
Medication-Related Complaints in Residential Aged Care

Abstract
:1. Introduction
2. Materials and Methods
2.1. Complaints Dataset
2.2. Qualitative Analysis
2.3. Statistical Analysis
3. Results
3.1. Keywords/Sub-Keywords Used to Describe Medication-Related Complaints
3.2. Types of Medication-Related Complaint Issues
‘The service has inadequate medication management procedures as staff are unfamiliar with S4 and S8 medications, drug charts are difficult to read, observations are not completed, and some medications (opioids) are not administered overnight because there is no RN’.(registered nurse)
- Not receiving medication at the right time
- Inadequate medication management systems, processes or policies in place
- Chemical restraint.
3.2.1. Not Receiving Medication on Time
‘Concern during a scheduled 4-week respite stay the service failed to provide appropriate medication management to consumer as his medication provided to the service upon admission was left untouched.’
‘Service did not provide adequate pain management. Specifically, there was a delay of 4 hours before morphine was given to her after the doctor had prescribed it at 1 pm. As a result, the resident was screaming in pain.’
3.2.2. Inadequate Medication Management Systems, Policies and Procedures
‘Medication management at the service simply does not meet the basic needs of its consumers’, and ‘Concern about the appropriate identification, handling, timing and management of medication.’
‘Registered nurses are not checking medications with another registered nurse but instead relying on PCA (personal care assistants) to check dosages.’ and ‘Kitchen staff are administering medications and they are not trained to do so.’
‘Enrolled nurses are administering Schedule 8 drugs to consumers unsupervised and on a daily basis.’(Schedule 8 drugs are controlled drugs of dependence, mainly opioids. Legally they must only be administered and documented by a registered nurse)
3.2.3. Chemical Restraint
‘The residents are being inappropriately medicated with either painkillers or psychotropics.’ and ‘It is a regular occurrence that you see a resident wandering around or being disruptive, something might happen and then the next time you see them they are heavily sedated.’
‘Consumer is unaware of what medication she is given, especially at night, and she often wakes up groggy, and has expressed concern that she was given sleeping tablets to prevent her from getting up during the night to use the toilet.’
‘Care recipients have ceased medications that may be classified as a form of restraint, which has led to an increase in unmanaged care recipient aggression.’
3.2.4. Other Complaint Issues
‘The consumer is being sedated against the wishes of her Enduring Power of Attorney. She is being administered risperidone (antipsychotic) with no diagnosis, medical reason and no explanation to her family.’
‘A concern that resident was being given inconsistent and incorrect doses of his medications while at the nursing home, resulting in repeated, unnecessary hospital admissions.’
‘Instead of ceasing medication for depression and replacing it with another, the resident was given both medications for 3 months.’
3.3. Medical Conditions and Medicines Associated with Medication-Related Complaint Issues
’The family were asked would they be happy to let the consumer go 12 hours without a morphine injection (until the RN came back on duty in the morning).’
‘Staff have not taken action to obtain a urine specimen from mum despite her daughter requesting a simple ‘dip stick’ be done to check if there is an indication of a UTI.’
‘The service does not provide my mum with her Parkinson’s medication before her shower. As a result, she is prone to falls.’
3.4. Associations between the Complainant and Medication-Related Complaints
4. Discussion
4.1. Resident and Family Involvement in Medication Management
4.2. Limitations and Strengths of this Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collins Dictionary. Available online: https://www.collinsdictionary.com/dictionary/english/medication (accessed on 7 December 2022).
- Commonwealth of Australia. Department of Health and Aged Care. Guiding Principles for Medication Management in Residential Aged Care Facilities; Commonwealth of Australia (Department of Health and Aged Care): Canberra, ACT, Australia, 2022. [Google Scholar]
- National Institute of Health (NIH); National Cancer Institute. NIH Dictionaries. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/administration (accessed on 7 December 2022).
- Australian Commission on Safety and Quality in Health Care (ACSQHC) Medication Safety Standard n.d. Available online: https://www.safetyandquality.gov.au/standards/nsqhs-standards/medication-safety-standard (accessed on 7 December 2022).
- Sluggett, J.; Ilomanki, J.; Seaman, K.; Corlis, M.; Bell, J.S. Medication management policy, practice and research in Australian residential aged care: Current and future directions. Pharmacol Res 2017, 116, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Bony, H.; Lloyd, R.A.; Hotham, E.D.; Corre, L.J.; Corlis, M.E.; Loffler, H.A.; Scarlett, G.K.; Tsimbinos, J.M.; Todd, I.P. Differences in the prescribing of potentially inappropriate medicines in older Australians: Comparison of community dwelling and residential aged care residents. Sci. Rep. 2020, 10, 10170. [Google Scholar] [CrossRef] [PubMed]
- NSW Nurses and Midwives’ Association. The State of Medication in NSW Residential Aged Care. NSW. 2017. Available online: https://www.nswnma.asn.au/wp-content/uploads/2017/12/Medication-in-NSW-RAS-FINAL-LR.pdf (accessed on 7 December 2022).
- Aged Care Quality and Safety Commission (ACQSC). The Aged Care Quality Standards. Canberra. 2021. Available online: www.agedcarequality.gov.au/providers/standards (accessed on 7 December 2022).
- ACSQHC. Quality Use of Medicines and Medicines Safety (10th National Health Priority). Discussion Paper for Public Consultation. Phase 1: Aged Care. Sydney. 2020. Available online: https://apo.org.au/node/317061 (accessed on 7 December 2022).
- Price, S.D.; Holman, C.D.J.; Sanfilippo, F.M.; Emery, J.D. Are high-care nursing home residents at greater risk of unplanned hospital admission than other elderly patients when exposed to Beers potentially inappropriate medications? Geriatr. Geront. Int. 2014, 14, 934–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pharmaceutical Society of Australia (PSA). Medication Safety in Aged Care. PSA. 2020. Available online: https://www.psa.org.au/advocacy/working-for-our-profession/medicine-safety/aged-care/ (accessed on 7 December 2022).
- ACQSC. The Complaints Process. 2020. Available online: https://www.agedcarequality.gov.au/makingcomplaint/complaints-process (accessed on 21 December 2022).
- Aged Care Complaints Commissioner. Annual Report 2017–18. 2018. Available online: https://www.agedcarequality.gov.au/about-us/corporate-publications/aged-care-complaints-commissioner (accessed on 21 December 2022).
- ACQSC. Aged Care Quality and Safety Commission’s Annual Report 2018–19. 2019. Available online: https://www.agedcarequality.gov.au/about-us/corporate-documents (accessed on 21 December 2022).
- ACQSC. Aged Care Quality and Safety Commission’s Annual Report 2019–20. 2020. Available online: https://www.agedcarequality.gov.au/about-us/corporate-documents (accessed on 21 December 2022).
- Reader, T.; Gillespie, A.; Roberts, J. Patient complaints in healthcare systems: A systematic review and coding taxonomy. BMJ Qual. Saf. 2014, 23, 678–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolbe, R.H.; Burnett, M.S. Content-analysis research: An examination of applications with directives for improving research reliability and objectivity. J. Consum. Res. 1991, 18, 243–250. [Google Scholar] [CrossRef]
- Hibbert, P.D.; Clay-Williams, R.; Westbrook, J.; Reed, R.L.; Georgiou, A.; Wiles, L.K.; Molloy, C.J.; Braithwaite, J. Reducing preventable harm to residents in aged care: A systems approach. Austral. J. Ageing 2021, 40, 72–76. [Google Scholar] [CrossRef] [PubMed]
- ACSQHC. National Residential Medication Chart User Guide for Nursing Staff (Version 4). 2021. ACSQHC, Sydney. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/national-residential-medication-chart-user-guide-nursing-staff (accessed on 5 January 2023).
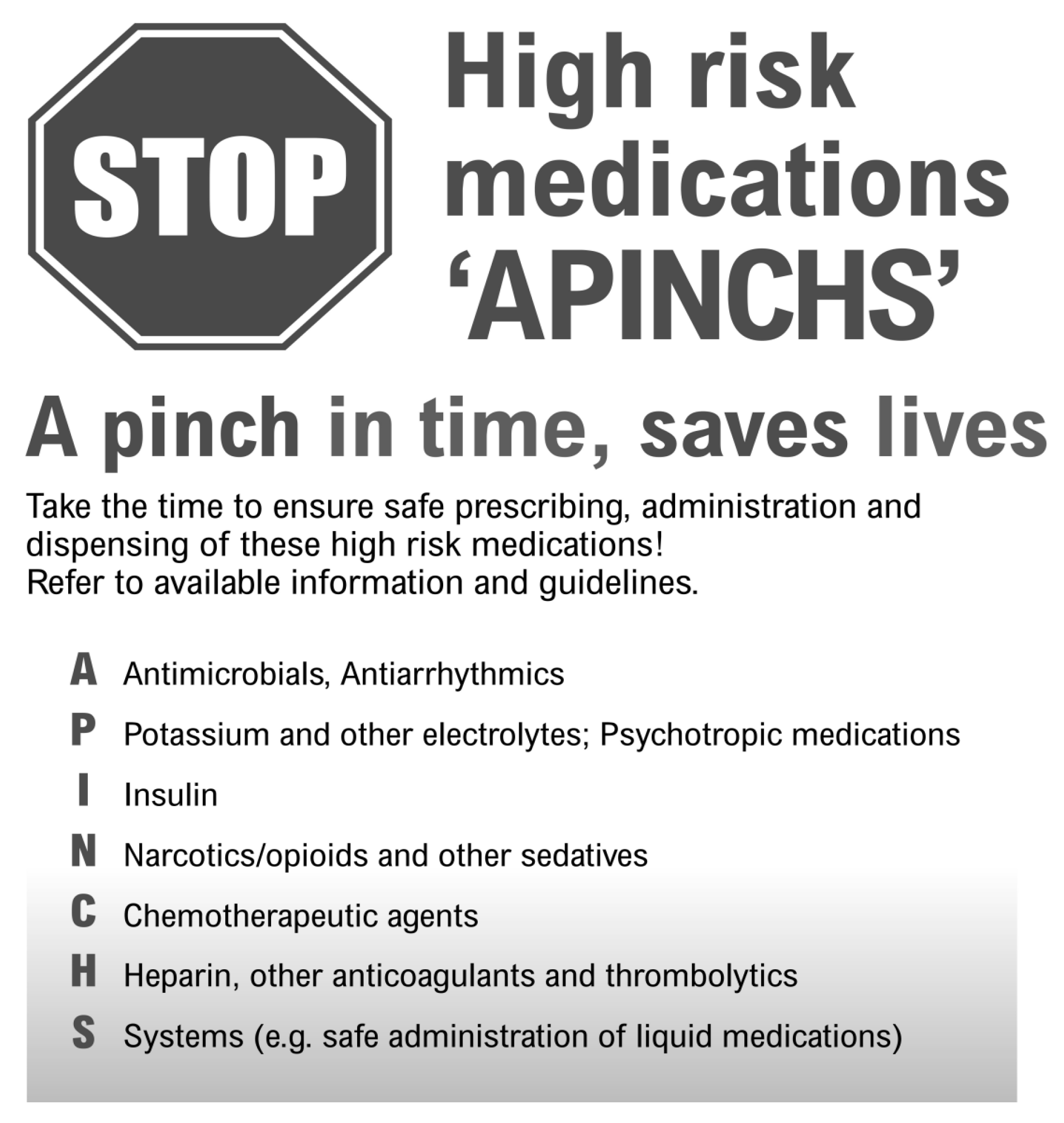
- ACSQHC. APINCHS Classification of High-Risk Medicines. 2019. Available online: https://www.safetyandquality.gov.au/our-work/medication-safety/high-risk-medicines/apinchs-classification-high-risk-medicines (accessed on 5 January 2023).
- Royal Perth Hospital Medication Safety Committee. High Risk Medications ‘APINCHS’. Poster. Department of Health Western Australia. 2015. Available online: https://ww2.health.wa.gov.au/~/media/Files/Corporate/general-documents/safety/PDF/Medication-safety-resources/High-risk-medications-APINCHS.pdf (accessed on 5 January 2023).
- MedCalc Software Ltd. Comparison of Proportions Calculator. Available online: https://www.medcalc.org/calc/comparison_of_proportions.php (accessed on 15 March 2023).
- Royal Commission into Aged Care Quality and Safety. Final Report: Final Report: Care, Dignity and Respect. 2021. Available online: https://agedcare.royalcommission.gov.au/publications/final-report (accessed on 9 January 2023).
- Australian Government. Federal Register of legislation. Quality of Care Principles 2014. 2022. Available online: https://www.legislation.gov.au/Details/F2022C01230 (accessed on 9 January 2023).
- Australian Government. Department of Health. Pharmacy Programs Administrator. Program Rules. Quality Use of Medicines. 2020. Available online: https://www.ppaonline.com.au/wp-content/uploads/2020/04/QUM-Program-Rules-COVID-19.pdf (accessed on 14 February 2023).
- Urbis. Evaluation of the Quality Use of Medicines Program. 2018. Available online: https://www.pbs.gov.au/general/sixth-cpa-pages/cpp-files/QUM-Evaluation-Final-Report.PDF (accessed on 9 January 2023).
- Australian Government. Ministers. On-Site Pharmacists to Improve Medication Management in RACFs. 2022. Available online: https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/on-site-pharmacists-to-improve-medication-management-in-racfs (accessed on 9 January 2023).
- Australian Government. Department of Health and Aged Care. National Aged Care Mandatory Quality Indicator Program (QI Program). 2022. Available online: https://www.health.gov.au/our-work/qi-program (accessed on 9 January 2023).
- Westbury, J.; Gee, P.; Ling, T.; Kitsos, A.; Peterson, G. More action needed: Psychotropic prescribing in Australian residential aged care. ANZJP 2019, 53, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Manias, E.; Bucknall, T.; Hutchinson, A.; Dow, B.; Borrott, N. Resident and family engagement in medication management in aged care facilities: A systematic review. Expert. Opin. Drug. Saf. 2021, 20, 1391–1409. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, A.; Bradley, S.; Xiao, L.; Belan, I.; Wallace, T. Antipsychotic use for behaviours by persons with dementia in residential aged care: The relatives’ perspectives. Aust. J. Adv. Nurs. 2017, 35, 23–32. [Google Scholar]
- Australian Government Department of Health and Ageing. Guiding Principles for Medication Management in Residential Aged Care Facilities—A Guide for Residents and Carers. 2012 Canberra: Australian Government Department of Health and Ageing. Available online: https://healthinfonet.ecu.edu.au/key-resources/resources/24378/?title=Guiding+principles+for+medication+management+in+residential+aged+care+facilities+%E2%80%93+a+guide+for+residents+and+carers&contentid=24378_1 (accessed on 24 January 2023).



{kind=link}
{kind=link}
| Keyword | Sub-Keyword | Issues |
|---|---|---|
| Abuse | Physical | 8 |
| Psychological/emotional | 1 | |
| Choice and dignity Client assessment & implementation Consultation and communication | Right to refuse medication | 7 |
| Polypharmacy review | 3 | |
| Ability to express needs/wants | 3 | |
| Information about medication | 31 | |
| Goods & equipment | Medical and pharmaceutical supplies | 12 |
| Healthcare | Allied health assessment and services | 10 |
| Chemical restraint | 77 | |
| Constipation and continence management | 22 | |
| Dementia management | 14 | |
| Falls prevention and post-falls management | 9 | |
| Infectious diseases and infection control | 23 | |
| Medication administration/management | 824 | |
| Pain management | 60 | |
| Palliative/end-of-life care | 18 | |
| Behaviour management | 11 | |
| Personal care | Personal safety and interventions | 1 |
| Total | 1134 |
| Keyword | Sub-Keyword | Categorization | Complaint Issue | No. Issues |
|---|---|---|---|---|
| Healthcare | Medication administration and management Nursing Chemical restraint | Right resident Right medicine Right dose Right time Right route Right documentation Monitoring Appropriate policies/ systems Appropriate policies/ systems Restrictive practice | - giving resident another’s medicine - staff giving incorrect medicine - given medicine they are allergic to - wrong dose given - medicine missed or withheld - medicine given late - medicine delayed or not started - medicine given incorrectly - medication given unlawfully - medication charts not accurate - adverse effects missed - residents not monitored for effect - inadequate policies and systems - poor storage and accountability - poor ‘prn’ medication policy - tablets found on floor or untaken - medicines given by unqualified staff - self-administration not facilitated - medication used as restraint | 25 36 10 53 119 113 80 27 44 38 30 22 116 30 16 13 68 28 168 |
| Choice & Dignity | Right to refuse medicine | Right to refuse medication | - informed consent not sought - forced to take medication | 65 13 |
| Consultation & Communication | Medication Information | Medication information | - no information at care transitions - not informed when changes made | 24 19 |
| Service Implementation | Polypharmacy review | Access to medication review | - medication regimen not reviewed | 13 |
| Goods & equipment | Pharmaceutical supplies | Quality provision of medicine | - substandard provision of medicine - poor pharmacy supply service | 47 7 |
| Total | 1224 |
| Medical Condition | Additional Details | No. of Issues | Total no. of Complaint Issues |
|---|---|---|---|
| Pain | S8/opioids | 91 | 181 |
| management/ | Paracetamol | 8 | |
| palliative care | S4 medication | 4 | |
| General pain management | 78 | ||
| Sedation | Antipsychotics | 35 | 172 |
| Benzodiazepines | 16 | ||
| Agent not specified | 121 | ||
| Infectious | Urinary tract infection (UTI) | 28 | 54 |
| disease | Respiratory infections | 4 | |
| Fungal infections | 4 | ||
| Skin infections | 3 | ||
| Antibiotics in general | 15 | ||
| Diabetes | Insulin | 16 | 29 |
| Other diabetes issues | 13 | ||
| Parkinson’s disease | Levodopa | 6 | 28 |
| Apomorphine | 2 | ||
| Late or missed doses | 20 | ||
| Asthma | Inhalers and nebulizers | 18 | 18 |
| Constipation | Laxatives | 16 | 16 |
| Eye | General eyedrop use | 14 | 14 |
| Anticoagulation | Warfarin or ‘blood-thinner’ | 8 | 11 |
| Aspirin | 1 | ||
| INR results | 2 | ||
| Vaccination | Influenza | 10 | 10 |
| Cardiovascular | Heart | 5 | 10 |
| Hypertension | 3 | ||
| Immunotherapy | Oedema | 2 | |
| Anticonvulsants | Corticosteroids/chemo | 6/2 | 8 |
| Thyroid | Valproate/carbamazepine | 3 | 2 |
| Thyroxine | 1 | 1 | |
| Total | 554 |
| Medicine | No of Complaint Issues |
|---|---|
| Morphine | 31 |
| Oxycontin | 22 |
| Risperidone | 16 |
| Insulin | 16 |
| Influenza vaccine | 10 |
| Paracetamol | 8 |
| Levodopa | 6 |
| Buprenorphine | 4 |
| Fentanyl | 4 |
| Warfarin | 4 |
| Quetiapine | 3 |
| Oxazepam | 3 |
| Prednisolone | 3 |
| Salbutamol | 3 |
| Complainant Type | No Medication-Related Complaints | Proportion of Complaints (%) | No of Complaints 2019–2020 Report [15] | Proportion of Complaints (%) | Proportion Difference (%) | Chi- Squared | p Value * |
|---|---|---|---|---|---|---|---|
| Representative or family | 622 | 54.9 | 4507 | 52.8 | 2.1 | 1.8 | 0.183 |
| Anonymous | 306 | 27.0 | 1569 | 18.4 | 8.6 | 47.3 | <0.0001 |
| Consumer | 96 | 8.5 | 1686 | 19.7 | −11.2 | 83.7 | <0.0001 |
| Other interested | 89 | 7.9 | 602 | 7.0 | 0.9 | 1.1 | 0.299 |
| External agency/ Internal referral | 20 | 1.8 | 175 | 2.1 | −0.4 | 0.8 | 0.372 |
| Total | 1134 | 100 | 8539 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Breen, J.L.; Williams, K.V.; Wroth, M.J. Medication-Related Complaints in Residential Aged Care. Pharmacy 2023, 11, 63. https://doi.org/10.3390/pharmacy11020063
Breen JL, Williams KV, Wroth MJ. Medication-Related Complaints in Residential Aged Care. Pharmacy. 2023; 11(2):63. https://doi.org/10.3390/pharmacy11020063
Chicago/Turabian StyleBreen, Juanita L., Kathleen V. Williams, and Melanie J. Wroth. 2023. "Medication-Related Complaints in Residential Aged Care" Pharmacy 11, no. 2: 63. https://doi.org/10.3390/pharmacy11020063