharmacy11050167
Harnett A, Byrne S, O’Connor J, Lyons D, Sahm LJ. Adult Patients with Difficulty Swallowing Oral Dosage Forms: A Systematic Review of the Quantitative Literature. Pharmacy. 2023; 11(5):167. https://doi.org/10.3390/pharmacy11050167
Chicago/Turabian StyleHarnett, Anne, Stephen Byrne, Jennifer O’Connor, Declan Lyons, and Laura J. Sahm. 2023. "Adult Patients with Difficulty Swallowing Oral Dosage Forms: A Systematic Review of the Quantitative Literature" Pharmacy 11, no. 5: 167. https://doi.org/10.3390/pharmacy11050167