
Community Pharmacies in the Asian Countries of Developing Health System: Formation, Regulation, and Implication
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Inclusion Criteria
- Published in the English language;
- Randomized controlled trials RCTs; both experimental and non-experimental studies; non-rcts, non-randomized (quasi-experimental) studies; observational, retrospective, and prospective cohort studies; and analytical and cross-sectional studies;
- Published in peer-reviewed journals, books, and professional websites of authority.
2.2. Exclusion Criteria
- Low levels of evidence, such as case reports, study protocols, commentaries, or blogs and speeches;
- Old laws abolished by new ones (if any).
3. Results
3.1. Formation of CPs
3.1.1. China
3.1.2. India
3.1.3. Indonesia
3.1.4. Iraq
3.1.5. Jordan
3.1.6. Malaysia
3.1.7. Nepal
3.1.8. Pakistan
3.1.9. Palestine
3.1.10. Qatar
3.1.11. Saudi Arabia
3.1.12. Sri Lanka
3.1.13. Thailand
3.1.14. Yemen
3.2. Challenges Associated with CPs’Services
3.2.1. Prescriptions Filling
3.2.2. Taking Patients’ History
3.2.3. Refer for Doctor Checkup
3.2.4. Drug Selling
3.2.5. Provision of Medication Advice
3.3. Determinants of Deprived Pharmacy Practices
3.3.1. Knowledge of Staff
3.3.2. Profit-Oriented Service
3.3.3. Regulatory Intervention
4. Conclusions
5. Limitations
- This study represents the snapshot of selected countries that cannot be generalized to other countries that are not represented in this review;
- This paper is an opinion according to its nature;however, different methodologiesor article types may change the results and representation;
- Todate, the data from many countries are insufficient and cause a hindrance in the presentation of a complete picture of practices in a country.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsuyuki, R.T.; Beahm, N.P.; Okada, H.; Al Hamarneh, Y.N. Pharmacists as accessible primary health care providers: Review of the evidence. Can. Pharm. J. 2018, 151, 4–5. [Google Scholar] [CrossRef] [Green Version]
- Roberts, A.S.; Benrimoj, S.I.; Chen, T.F.; Williams, K.; Aslani, P. Implementing cognitive services in community pharmacy: A review of facilitators used in practice change. Int. J. Pharm. Pract. 2006, 14, 163–170. [Google Scholar] [CrossRef]
- Moullin, J.C.; Sabater-Hernández, D.; Fernandez-Llimos, F.; Benrimoj, S.I. Defining professional pharmacy services in community pharmacy. Res. Soc. Adm. Pharm. 2013, 9, 989–995. [Google Scholar] [CrossRef]
- Anderson, C.; Sharma, R. Primary health care policy and vision for community pharmacy and pharmacists in England. Pharm. Pract. 2020, 18, 1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gastelurrutia, M.A.; Faus, M.J.; Martínez-Martínez, F. Primary health care policy and vision for community pharmacy and pharmacists in Spain. Pharm. Pract. 2020, 18, 1999. [Google Scholar] [CrossRef] [PubMed]
- Dineen-Griffin, S.; Benrimoj, S.I.; Garcia-Cardenas, V. Primary health care policy and vision for community pharmacy and pharmacists in Australia. Pharm. Pract. 2020, 18, 1967. [Google Scholar] [CrossRef]
- Raiche, T.; Pammett, R.; Dattani, S.; Dolovich, L.; Hamilton, K.; Kennie-Kaulbach, N.; McCarthy, L.; Jorgenson, D. Community pharmacists’ evolving role in Canadian primary health care: A vision of harmonization in a patchwork system. Pharm. Pract. 2020, 18, 2171. [Google Scholar] [CrossRef]
- Hansen, R.N.; Nørgaard, L.S.; Hedegaard, U.; Søndergaard, L.; Servilieri, K.; Bendixen, S.; Rossing, C. Integration of and visions for community pharmacy in primary health care in Denmark. Pharm. Pract. 2021, 19, 2212. [Google Scholar] [CrossRef]
- George, P.P.; Molina, J.A.; Cheah, J.; Chan, S.C.; Lim, B. The evolving role of the community pharmacist in chronic disease management-a literature review. Ann. Acad. Med. Singap. 2010, 39, 861–867. [Google Scholar] [CrossRef]
- Latif, A. Community pharmacy medicines use review: Current challenges. Integr. Pharm. Res. Pract. 2018, 7, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Dhital, R.; Sakulwach, S.; Robert, G.; Vasilikou, C.; Sin, J. Systematic review on the effects of the physical and social aspects of community pharmacy spaces on service users and staff. Perspect. Public Health 2022, 142, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Azhar, S.; Hassali, M.A.; Ibrahim, M.I.M.; Ahmad, M.; Masood, I.; Shafie, A. The role of pharmacists in developing countries: The current scenario in Pakistan. Hum. Resour. Health 2009, 7, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, M.M.; Fang, Y. Pakistan should immediately curb the sale of non-prescribed antibiotics from community pharmacies. Int. J. Health Plan. Manag. 2019, 34, e1376–e1377. [Google Scholar] [CrossRef] [PubMed]
- Assab, M.A.; Alhamad, H.; Almazari, I.; Azzam, B.; Abu Assab, H. Barriers to medication review process implementation—Cross-sectional study among community pharmacists in Jordan. Healthcare 2022, 10, 651. [Google Scholar] [CrossRef]
- Chang, J.; Lv, B.; Zhu, S.; Yu, J.; Zhang, Y.; Ye, D.; Aziz, M.M.; Yang, C.; Fang, Y. Non-prescription use of antibiotics among children in urban China: A cross-sectional survey of knowledge, attitudes, and practices. Expert Rev. Anti. Infect. Ther. 2018, 16, 163–172. [Google Scholar] [CrossRef]
- Erku, D.A.; Belachew, S.A.; Mekuria, A.B. The role of community pharmacists in patient counseling and health education: A survey of their knowledge and level of involvement in relation to type 2 diabetes mellitus. Integr. Pharm. Res. Pract. 2017, 6, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Alo, A. Pharmacy in Nigeria. Am. J. Heal. Pharm. 2006, 63, 670–673. [Google Scholar] [CrossRef]
- Ye, D.; Jie, C.; Yang, C.; Yan, K.; Ji, W.; Aziz, M.M.; Gillani, A.H.; Fang, Y. How does the general public view antibiotic use in china? Result from multicenter cross sectional survey. Int. J. Clin. Pharm. 2016, 39, 927–934. [Google Scholar] [CrossRef]
- Olsson, E.; Tuyet, L.T.; Nguyen, H.A. Health professionals’ and consumers’ views on the role of the pharmacy personnel and the pharmacy service in Hanoi, Vietnam--a qualitative study. J. Clin. Pharm. Ther. 2002, 27, 273–280. [Google Scholar] [CrossRef]
- Khan, M.M.H.; Grbner, O.; Krämer, A. Frequently used healthcare services in urban slums of Dhaka and adjacent rural areas and their determinants. J. Public Health 2012, 34, 261–271. [Google Scholar] [CrossRef] [Green Version]
- National Medical Products Administration. Available online: http://english.nmpa.gov.cn/ (accessed on 17 May 2023).
- Yu, F. Pharmacy Practice in China; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000046 (accessed on 17 May 2023).
- Drug Administration Law of the People’s Republic of China. Available online: http://www.npc.gov.cn/englishnpc/c23934/202012/3c19c24f9ca04d1ba0678c6f8f8a4a8a.shtml (accessed on 17 May 2023).
- Regulation for the Supervision and Administration of Medical Devices. Available online: http://www.sfdachina.com/info/69-1.htm (accessed on 17 May 2023).
- Chang, J.; Ye, D.; Lv, B.; Jiang, M.; Zhu, S.; Yan, K.; Tian, Y.; Fang, Y. Sale of antibiotics without a prescription at community pharmacies in urban China. A multicentre cross-sectional survey. J. Antimicrob.Chemother. 2017, 72, 1235–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deere, D. Regulatory reform in China creates opportunities. Pharm. Technol. 2016, 2, 14–23. [Google Scholar]
- Basak, S.C.; Sathyanarayana, D. Community pharmacy practice in India: Past, present and future. South. Med. Rev. 2009, 2, 11–14. [Google Scholar] [PubMed]
- Karim, S.; Adnan, M. Pharmacy Practice in India; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000071 (accessed on 17 May 2023).
- Sachan, A.; Sachan, A.K.; Gangwar, S.S. Pharmacy education in India and its neighbouringcountries. Int.Curr. Pharm. J. 2012, 1, 294–301. [Google Scholar] [CrossRef] [Green Version]
- Andayani, T.M.; Satibi, S. Pharmacy Practice in Indonesia; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000034 (accessed on 17 May 2023).
- Hermansyah, A.; Sainsbury, E.; Krass, I. Multiple policy approaches in improving community pharmacy practice: The case in Indonesia. BMC Health Serv. Res. 2018, 18, 449. [Google Scholar] [CrossRef]
- Ibrahim, R.I.; Wayyes, A.R. Pharmacy Practice in Iraq; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000101 (accessed on 17 May 2023).
- Ibrahim, I.R.; Tukmagi, H.F.; Al Wayyes, A. Attitudes of Iraqi society towards the role of community pharmacist. Innov. Pharm. 2013, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kheir, N.; Zaidan, M.; Younes, H.; El Hajj, M.; Wilbur, K.; Jewesson, P.J. Pharmacy education and practice in 13 middle eastern countries. Am. J. Pharm. Educ. 2008, 72, 133. [Google Scholar] [CrossRef] [Green Version]
- Nazer, L.H.; Tuffaha, H. Health Care and Pharmacy Practice in Jordan. Can. J. Hosp. Pharm. 2017, 70, 150–155. [Google Scholar] [CrossRef]
- Al-Wazaify, M.; Albsoul-Younes, A. Pharmacy in Jordan. Am. J. Health Pharm. 2005, 62, 2548–2551. [Google Scholar] [CrossRef]
- Al-Abbadi, I.; Qawwas, A.; Jaafreh, M.; Abosamen, T.; Saket, M. One-year assessment of joint procurement of pharmaceuticals in the public health sector in Jordan. Clin. Ther. 2009, 31, 1335–1344. [Google Scholar] [CrossRef]
- Shilbayeh, S.A. Exploring knowledge and attitudes towards counselling about vitamin supplements in Jordanian community pharmacies. Pharm. Pract. 2011, 9, 242–251. [Google Scholar] [CrossRef] [Green Version]
- Hassali, M.A.A.; Shafie, A.A.; See, O.G.; Wong, Z.Y. Pharmacy Practice in Malaysia; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000022 (accessed on 17 May 2023).
- Pharmaceutical Services Division. Ministry of Health MalaysiaCommunity. Pharmacy Benchmarking Guideline 2011. Available online: https://www.pharmacy.gov.my/v2/en/documents/community-pharmacy-benchmarking-guideline.html (accessed on 17 May 2023).
- Prasad, R.R. Number of registered pharmacy outlets till June 2012. Drug Bull. Nepal. 2012, 24, 7–9. [Google Scholar]
- Ranjit, E. Pharmacy Practice in Nepal. Can. J. Hosp. Pharm. 2016, 69, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Ansari, M. Evaluation of the most commonly dispensed antibiotics among the pharmacies located in and around national medical college teaching hospital, Birgunj, Nepal. Indian J. Pharm. Pract. 2013, 6, 62–64. [Google Scholar]
- Ansari, M. Evaluation of community pharmacies regarding dispensing practices of antibiotics in two districts of central Nepal. PLoS ONE 2017, 12, e0183907. [Google Scholar] [CrossRef] [Green Version]
- Ansari, M.; Alam, K. Pharmacy Practice in Nepal; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000083 (accessed on 17 May 2023).
- Aziz, M.M.; Yang, S.; Masood, I.; Zhu, S.; Raza, M.A.; Ji, W.; Anwar, N.; Saeed, A.; Fang, Y. An assessment of counseling quality provided by community pharmacies to type 2 diabetic adult patients for oral therapy: A simulated patient study from Pakistan. Endocr. J. 2019, 66, 233–239. [Google Scholar] [CrossRef]
- Hussain, A.; Ibrahim, M.I. Medication counselling and dispensing practices at community pharmacies: A comparative cross sectional study from Pakistan. Int. J. Clin. Pharm. 2011, 33, 859–867. [Google Scholar] [CrossRef]
- Majid Aziz, M.; Haider, F.; Rasool, M.F.; Hashmi, F.K.; Bahsir, S.; Li, P.; Zhao, M.; Alshammary, T.M.; Fang, Y. Dispensing of Non-Prescribed Antibiotics from Community Pharmacies of Pakistan: A Cross-Sectional Survey of Pharmacy Staff’s Opinion. Antibiotics 2021, 10, 482. [Google Scholar] [CrossRef]
- Hussain, A.; Ibrahim, M.I.M.; Baber, Z.D. Compliance with legal requirements at community pharmacies: A cross sectional study from Pakistan. Int. J. Pharm. Pract. 2011, 20, 183–190. [Google Scholar] [CrossRef]
- Aziz, M.M.; Jiang, M.; Masood, I.; Chang, J.; Shan, Z.; Raza, M.A.; Ji, W.; Yang, C.; Fang, Y. Patients’ anticipation for the pharmacies of rural communities: A qualitative study from Pakistan. Int. J. Environ. Res. Public Health 2019, 16, 143. [Google Scholar] [CrossRef] [Green Version]
- Aslam, F.; Aziz, M.M.; Yang, Y.; Babar, Z.U.D. How the medicine inventory is managed by pharmacy retailers: A cross sectional study from Punjab, Pakistan. Value Health 2020, 23, S315. [Google Scholar]
- Aziz, M.M.; Masood, I.; Yousaf, M.; Saleem, H.; Ye, D.; Fang, Y. Pattern of medication selling and self-medication practices: A study from Punjab, Pakistan. PLoS ONE 2018, 13, e0194240. [Google Scholar] [CrossRef] [Green Version]
- Aziz, M.M.; Ji, W.; Masood, I.; Farooq, M.; Malik, M.Z.; Chang, J.; Jiang, M.; Atif, N.; Fang, Y. Patient satisfaction with communitypharmacies services: A cross-sectional survey from Punjab; Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 2914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, M.M.; Wajid, M.; Fang, Y. A societal perception about community pharmacies in Pakistan: An outline of prospective investigation. Res. Social Adm. Pharm. 2017, 13, e7. [Google Scholar] [CrossRef]
- Waleed, M.; Sweileh, S.H.; Zyoud, M.S.A.H. Pharmacy Practice in Palestine; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://staff.najah.edu/media/scientificresearch/books/2016/05/19/3-s2.0-B9780128017142000137-main.pdf (accessed on 17 May 2023).
- Zaid, A.N.; Al-Ramahi, R.; Shahed, Q.; Saleh, B.; Elaraj, J. Determinants and frequency of pharmaceutical compounding in pharmacy practice in Palestine. Int. J. Pharm. Pract. 2012, 20, 9–14. [Google Scholar] [CrossRef]
- Sawalha, A.; Sweileh, W.; Zyoud, S.; Al Jabi, S.; Shamseh, F.B.; Odah, A. Analysis of prescriptions dispensed at community pharmacies in Nablus, Palestine. East. Mediterr. Health J. 2010, 17, 788–792. [Google Scholar] [CrossRef]
- Sweileh, W. Self–medication and over-the-counter practices: A study in Palestine. W. Sweileh. J. Al-Aqsa Unv. 2004, 8, 1–9. [Google Scholar]
- Al-Ramahi, R. Patterns and attitudes of self-medication practices and possible role of community pharmacists in Palestine. Int. J. Clin. Pharmacol. Ther. 2013, 51, 562–567. [Google Scholar] [CrossRef]
- Kheir, N. Pharmacy Practice in Qatar; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000125 (accessed on 17 May 2023).
- Kheir, N.F.M. Pharmacy practice in Qatar: Challenges and opportunities. South. Med. Rev. 2011, 4, 45–49. [Google Scholar] [CrossRef]
- Elkassem, W.; Pallivalapila, A.; Al Hail, M.; McHattie, L.; Diack, L.; Stewart, D. Advancing the pharmacy practice research agenda: Views and experiences of pharmacists in Qatar. Int. J. Clin. Pharm. 2013, 35, 692–696. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A.; Almanasef, M.; Asiri, A. A cross-sectional study on pharmacy students’ career choices in the light of Saudi vision 2030: Will community pharmacy continue to be the most promising, but least preferred, sector? Int. J. Environ. Res. Public Health Artic. 2021, 18, 4589. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A.; Asiri, R.; Albugami, N. Pharmacy workforce in Saudi Arabia: Challenges and opportunities: A cross-sectional study. Int. J. Health Plan. Manag. 2018, 34, e583–e593. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, M.K.; Alqasoumi, A.; Hasan, S.S.; Babar, Z. The community pharmacy practice change towards patient-centered care in Saudi Arabia: A qualitative perspective. J. Pharm. Policy Pract. 2020, 13, 59–61. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A. Using a global systematic framework tool to identify pharmacy workforce development needs: A national case study on Saudi Arabia. Risk Manag. HealthPolicy 2021, 14, 3233–3245. [Google Scholar] [CrossRef]
- Almohammed, O.A.; Alsanea, S. Public perception and attitude toward community pharmacists in Saudi Arabia. Saudi J. Health Syst. Res. 2021, 1, 67–74. [Google Scholar] [CrossRef]
- Al-Jedai, A.; Qaisi, S.; Al-Meman, A. Pharmacy practice and the health care system in Saudi Arabia. Can. J. Hosp. Pharm. 2016, 69, 231–237. [Google Scholar] [CrossRef]
- Alsheikh, M.Y.; Alasmari, M.M. A national survey of community pharmacists’ viewpoints about pharmacovigilance and adverse drug reaction reporting in Saudi Arabia. Front. Pharmacol. 2022, 26, 819551. [Google Scholar] [CrossRef]
- Riyadh (Saudi Arabia): Ministry of Health. Statistical Year Book Kingdom of Saudi Arabia 2014 G/1435 H. 2014. Available online: www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Book-for-the-Year-1435.pdf (accessed on 12 April 2023).
- Colombo. Sri Lanka Chamber of the Pharmaceutical Industry. Available online: http://www.slcpi.org/ (accessed on 12 May 2023).
- Reginoald-Prasad, C. Pharmacy Retail in Sri Lanka Compared to Norway; Umeå University: Umeå, Sweden, 2014. [Google Scholar]
- Chaiyakunapruk, N.; Jones, S.M.; Dhippayom, T.; Sumpradit, N. Pharmacy Practice in Thailand; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000010 (accessed on 12 April 2023).
- Khumsikiew, J.; Arkaravichien, W.; Honsamoot, D.S.P. Diabetes and hypertension screening by accredited community pharmacy in KhonKaen under a pilot project with the national health security scheme. Srinagarind. Med. J. 2009, 24, 215–223. [Google Scholar]
- Chaiyakunapruk, N.; Laowakul, A.; Pikulthong, N. Implementation and evaluation of osteoporosis screening services in community pharmacy, using the osteoporosis self-assessment tool for Asians (OSTA). J. Am. Pharm. Assoc. 2006, 46, 391–396. [Google Scholar] [CrossRef]
- Dhippayom, T.; Fuangchan, A.; Tunpichart, S.; Chaiyakunapruk, N. Opportunistic screening and health promotion for type 2 diabetes: An expanding public health role for the community pharmacist. J. Public Health 2013, 35, 262–269. [Google Scholar] [CrossRef] [Green Version]
- Tunpichart, S.; Sakulbumrungsil, R.; Somrongthong, R.H.D. Chronic care model for diabetics by pharmacist home health in Bangkok Metropolitan: A community based study. Int. J. Med. Sci. 2012, 4, 90–96. [Google Scholar] [CrossRef]
- Chalongsuk, R.L.S. Client satisfaction in pharmacy under the Thai universal coverage scheme: A case study at the community pharmacy of Sawang Dan Din crown prince hospital. Thai J. Health Res. 2006, 20, 41–57. [Google Scholar]
- Chalongsuk, R.; Lochid-amnuay, S.S.W. A study of a refill prescription service system comparing a hospital pharmacy and an acrredited pharmacy. J. Heal. Syst. Res. 2007, 1, 249–261. [Google Scholar]
- Nimpitakpong, P.; Chaiyakunapruk, N.D.T. Smoking cessation education in Thai schools of pharmacy. Pharm. Educ. 2011, 11, 8–11. [Google Scholar]
- Thananithisak, C.; Nimpitakpong, P.C.N. Providing, Activities and perceptions of pharmacists Thailand., tobacco control services in community pharmacy. Nicotine. Tob. Res. 2008, 10, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Nimpitakpong, P.; Chaiyakunapruk, N.D.T. A national survey of training and smoking cessation services provided in community pharmacies in Thailand. J.Community Health 2010, 35, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Al-Worafi, Y.M.A. Pharmacy Practice in Yemen; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000149 (accessed on 12 April 2023).
- Al-Worafi, Y.M. Pharmacy practice and its challenges in Yemen. Australas. Med. J. 2014, 7, 17–23. [Google Scholar] [CrossRef]
- Al-Worafi, Y.M. Appropriateness of metered-dose inhaler use in the Yemeni community pharmacies. J. Taibah Univ. Med. Sci. 2015, 10, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.; Goodman, C. Performance of retail pharmacies in low- and middle-income Asian settings: A systematic review. Health Policy Plan. 2016, 31, 940–953. [Google Scholar] [CrossRef] [Green Version]
- Greenhalgh, T. Drug prescription and self-medication in India: An exploratory survey. Soc. Sci. Med. 1987, 25, 307–318. [Google Scholar] [CrossRef]
- Kamat, V.R.; Nichter, M. Pharmacies, self-medication and pharmaceutical marketing in Bombay, India. Soc. Sci. Med. 1998, 47, 779–794. [Google Scholar] [CrossRef]
- Basak, S.C.; Sathyanarayana, D. Evaluating medicines dispensing patterns at private community pharmacies in Tamil Nadu, India. South. Med. Rev. 2010, 3, 27–31. [Google Scholar]
- Puspitasari, H.P.; Faturrohmah, A.H.A. Do Indonesian community pharmacy workers respond to antibiotics requests appropriately? Trop. Med. Int. Health 2011, 16, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Roy, J. Health status, treatment and drug use in rural Bangladesh: A case study of a village. Aust. J. Rural. Health 1997, 5, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Ross-Degnan, D.; Soumerai, S.B.; Goel, P.K.; Bates, J.; Makhulo, J.; Dondi, N.; Sutoto; Adi, D.; Ferraz-Tabor, L.; Hogan, R. The impact of face-to-face educational outreach on diarrhoea treatment in pharmacies. Health Policy Plan. 1996, 11, 308–318. [Google Scholar] [CrossRef] [Green Version]
- Chuc, N.T.; Larsson, M.; Falkenberg, T. Management of childhood acute respiratory infections at private pharmacies in Vietnam. Ann.Pharmacother. 2001, 35, 1283–1288. [Google Scholar] [CrossRef]
- Bista, K.P.; Chaudhary, P.; Slanger, T.E. The practice of STI treatment among chemists and druggists in Pokhara, Nepal. Sex. Transm. Infect. 2002, 78, 223. [Google Scholar] [CrossRef] [Green Version]
- Van-Sickle, D. Management of asthma at private pharmacies in India. Int. J. Tuberc. Lung Dis. 2006, 10, 1386–1392. [Google Scholar]
- Saengcharoen, W.; Lerkiatbundit, S. Practice and attitudes regarding the management of childhood diarrhoea among pharmacies in Thailand. Int. J. Pharm. Pract. 2010, 18, 323–331. [Google Scholar] [CrossRef]
- Minh, P.D.; Huong, D.T.; Byrkit, R. Strengthening pharmacy practice in Vietnam: Findings of a training intervention stud. Trop Med. Int. Health 2013, 18, 426–434. [Google Scholar] [CrossRef]
- Wachter, D.A.; Joshi, M.P.; Rimal, B. Antibiotic dispensing by drug retailers in Kathmandu, Nepal. Trop. Med. Int. Health 1999, 4, 782–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.; Ibrahim, M.I. Management of diarrhoea cases by community pharmacies in 3 cities of Pakistan. East.Mediterr. Health J. 2012, 18, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Duong, D.V.; Van, L.T.; Binns, C.W. Diarrhoea management by pharmacy staff in retail pharmacies in Hanoi, Vietnam. Int. J. Pharm. Pract. 1997, 5, 97–100. [Google Scholar] [CrossRef]
- Chalker, J.; Chuc, N.; Falkenberg, T.; Do, N.T.; Tomson, G. STD management by private pharmacies in Hanoi: Practice and knowledge of drug sellers. Sex. Transm. Infect. 2000, 76, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Rathnakar, U.P.; Sharma, N.K.; Garg, R. A study on the sale of antimicrobial agents without prescriptions in pharmacies in an urban area in south India. J. Clin.Diagn. Res. 2012, 6, 951–954. [Google Scholar]
- Tomson, G.; Sterky, G. Self-prescribing by way of pharmacies in three Asian developing countries. Lancet 1986, 328, 620–622. [Google Scholar] [CrossRef]
- Tuladhar, S.M.; Mills, S.; Acharya, S. The role of pharmacists in HIV/STD prevention: Evaluation of an STD syndromic management intervention in Nepal. AIDS 1998, 12, 81–87. [Google Scholar]
- Apisarnthanarak, A.; Tunpornchai, J.; Tanawitt, K. Nonjudicious dispensing of antibiotics by drug stores in Pratumthani, Thailand. Infect. Control. Hosp. Epidemiol. 2008, 29, 572–575. [Google Scholar] [CrossRef]
- Vu, D.H.; van Rein, N.; Cobelens, F.G.; Nguyen, T.T.H.; Le, V.H.; Brouwers, J.R.B.J. Suspected tuberculosis case detection and referral in private pharmacies in Viet Nam. Int. J.Tuberc. Lung Dis. 2012, 16, 1625–1629. [Google Scholar] [CrossRef] [Green Version]
- Krishnaswamy, K.; Kumar, B.D.; Radhaiah, G. A drug survey—Precepts and practices. Eur. J. Clin. Pharmacol. 1985, 29, 363–370. [Google Scholar] [CrossRef]
- Wolffers, I. Drug information and sale practices in some pharmacies of Colombo, Sri Lanka. Soc. Sci. Med. 1987, 25, 319–321. [Google Scholar] [CrossRef]
- Lansang, M.A.; Lucas-Aquino, R.; Tupasi, T.E.; Mina, V.S.; Salazar, L.S.; Juban, N.; Limjoco, T.T.; Nisperos, L.E.; Kunin, C.M. Purchase of antibiotics without prescription in Manila, the Philippines. Inappropriate choices and doses. J. Clin. Epidemiol. 1990, 43, 61–67. [Google Scholar] [CrossRef]
- Dua, V.; Kunin, C.M.; White, L.V. The use of antimicrobial drugs in Nagpur, India. A window on medical care in a developing country. Soc. Sci. Med. 1994, 38, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Modal, T.; Lamba, L. Practices of chemist regarding diarrhoea management. Indian J. Pediatr. 1994, 31, 1535–1536. [Google Scholar]
- Dineshkumar, B.; Raghuram, T.C.; Radhaiah, G. Profile of drug use in urban and rural India. Pharmacoeconomics 1995, 7, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Cong, L.D.; Yen, P.T.; Nhu, T.V. Use and quality of antimalarial drugs in the private sector in Viet Nam. Bull. World Health Organ. 1998, 76, 51–58. [Google Scholar] [PubMed]
- Podhipak, A.; Varavithya, W.; Punyaratabandhu, P.; Vathanophas, K.; Sangchai, R. Impact of an educational program on the treatment practices of diarrheal diseases among pharmacists and drugsellers. Southeast Asian J. Trop. Med. Public Health 1993, 24, 32–39. [Google Scholar] [PubMed]
- Hadi, U.; Broek, P.V.D.; Kolopaking, E.P. Cross-sectional study of availability and pharmaceutical quality of antibiotics requested with or without prescription (over the counter) in Surabaya, Indonesia. BMC Infect. Dis. 2010, 10, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafle, K.; Karkee, S.; Shrestha, N.; Prasad, R.R.; Bhuju, G.B.; Das, P.L.; Shrestha, A.D.; Ross-Degnan, D. Improving private drug sellers’ practices for managing common health problems in Nepal. J. Nepal Health Res. Counc. 2013, 11, 198–204. [Google Scholar]
- Aziz, M.M.; Rasool, M.F.; Alanazi, M.; Alharby, T.N.; Alanazi, J.; Huwaimel, B. Evaluating the counseling standards and ability of pharmacy staff to detect antibiotic-drugs interactions: A simulated client study from Pakistan. Antibiotics 2023, 12, 931. [Google Scholar] [CrossRef]
- Saengcharoen, W.; Lerkiatbundit, S. Migraine management in community pharmacies: Practice patterns and knowledge of pharmacy personnel in Thailand. Headache 2013, 53, 1451–1463. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.; Alam, A.; Fournier, P. Medicine sellers for prevention and control of sexually transmitted infections: Effect of a quasi-experimental training intervention in Bangladesh. Biomed. Res. Int. 2015, 2015, 570340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qidwai, W.; Krishanani, M.; Hashmi, S. Private drug sellers’ education in improving prescribing practices. J. Coll.Physicians Surg. Pak. 2006, 16, 743–746. [Google Scholar]
- Pham, D.M.; Byrkit, M.; van Pham, H. Improving pharmacy staff knowledge and practice on childhood diarrhea management in Vietnam: Are educational interventions effective? PLoS ONE 2013, 8, 570340. [Google Scholar] [CrossRef]
- Stenson, B.; Syhakhang, L.; Eriksson, B. Real world pharmacy: Assessing the quality of private pharmacy practice in the Lao People’s Democratic Republic. Soc. Sci. Med. 2001, 52, 393–404. [Google Scholar] [CrossRef] [PubMed]
- Thamlikitkul, V. Antibiotic dispensing by drug store personnel in Bangkok, Thailand. J. Antimicrob.Chemoth. 1988, 21, 125–131. [Google Scholar] [CrossRef]
- Saradamma, R.D.; Higginbotham, N.; Nichter, M. Social factors influencing the acquisition of antibiotics without prescription in Kerala State, south India. Soc. Sci. Med. 2000, 50, 891–903. [Google Scholar] [CrossRef]
- Chuc, N.T.K.; Tomson, G. “Doi moi” and private pharmacies: A case study on dispensing and financial issues in Hanoi, Vietnam. Eur. J. Clin.Pharmacol. 1999, 55, 325–332. [Google Scholar] [CrossRef]
- Mamun, K.Z.; Tabassum, S.; Shears, P. A survey of antimicrobial prescribing and dispensing practices in rural Bangladesh. Mymensingh. Med. J. 2006, 15, 81–84. [Google Scholar] [CrossRef]
- Ratanajamit, C.; Chongsuvivatwong, V. Survey of knowledge and practice on oral contraceptive and emergency contraceptive pills of drugstore personnel in Hat Yai, Thailand. Pharmacoepidemiol. Drug Saf. 2001, 10, 149–156. [Google Scholar] [CrossRef]
- Kafle, K.K.; Madden, J.M.; Shrestha, A.D.; Karkee, S.B.; Das, P.L.; Pradhan, Y.M.; Quick, J.D. Can licensed drug sellers contribute to safe motherhood? A survey of the treatment of pregnancy-related anaemia in Nepal. Soc. Sci. Med. 1996, 42, 1577–1588. [Google Scholar] [CrossRef] [PubMed]
- Ngo, T.D.; Park, M.H.; Nguyen, T.H. Pharmacy workers’ knowledge and provision of abortifacients in Ho Chi Minh City, Vietnam. Int. J. Gynaecol. Obstet. 2012, 117, 187–188. [Google Scholar] [CrossRef]
- Butt, Z.A.; Gilani, A.H.; Nanan, D.; Sheikh, A.L.; White, F. Quality of pharmacies in Pakistan: A cross-sectional survey. Int. J. Qual. Health Care 2005, 17, 307–313. [Google Scholar] [CrossRef]
- Khan, T. Challenges to pharmacy and pharmacy practice in Pakistan. Australas. Med. J. 2011, 4, 230–235. [Google Scholar] [CrossRef]
- Hussain, A.; Ibrahim, M.I.M. Qualification, knowledge and experience of dispensers working at community pharmacies in Pakistan. Pharm. Pract. 2011, 9, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Tamang, A.; Puri, M.; Lama, K. Pharmacy workers in Nepal can provide the correct information about using mifepristone and misoprostol to women seeking medication to induce abortion. Reprod. Health Matters 2015, 22, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Maharjan, R.; Prajapati, A. Assessment of knowledge and practice of community pharmacy personnel on diabetes mellitus management in Kathmandu district: A cross sectional descriptive study. J. Diabetes. Metab.Disord. 2015, 14, 71. [Google Scholar] [CrossRef] [Green Version]
- Khalid, L.; Mahsood, N.; Ali, I. The public health problem of OTC antibiotics in developing nations. Res. Soc. Adm. Pharm. 2016, 12, 801–802. [Google Scholar] [CrossRef]
- Deshpande, P.; Vantipalli, R.; Lakshmi, C.C.; Rao, E.; Regmi, B.; Ahad, A.; Nirojini, P. Clinical pharmacists: The major support to Indian healthcare system in near future. J. Pharm. Bioallied. Sci. 2015, 7, 161–174. [Google Scholar] [CrossRef]
- Chanakit, T.; Low, B.Y.; Wongpoowarak, P.; Moolasarn, S.; Anderson, C. A survey of pharmacy education in Thailand. Am. J. Pharm. Educ. 2014, 78, 6–8. [Google Scholar] [CrossRef] [Green Version]
- Seeberg, J. Connecting pills and people: An ethnography of the pharmaceutical nexus in Odisha, India. Med. Anthropol. Q. 2012, 26, 182–200. [Google Scholar] [CrossRef]
- Chalker, J.; Ratanawijitrasin, S.; Chuc, N.; Petzold, M.; Tomson, G. Effectiveness of a multi-component intervention on dispensing practices at private pharmacies in Vietnam and Thailand—A randomized controlled trial. Soc. Sci. Med. 2005, 60, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Stenson, B.; Syhakhang, L.; Lundborg, C.S. Private pharmacy practice and regulation. A randomized trial in Lao P.D.R. Int. J. Technol. Assess Health Care 2001, 17, 579–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pezzola, A.; Sweet, C.M. Global pharmaceutical regulation: The challenge of integration for developing states. Global Health 2016, 12, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
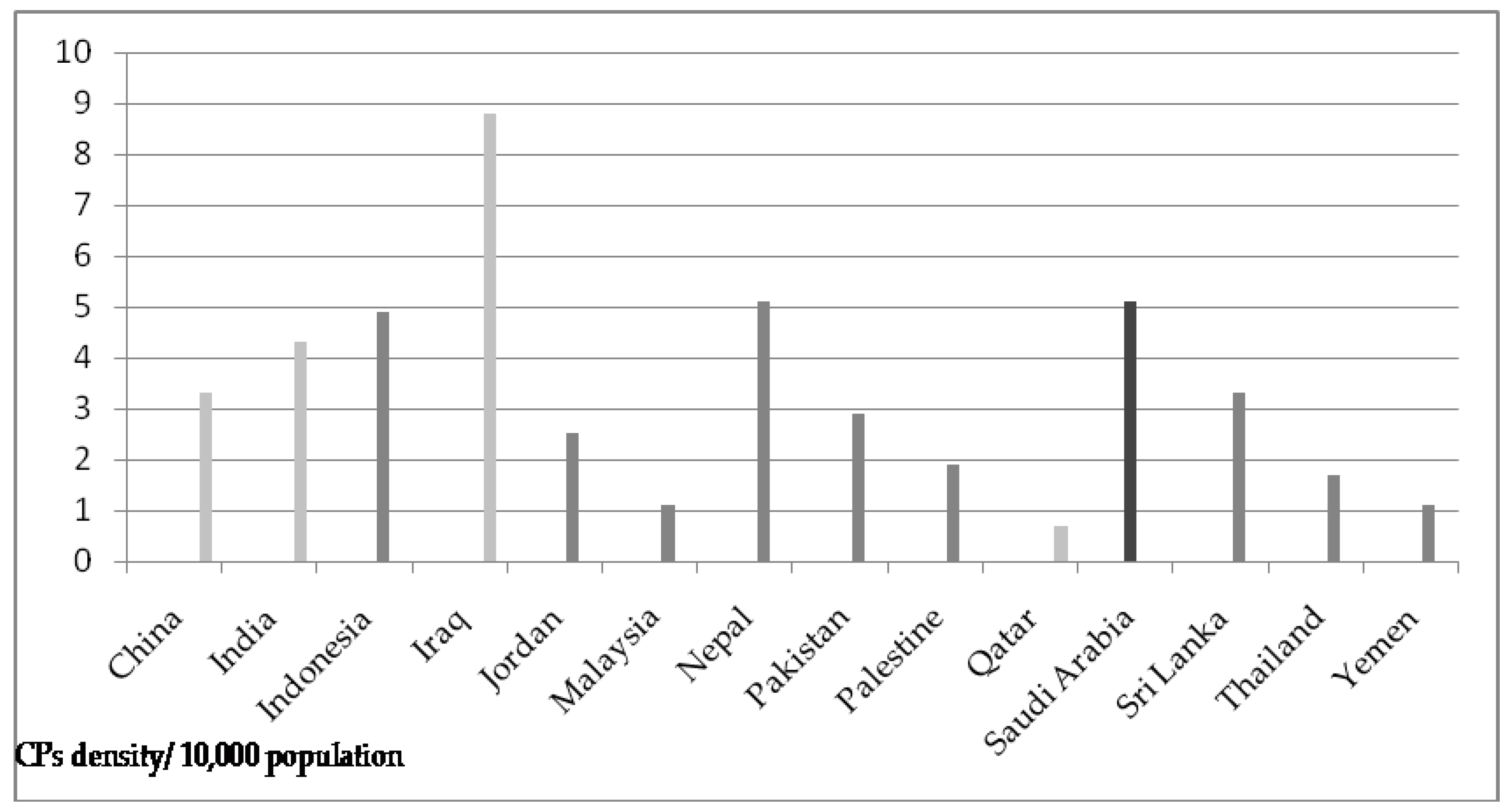
| Sr. # | Country | Number * | Density ** | Jurisdiction | PC | Traits | Challenges |
|---|---|---|---|---|---|---|---|
| 1 | China | 472,000 | 3.3 | Drug Administration Law, 2001 | Limited |
|
|
| 2 | India | 600,000 | 4.3 | Pharmacy Act, 1948taozhuozzzDrugs and Cosmetics Act and Rules, 1945 | Very limited |
|
|
| 3 | Indonesia | 135,000 | 4.9 | Section 51, Act 2009 | Limited |
|
|
| 4 | Iraq | 9000 | 8.8 | Pharmacy Act, 1923 | Good (MTM) |
|
|
| 5 | Jordan | 2500 | 2.5 | Drug and Pharmacy Law, 2001 | Moderate |
|
|
| 6 | Malaysia | 3300 | 1.1 | Poison Act of 1952 | Moderate |
|
|
| 7 | Nepal | 14,899 | 5.1 | Drug Act, 1978 | Limited |
|
|
| 8 | Pakistan | 63,000 | 2.9 | Drug Act, 1976 Pharmacy Act, 1967 | Very limited |
|
|
| 9 | Palestine | 1000 | 1.9 | Palestinian pharmacy practice law | Very limited |
|
|
| 10 | Qatar | 200 | 0.7 | Almeezan Law No. 3, 1983 | Very limited |
|
|
| 11 | Saudi Arabia | 17,815 | 5.1 | MOH, 1978 | Limited |
|
|
| 12 | Sri Lanka | 7029 | 3.3 | Drugs Act No. 27, 1980 | Limited |
|
|
| 13 | Thailand | 11,603 | 1.7 | Thai Drug Act,1967 | Limited |
|
|
| 14 | Yemen | 3315 | 1.1 | Law # 26 of 2002 | Very limited |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenezi, S.; Alanazi, M.; Aljazaeri, R.; Almuzaini, M.; Alrasheidi, S.; Shamlan, W.B.; Aljohani, R.; Alhawiti, G.; Alqarni, M.; Aljabri, E.; et al. Community Pharmacies in the Asian Countries of Developing Health System: Formation, Regulation, and Implication. Pharmacy 2023, 11, 127. https://doi.org/10.3390/pharmacy11040127
Alenezi S, Alanazi M, Aljazaeri R, Almuzaini M, Alrasheidi S, Shamlan WB, Aljohani R, Alhawiti G, Alqarni M, Aljabri E, et al. Community Pharmacies in the Asian Countries of Developing Health System: Formation, Regulation, and Implication. Pharmacy. 2023; 11(4):127. https://doi.org/10.3390/pharmacy11040127
Chicago/Turabian StyleAlenezi, Shaymaa, Mona Alanazi, Reaam Aljazaeri, Marwah Almuzaini, Shorouq Alrasheidi, Wafa Bin Shamlan, Raghad Aljohani, Ghadeer Alhawiti, Meaad Alqarni, Ehdaa Aljabri, and et al. 2023. "Community Pharmacies in the Asian Countries of Developing Health System: Formation, Regulation, and Implication" Pharmacy 11, no. 4: 127. https://doi.org/10.3390/pharmacy11040127