

Counselling for Chronic Insomnia in Swiss Pharmacies: A Survey Study Based on Case Vignettes
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
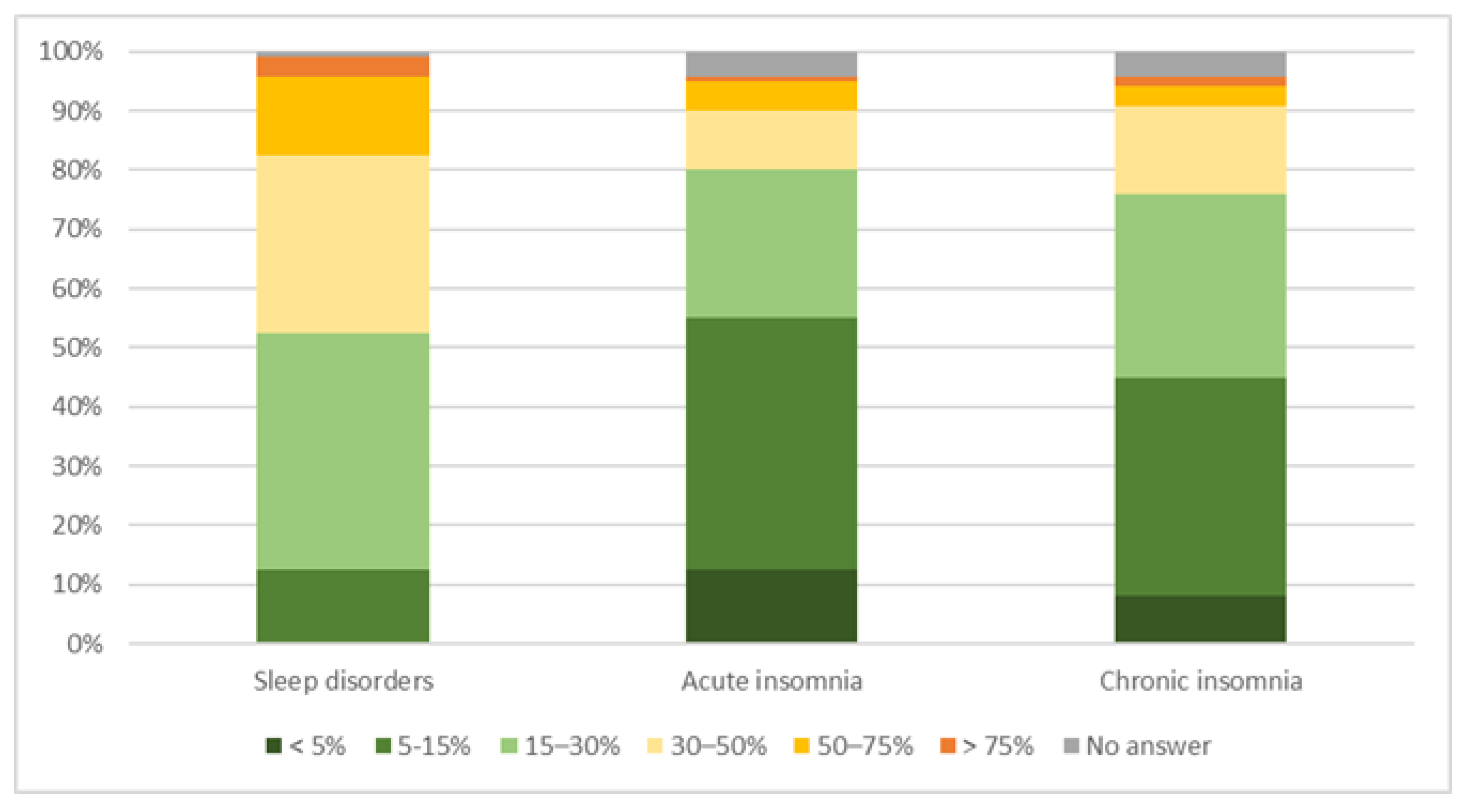
3.1. Knowledge about Insomnia
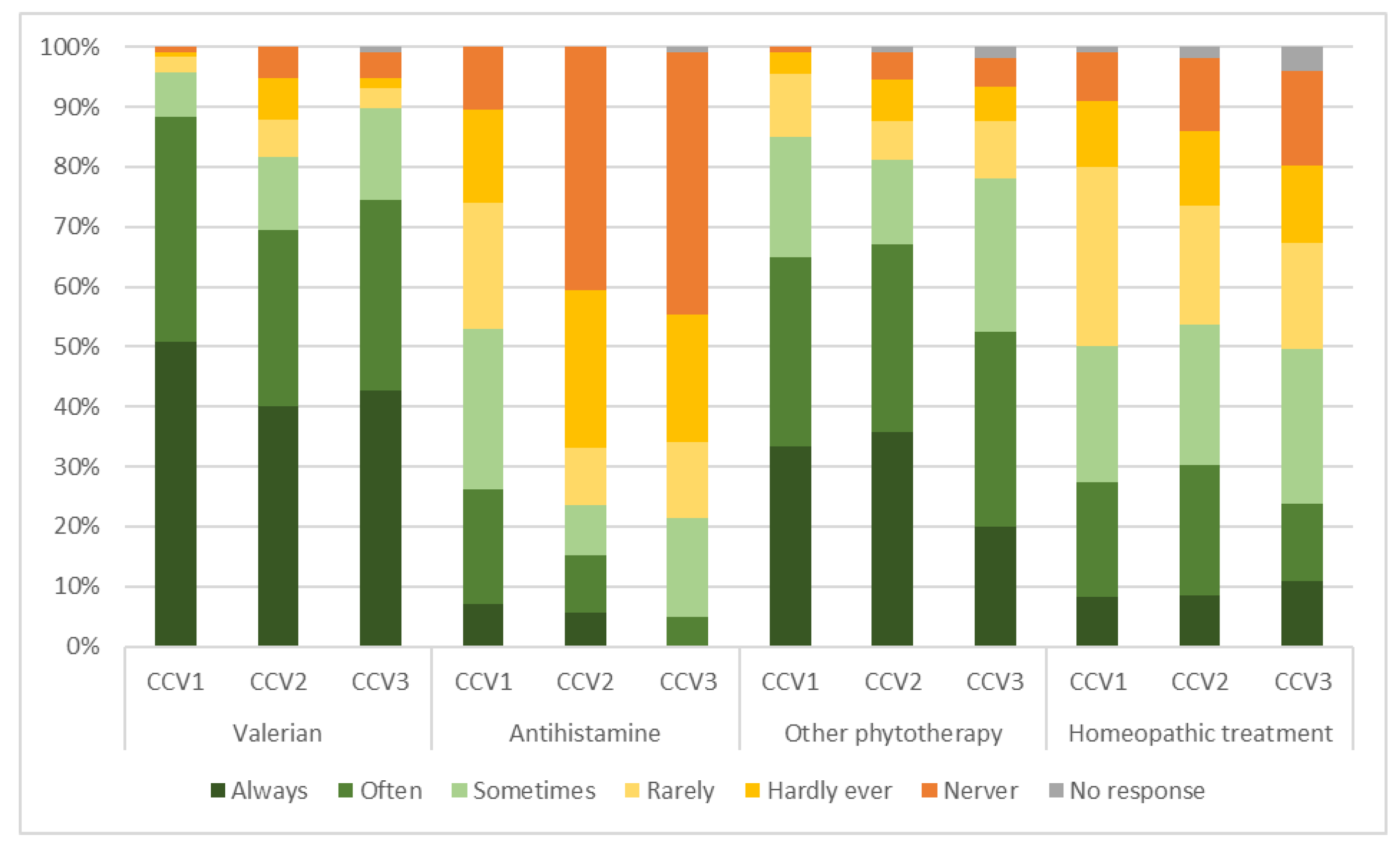
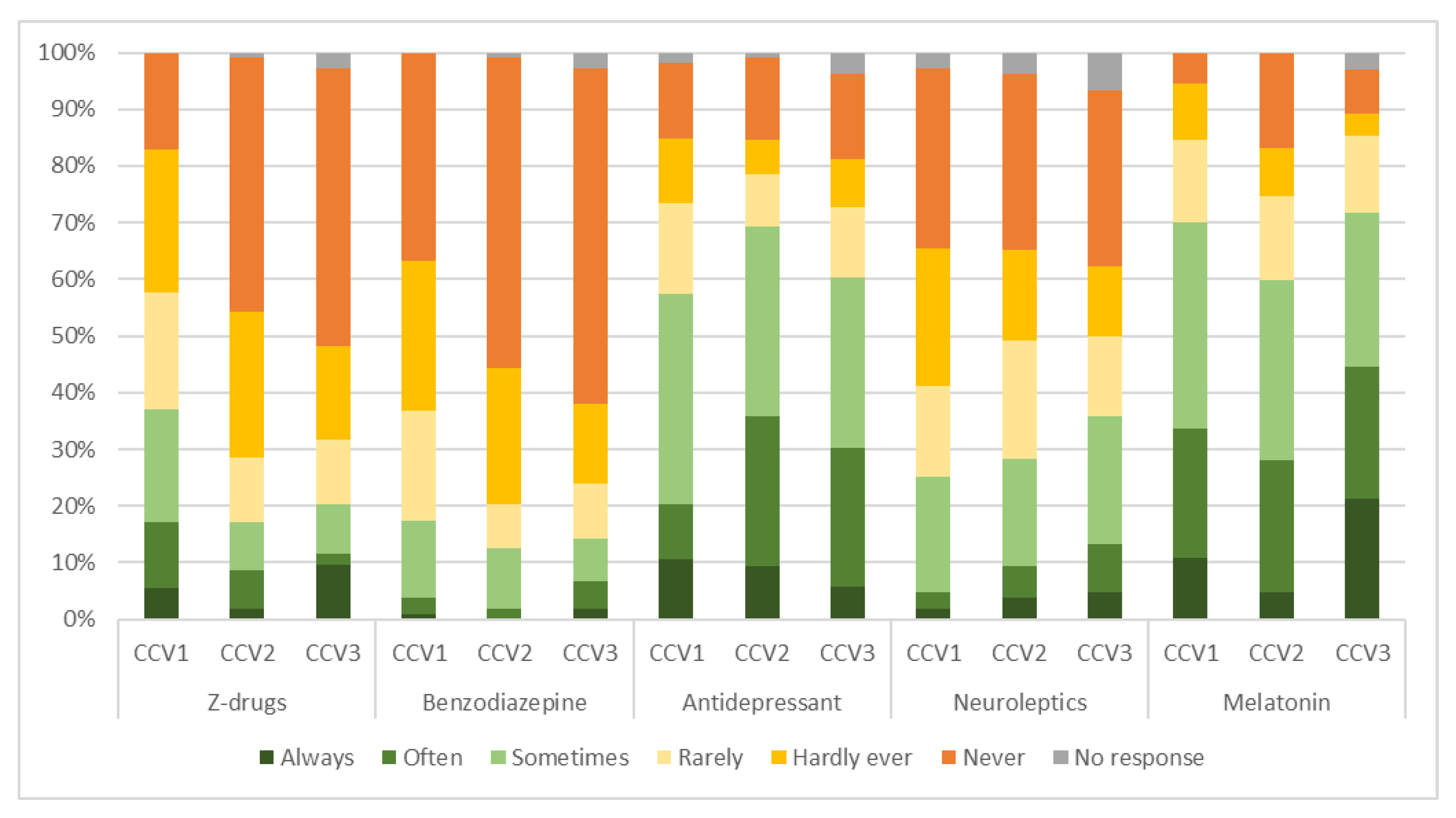
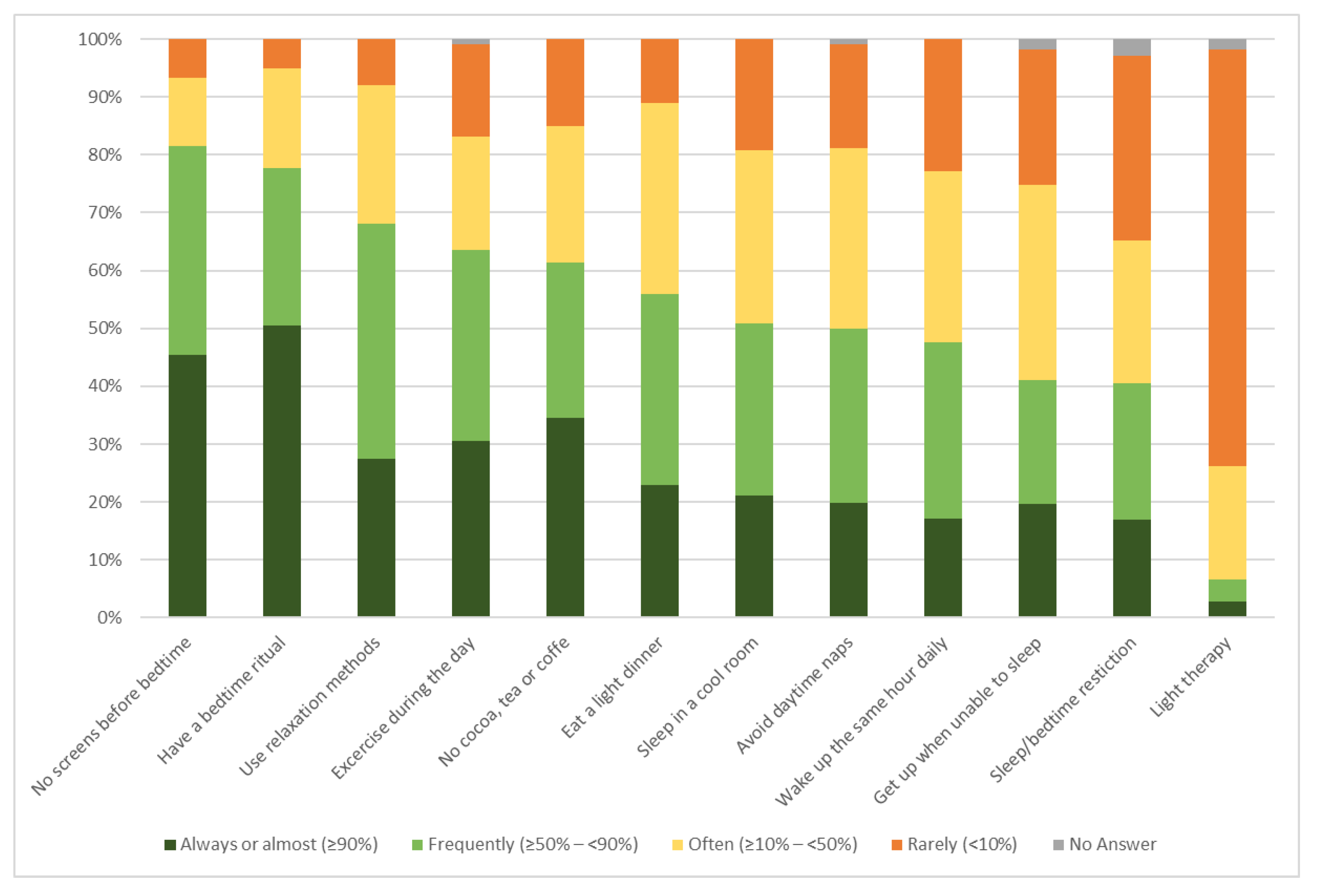
3.2. Counselling and Dispensing Practices
3.3. Knowledge about CBT-I
4. Discussion
4.1. Knowledge about Insomnia
4.2. Counselling and Dispensing Practices
4.3. Knowledge about CBT-I
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic And Statistical Manual Of Mental Disorders—DSM-5, 5th ed.; American Psychiatric Publishers: Washington, DC, USA, 2014. [Google Scholar]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Altena, E.; Bjorvatn, B.; Blom, K.; Bothelius, K.; Devoto, A.; Espie, C.A.; Frase, L.; Gavriloff, D.; Tuuliki, H.; et al. The European Academy for Cognitive Behavioural Therapy for Insomnia: An initiative of the European Insomnia Network to promote implementation and dissemination of treatment. J. Sleep Res. 2020, 29, e12967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delini-Stula, A.; Bischof, R.; Holsboer-Trachsler, E. Sleep behavior of the Swiss population: Prevalence and the daytime consequences of insomnia. Somnologie 2007, 11, 193–201. [Google Scholar] [CrossRef]
- Maire, M.; Linder, S.; Dvorak, C.; Merlo, C.; Essig, S.; Tal, K.; Del Giovane, C.; Syrogiannouli, L.; Duss, S.B.; Heinzer, R.; et al. Prevalence and management of chronic insomnia in Swiss primary care: Cross-sectional data from the “Sentinella” practice-based research network. J. Sleep Res. 2020, 29, e13121. [Google Scholar] [CrossRef]
- Schwegler, K.; Klaghofer, R.; Nirkko, A.C.; Mathis, J.; Hersberger, K.E.; Bloch, K.E. Sleep and wakefulness disturbances in Swiss pharmacy customers. Swiss Med. Wkly. 2006, 136, 149–154. [Google Scholar] [CrossRef]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Yaffe, K.; Falvey, C.M.; Hoang, T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014, 13, 1017–1028. [Google Scholar] [CrossRef]
- Li, M.; Zhang, X.W.; Hou, W.S.; Tang, Z.Y. Insomnia and risk of cardiovascular disease: A meta-analysis of cohort studies. Int. J. Cardiol. 2014, 176, 1044–1047. [Google Scholar] [CrossRef]
- Wickwire, E.M.; Shaya, F.T.; Scharf, S.M. Health economics of insomnia treatments: The return on investment for a good night’s sleep. Sleep Med. Rev. 2016, 30, 72–82. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Goncalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef]
- Riemann, D.; Perlis, M.L. The treatments of chronic insomnia: A review of benzodiazepine receptor agonists and psychological and behavioral therapies. Sleep Med. Rev. 2009, 13, 205–214. [Google Scholar] [CrossRef]
- Krieger, T.; Urech, A.; Duss, S.B.; Blattler, L.; Schmitt, W.; Gast, H.; Bassetti, C.; Berger, T. A randomized controlled trial comparing guided internet-based multi-component treatment and internet-based guided sleep restriction treatment to care as usual in insomnia. Sleep Med. 2019, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Maurer, L.F.; Schneider, J.; Miller, C.B.; Espie, C.A.; Kyle, S.D. The clinical effects of sleep restriction therapy for insomnia: A meta-analysis of randomised controlled trials. Sleep Med. Rev. 2021, 58, 101493. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.J.; Marshall, N.S.; Williams, A.; Grunstein, R.R. Predictors of primary medical care consultation for sleep disorders. Sleep Med. 2008, 9, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Wazaify, M.; Elayeh, E.; Tubeileh, R.; Hammad, E.A. Assessing insomnia management in community pharmacy setting in Jordan: A simulated patient approach. PLoS ONE 2019, 14, e0226076. [Google Scholar] [CrossRef] [Green Version]
- Linder, S.; Duss, S.B.; Dvorak, C.; Merlo, C.; Essig, S.; Tal, K.; Del Giovane, C.; Syrogiannouli, L.; Heinzer, R.; Nissen, C.; et al. Treating insomnia in Swiss primary care practices: A survey study based on case vignettes. J. Sleep Res. 2021, 30, e13169. [Google Scholar] [CrossRef]
- Peabody, J.W.; Luck, J.; Glassman, P.; Jain, S.; Hansen, J.; Spell, M.; Lee, M. Measuring the quality of physician practice by using clinical vignettes: A prospective validation study. Ann. Intern. Med. 2004, 141, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Landolt, S.; Rosemann, T.; Blozik, E.; Brungger, B.; Huber, C.A. Benzodiazepine and Z-Drug Use in Switzerland: Prevalence, Prescription Patterns and Association with Adverse Healthcare Outcomes. Neuropsychiatr. Dis. Treat. 2021, 17, 1021–1034. [Google Scholar] [CrossRef]
- Schur, N.; Twerenbold, S.; Reinau, C.; Schwenkglenks, M.; Meier, C.R. Helsana Medication Use Report 2020; Helsana Health Insurance Company: Lucerne, Switzerland, 2020. [Google Scholar]
- Schneider, S.; Schur, N.; Reinau, D.; Schwenkglenks, M.; Meier, C.R. Helsana Medication Use Report 2017; Helsana Health Insurance Company: Lucerne, Switzerland, 2017. [Google Scholar]
- Meolie, A.L.; Rosen, C.; Kristo, D.; Kohrman, M.; Gooneratne, N.; Aguillard, R.N.; Fayle, R.; Troell, R.; Townsend, D.; Claman, D.; et al. Oral nonprescription treatment for insomnia: An evaluation of products with limited evidence. J. Clin. Sleep Med. 2005, 1, 173–187. [Google Scholar] [CrossRef] [Green Version]
- Culpepper, L.; Wingertzahn, M.A. Over-the-Counter Agents for the Treatment of Occasional Disturbed Sleep or Transient Insomnia: A Systematic Review of Efficacy and Safety. Prim. Care Companion CNS Disord. 2015, 17, 26162. [Google Scholar] [CrossRef] [Green Version]
- Feehan, M.; Walsh, M.; Godin, J.; Sundwall, D.; Munger, M.A. Patient preferences for healthcare delivery through community pharmacy settings in the USA: A discrete choice study. J. Clin. Pharm. Ther. 2017, 42, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Whitty, J.A.; Kendall, E.; Sav, A.; Kelly, F.; McMillan, S.S.; King, M.A.; Wheeler, A.J. Preferences for the delivery of community pharmacy services to help manage chronic conditions. Res. Social Adm. Pharm. 2015, 11, 197–215. [Google Scholar] [CrossRef] [Green Version]
- Basheti, M.M.; Tran, M.; Wong, K.; Gordon, C.; Grunstein, R.; Saini, B. Australian Consultant Pharmacists’ Potential Roles in Sleep Health Care: Exploring a New Avenue for Improving the Management of Insomnia. Behav. Sleep Med. 2022, 20, 622–637. [Google Scholar] [CrossRef]
- Fuller, J.M.; Wong, K.K.; Hoyos, C.; Krass, I.; Saini, B. Dispensing good sleep health behaviours not pills--a cluster-randomized controlled trial to test the feasibility and efficacy of pharmacist-provided brief behavioural treatment for insomnia. J. Sleep Res. 2016, 25, 104–115. [Google Scholar] [CrossRef]
- Spath, M.; Hertenstein, E.; Schneider, C.L.; Trinca, E.; Maire, M.; Scharf, T.; Auer, R.; Nissen, C. Insomnia management in the family practice. Prim. Hosp. Care Allg. Inn. Med. 2022, 22, 76–80. [Google Scholar]
- Moloney, M.E.; Martinez, A.I.; Badour, C.L.; Moga, D.C. Internet-Based Cognitive Behavioral Therapy for Insomnia in Appalachian Women: A Pilot Study. Behav. Sleep Med. 2020, 18, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Pchelina, P.; Poluektov, M.; Berger, T.; Krieger, T.; Duss, S.B.; Bassetti, C. Effectiveness and Cost-Effectiveness of Internet-Based Cognitive Behavioral Therapy for Insomnia in Clinical Settings. Front. Psychiatry 2020, 11, 838. [Google Scholar] [CrossRef] [PubMed]
- Pchelina, P.; Duss, S.B.; Bernasconi, C.; Berger, T.; Krieger, T.; Bassetti, C.L.A.; Urech, A. Guided Internet-Based Cognitive Behavioral Therapy for Insomnia: Prognostic and Treatment-Predictive Factors. Diagnostics 2023, 13, 781. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic (N = 123) | N (SD) | % |
|---|---|---|
| Sex | ||
| Female | 97 | 78.9% |
| Male | 26 | 21.1% |
| Other | 0 | 0.0% |
| Missing | 0 | 0.0% |
| Age group | ||
| <30 years old | 12 | 9.8% |
| 31–40 years old | 20 | 16.3% |
| 41–50 years old | 26 | 21.1% |
| 51–60 years old | 40 | 32.5% |
| >60 years old | 25 | 20.3% |
| Missing | 0 | 0.0% |
| Language | ||
| French | 48 | 39.0% |
| German | 75 | 61.0% |
| Pharmacy experience in a community setting | ||
| <5 years | 15 | 12.2% |
| 6–15 years | 27 | 22.0% |
| 16–25 years | 32 | 26.0% |
| 26–35 years | 28 | 22.8% |
| >35 years | 21 | 17.1% |
| Missing | 0 | 0.0% |
| Function in the community pharmacy | ||
| Pharmacist and owner | 19 | 15.5% |
| Managing pharmacist | 28 | 22.8% |
| Deputy pharmacist | 61 | 49.6% |
| Surrogate | 10 | 8.1% |
| Other | 5 | 4.1% |
| Missing | 0 | 0.0% |
| Initial university degree from | ||
| Basel (Switzerland) | 36 | 29.3% |
| Bern (Switzerland) | 10 | 8.1% |
| ETH Zurich (Switzerland) | 27 | 22.0% |
| Geneva and/or Lausanne (Switzerland) | 29 | 23.6% |
| Other | 16 | 13.0% |
| Missing | 5 | 4.0% |
| Post-graduate pharmacy qualification | ||
| FPH in Community Pharmacy | 47 | 27.0% |
| FPH in Hospital Pharmacy | 0 | 0.0% |
| FPH in Clinical Pharmacy | 0 | 0.0% |
| FPH in Anamnesis in primary care | 36 | 20.7% |
| Course for leading quality circles | 30 | 17.2% |
| CAS in Clinical Pharmacy, Geneva | 1 | 0.6% |
| CAS in Clinical Pharmacy, Zurich/Basel | 4 | 2.3% |
| Doctorate | 9 | 5.2% |
| None | 25 | 14.4% |
| Other | 22 | 12.6% |
| Location of the pharmacy | ||
| City centre | 38 | 30.9% |
| Urban | 47 | 38.2% |
| Rural | 38 | 30.9% |
| Missing | 0 | 0.0% |
| Type of drug dispensing * | ||
| Dispensed by pharmacies only | 52 | 42.2% |
| Dispensed by physicians only | 42 | 34.1% |
| Mixed dispensing | 28 | 22.8% |
| Missing | 1 | 0.9% |
| Community pharmacy structure | ||
| Pharmacy chain | 29 | 23.6% |
| Pharmaceutical group | 36 | 29.3% |
| Group-purchasing pharmacy | 10 | 8.1% |
| Independent pharmacy | 46 | 37.4% |
| Other | 1 | 0.8% |
| Missing | 1 | 0.8% |
| Discussing Sleep Disorders | Discussing Sleep Hygiene | |
|---|---|---|
| <5 min | 3.4% | 32.8% |
| 5–10 min | 52.1% | 42.9% |
| >10 to 15 min | 37.0% | 19.3% |
| >15 min | 6.7% | 5.0% |
| No answer | 0.8% | 0.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mulder, F.; Löwinger, D.; Jenkinson, S.P.; Kaiser, E.; Scharf, T.; Maire, M.; Duss, S.; Bassetti, C.; Heinzer, R.; Auer, R.; et al. Counselling for Chronic Insomnia in Swiss Pharmacies: A Survey Study Based on Case Vignettes. Pharmacy 2023, 11, 105. https://doi.org/10.3390/pharmacy11030105
Mulder F, Löwinger D, Jenkinson SP, Kaiser E, Scharf T, Maire M, Duss S, Bassetti C, Heinzer R, Auer R, et al. Counselling for Chronic Insomnia in Swiss Pharmacies: A Survey Study Based on Case Vignettes. Pharmacy. 2023; 11(3):105. https://doi.org/10.3390/pharmacy11030105
Chicago/Turabian StyleMulder, Fanny, Dimitri Löwinger, Stephen P. Jenkinson, Estelle Kaiser, Tamara Scharf, Micheline Maire, Simone Duss, Claudio Bassetti, Raphaël Heinzer, Reto Auer, and et al. 2023. "Counselling for Chronic Insomnia in Swiss Pharmacies: A Survey Study Based on Case Vignettes" Pharmacy 11, no. 3: 105. https://doi.org/10.3390/pharmacy11030105