
Antimicrobial Stewardship and Dose Adjustment of Restricted Antimicrobial Drugs in Hospital Setting

Abstract
:1. Introduction
2. Materials and Methods
- name of department/clinic;
- patient information including age and weight;
- clinical data: main diagnosis for use of restricted antimicrobials, other diagnoses, renal function (normal or impaired), type of infection (out-of-hospital or in-hospital), type of antibiotic therapy (empirical, targeted, prophylaxis or continuation of already approved therapy), previous antimicrobial therapy, microbiological sample, isolated causative agent and sensitivity to antimicrobials (in case of targeted therapy);
- name of the required antimicrobial drug and daily dosage;
- special observations and prescriber’s explanation for the required antimicrobial;
- section for clinical pharmacologist’s opinion/commentary;
- section for infectologist’s opinion/comment;
- section for clinical pharmacist’s opinion/commentary.
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 15 December 2022).
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 20 March 2023).
- European Centre for Disease Prevention and Control. Antimicrobial Resistance—Tackling the Burden in the European Union. Available online: https://www.oecd.org/health/health-systems/AMR-Tackling-the-Burden-in-the-EU-OECD-ECDC-Briefing-Note-2019.pdf (accessed on 15 December 2022).
- Agency for Medicinal Products and Medical Devices of Croatia. Annual Report on Drug Utilisation for 2021—Croatian Document. Available online: https://www.halmed.hr/en/Novosti-i-edukacije/Publikacije-i-izvjesca/Izvjesca-o-potrosnji-lijekova/ (accessed on 20 December 2022).
- Browne, A.J.; Chipeta, M.G.; Haines-Woodhouse, G.; Kumaran, E.P.A.; Hamadani, B.H.K.; Zaraa, S.; Henry, N.J.; Deshpande, A.; Reiner, R.C., Jr.; Day, N.P.J.; et al. Global antibiotic consumption and usage in humans, 2000-18: A spatial modelling study. Lancet Planet Health 2021, 5, e893–e904. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.C.; Zembower, T.R. Global increases in antibiotic consumption: A concerning trend for WHO targets. Lancet Infect. Dis. 2021, 21, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Milkowska-Shibata, M.; Tseng, K.K.; Sharland, M.; Gandra, S.; Pulcini, C.; Laxminarayan, R. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000-15: An analysis of pharmaceutical sales data. Lancet Infect. Dis. 2021, 21, 107–115. [Google Scholar] [CrossRef]
- Mendelson, M.; Morris, A.M.; Thursky, K.; Pulcini, C. How to start an antimicrobial stewardship programme in a hospital. Clin. Microbiol. Infect. 2020, 26, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Pulcini, C.; Gyssens, I.C. How to educate prescribers in antimicrobial stewardship practices. Virulence 2013, 4, 192–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Antimicrobial Stewardship Programmes in Health-Care Facilities in Low- and Middle-Income Countries. Available online: https://apps.who.int/iris/bitstream/handle/10665/329404/9789241515481-eng.pdf (accessed on 20 December 2022).
- European Centre for Disease Prevention and Control. Infographics about Antibiotic Stewardship Programmes. Available online: https://antibiotic.ecdc.europa.eu/en/infographics-about-antibiotic-stewardship-programmes (accessed on 20 December 2022).
- Nathwani, D.; Varghese, D.; Stephens, J.; Ansari, W.; Martin, S.; Charbonneau, C. Value of hospital antimicrobial stewardship programs [ASPs]: A systematic review. Antimicrob. Resist. Infect. Control 2019, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- World Health Organization. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis. Available online: https://apps.who.int/iris/handle/10665/311820 (accessed on 5 January 2023).
- Thuong, M.; Shortgen, F.; Zazempa, V.; Girou, E.; Soussy, C.J.; Brun-Buisson, C. Appropriate use of restricted antimicrobial agents in hospitals: The importance of empirical therapy and assisted re-evaluation. J. Antimicrob. Chemother. 2000, 46, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Tarcea Bizo, P.; Dumitras, D.; Popa, A. Evaluation of restricted antibiotic use in a hospital in Romania. Int. J. Clin. Pharm. 2015, 37, 452–456. [Google Scholar] [CrossRef]
- Samardžić, I.; Marinović, I.; Matković, I.; Mamić, I.; Bačić Vrca, V. Antimicrobial drugs involved in potential drug- drug-interactions in cardiosurgical patients. Pharmazie 2021, 76, 6–11. [Google Scholar]
- Dellit, T.H.; Owens, R.C.; McGowan, J.E., Jr.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Karanika, S.; Paudel, S.; Grigoras, C.; Kalbasi, A.; Mylonakis, E. Systematic Review and Meta-analysis of Clinical and Economic Outcomes from the Implementation of Hospital-Based Antimicrobial Stewardship Programs. Antimicrob. Agents Chemother. 2016, 60, 4840–4852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, K.A.; Kullar, R.; Gilchrist, M.; File, T.M., Jr. Antibiotics and adverse events: The role of antimicrobial stewardship programs in ‘doing no harm’. Curr. Opin. Infect. Dis. 2019, 32, 553–558. [Google Scholar] [CrossRef]
- Bouvy, J.C.; De Bruin, M.L.; Koopmanschap, M.A. Epidemiology of adverse drug reactions in Europe: A review of recent observational studies. Drug Saf. 2015, 38, 437–453. [Google Scholar] [CrossRef] [Green Version]
- Tamma, P.D.; Avdic, E.; Li, D.X.; Dzintars, K.; Cosgrove, S.E. Association of Adverse Events With Antibiotic Use in Hospitalized Patients. JAMA Intern. Med. 2017, 177, 1308–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagiya, H.; Kokado, R.; Ueda, A.; Okuno, H.; Morii, D.; Hamaguchi, S.; Yamamoto, N.; Yoshida, H.; Tomono, K. Association of adverse drug events with broad-spectrum antibiotic use in hospitalized patients: A single-center study. Intern. Med. 2019, 58, 2621–2625. [Google Scholar] [CrossRef] [Green Version]
- Pretorius, R.W.; Gataric, G.; Swedlund, S.K.; Miller, J.R. Reducing the risk of adverse drug events in older adults. Am. Fam. Physician 2013, 87, 331–336. [Google Scholar]
- Hammond, D.A.; Smith, M.N.; Li, C.; Hayes, S.M.; Lusardi, K.; Bookstaver, P.B. Systematic Review and Meta-Analysis of Acute Kidney Injury Associated with Concomitant Vancomycin and Piperacillin/tazobactam. Clin. Infect. Dis. 2017, 64, 666–674. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, L.A.; Levey, A.S. Chronic kidney disease in the elderly—How to assess risk. N. Engl. J. Med. 2005, 352, 2122–2124. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Inter. Suppl. 2013, 3, 1–150. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612, Erratum in Ann. Intern. Med. 2011, 155, 408. [Google Scholar] [CrossRef] [PubMed]
- Radišić Biljak, V.; Honović, L.; Matica, J.; Krešić, B.; Šimić Vojak, S. The role of laboratory testing in detection and classification of chronic kidney disease: National recommendations. Biochem. Med. 2017, 27, 153–176. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Quality of Health Care in America; Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. (Eds.) To Err is Human: Building a Safer Health System; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Lassiter, J.; Bennett, W.M.; Olyaei, A.J. Drug dosing in the elderly patients with chronic kidney disease. Clin. Geriatr. Med. 2009, 25, 459–527. [Google Scholar] [CrossRef]
- Davies, E.C.; Green, C.F.; Mottram, D.R.; Pirmohamed, M. Adverse drug reactions in hospital in-patients: A pilot study. J. Clin. Pharm. Ther. 2006, 31, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Huang, Y.J.; Hung, M.C.; Hung, S.C.; Hsiao, C.Y.; Cho, H.L.; Lai, L.F.; Tong, S.H.; Wang, J.T. Risk factors associated with the development of seizures among adult patients treated with ertapenem: A matched case-control study. PLoS ONE 2017, 12, e0182046. [Google Scholar] [CrossRef] [Green Version]
- Baggio, D.; Ananda-Rajah, M.R. Fluoroquinolone antibiotics and adverse events. Aust. Prescr. 2021, 44, 161–164. [Google Scholar] [CrossRef]
- Rawla, P.; El Helou, M.L.; Vellipuram, A.R. Fluoroquinolones and the Risk of Aortic Aneurysm or Aortic Dissection: A Systematic Review and Meta-Analysis. Cardiovasc. Hematol. Agents Med. Chem. 2019, 17, 3–10. [Google Scholar] [CrossRef]
- Saito, T.; Nakamura, M.; Watari, M.; Isse, K. Tardive seizure and antibiotics: Case reports and review of the literature. J. ECT 2008, 24, 275–276. [Google Scholar] [CrossRef]
- Grill, M.F.; Maganti, R.K. Neurotoxic effects associated with antibiotic use: Management considerations. Br. J. Clin. Pharmacol. 2011, 72, 381–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schliamser, S.E.; Cars, O.; Norrby, S.R. Neurotoxicity of beta-lactam antibiotics: Predisposing factors and pathogenesis. J. Antimicrob. Chemother. 1991, 27, 405–425. [Google Scholar] [CrossRef] [PubMed]
- Bailie, G.R.; Neal, D. Vancomycin ototoxicity and nephrotoxicity. A review. Med. Toxicol. Adverse Drug Exp. 1988, 3, 376–386. [Google Scholar] [CrossRef]
- Lin, Y.F.; Yang, C.H.; Sindy, H.; Lin, J.Y.; Rosaline Hui, C.Y.; Tsai, Y.C.; Wu, T.S.; Huang, C.T.; Kao, K.C.; Hu, H.C.; et al. Severe cutaneous adverse reactions related to systemic antibiotics. Clin. Infect. Dis. 2014, 58, 1377–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conly, J.; Johnston, B. Colistin: The phoenix arises. Can. J. Infect. Dis. Med. Microbiol. 2006, 17, 267–269. [Google Scholar] [CrossRef] [Green Version]
- Teva UK Limited. Colomycin 1 Million International Units (IU) Powder for Solution for Injection, Infusion or Inhalation: Summary of Product Characteristics. Available online: https://www.medicines.org.uk/emc/product/1094/smpc#gref (accessed on 10 January 2023).
- Eljaaly, K.; Bidell, M.R.; Gandhi, R.G.; Alshehri, S.; Enani, M.A.; Al-Jedai, A.; Lee, T.C. Colistin Nephrotoxicity: Meta-Analysis of Randomized Controlled Trials. Open Forum Infect. Dis. 2021, 8, ofab026. [Google Scholar] [CrossRef]
- Salman, B.; Al-Hashar, A.; Al-Khirbash, A.; Al-Zakwani, I. Clinical and Cost Implications of Clinical Pharmacist Interventions on Antimicrobial Use at Sultan Qaboos University Hospital in Oman. Int. J. Infect. Dis. 2021, 109, 137–141. [Google Scholar] [CrossRef]
- Chahine, B. Antibiotic dosing adjustments in hospitalized patients with chronic kidney disease: A retrospective chart review. Int. Urol. Nephrol. 2022, 54, 157–163. [Google Scholar] [CrossRef]
- McCarthy, L.M.; Visentin, J.D.; Rochon, P.A. Assessing the scope and appropriateness of prescribing cascades. J. Am. Geriatr. Soc. 2019, 67, 1023–1026. [Google Scholar] [CrossRef]
- Davies, E.C.; Green, C.F.; Taylor, S.; Williamson, P.R.; Mottram, D.R.; Pirmohamed, M. Adverse drug reactions in hospital in-patients: A prospective analysis of 3695 patient-episodes. PLoS ONE 2009, 4, e4439. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Available online: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf (accessed on 20 March 2023).
- World Health Organization. Antimicrobial Resistance: A Manual for Developing National Action Plans. Available online: https://www.who.int/publications/i/item/antimicrobial-resistance-a-manual-for-developing-national-action-plans (accessed on 20 March 2023).



{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| Number of patients | 913 |
| Male | 540 (59.1) |
| Mean age, years | 67.5 |
| <65 | 323 (35.4) |
| 65–75 | 259 (28.4) |
| 75–85 | 240 (26.3) |
| >=85 | 91 (10.0) |
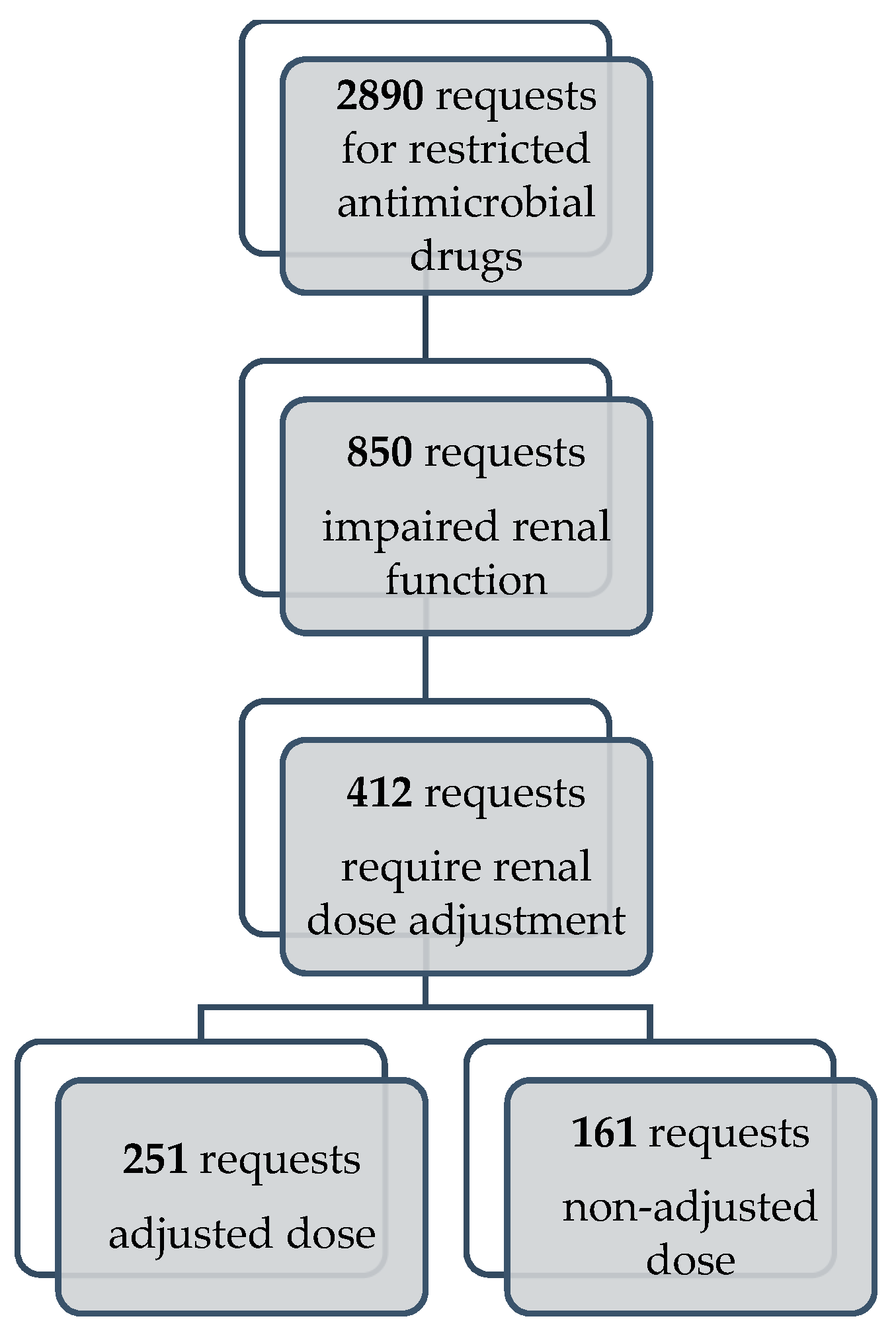
| Number of requests for restricted antimicrobial drugs (RAD) | 2890 |
| Mean number of requests for RAD per patient | 3.17 |
| Number of different RAD per patient (range) | 1.6 (1–9) |
| Number of patients with 2 or more RAD simultaneously | 133 |
| eGFR stage (KDIGO classification) | |
| G1 Normal or high | 1332 (46.1) |
| G2 Mildly decreased | 708 (24.5) |
| G3a Mildly to moderate decreased | 280 (9.7) |
| G3b Moderately to severely decreased | 230 (8.0) |
| G4 Severely decreased | 198 (6.9) |
| G5 Kidney failure | 142 (4.9) |
| General principles of antimicrobial therapy, n (%) | |
| Empiric | 1039 (33.0) |
| Directed | 945 (30.0) |
| Prophylaxis | 292 (9.3) |
| Continuation | 874 (27.7) |
| Most frequently isolated microorganism, n (%) | |
| Acinetobacter baummannii | 169 (17.9) |
| Klebsiella pneumoniae | 140 (14.8) |
| Pseudomonas aeruginosa | 128 (13.5) |
| Escherichia coli | 87 (9.2) |
| Clostridiodes difficile | 81 (8.6) |
| Number of requests per department, n (%) | |
| Department of gastroenterology, hepatology and clinical nutrition | 284 (9.8) |
| Department of nephrology | 244 (8.4) |
| Department of clinical immunology and rheumatology | 232 (8.0) |
| Department of hematology | 219 (7.6) |
| Intensive care unit, Department of internal medicine | 198 (6.9) |
| Localization of infection, n (%) | |
| Respiratory tract | 577 (20.0) |
| Urinary tract | 524 (18.1) |
| Intra-abdominal | 308 (10.7) |
| Sepsis | 282 (9.8) |
| Skin and soft tissue | 208 (7.2) |
| Restricted Antimicrobial Drug | Total Number of Requests | Number of Requests Which Required Dose Adjustment according to Renal Function | Unadjusted Dose | Unadjusted Dose/Number of Requests That Required Renal Dose Adjustment (%) |
|---|---|---|---|---|
| Meropenem | 540 | 125 | 54 | 43.2 |
| Ciprofloxacin | 455 | 121 | 33 | 27.3 |
| Piperacillin/Tazobactam | 195 | 39 | 10 | 25.6 |
| Vancomycin | 290 | 35 | 20 | 57.1 |
| Colistin | 113 | 24 | 16 | 66.7 |
| Fluconazole | 230 | 21 | 5 | 23.8 |
| Cefepime | 63 | 9 | 2 | 22.2 |
| Teicoplanin | 17 | 8 | 6 | 75 |
| Imipenem/Cilastatin | 16 | 8 | 0 | 0 |
| Ceftazidime/Avibactam | 39 | 6 | 6 | 100 |
| Amikacin | 49 | 6 | 4 | 66.7 |
| Levofloxacin | 38 | 3 | 3 | 100 |
| Fosfomycin | 28 | 2 | 1 | 50 |
| Ampicillin/Sulbactam | 66 | 2 | 0 | 0 |
| Sulfamethoxazole-trimethoprim | 29 | 2 | 0 | 0 |
| Cefpodoxime | 8 | 1 | 1 | 100 |
| Cefixime | 2 | 0 | 0 | 0 |
| Ceftazidime | 4 | 0 | 0 | 0 |
| Ceftriaxone | 430 | 0 | 0 | 0 |
| Ertapenem | 18 | 0 | 0 | 0 |
| Total | 2630 | 412 | 161 |
| Restricted Antimicrobial Drug | ATC Classification | Requests, n |
|---|---|---|
| Linezolid | J01X | 95 |
| Vancomycin (oral use) | J01X | 90 |
| Moxifloxacin | J01M | 49 |
| Posaconazole | J02A | 9 |
| Anidulafungin | J02A | 7 |
| Isavuconazole | J02A | 5 |
| Micafungin | J02A | 1 |
| Fidaxomicin | A07A | 1 |
| Tigecycline | J01A | 1 |
| Itraconazole | J02A | 1 |
| Voriconazole | J02A | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlak, I.; Samardžić, I.; Marinović, I.; Bušić, N.; Vrca, V.B. Antimicrobial Stewardship and Dose Adjustment of Restricted Antimicrobial Drugs in Hospital Setting. Pharmacy 2023, 11, 68. https://doi.org/10.3390/pharmacy11020068
Vlak I, Samardžić I, Marinović I, Bušić N, Vrca VB. Antimicrobial Stewardship and Dose Adjustment of Restricted Antimicrobial Drugs in Hospital Setting. Pharmacy. 2023; 11(2):68. https://doi.org/10.3390/pharmacy11020068
Chicago/Turabian StyleVlak, Iva, Ivana Samardžić, Ivana Marinović, Nikolina Bušić, and Vesna Bačić Vrca. 2023. "Antimicrobial Stewardship and Dose Adjustment of Restricted Antimicrobial Drugs in Hospital Setting" Pharmacy 11, no. 2: 68. https://doi.org/10.3390/pharmacy11020068